HLA Class I Allele Expression and Clinical Outcome in De Novo Metastatic Prostate Cancer


Abstract
1. Introduction
2. Results
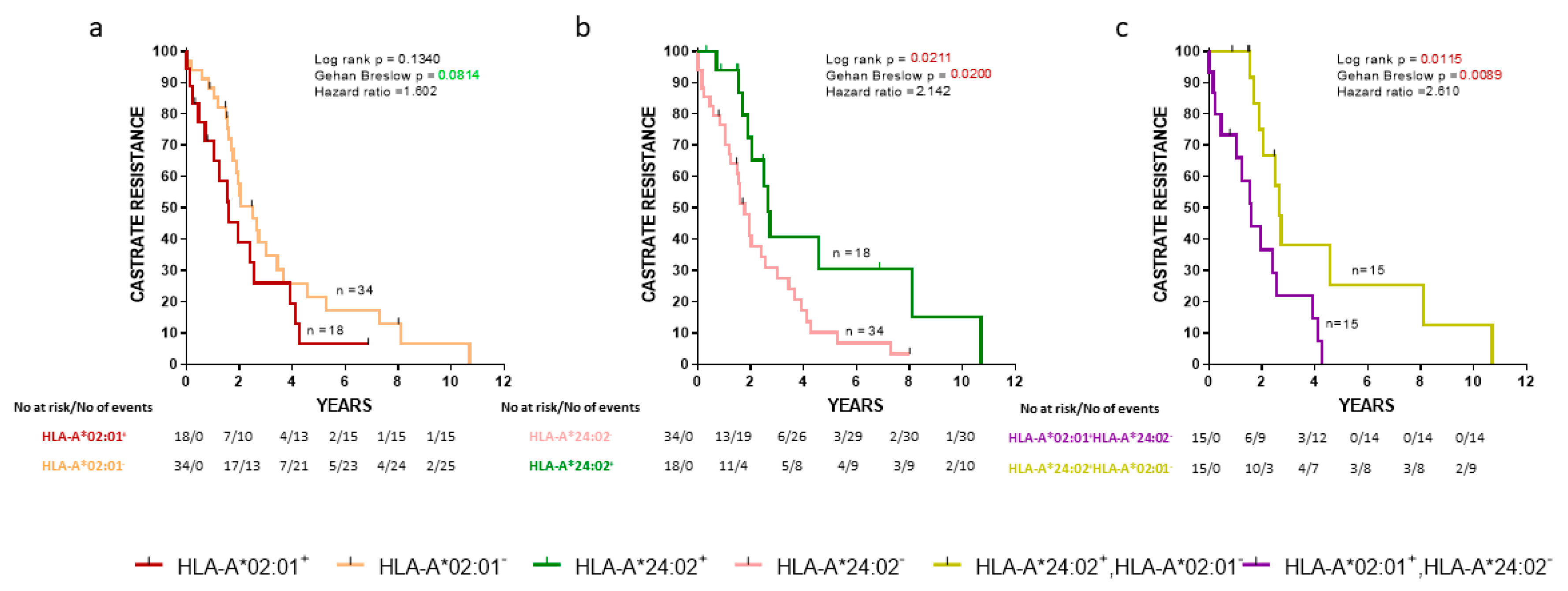
2.1. HLA-A*02:01 and HLA-A*24:02 Alleles Influence the Progression to CR in De Novo mPCa Patients
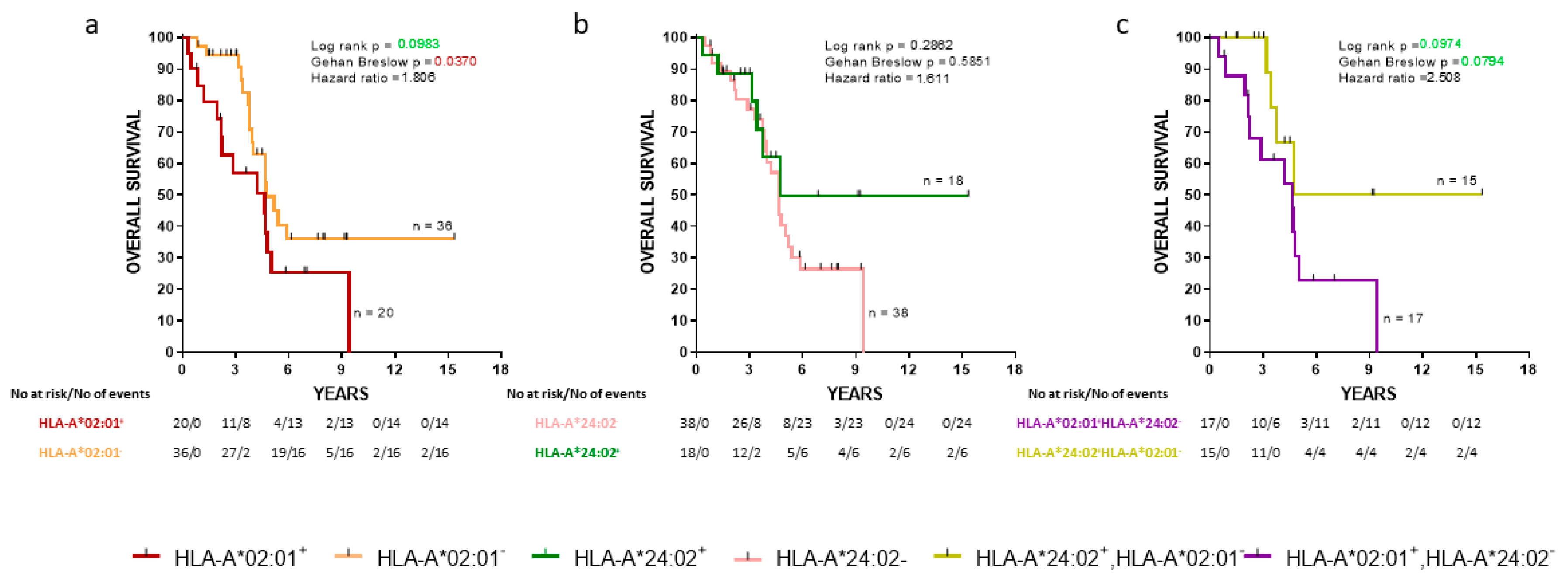
2.2. HLA-A*02:01 and HLA-A*24:02 Alleles Influence OS in De Novo mPCa Patients
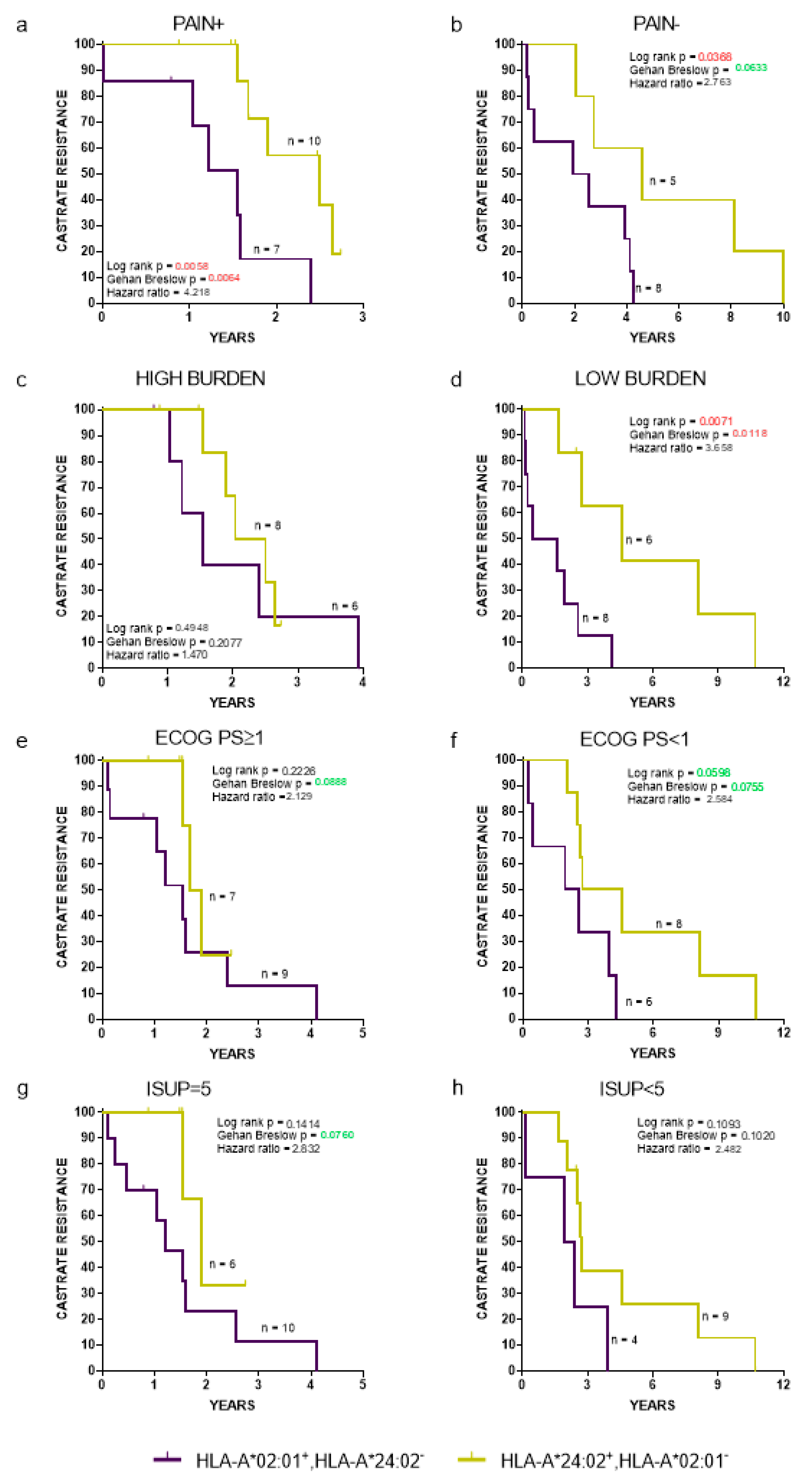
2.3. The Prognostic Value of HLA-A*02:01 and HLA-A*24:02 Alleles Is Independent of Established Prognostic Clinicopathological Factors
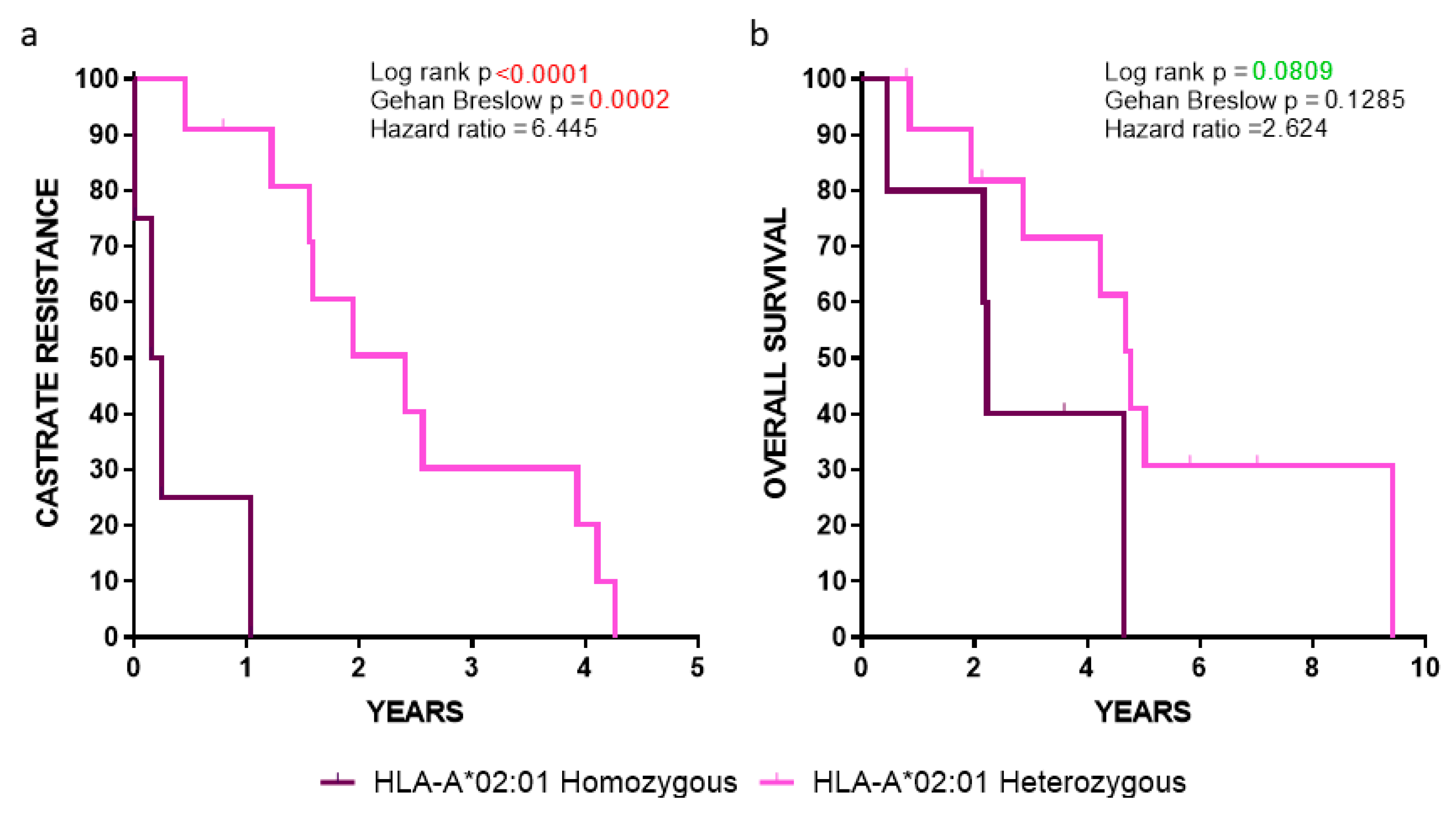
2.4. Clinical Outcomes in HLA-A*02:01 Homozygous vs. Heterozygous Patients
2.5. HLA Status as an Independent Prognostic Biomarker
3. Discussion
4. Materials and Methods
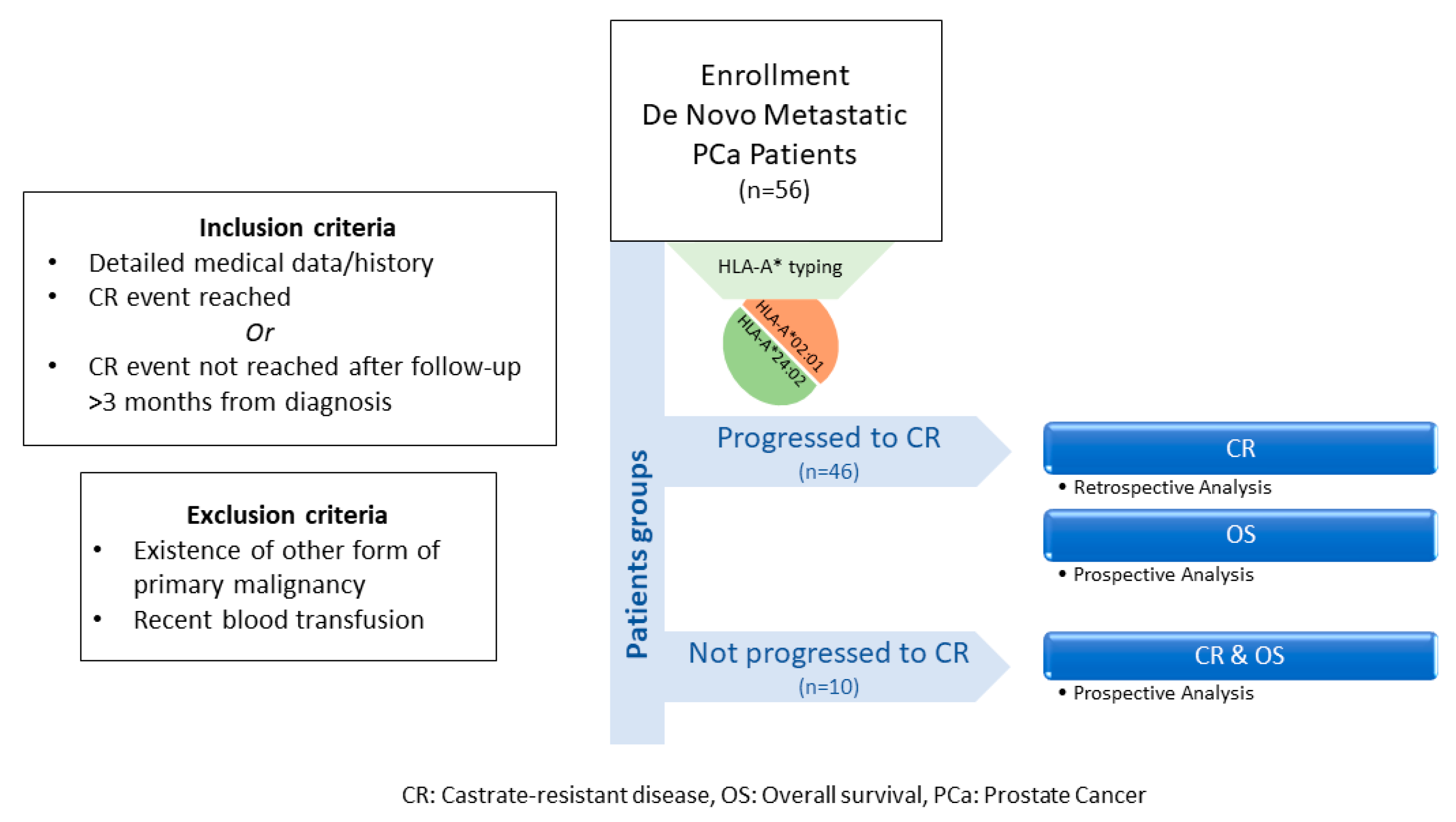
4.1. Study Population and Study Design
4.2. HLA Typing
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- The, L. GLOBOCAN 2018: Counting the toll of cancer. Lancet 2018, 392, 985. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Globocan. 2018. Available online: https://gco.iarc.fr/today/home (accessed on 3 April 2020).
