Identification of a Blood-Based Protein Biomarker Panel for Lung Cancer Detection

 , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Results
2.1. Patient and Healthy Donor Demographics
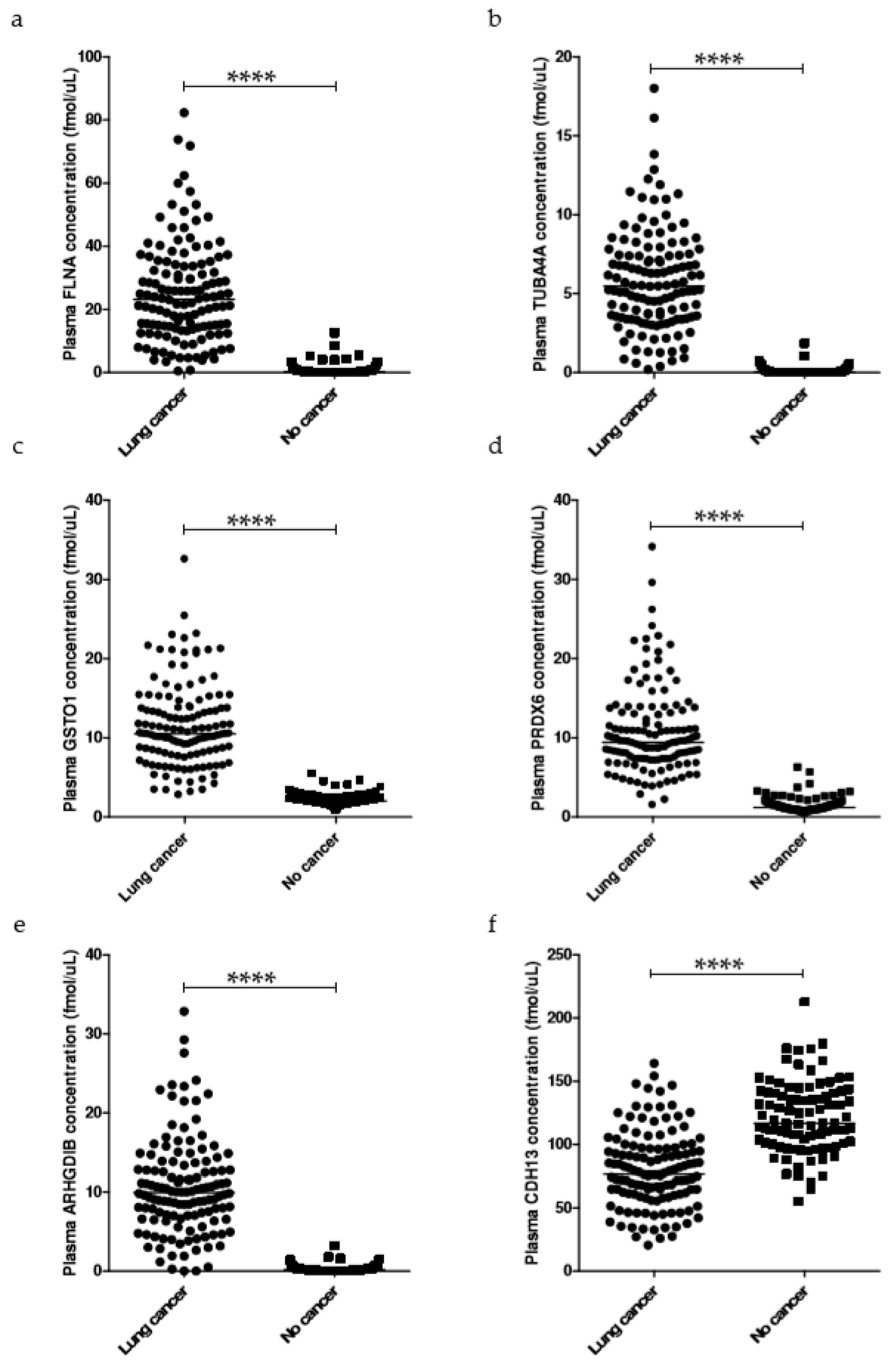
2.2. Broad Selection of Potential Tumor Predictors in Plasma
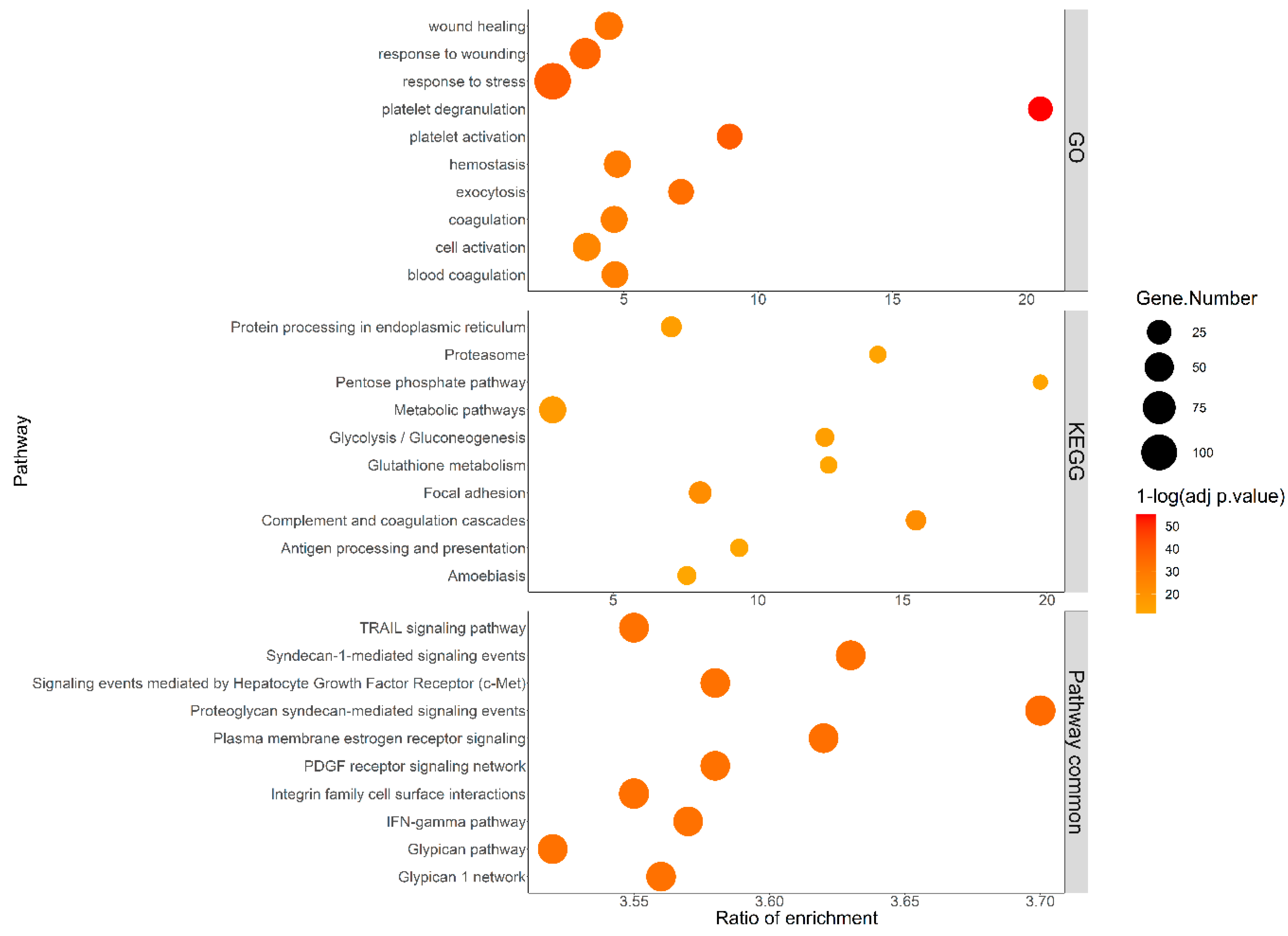
2.3. Pathways Analysis and Interaction Network of the Differentially Expressed Proteins
2.4. Refinement of Biomarker Selection
2.5. Performance Analysis of the Models
2.6. Determination of Biomarker Thresholds for Outcome Prediction
2.7. Panel Performance on the Validation Dataset
3. Discussion
4. Materials and Methods
4.1. Study Cohort
4.2. Plasma Depletion and Processing
4.3. LC-PRM Analysis
4.4. Model Development and Statistical Analysis
4.5. Use of PanelomiX for Threshold Selection
4.6. Pathway Analysis and Protein Interaction
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sturgeon, C. Practice guidelines for tumor marker use in the clinic. Clin. Chem. 2002, 48, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- Marrugo-Ramirez, J.; Mir, M.; Samitier, J. Blood-Based Cancer Biomarkers in Liquid Biopsy: A Promising Non-Invasive Alternative to Tissue Biopsy. Int. J. Mol. Sci. 2018, 19. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.D.; Li, L.; Wang, Y.; Thoburn, C.; Afsari, B.; Danilova, L.; Douville, C.; Javed, A.A.; Wong, F.; Mattox, A.; et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science 2018, 359, 926–930. [Google Scholar] [CrossRef] [PubMed]
- Young, R.P.; Christmas, T.; Hopkins, R.J. Multi-analyte assays and early detection of common cancers. J. Thorac. Dis. 2018, 10, S2165–S2167. [Google Scholar] [CrossRef]
- Duffy, M.J.; O’Byrne, K. Tissue and Blood Biomarkers in Lung Cancer: A Review. Adv. Clin. Chem. 2018, 86, 1–21. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef]
- Ridge, C.A.; McErlean, A.M.; Ginsberg, M.S. Epidemiology of lung cancer. Semin. Intervent. Radiol. 2013, 30, 93–98. [Google Scholar] [CrossRef] [PubMed]
- National Lung Screening Trial Research, T.; Aberle, D.R.; Adams, A.M.; Berg, C.D.; Black, W.C.; Clapp, J.D.; Fagerstrom, R.M.; Gareen, I.F.; Gatsonis, C.; Marcus, P.M.; et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Kennedy, J.; Lee, L.W.; Lin, C.; Yan, P.; Whiteaker, J.; Lorentzen, T.; Schlesser, M.; Wendt, G.; Chalabi, K.; et al. Integrated Strategy for Lung Cancer Biomarker Candidate Discovery by Quantitative Proteomics Profiling on Tumor and Adjacent Normal Lung Tissue. In Proceedings of the 59 th ASMS Conference on Mass Spectrometry and Allied Topics, Denver, CO, USA, 5–9 June 2011. Abstract nr MP 679. [Google Scholar]
