Multi-Parametric Deep Learning Model for Prediction of Overall Survival after Postoperative Concurrent Chemoradiotherapy in Glioblastoma Patients

 , ,
, ,
Abstract
1. Introduction
2. Results
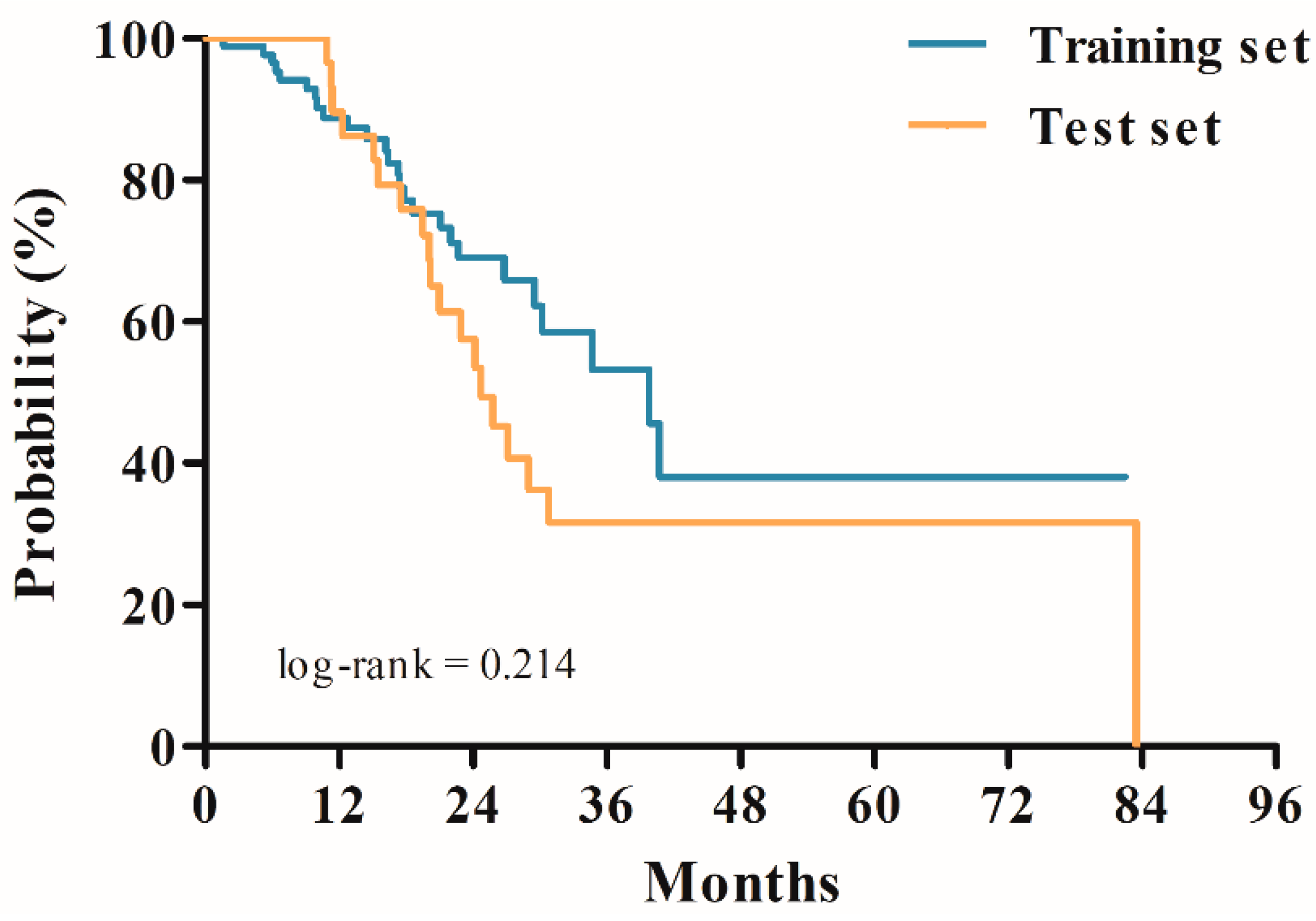
2.1. Patient Characteristics
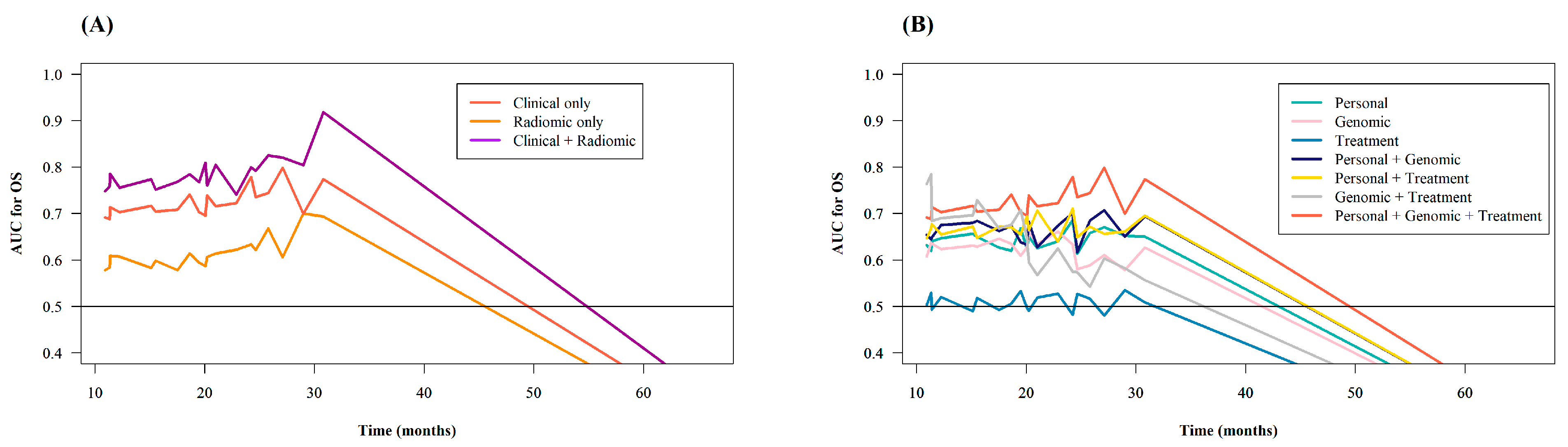
2.2. Model Performance Measured by C-Index and Integrated Area Under the Time-Dependent Receiver Operating Characteristic (ROC) Curve (iAUC)
3. Discussion
4. Materials and Methods
4.1. Patient Selection
4.2. Image Acquisition and Pre-Processing
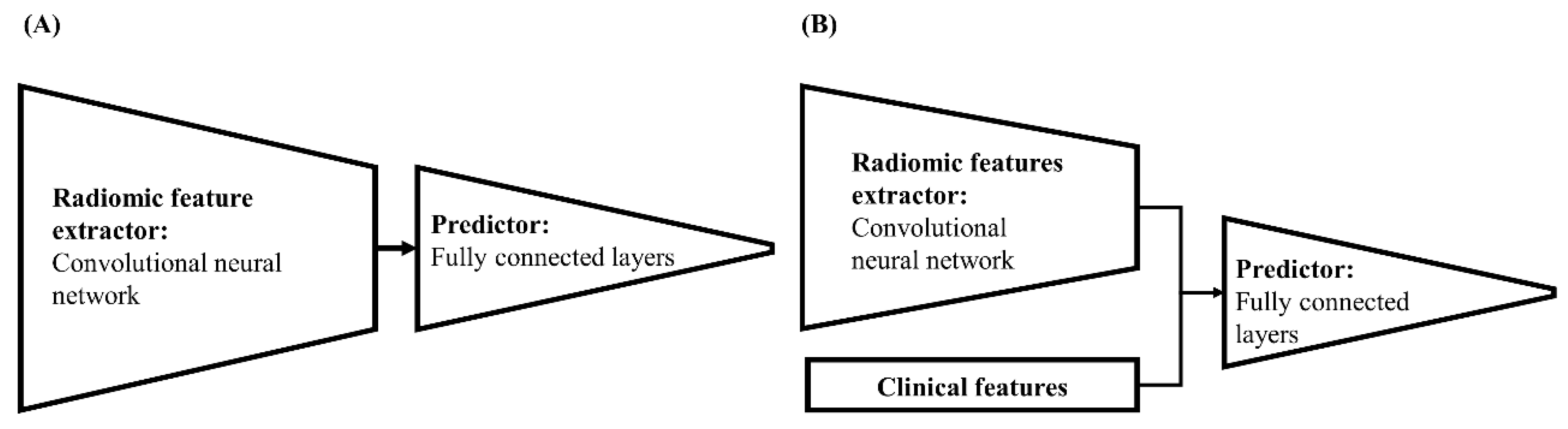
4.3. Building Neural Network-Based Survival-Prediction Models
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bleeker, F.E.; Molenaar, R.J.; Leenstra, S. Recent advances in the molecular understanding of glioblastoma. J. Neurooncol. 2012, 108, 11–27. [Google Scholar] [CrossRef]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Koshy, M.; Villano, J.L.; Dolecek, T.A.; Howard, A.; Mahmood, U.; Chmura, S.J.; Weichselbaum, R.R.; McCarthy, B.J. Improved survival time trends for glioblastoma using the SEER 17 population-based registries. J. Neurooncol. 2012, 107, 207–212. [Google Scholar] [CrossRef]
- Kim, N.; Chang, J.S.; Wee, C.W.; Kim, I.A.; Chang, J.H.; Lee, H.S.; Kim, S.H.; Kang, S.G.; Kim, E.H.; Yoon, H.I.; et al. Validation and optimization of a web-based nomogram for predicting survival of patients with newly diagnosed glioblastoma. Strahlenther. Onkol. 2020, 196, 58–69. [Google Scholar] [CrossRef]
- Gittleman, H.; Lim, D.; Kattan, M.W.; Chakravarti, A.; Gilbert, M.R.; Lassman, A.B.; Lo, S.S.; Machtay, M.; Sloan, A.E.; Sulman, E.P.; et al. An independently validated nomogram for individualized estimation of survival among patients with newly diagnosed glioblastoma: NRG Oncology RTOG 0525 and 0825. Neuro-oncology 2017, 19, 669–677. [Google Scholar]
