
The Impact of Time Interval between Hepatic Resection and Liver Transplantation on Clinical Outcome in Patients with Hepatocellular Carcinoma




Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Variables
2.3. Statistical Analysis
2.3.1. Fractional Polynomial Regression
2.3.2. Survival Analysis
3. Results
3.1. Predictors of Comprehensive Complication Index (CCI) ≥ 29.6
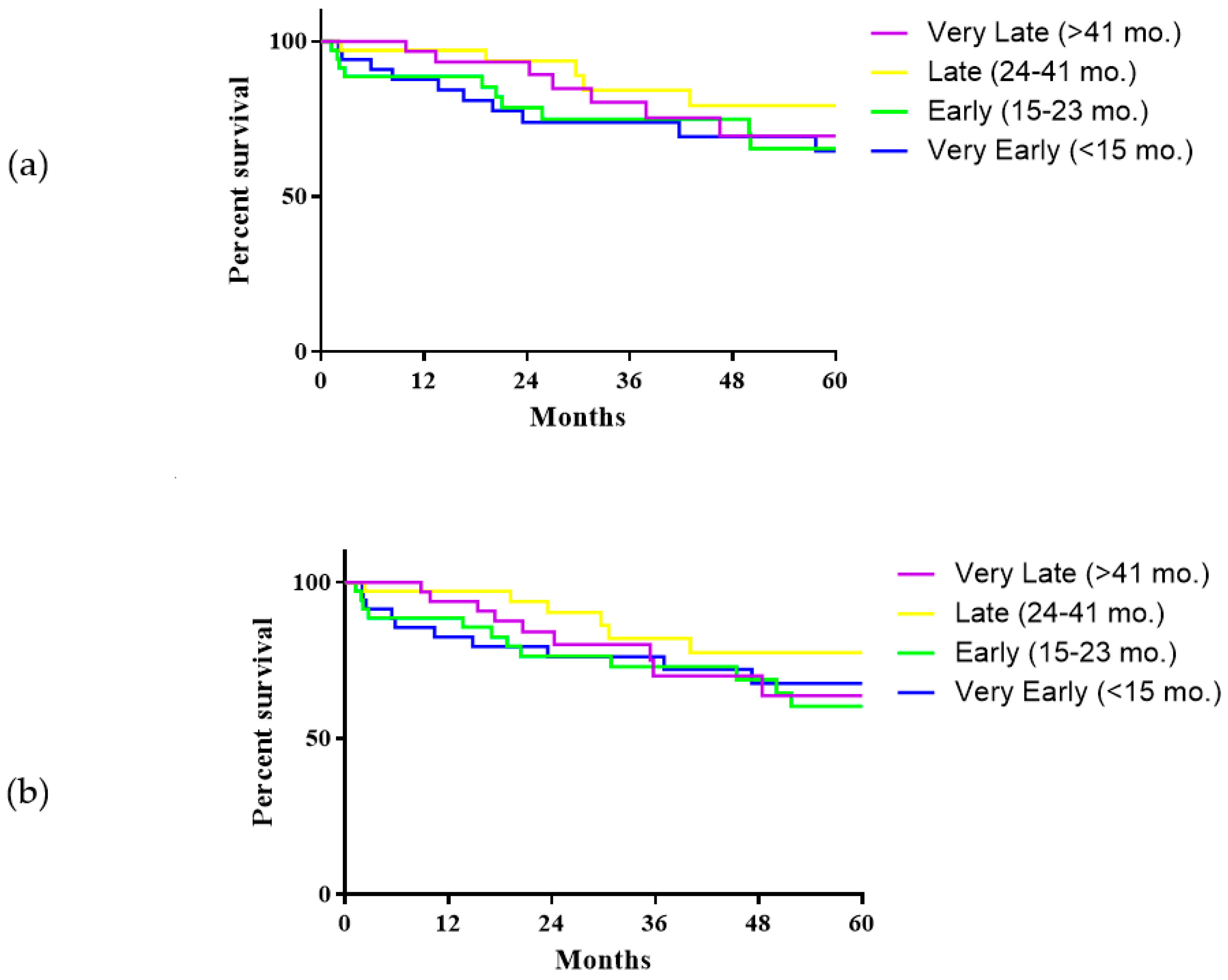
3.2. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fan, S.-T.; Lo, C.-M.; Liu, C.-L.; Lam, C.-M.; Yuen, W.-K.; Yeung, C.; Wong, J. Hepatectomy for Hepatocellular Carcinoma: Toward Zero Hospital Deaths. Ann. Surg. 1999, 229, 322–330. [Google Scholar] [CrossRef]
- Centonze, L.; Di Sandro, S.; Lauterio, A.; De Carlis, R.; Frassoni, S.; Rampoldi, A.; Tuscano, B.; Bagnardi, V.; Vanzulli, A.; De Carlis, L. Surgical Resection vs. Percutaneous Ablation for Single Hepatocellular Carcinoma: Exploring the Impact of Li-RADS Classification on Oncological Outcomes. Cancers 2021, 13, 1671. [Google Scholar] [CrossRef] [PubMed]
- Bhangui, P.; Allard, M.A.; Vibert, E.; Cherqui, D.; Pelletier, G.; Cunha, A.S.; Guettier, C.; Vallee, J.-C.D.; Saliba, F.; Bismuth, H.; et al. Salvage Versus Primary Liver Transplantation for Early Hepatocellular Carcinoma. Ann. Surg. 2016, 264, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Del Gaudio, M.; Ercolani, G.; Ravaioli, M.; Cescon, M.; Lauro, A.; Vivarelli, M.; Zanello, M.; Cucchetti, A.; Vetrone, G.; Tuci, F.; et al. Liver Transplantation for Recurrent Hepatocellular Carcinoma on Cirrhosis After Liver Resection: University of Bologna Experience. Arab. Archaeol. Epigr. 2008, 8, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Belghiti, J.; Cortes, A.; Abdalla, E.K.; Régimbeau, J.M.; Prakash, K.; Durand, F.; Sommacale, D.; Dondero, F.; Lesurtel, M.; Sauvanet, A.; et al. Resection Prior to Liver Transplantation for Hepatocellular Carcinoma. Ann. Surg. 2003, 238, 885–893. [Google Scholar] [CrossRef] [PubMed]