- Zhang, H.; Whiteaker, J.; Lin, C.; Yan, P.; Kim, Y.J.; Ross, H.; Tegeler, T.; Selinsky, C.; Petritis, K.; Berchem, G.; et al. Prioritization of Plasma-Based Predictive Markers for Chemotherapy in Lung Cancer Using Fractionation and Targeted Mass Spectrometry. In Proceedings of the 61st ASMS Conference on Mass Spectrometry and Allied Topics, Minneapolis, MN, USA, 9–13 June 2013. Abstract nr MP 541. [Google Scholar]
- Kearney, P.; Boniface, J.J.; Price, N.D.; Hood, L. The building blocks of successful translation of proteomics to the clinic. Curr. Opin. Biotechnol. 2018, 51, 123–129. [Google Scholar] [CrossRef]
- Kim, Y.J.; Sertamo, K.; Pierrard, M.A.; Mesmin, C.; Kim, S.Y.; Schlesser, M.; Berchem, G.; Domon, B. Verification of the biomarker candidates for non-small-cell lung cancer using a targeted proteomics approach. J. Proteome Res. 2015, 14, 1412–1419. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Gallien, S.; van Oostrum, J.; Domon, B. Targeted proteomics strategy applied to biomarker evaluation. Proteom. Clin. Appl. 2013, 7, 739–747. [Google Scholar] [CrossRef]
- Percy, A.J.; Chambers, A.G.; Smith, D.S.; Borchers, C.H. Standardized protocols for quality control of MRM-based plasma proteomic workflows. J. Proteome Res. 2013, 12, 222–233. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Gallien, S.; El-Khoury, V.; Goswami, P.; Sertamo, K.; Schlesser, M.; Berchem, G.; Domon, B. Quantification of SAA1 and SAA2 in lung cancer plasma using the isotype-specific PRM assays. Proteomics 2015, 15, 3116–3125. [Google Scholar] [CrossRef] [PubMed]
- Sievers, E.M.; Bart, R.D.; Backhus, L.M.; Lin, Y.; Starnes, M.; Castanos, R.; Starnes, V.A.; Bremner, R.M. Evaluation of cyclooxygenase-2 inhibition in an orthotopic murine model of lung cancer for dose-dependent effect. J. Thorac. Cardiovasc. Surg. 2005, 129, 1242–1249. [Google Scholar] [CrossRef] [PubMed]
- Salhia, B.; Kiefer, J.; Ross, J.T.; Metapally, R.; Martinez, R.A.; Johnson, K.N.; DiPerna, D.M.; Paquette, K.M.; Jung, S.; Nasser, S.; et al. Integrated genomic and epigenomic analysis of breast cancer brain metastasis. PLoS ONE 2014, 9, e85448. [Google Scholar] [CrossRef]