- Lemee, J.M.; Clavreul, A.; Menei, P. Intratumoral heterogeneity in glioblastoma: Don’t forget the peritumoral brain zone. Neuro-oncology 2015, 17, 1322–1332. [Google Scholar] [CrossRef]
- Soeda, A.; Hara, A.; Kunisada, T.; Yoshimura, S.; Iwama, T.; Park, D.M. The evidence of glioblastoma heterogeneity. Sci. Rep. 2015, 5, 7979. [Google Scholar] [CrossRef]
- Inda, M.M.; Bonavia, R.; Seoane, J. Glioblastoma multiforme: A look inside its heterogeneous nature. Cancers (Basel) 2014, 6, 226–239. [Google Scholar] [CrossRef]
- Juan-Albarracin, J.; Fuster-Garcia, E.; Garcia-Ferrando, G.A.; Garcia-Gomez, J.M. ONCOhabitats: A system for glioblastoma heterogeneity assessment through MRI. Int. J. Med. Inf. 2019, 128, 53–61. [Google Scholar] [CrossRef]
- Bae, S.; Choi, Y.S.; Ahn, S.S.; Chang, J.H.; Kang, S.G.; Kim, E.H.; Kim, S.H.; Lee, S.K. Radiomic MRI phenotyping of glioblastoma: Improving survival prediction. Radiology 2018, 289, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Lao, J.; Chen, Y.; Li, Z.C.; Li, Q.; Zhang, J.; Liu, J.; Zhai, G. A deep learning-based radiomics model for prediction of survival in glioblastoma multiforme. Sci. Rep. 2017, 7, 10353. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.; Xu, Y.; Jin, L.; Aibaidula, A.; Lu, J.; Jiao, Z.; Wu, J.; Zhang, H.; Shen, D. Deep learning of imaging phenotype and genotype for predicting overall survival time of glioblastoma patients. IEEE Trans. Med. Imaging 2020, 39, 2100–2109. [Google Scholar] [CrossRef] [PubMed]
- Sanghani, P.; Ang, B.T.; King, N.K.K.; Ren, H. Overall survival prediction in glioblastoma multiforme patients from volumetric, shape and texture features using machine learning. Surg. Oncol. 2018, 27, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Xu, X.; Yin, L.; Zhang, X.; Li, L.; Lu, H. Relationship between glioblastoma heterogeneity and survival time: An MR imaging texture analysis. AJNR Am. J. Neuroradiol. 2017, 38, 1695–1701. [Google Scholar] [CrossRef]