- Sadamori, H.; Yagi, T.; Shinoura, S.; Umeda, Y.; Yoshida, R.; Satoh, D.; Nobuoka, D.; Utsumi, M.; Fujiwara, T. Risk factors for major morbidity after liver resection for hepatocellular carcinoma. BJS 2012, 100, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Slankamenac, K.; Graf, R.; Barkun, J.; Puhan, M.A.; Clavien, P.-A. The Comprehensive Complication Index. Ann. Surg. 2013, 258, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Muller, X.; Marcon, F.; Sapisochin, G.; Marquez, M.; Dondero, F.; Rayar, M.; Doyle, M.M.B.; Callans, L.; Li, J.; Nowak, G.; et al. Defining Benchmarks in Liver Transplantation. Ann. Surg. 2018, 267, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Long, J.; Ryoo, J.H. Using fractional polynomials to model non-linear trends in longitudinal data. Br. J. Math. Stat. Psychol. 2010, 63, 177–203. [Google Scholar] [CrossRef]
- Fine, J.P.; Gray, R.J. A Proportional Hazards Model for the Subdistribution of a Competing Risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.-I.; Shirabe, K.; Tsuijita, E.; Takeishi, K.; Ikegami, T.; Yoshizumi, T.; Soejima, Y.; Ikeda, T.; Utsunomiya, T.; Maehara, Y. Third or more repeat hepatectomy for recurrent hepatocellular carcinoma. Surg. 2013, 154, 1038–1045. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Azoulay, D.; Castaing, D.; Eshkenazy, R.; Pascal, G.; Hashizume, K.; Samuel, D.; Bismuth, H. Liver Resection as a Bridge to Transplantation for Hepatocellular Carcinoma on Cirrhosis. Ann. Surg. 2003, 238, 508–519. [Google Scholar] [CrossRef]
- Yadav, D.K.; Chen, W.; Bai, X.; Singh, A.; Li, G.; Ma, T.; Yu, X.; Xiao, Z.; Huang, B.; Liang, T. Salvage Liver Transplant versus Primary Liver Transplant for Patients with Hepatocellular Carcinoma. Ann. Transplant. 2018, 23, 524–545. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Q.; Geng, T.-T.; He, L.; Gao, H. Harm and Benefits of Salvage Transplantation for Hepatocellular Carcinoma: An Updated Meta-analysis. Transplant. Proc. 2016, 48, 3336–3347. [Google Scholar] [CrossRef]
- Ma, K.W.; Chok, K.S.H.; She, W.H.; Chan, A.C.Y.; Cheung, T.T.; Dai, W.C.; Fung, J.Y.Y.; Lo, C.M. Defining Optimal Surgical Treatment for Recurrent Hepatocellular Carcinoma: A Propensity Score Matched Analysis. Liver Transplant. 2018, 24, 1062–1069. [Google Scholar] [CrossRef]
- Hu, Z.; Wang, W.; Li, Z.; Ye, S.; Zheng, S.-S. Recipient outcomes of salvage liver transplantation versus primary liver transplantation: A systematic review and meta-analysis. Liver Transplant. 2012, 18, 1316–1323. [Google Scholar] [CrossRef]