- Theocharis, A.D.; Karamanos, N.K. Proteoglycans remodeling in cancer: Underlying molecular mechanisms. Matrix. Biol. 2019, 75-76, 220–259. [Google Scholar] [CrossRef]
- Desgrosellier, J.S.; Cheresh, D.A. Integrins in cancer: Biological implications and therapeutic opportunities. Nat. Rev. Cancer 2010, 10, 9–22. [Google Scholar] [CrossRef]
- Noskovicova, N.; Petrek, M.; Eickelberg, O.; Heinzelmann, K. Platelet-derived growth factor signaling in the lung. From lung development and disease to clinical studies. Am. J. Respir Cell Mol. Biol. 2015, 52, 263–284. [Google Scholar] [CrossRef]
- Pietras, R.J.; Marquez-Garban, D.C. Membrane-associated estrogen receptor signaling pathways in human cancers. Clin. Cancer Res. 2007, 13, 4672–4676. [Google Scholar] [CrossRef]
- Landi, L.; Minuti, G.; D’Incecco, A.; Cappuzzo, F. Targeting c-MET in the battle against advanced nonsmall-cell lung cancer. Curr. Opin. Oncol. 2013, 25, 130–136. [Google Scholar] [CrossRef]
- Giubellino, A.; Burke, T.R., Jr.; Bottaro, D.P. Grb2 signaling in cell motility and cancer. Expert Opin Ther Targets 2008, 12, 1021–1033. [Google Scholar] [CrossRef] [PubMed]
- Vachani, A.; Hammoud, Z.; Springmeyer, S.; Cohen, N.; Nguyen, D.; Williamson, C.; Starnes, S.; Hunsucker, S.; Law, S.; Li, X.J.; et al. Clinical Utility of a Plasma Protein Classifier for Indeterminate Lung Nodules. Lung 2015, 193, 1023–1027. [Google Scholar] [CrossRef] [PubMed]
- Molina-Pinelo, S.; Pastor, M.D.; Paz-Ares, L. VeriStrat: A prognostic and/or predictive biomarker for advanced lung cancer patients? Expert Rev. Respir. Med. 2014, 8, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Sone, S.; Takashima, S.; Li, F.; Yang, Z.; Honda, T.; Maruyama, Y.; Hasegawa, M.; Yamanda, T.; Kubo, K.; Hanamura, K.; et al. Mass screening for lung cancer with mobile spiral computed tomography scanner. Lancet 1998, 351, 1242–1245. [Google Scholar] [CrossRef]
- Vachani, A.; Pass, H.I.; Rom, W.N.; Midthun, D.E.; Edell, E.S.; Laviolette, M.; Li, X.J.; Fong, P.Y.; Hunsucker, S.W.; Hayward, C.; et al. Validation of a multiprotein plasma classifier to identify benign lung nodules. J. Thorac. Oncol. 2015, 10, 629–637. [Google Scholar] [CrossRef]