- Prasanna, P.; Patel, J.; Partovi, S.; Madabhushi, A.; Tiwari, P. Radiomic features from the peritumoral brain parenchyma on treatment-naive multi-parametric MR imaging predict long versus short-term survival in glioblastoma multiforme: Preliminary findings. Eur. Radiol. 2017, 27, 4188–4197. [Google Scholar] [CrossRef]
- Chaddad, A.; Sabri, S.; Niazi, T.; Abdulkarim, B. Prediction of survival with multi-scale radiomic analysis in glioblastoma patients. Med. Biol. Eng. Comput. 2018, 56, 2287–2300. [Google Scholar] [CrossRef]
- Jang, B.S.; Jeon, S.H.; Kim, I.H.; Kim, I.A. Prediction of pseudoprogression versus progression using machine learning algorithm in glioblastoma. Sci. Rep. 2018, 8, 12516. [Google Scholar] [CrossRef]
- Jeong, J.W.; Lee, M.H.; John, F.; Robinette, N.L.; Amit-Yousif, A.J.; Barger, G.R.; Mittal, S.; Juhasz, C. Feasibility of multimodal mri-based deep learning prediction of high amino acid uptake regions and survival in patients with glioblastoma. Front. Neurol. 2019, 10, 1305. [Google Scholar] [CrossRef]
- Macdonald, D.R.; Cascino, T.L.; Schold, S.C., Jr.; Cairncross, J.G. Response criteria for phase II studies of supratentorial malignant glioma. J. Clin. Oncol. 1990, 8, 1277–1280. [Google Scholar] [CrossRef]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; Degroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B.; et al. Updated response assessment criteria for high-grade gliomas: Response assessment in neuro-oncology working group. J. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef]
- Kucharczyk, M.J.; Parpia, S.; Whitton, A.; Greenspoon, J.N. Evaluation of pseudoprogression in patients with glioblastoma. Neurooncol. Pract. 2017, 4, 120–134. [Google Scholar] [CrossRef] [PubMed]