- Quinn, M.; Babb, P. Patterns and trends in prostate cancer incidence, survival, prevalence and mortality. Part I: International comparisons. BJU Int. 2002, 90, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Mosillo, C.; Iacovelli, R.; Ciccarese, C.; Fantinel, E.; Bimbatti, D.; Brunelli, M.; Bisogno, I.; Kinspergher, S.; Buttigliero, C.; Tucci, M.; et al. De novo metastatic castration sensitive prostate cancer: State of art and future perspectives. Cancer Treat. Rev. 2018, 70, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Buzzoni, C.; Auvinen, A.; Roobol, M.J.; Carlsson, S.; Moss, S.M.; Puliti, D.; de Koning, H.J.; Bangma, C.H.; Denis, L.J.; Kwiatkowski, M.; et al. Metastatic Prostate Cancer Incidence and Prostate-specific Antigen Testing: New Insights from the European Randomized Study of Screening for Prostate Cancer. Eur. Urol. 2015, 68, 885–890. [Google Scholar] [CrossRef]
- James, N.D.; Spears, M.R.; Clarke, N.W.; Dearnaley, D.P.; de Bono, J.S.; Gale, J.; Hetherington, J.; Hoskin, P.J.; Jones, R.J.; Laing, R.; et al. Survival with Newly Diagnosed Metastatic Prostate Cancer in the “Docetaxel Era”: Data from 917 Patients in the Control Arm of the STAMPEDE Trial (MRC PR08, CRUK/06/019). Eur. Urol. 2015, 67, 1028–1038. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.N.; Fish, K.M.; Evans, C.P.; White, R.W.D.; Dall’Era, M.A. No improvement noted in overall or cause-specific survival for men presenting with metastatic prostate cancer over a 20-year period. Cancer 2014, 120, 818–823. [Google Scholar] [CrossRef] [PubMed]
- Helgstrand, J.T.; Roder, M.A.; Klemann, N.; Toft, B.G.; Lichtensztajn, D.Y.; Brooks, J.D.; Brasso, K.; Vainer, B.; Iversen, P. Trends in incidence and 5-year mortality in men with newly diagnosed, metastatic prostate cancer-A population-based analysis of 2 national cohorts. Cancer 2018, 124, 2931–2938. [Google Scholar] [CrossRef]
- Boyd, L.K.; Mao, X.; Lu, Y.J. The complexity of prostate cancer: Genomic alterations and heterogeneity. Nat. Rev. Urol. 2012, 9, 652–664. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Carroll, P.R.; Dall’Era, M.A.; Davies, B.J.; Davis, J.W.; Eggener, S.E.; Feng, F.Y.; Lin, D.W.; Morgan, T.M.; Morgans, A.K.; et al. The State of the Science on Prostate Cancer Biomarkers: The San Francisco Consensus Statement. Eur. Urol. 2019, 76, 268–272. [Google Scholar] [CrossRef]