- Li, X.J.; Hayward, C.; Fong, P.Y.; Dominguez, M.; Hunsucker, S.W.; Lee, L.W.; McLean, M.; Law, S.; Butler, H.; Schirm, M.; et al. A blood-based proteomic classifier for the molecular characterization of pulmonary nodules. Sci. Transl. Med. 2013, 5, 207ra142. [Google Scholar] [CrossRef]
- Fornier, M.N.; Seidman, A.D.; Schwartz, M.K.; Ghani, F.; Thiel, R.; Norton, L.; Hudis, C. Serum HER2 extracellular domain in metastatic breast cancer patients treated with weekly trastuzumab and paclitaxel: Association with HER2 status by immunohistochemistry and fluorescence in situ hybridization and with response rate. Ann. Oncol. 2005, 16, 234–239. [Google Scholar] [CrossRef]
- Lam, L.; McAndrew, N.; Yee, M.; Fu, T.; Tchou, J.C.; Zhang, H. Challenges in the clinical utility of the serum test for HER2 ECD. Biochim. Biophys. Acta 2012, 1826, 199–208. [Google Scholar] [CrossRef]
- Kulasingam, V.; Diamandis, E.P. Strategies for discovering novel cancer biomarkers through utilization of emerging technologies. Nat. Clin. Pract. Oncol. 2008, 5, 588–599. [Google Scholar] [CrossRef]
- Abelev, G.I.; Eraiser, T.L. Cellular aspects of alpha-fetoprotein reexpression in tumors. Semin. Cancer Biol. 1999, 9, 95–107. [Google Scholar] [CrossRef]
- Mattarollo, S.R.; Smyth, M.J. A novel axis of innate immunity in cancer. Nat. Immunol. 2010, 11, 981–982. [Google Scholar] [CrossRef] [PubMed]
- Pitteri, S.J.; Kelly-Spratt, K.S.; Gurley, K.E.; Kennedy, J.; Buson, T.B.; Chin, A.; Wang, H.; Zhang, Q.; Wong, C.H.; Chodosh, L.A.; et al. Tumor microenvironment-derived proteins dominate the plasma proteome response during breast cancer induction and progression. Cancer Res. 2011, 71, 5090–5100. [Google Scholar] [CrossRef] [PubMed]
- Griner, E.M.; Dancik, G.M.; Costello, J.C.; Owens, C.; Guin, S.; Edwards, M.G.; Brautigan, D.L.; Theodorescu, D. RhoC Is an Unexpected Target of RhoGDI2 in Prevention of Lung Colonization of Bladder Cancer. Mol. Cancer Res. 2015, 13, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Niu, H.; Wu, B.; Peng, Y.; Jiang, H.; Zhang, Y.; Wang, J.; Zhang, Y.; He, P. RNA interference-mediated knockdown of RhoGDI2 induces the migration and invasion of human lung cancer A549 cells via activating the PI3K/Akt pathway. Tumour. Biol. 2015, 36, 409–419. [Google Scholar] [CrossRef]