- Peus, D.; Newcomb, N.; Hofer, S. Appraisal of the Karnofsky Performance Status and proposal of a simple algorithmic system for its evaluation. BMC Med. Inform. Decis. Mak. 2013, 13, 72. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Bai, H.; Chen, Y.; Sun, Q.; Liu, L.; Zhou, S.; Wang, G.; Liang, C.; Li, Z.C. A fully-automatic multiparametric radiomics model: Towards reproducible and prognostic imaging signature for prediction of overall survival in glioblastoma multiforme. Sci. Rep. 2017, 7, 14331. [Google Scholar] [CrossRef] [PubMed]
- Kahn, C.E., Jr. From images to actions: Opportunities for artificial intelligence in radiology. Radiology 2017, 285, 719–720. [Google Scholar] [CrossRef]
- Yasaka, K.; Akai, H.; Kunimatsu, A.; Kiryu, S.; Abe, O. Deep learning with convolutional neural network in radiology. Jpn. J. Radiol. 2018, 36, 257–272. [Google Scholar] [CrossRef]
- Bhandari, A.; Koppen, J.; Agzarian, M. Convolutional neural networks for brain tumour segmentation. Insights Imaging 2020, 11, 77. [Google Scholar] [CrossRef]
- Wong, D.J.; Gandomkar, Z.; Wu, W.J.; Zhang, G.; Gao, W.; He, X.; Wang, Y.; Reed, W. Artificial intelligence and convolution neural networks assessing mammographic images: A narrative literature review. J. Med. Radiat. Sci. 2020, 67, 134–142. [Google Scholar] [CrossRef]
- Bernal, J.; Kushibar, K.; Asfaw, D.S.; Valverde, S.; Oliver, A.; Marti, R.; Llado, X. Deep convolutional neural networks for brain image analysis on magnetic resonance imaging: A review. Artif. Intell. Med. 2019, 95, 64–81. [Google Scholar] [CrossRef]
- Qi, M.; Li, Y.; Wu, A.; Jia, Q.; Li, B.; Sun, W.; Dai, Z.; Lu, X.; Zhou, L.; Deng, X.J.M.P. Multi-sequence MR image-based synthetic CT generation using a generative adversarial network for head and neck MRI-only radiotherapy. Med. Phys. 2020, 47, 1880–1894. [Google Scholar] [CrossRef]
- Lamborn, K.R.; Chang, S.M.; Prados, M.D. Prognostic factors for survival of patients with glioblastoma: Recursive partitioning analysis. Neuro-Oncology 2004, 6, 227–235. [Google Scholar] [CrossRef]