- Zelic, R.; Garmo, H.; Zugna, D.; Stattin, P.; Richiardi, L.; Akre, O.; Pettersson, A. Predicting Prostate Cancer Death with Different Pretreatment Risk Stratification Tools: A Head-to-head Comparison in a Nationwide Cohort Study. Eur. Urol. 2019. [Google Scholar] [CrossRef]
- Halabi, S.; Small, E.J.; Kantoff, P.W.; Kattan, M.W.; Kaplan, E.B.; Dawson, N.A.; Levine, E.G.; Blumenstein, B.A.; Vogelzang, N.J. Prognostic model for predicting survival in men with hormone-refractory metastatic prostate cancer. J. Clin. Oncol. 2003, 21, 1232–1237. [Google Scholar] [CrossRef]
- Smaletz, O.; Scher, H.I.; Small, E.J.; Verbel, D.A.; McMillan, A.; Regan, K.; Kelly, W.K.; Kattan, M.W. Nomogram for overall survival of patients with progressive metastatic prostate cancer after castration. J. Clin. Oncol. 2002, 20, 3972–3982. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.J.; Garrett-Mayer, E.S.; Yang, Y.C.; de Wit, R.; Tannock, I.F.; Eisenberger, M. A contemporary prognostic nomogram for men with hormone-refractory metastatic prostate cancer: A TAX327 study analysis. Clin. Cancer Res. 2007, 13, 6396–6403. [Google Scholar] [CrossRef]