- Pacifici, F.; Della Morte, D.; Capuani, B.; Pastore, D.; Bellia, A.; Sbraccia, P.; Di Daniele, N.; Lauro, R.; Lauro, D. Peroxiredoxin6, a Multitask Antioxidant Enzyme Involved in the Pathophysiology of Chronic Noncommunicable Diseases. Antioxid. Redox. Signal. 2019, 30, 399–414. [Google Scholar] [CrossRef]
- Vitali, E.; Boemi, I.; Rosso, L.; Cambiaghi, V.; Novellis, P.; Mantovani, G.; Spada, A.; Alloisio, M.; Veronesi, G.; Ferrero, S.; et al. FLNA is implicated in pulmonary neuroendocrine tumors aggressiveness and progression. Oncotarget 2017, 8, 77330–77340. [Google Scholar] [CrossRef]
- Yi, B.; Zhang, Y.; Zhu, D.; Zhang, L.; Song, S.; He, S.; Zhang, B.; Li, D.; Zhou, J. Overexpression of RhoGDI2 correlates with the progression and prognosis of pancreatic carcinoma. Oncol. Rep. 2015, 33, 1201–1206. [Google Scholar] [CrossRef]
- Yun, H.M.; Park, K.R.; Lee, H.P.; Lee, D.H.; Jo, M.; Shin, D.H.; Yoon, D.Y.; Han, S.B.; Hong, J.T. PRDX6 promotes lung tumor progression via its GPx and iPLA2 activities. Free Radic. Biol. Med. 2014, 69, 367–376. [Google Scholar] [CrossRef]
- Board, P.G.; Menon, D. Structure, function and disease relevance of Omega-class glutathione transferases. Arch. Toxicol. 2016, 90, 1049–1067. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, Q.; Peng, B.; Shao, Q.; Qian, W.; Zhang, J.Y. Identification of glutathione S-transferase omega 1 (GSTO1) protein as a novel tumor-associated antigen and its autoantibody in human esophageal squamous cell carcinoma. Tumour. Biol. 2014, 35, 10871–10877. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Song, X.; Liu, L.; Niu, L.; Wang, X.; Song, X.; Xie, L. Circulating exosomes contain protein biomarkers of metastatic non-small-cell lung cancer. Cancer Sci. 2018, 109, 1701–1709. [Google Scholar] [CrossRef] [PubMed]
- Pu, W.; Geng, X.; Chen, S.; Tan, L.; Tan, Y.; Wang, A.; Lu, Z.; Guo, S.; Chen, X.; Wang, J. Aberrant methylation of CDH13 can be a diagnostic biomarker for lung adenocarcinoma. J. Cancer 2016, 7, 2280–2289. [Google Scholar] [CrossRef] [PubMed]
- Sun, N.; Chen, Z.; Tan, F.; Zhang, B.; Yao, R.; Zhou, C.; Li, J.; Gao, Y.; Liu, Z.; Tan, X.; et al. Isocitrate dehydrogenase 1 is a novel plasma biomarker for the diagnosis of non-small cell lung cancer. Clin. Cancer Res. 2013, 19, 5136–5145. [Google Scholar] [CrossRef]