- Li, J.; Wang, M.; Won, M.; Shaw, E.G.; Coughlin, C.; Curran, W.J., Jr.; Mehta, M.P. Validation and simplification of the Radiation Therapy Oncology Group recursive partitioning analysis classification for glioblastoma. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Kamarudin, A.N.; Cox, T.; Kolamunnage-Dona, R. Time-dependent ROC curve analysis in medical research: Current methods and applications. BMC Med. Res. Methodol. 2017, 17, 53. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Zhang, Y.; Shao, Y. On comparing 2 correlated C indices with censored survival data. Stat. Med. 2017, 36, 4041–4049. [Google Scholar] [CrossRef] [PubMed]
- Alom, M.Z.; Yakopcic, C.; Hasan, M.; Taha, T.M.; Asari, V.K. Recurrent residual U-Net for medical image segmentation. J. Med. Imaging (Bellingham) 2019, 6, 014006. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Song, J.; Li, L.; Tang, Q. Improving brain tumor segmentation on MRI based on the deep U-net and residual units. J. Xray Sci. Technol. 2020, 28, 95–110. [Google Scholar] [CrossRef]
- Emblem, K.E.; Pinho, M.C.; Zollner, F.G.; Due-Tonnessen, P.; Hald, J.K.; Schad, L.R.; Meling, T.R.; Rapalino, O.; Bjornerud, A. A generic support vector machine model for preoperative glioma survival associations. Radiology 2015, 275, 228–234. [Google Scholar] [CrossRef]
- Wang, S.H.; Phillips, P.; Sui, Y.; Liu, B.; Yang, M.; Cheng, H. Classification of Alzheimer’s Disease Based on Eight-Layer Convolutional Neural Network with Leaky Rectified Linear Unit and Max Pooling. J. Med. Syst. 2018, 42, 85. [Google Scholar] [CrossRef]
- Heagerty, P.J.; Saha-Chaudhuri, P.; Saha-Chaudhuri, M.P. Package ‘RisksetROC’. 2012. Available online: http://cran.rapporter.net/web/packages/risksetROC/risksetROC.pdf (accessed on 26 September 2012).