- McHugh, P.P.; Shah, S.H.; Johnston, T.D.; Gedaly, R.; Ranjan, D. Predicting dry weight in patients with ascites and liver cirrhosis using computed tomography imaging. Hepato-Gastroenterol. 2010, 57, 591–597. [Google Scholar]
- Staiger, R.D.; Schwandt, H.; Puhan, M.A.; Clavien, P. Improving surgical outcomes through benchmarking. BJS 2018, 106, 59–64. [Google Scholar] [CrossRef]
- Bismuth, H.; Majno, P.E. Hepatobiliary surgery. J. Hepatol. 2000, 32, 208–224. [Google Scholar] [CrossRef]
- Csikesz, N.G.; Simons, J.P.; Tseng, J.F.; Shah, S.A. Surgical Specialization and Operative Mortality in Hepato-Pancreatico-Biliary (HPB) Surgery. J. Gastrointest. Surg. 2008, 12, 1534–1539. [Google Scholar] [CrossRef] [PubMed]
- Ausania, F.; Al Shwely, F.; Farguell, J.; Beltrán, J.; Calatayud, D.; Sánchez-Cabús, S.; Ferrer, J.; Rull, R.; Fuster, J.; García-Valdecasas, J.C.; et al. Factors Associated with Prolonged Recipient Hepatectomy Time During Liver Transplantation: A Single-Centre Experience. World J. Surg. 2020, 44, 3486–3490. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.P.; Berger, N.G.; Yin, Z.; Liu, Y.; Tsai, S.; Christians, K.K.; Clarke, C.N.; Mogal, H.; Gamblin, T.C. The effect of prior upper abdominal surgery on outcomes after liver transplantation for hepatocellular carcinoma: An analysis of the database of the organ procurement transplant network. Surgery 2018, 163, 1028–1034. [Google Scholar] [CrossRef] [PubMed]
- Rana, A.; Petrowsky, H.; Hong, J.C.; Agopian, V.G.; Kaldas, F.M.; Farmer, D.; Yersiz, H.; Hiatt, J.R.; Busuttil, R.W. Blood Transfusion Requirement During Liver Transplantation Is an Important Risk Factor for Mortality. J. Am. Coll. Surg. 2013, 216, 902–907. [Google Scholar] [CrossRef] [PubMed]
- Oligane, H.C.; Xing, M.; Kim, H.S. Effect of Bridging Local-Regional Therapy on Recurrence of Hepatocellular Carcinoma and Survival after Orthotopic Liver Transplantation. Radiology 2017, 282, 869–879. [Google Scholar] [CrossRef]
- Cescon, M.; Cucchetti, A.; Ravaioli, M.; Pinna, A.D. Hepatocellular carcinoma locoregional therapies for patients in the waiting list. Impact on transplantability and recurrence rate. J. Hepatol. 2013, 58, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Di Sandro, S.; Bagnardi, V.; Cucchetti, A.; Lauterio, A.; De Carlis, R.; Benuzzi, L.; Danieli, M.; Botta, F.; Centonze, L.; Najjar, M.; et al. From a Philosophical Framework to a Valid Prognostic Staging System of the New "Comprehensive Assessment" for Transplantable Hepatocellular Carcinoma. Cancers 2019, 11, 741. [Google Scholar] [CrossRef]