- Wong, M.C.S.; Lao, X.Q.; Ho, K.F.; Goggins, W.B.; Tse, S.L.A. Incidence and mortality of lung cancer: Global trends and association with socioeconomic status. Sci. Rep. 2017, 7, 14300. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Noguchi, M.; Nicholson, A.G.; Geisinger, K.R.; Yatabe, Y.; Beer, D.G.; Powell, C.A.; Riely, G.J.; Van Schil, P.E.; et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J. Thorac. Oncol. 2011, 6, 244–285. [Google Scholar] [CrossRef]
- Tanoue, L.T.; Detterbeck, F.C. New TNM classification for non-small-cell lung cancer. Expert Rev. Anticancer Ther. 2009, 9, 413–423. [Google Scholar] [CrossRef]
- Trajman, A.; Luiz, R.R. McNemar chi2 test revisited: Comparing sensitivity and specificity of diagnostic examinations. Scand. J. Clin. Lab. Investig. 2008, 68, 77–80. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. (Zagreb) 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Robin, X. PanelomiX for the Combination of Biomarkers. Methods Mol. Biol. 2019, 1959, 261–273. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Model | AIC | AUC | PPV | NPV | Specificity | Sensitivity |
|---|---|---|---|---|---|---|
| 6-protein combination | 30.876 | 0.999 | 0.992 | 0.989 | 0.989 | 0.992 |
| 3-protein combination | 31.402 | 0.999 | 0.984 | 0.968 | 0.978 | 0.977 |
| FLNA | 65.647 | 0.990 | 0.967 | 0.908 | 0.957 | 0.930 |
| TUBA4A | 41.556 | 0.997 | 0.984 | 0.948 | 0.978 | 0.961 |
| GSTO1 | 45.427 | 0.996 | 0.976 | 0.947 | 0.968 | 0.961 |
| PRDX6 | 51.763 | 0.993 | 0.976 | 0.957 | 0.968 | 0.969 |
| ARHGDIB | 54.303 | 0.981 | 0.992 | 0.929 | 0.989 | 0.945 |
| CDH13 | 219.090 | 0.845 | 0.791 | 0.747 | 0.699 | 0.828 |
| TFPI | 204.860 | 0.851 | 0.836 | 0.737 | 0.785 | 0.797 |
| Xpresys® XL panel | 45.592 | 0.996 | 0.969 | 0.957 | 0.957 | 0.969 |
| ALDOA | 43.946 | 0.994 | 0.969 | 0.947 | 0.957 | 0.961 |
| COL18A1 | 250.790 | 0.767 | 0.752 | 0.630 | 0.677 | 0.711 |
| FTL | 297.720 | 0.554 | 0.579 | NaN | 0.000 | 1.000 |
| LGALS3BP | 295.220 | 0.601 | 0.601 | 0.500 | 0.258 | 0.813 |
| THBS1 | 161.780 | 0.924 | 0.871 | 0.794 | 0.828 | 0.844 |
| Cancer stages | Clinically Annotated Stages | ||||||
|---|---|---|---|---|---|---|---|
| No cancer | Stage NA * | Stage I | Stage II | Stage III | Stage IV | ||
| No cancer | 92 | 1 | 1 | 0 | 1 | 0 | |
| Predicted stages | Stage NA * | 0 | 2 | 0 | 1 | 0 | 0 |
| Stage I | 0 | 2 | 9 | 1 | 2 | 6 | |
| Stage II | 0 | 0 | 0 | 0 | 0 | 1 | |
| Stage III | 0 | 0 | 0 | 1 | 0 | 0 | |
| Stage IV | 1 | 6 | 13 | 8 | 16 | 57 | |
| Sum | 93 | 11 | 23 | 11 | 19 | 64 | |