- Heagerty, P.J.; Zheng, Y. Survival model predictive accuracy and ROC curves. Biometrics 2005, 61, 92–105. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Training Set (n = 88) a | Test Set (n = 30) | p-Value |
|---|---|---|---|
| Age (years) | Median 59 (IQR 50.75–64.25) | Median 54.5 (IQR 48–65.5) | 0.410 |
| Survival time (months) b | Median 17.60 (IQR 10.35–26.68) | Median 23.00 (IQR 17.03–33.59) | 0.214 c |
| Sex | 0.531 | ||
| Male Female | 44 (50.0%) 44 (50.0%) | 13 (43.3%) 17 (56.7%) | |
| ECOG Performance Status | 0.753 | ||
| 0–1 2 | 73 (83.0%) 15 (17.0%) | 27 (90.0%) 3 (10.0%) | |
| Resection | 0.931 | ||
| Gross total resection Subtotal resection | 36 (40.9%) 52 (59.1%) | 12 (40.0%) 18 (60.0%) | |
| IDH mutation | 0.468 | ||
| Yes No | 7 (8.0%) 81 (92.0%) | 4 (13.3%) 26 (86.7%) | |
| MGMT hypermethylation | 0.921 | ||
| Yes No | 42 (47.7%) 46 (52.3%) | 14 (46.7%) 16 (53.3%) | |
| Adjuvant TMZ cycles | Median 6 (IQR 4–6) | Median 6 (IQR 4.5–6) | 0.300 |
| Total radiotherapy dose | 0.778 d | ||
| ≥60 Gy <60 Gy | 73 (83.0%) 15 (17.0%) | 26 (86.7%) 4 (13.3%) |
| Model | Included Features | RMSE (Months) a | Correlation Coefficient |
|---|---|---|---|
| MC1a | Personal only | 16.96 ± 23.89 | 0.562 |
| MC1b | Genomic only | 19.88 ± 30.40 | 0.194 |
| MC1c | Treatment only | 25.18 ± 36.89 | 0.073 |
| MC2a | Personal + Genomic | 17.19 ± 22.96 | 0.579 |
| MC2b | Personal + Treatment | 16.64 ± 28.92 | 0.593 |
| MC2c | Genomic + Treatment | 29.18 ± 38.57 | −0.222 |
| MC3 | Personal + Genomic + Treatment = Clinical | 16.01 ± 26.54 | 0.712 |
| MR | Radiomic only | 17.14 ± 25.47 | 0.499 |
| MCR | Clinical + Radiomic | 14.21 ± 23.07 | 0.788 |
| Model | Included Features | C-Index (95% CI) | iAUC (95% CI) |
|---|---|---|---|
| MC1a | Personal only | 0.644 (0.635, 0.653) | 0.644 (0.636, 0.653) |
| MC1b | Genomic only | 0.664 (0.656, 0.671) | 0.641 (0.634, 0.649) |
| MC1c | Treatment only | 0.562 (0.553, 0.570) | 0.579 (0.572, 0.586) |
| MC2a | Personal + Genomic | 0.696 (0.688, 0.704) | 0.675 (0.666, 0.684) |
| MC2b | Personal + Treatment | 0.665 (0.655, 0.675) | 0.671 (0.663, 0.679) |
| MC2c | Genomic + Treatment | 0.640 (0.630, 0.650) | 0.664 (0.657, 0.672) |
| MC3 | Personal + Genomic + Treatment = Clinical | 0.693 (0.685, 0.701) | 0.723 (0.716, 0.731) |
| MR | Radiomic only | 0.590 (0.579, 0.600) | 0.614 (0.607, 0.621) |
| MCR | Clinical + Radiomic | 0.768 (0.759, 0.776) | 0.790 (0.783, 0.797) |
| Index | Model 1 | Model 2 | Value Difference (95% CI) a | p-Value b |
|---|---|---|---|---|
| C-Index | Clinical only | Clinical + Radiomic | 0.074 (0.070, 0.078) | <0.001 |
| Radiomic only | Clinical + Radiomic | 0.178 (0.174, 0.183) | <0.001 | |