- Buelens, S.; Poelaert, F.; Dhondt, B.; Fonteyne, V.; de Visschere, P.; Ost, P.; Verbeke, S.; Villeirs, G.; de Man, K.; Rottey, S.; et al. Metastatic burden in newly diagnosed hormone-naive metastatic prostate cancer: Comparing definitions of CHAARTED and LATITUDE trial. Urol. Oncol. 2018, 36, 158.e13–158.e20. [Google Scholar] [CrossRef] [PubMed]
- Iacovelli, R.; Ciccarese, C.; Mosillo, C.; Bimbatti, D.; Fantinel, E.; Stefani, L.; Simbolo, M.; Romano, M.; Mazzarotto, R.; Brunelli, M.; et al. Comparison Between Prognostic Classifications in De Novo Metastatic Hormone Sensitive Prostate Cancer. Target. Oncol. 2018, 13, 649–655. [Google Scholar] [CrossRef] [PubMed]
- De Velasco, M.A.; Uemura, H. Prostate cancer immunotherapy: Where are we and where are we going? Curr. Opin. Urol. 2018, 28, 15–24. [Google Scholar] [CrossRef]
- Baxevanis, C.N.; Fortis, S.P.; Perez, S.A. Prostate cancer: Any room left for immunotherapies? Immunotherapy 2019, 11, 69–74. [Google Scholar] [CrossRef]
- Parham, P.; Ohta, T. Population biology of antigen presentation by MHC class I molecules. Science 1996, 272, 67–74. [Google Scholar] [CrossRef]