- Cucchetti, A.; Serenari, M.; Sposito, C.; Di Sandro, S.; Mosconi, C.; Vicentin, I.; Garanzini, E.; Mazzaferro, V.; De Carlis, L.; Golfieri, R.; et al. Including mRECIST in the Metroticket 2.0 criteria improves prediction of hepatocellular carcinoma-related death after liver transplant. J. Hepatol. 2020, 73, 342–348. [Google Scholar] [CrossRef]
- Laurent, A.; Tayar, C.; Andréoletti, M.; Lauzet, J.-Y.; Merle, J.-C.; Cherqui, D. Laparoscopic liver resection facilitates salvage liver transplantation for hepatocellular carcinoma. J. Hepato-Biliary-Pancreatic Surg. 2009, 16, 310–314. [Google Scholar] [CrossRef]
- Felli, E.; Cillo, U.; Pinna, A.D.; De Carlis, L.; Ercolani, G.; Santoro, R.; Gringeri, E.; Di Sandro, S.; Di Laudo, M.; Di Giunta, M.; et al. Salvage liver transplantation after laparoscopic resection for hepatocellular carcinoma: A multicenter experience. Updat. Surg. 2015, 67, 215–222. [Google Scholar] [CrossRef]
- Rhu, J.; Kim, J.M.; Choi, G.S.; Kwon, C.H.D.; Joh, J.-W.; Soubrane, O. Laparoscopy of hepatocellular carcinoma is helpful in minimizing intra-abdominal adhesion during salvage transplantation. Ann. Surg. Treat. Res. 2018, 95, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Sandri, G.B.L.; Lai, Q.; Ravaioli, M.; Di Sandro, S.; Balzano, E.; Pagano, D.; Magistri, P.; Di Benedetto, F.; Rossi, M.; Gruttadauria, S.; et al. The Role of Salvage Transplantation in Patients Initially Treated with Open Versus Minimally Invasive Liver Surgery: An Intention-to-Treat Analysis. Liver Transplant. 2020, 26, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Ratti, F.; Cipriani, F.; Reineke, R.; Catena, M.; Comotti, L.; Beretta, L.; Aldrighetti, L. Impact of ERAS approach and minimally-invasive techniques on outcome of patients undergoing liver surgery for hepatocellular carcinoma. Dig. Liver Dis. 2016, 48, 1243–1248. [Google Scholar] [CrossRef]