| iAUC | Clinical only | Clinical + Radiomic | 0.067 (0.064, 0.070) | <0.001 |
| Radiomic only | Clinical + Radiomic | 0.176 (0.174, 0.179) | <0.001 |
| Layer | Filter Shape | Shape | Activation/Pooling | |
|---|---|---|---|---|
| Input layer | Input layer | - | 1 × 256 × 256 × 36 † | None |
| Hidden layer: Extractor | Convolution layer | 1 × 1 × 36 × 1 | 1 × 256 × 256 × 1 | None/Max pooling |
| Convolution layer | 1 × 28 × 28 × 1 | 1 ×128 × 128 × 1 | LReLu */Max pooling | |
| Convolution layer | 1 × 14 × 14 × 1 | 1 × 64 × 64 × 1 | LReLu/Max pooling | |
| Convolution layer | 1 × 14 × 14 × 1 | 1 × 32 × 32 × 1 | LReLu/Max pooling | |
| Convolution layer | 1 × 7 × 7 × 1 | 1 × 16 × 16 × 1 | LReLu/None | |
| Convolution layer | 1 × 7 × 7 × 1 | 1 × 16 × 16 × 1 | LReLu/None | |
| Flatten | 1 × 1 × 256 | None | ||
| Fully connected layer | 1 × 256 × 242 | 1 × 1 × 242 | LReLu/None | |
| Concatenate | Concatenate: clinical (14) and radiomic (242) features | 1 × 1 × 256 | None | |
| Hidden layer: Predictor | Fully connected layer | 1 × 242 × 256 | 1 × 1 × 256 | LReLu/None |
| Fully connected layer | 1 × 256 × 128 | 1 × 1 × 128 | LReLu/None | |
| Fully connected layer | 1 × 128 × 64 | 1 × 1 × 64 | LReLu/None | |
| Fully connected layer | 1 × 64 × 32 | 1 × 1 × 32 | None/None | |
| Output layer | Fully connected layer | 1 × 32 × 1 | 1 × 1 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, H.G.; Cheon, W.; Jeong, S.W.; Kim, H.S.; Kim, K.; Nam, H.; Han, Y.; Lim, D.H. Multi-Parametric Deep Learning Model for Prediction of Overall Survival after Postoperative Concurrent Chemoradiotherapy in Glioblastoma Patients. Cancers 2020, 12, 2284. https://doi.org/10.3390/cancers12082284
Yoon HG, Cheon W, Jeong SW, Kim HS, Kim K, Nam H, Han Y, Lim DH. Multi-Parametric Deep Learning Model for Prediction of Overall Survival after Postoperative Concurrent Chemoradiotherapy in Glioblastoma Patients. Cancers. 2020; 12(8):2284. https://doi.org/10.3390/cancers12082284
Chicago/Turabian StyleYoon, Han Gyul, Wonjoong Cheon, Sang Woon Jeong, Hye Seung Kim, Kyunga Kim, Heerim Nam, Youngyih Han, and Do Hoon Lim. 2020. "Multi-Parametric Deep Learning Model for Prediction of Overall Survival after Postoperative Concurrent Chemoradiotherapy in Glioblastoma Patients" Cancers 12, no. 8: 2284. https://doi.org/10.3390/cancers12082284
APA StyleYoon, H. G., Cheon, W., Jeong, S. W., Kim, H. S., Kim, K., Nam, H., Han, Y., & Lim, D. H. (2020). Multi-Parametric Deep Learning Model for Prediction of Overall Survival after Postoperative Concurrent Chemoradiotherapy in Glioblastoma Patients. Cancers, 12(8), 2284. https://doi.org/10.3390/cancers12082284