| Protein Biomarker | TA | TS |
|---|---|---|
| FLNA | >0.48091298 | >0.48091298 |
| TUBA4A | >1.6875327 | >0.18983749 |
| GSTO1 | >5.363042 | >5.363042 |
| PRDX6 | >5.9975386 | >4.038682 |
| ARHGDIB | >0.5091874 | >0.5091874 |
| CDH13 | <69.826614 | <148.1571 |
| Performance metrics | 6-Protein Panel | Xpresys® XL Panel | ||
|---|---|---|---|---|
| TA Thresholds | TS Thresholds | Logistic Regression | Logistic Regression | |
| NPV (95% CI) | 0.840 (0.709–0.928) | 0.849 (0.724–0.933) | 0.935 (0.821–0.986) | 0.930 (0.809–0.985) |
| PPV (95% CI) | 0.851 (0.717–0.938) | 0.909 (0.783–0.975) | 0.882 (0.761–0.956) | 0.833 (0.707–0.921) |
| Sensitivity (95% CI) | 0.833 (0.698–0.925) | 0.833 (0.698–0.925) | 0.938 (0.828–0.987) | 0.938 (0.828–0.987) |
| Specificity (95% CI) | 0.857 (0.728–0.941) | 0.918 (0.804–0.977) | 0.878 (0.752–0.954) | 0.816 (0.680–0.912) |
| AUC (95% CI) | 0.845 (0.773–0.918) | 0.876 (0.810–0.942) | 0.908 (0.850–0.965) | 0.877 (0.812–0.942) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Khoury, V.; Schritz, A.; Kim, S.-Y.; Lesur, A.; Sertamo, K.; Bernardin, F.; Petritis, K.; Pirrotte, P.; Selinsky, C.; Whiteaker, J.R.; et al. Identification of a Blood-Based Protein Biomarker Panel for Lung Cancer Detection. Cancers 2020, 12, 1629. https://doi.org/10.3390/cancers12061629
El-Khoury V, Schritz A, Kim S-Y, Lesur A, Sertamo K, Bernardin F, Petritis K, Pirrotte P, Selinsky C, Whiteaker JR, et al. Identification of a Blood-Based Protein Biomarker Panel for Lung Cancer Detection. Cancers. 2020; 12(6):1629. https://doi.org/10.3390/cancers12061629
Chicago/Turabian StyleEl-Khoury, Victoria, Anna Schritz, Sang-Yoon Kim, Antoine Lesur, Katriina Sertamo, François Bernardin, Konstantinos Petritis, Patrick Pirrotte, Cheryl Selinsky, Jeffrey R. Whiteaker, and et al. 2020. "Identification of a Blood-Based Protein Biomarker Panel for Lung Cancer Detection" Cancers 12, no. 6: 1629. https://doi.org/10.3390/cancers12061629
APA StyleEl-Khoury, V., Schritz, A., Kim, S.-Y., Lesur, A., Sertamo, K., Bernardin, F., Petritis, K., Pirrotte, P., Selinsky, C., Whiteaker, J. R., Zhang, H., Kennedy, J. J., Lin, C., Lee, L. W., Yan, P., Tran, N. L., Inge, L. J., Chalabi, K., Decker, G., ... Kim, Y. J. (2020). Identification of a Blood-Based Protein Biomarker Panel for Lung Cancer Detection. Cancers, 12(6), 1629. https://doi.org/10.3390/cancers12061629