- Ratti, F.; Cipriani, F.; Ariotti, R.; Giannone, F.; Paganelli, M.; Aldrighetti, L. Laparoscopic major hepatectomies: Current trends and indications. A comparison with the open technique. Updat. Surg. 2015, 67, 157–167. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | n = 140 |
|---|---|
| Age, median (range), years | 56 (12–70) |
| LRT before HR, n (%) | 27 (19.3) |
| Laparoscopic approach, n (%) | 21 (15) |
| Type of HR, n (%) | |
| Wedge | 44 (31.4) |
| Bisegmentectomy | 39 (27.9) |
| Segmentectomy | 39 (27.8) |
| Right hepatectomy | 9 (6.4) |
| Left hepatectomy | 6 (4.3) |
| Right trisectionectomy | 2 (1.4) |
| Central hepatectomy | 1 (0.8) |
| HR +RFA, n (%) | 9 (6.4) |
| IAC after HR, n (%) | 27 (19) |
| Tumor number, median (IQR), n | 1 (1–2) |
| Tumor diameter max, median (IQR), mm | 29 (20–44) |
| Variable | n = 140 |
|---|---|
| Age, median (range), years | 59 (12–73) |
| Male sex, n (%) | 123 (88) |
| Cardiovascular disease, n (%) | 51 (36.4) |
| Renal disease, n (%) | 16 (11.4) |
| Pulmonary disease, n (%) | 33 (23.6) |
| Diabetes, n (%) | 41 (29.3) |
| BMI, median, (IQR), kg/m2 | 26 (23–28) |
| MELD, median, (IQR), points | 9 (8–12) |
| MELD > 20, n (%) | 14 (10) |
| Viral etiology, n (%) | 97 (70) |
| Time HR-SLT, median (IQR) months | 23.1 (IQR: 14–41) |
| SLT era, n (%) 2000–2009 2010–2018 | 45 (32) 95 (68) |
| Donor age, median (range), years | 59 (10–87) |
| Tumor number, median (IQR), n * | 1 (0–3) |
| Tumor diameter max, median (IQR), mm * | 13 (0–23) |
| mVI+, n (%) * | 48 (34.5) |
| Alpha-fetoprotein, median (IQR), ng/mL | 7 (4–17) |
| Cold Ischemia Time, median (IQR), min | 407 (339–510) |
| Operative Time, median (IQR), min | 480 (405–600) |
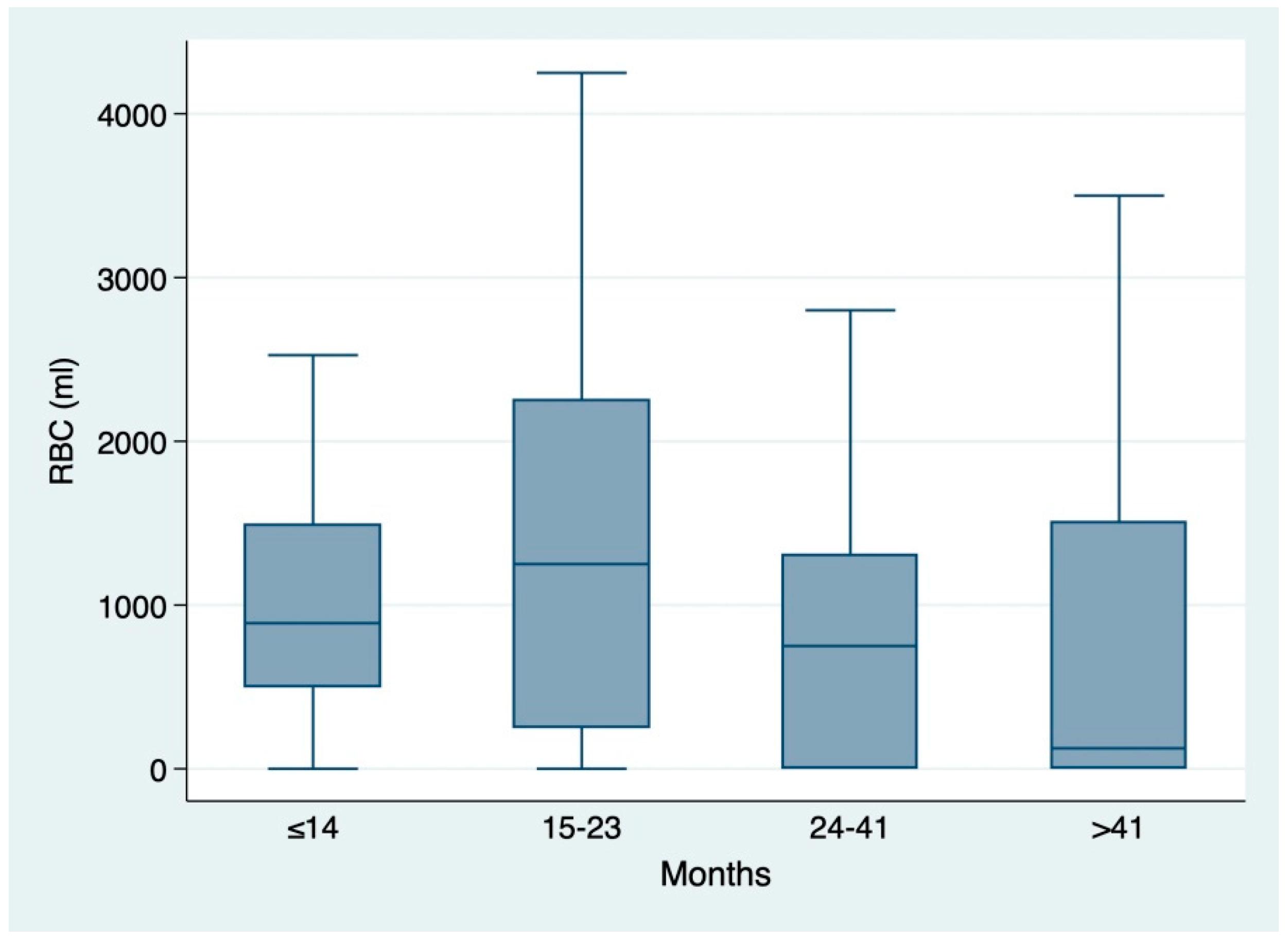
| Blood transfusion, median (IQR), ml | 889 (0–2250) |
| ICU stay, median (IQR), days | 5 (3–8) |
| Post-operative hemorrhage, n (%) | 6 (4.3) |
| Biliary complications, n (%) | 14 (10) |
| Hepatic artery thrombosis, n (%) | 1 (0.7) |
| Re-operation, n (%) | 20 (14.3) |
| PGNF, n (%) | 5 (3.6) |
| Re-LT, n (%) | 6 (4.3) |
| CCI, median (IQR), points | 20.9 (0–42.4) |
| Clavien ≥ IIIA morbidity, n (%) | 49 (35) |
| Hospital stay, median (IQR), days | 16 (0–25) |
| In-hospital mortality, n (%) | 2 (1.4) |
| 90-day mortality, n (%) | 7 (5) |
| Variable | CCI < 29.6 (n = 90) | CCI ≥ 29.6 (n = 50) | p-Value |
|---|---|---|---|
| Male sex, n (%) | 76 (84) | 47 (94) | 0.097 |
| BMI, median (IQR), kg/m2 | 25.1 (23–27) | 27 (24–29) | 0.041 |
| Comorbidities, n (%) | 32 (35) | 25 (50) | 0.096 |
| LRT after HR, n (%) | 60 (67) | 34 (68) | 0.872 |
| SLT era (2010–2018), n (%) | 56 (62) | 39 (78) | 0.055 |
| Laparoscopic approach, n (%) | 13 (14) | 8 (16) | 0.805 |
| Type of HR | 0.775 | ||
| Segmentectomy, n (%) | 27 (30) | 12 (24) | |
| Wedge, n (%) | 26 (29) | 18 (36) | |
| Bisegmentectomy, n (%) | 26 (29) | 13 (26) | |
| Major hepatectomy, n (%) | 11 (12) | 7 (14) | |
| HR + RFA, n (%) | 6 (7) | 3 (6) | 0.878 |
| Repeat HR | 4 (4.4) | 4 (8) | 0.385 |
| IAC after HR, n (%) | 50 (56) | 28 (56) | 0.960 |
| Time HR-SLT, n (%) | |||
| ≤14 mo. | 25 (71.4) | 10 (28.6) | 0.055 |
| 15–23 mo. | 16 (45.7) | 19 (54.3) | |
| 24–41 mo. | 23 (65.7) | 12 (34.3) | |
| >41 mo. | 26 (74.3) | 9 (25.7) | |
| Recipient age, median (range), years | 58 (16–73) | 60 (12–70) | 0.429 |
| MELD, median, (IQR), points | 9 (7–12) | 10 (9–15) | 0.005 |
| Donor age, median (range), years | 58 (17–87) | 63 (10–85) | 0.155 |
| ICU stay, median (IQR), days | 4 (3–6) | 9 (6–13) | <0.001 |
| Blood transfusion, median (IQR), ml | 642 (0–1735) | 1058 (500–2400) | 0.069 |
| Biliary complications, n (%) | 5 (5.5) | 9 (18) | 0.019 |
| Hepatic artery thrombosis, n (%) | 0 (0) | 1 (2) | 0.178 |
| Re-operation, n (%) | 0 (0) | 20 (40) | <0.001 |
| Post-operative hemorrhage, n (%) | 0 (0) | 6 (12) | 0.001 |
| Hospital stay, median (IQR), days | 13 (9–20) | 21 (15–29) | 0.001 |
| PGNF, n (%) | 0 | 5 (10) | 0.002 |
| Re-LT, n (%) | 0 (0) | 6 (12) | 0.001 |
| 90-day mortality, n (%) | 3 (3) | 4 (8) | 0.225 |
| Variable | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Male Sex | 2.89 | 2.44–3.42 | <0.001 | 4.67 | 0.97–22.32 | 0.053 |
| Comorbidities | 1.81 | 0.89–3.69 | 0.101 | |||
| BMI (per 1 kg/m2) | 1.05 | 1.03–1.08 | <0.001 | 1.07 | 1.07–1.08 | <0.001 |
| TACE | 1.35 | 0.87–2.11 | 0.182 | |||
| RFA | 0.74 | 0.49–1.11 | 0.144 | |||
| Major hepatectomy | 1.17 | 0.75–1.83 | 0.494 | |||
| Repeat resection | 1.87 | 0.75–4.67 | 0.181 | |||
| Laparoscopic approach | 1.13 | 0.35–3.65 | 0.840 | |||
| Time HR-SLT (per 1 mo.) | 0.98 | 0.98–0.99 | 0.007 | 0.98 | 0.98–0.99 | <0.001 |
| IAC post-HR | 1.02 | 0.68–1.53 | 0.931 | |||
| SLT era (2010–2018) | 2.15 | 0.81–5.70 | 0.123 | |||
| Recipient age (per 1 yr) | 1.01 | 0.98–1.04 | 0.521 | |||
| MELD score (per 1 point) | 1.06 | 1.01–1.12 | 0.022 | 1.08 | 0.98–1.18 | 0.041 |
| Donor age > 60 yrs | 1.49 | 0.70–3.17 | 0.300 | |||
| Variable | Multivariate Analysis | ||
|---|---|---|---|
| OR | 95% CI | p-Value | |
| BMI | 1.07 | 1.07–1.08 | <0.001 |
| Male Sex | 4.6 | 0.95–22.57 | 0.058 |
| MELD score | 1.07 | 1.00–1.14 | 0.036 |
| time HR-SLTFP | 0.88 | 0.84–0.94 | <0.001 |
| Variable | Competing Risk Regression | ||
|---|---|---|---|
| sHR | CI 95% | p-Value | |
| Last AFP before LT | 0.99 | 0.99–1.00 | 0.351 |
| mVI * | 4.22 | 1.42–12.52 | 0.009 |
| Tumor number * | 1.02 | 0.97–1.06 | 0.504 |
| Tumor diameter * | 1.05 | 1.02–1.07 | 0.001 |
| Time HR-SLTFP | 1.06 | 0.69–1.62 | 0.796 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serenari, M.; Prosperi, E.; Allard, M.-A.; Paterno, M.; Golse, N.; Laurenzi, A.; Adam, R.; Ravaioli, M.; Cherqui, D.; Cescon, M. The Impact of Time Interval between Hepatic Resection and Liver Transplantation on Clinical Outcome in Patients with Hepatocellular Carcinoma. Cancers 2021, 13, 2398. https://doi.org/10.3390/cancers13102398
Serenari M, Prosperi E, Allard M-A, Paterno M, Golse N, Laurenzi A, Adam R, Ravaioli M, Cherqui D, Cescon M. The Impact of Time Interval between Hepatic Resection and Liver Transplantation on Clinical Outcome in Patients with Hepatocellular Carcinoma. Cancers. 2021; 13(10):2398. https://doi.org/10.3390/cancers13102398
Chicago/Turabian StyleSerenari, Matteo, Enrico Prosperi, Marc-Antoine Allard, Michele Paterno, Nicolas Golse, Andrea Laurenzi, René Adam, Matteo Ravaioli, Daniel Cherqui, and Matteo Cescon. 2021. "The Impact of Time Interval between Hepatic Resection and Liver Transplantation on Clinical Outcome in Patients with Hepatocellular Carcinoma" Cancers 13, no. 10: 2398. https://doi.org/10.3390/cancers13102398
APA StyleSerenari, M., Prosperi, E., Allard, M.-A., Paterno, M., Golse, N., Laurenzi, A., Adam, R., Ravaioli, M., Cherqui, D., & Cescon, M. (2021). The Impact of Time Interval between Hepatic Resection and Liver Transplantation on Clinical Outcome in Patients with Hepatocellular Carcinoma. Cancers, 13(10), 2398. https://doi.org/10.3390/cancers13102398