- Rivoltini, L.; Carrabba, M.; Huber, V.; Castelli, C.; Novellino, L.; Dalerba, P.; Mortarini, R.; Arancia, G.; Anichini, A.; Fais, S.; et al. Immunity to cancer: Attack and escape in T lymphocyte-tumor cell interaction. Immunol. Rev. 2002, 188, 97–113. [Google Scholar] [CrossRef]
- Dendrou, C.A.; Petersen, J.; Rossjohn, J.; Fugger, L. HLA variation and disease. Nat. Rev. Immunol. 2018, 18, 325–339. [Google Scholar] [CrossRef] [PubMed]
- De Petris, L.; Bergfeldt, K.; Hising, C.; Lundqvist, A.; Tholander, B.; Pisa, P.; van der Zanden, H.G.; Masucci, G. Correlation between HLA-A2 gene frequency, latitude, ovarian and prostate cancer mortality rates. Med. Oncol. 2004, 21, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Voutsas, I.F.; Anastasopoulou, E.A.; Tzonis, P.; Papamichail, M.; Perez, S.A.; Baxevanis, C.N. Unraveling the role of preexisting immunity in prostate cancer patients vaccinated with a HER-2/neu hybrid peptide. J. Immunother. Cancer 2016, 4, 75. [Google Scholar] [CrossRef]
- Anastasopoulou, E.A.; Voutsas, I.F.; Papamichail, M.; Baxevanis, C.N.; Perez, S.A. MHC class II tetramer analyses in AE37-vaccinated prostate cancer patients reveal vaccine-specific polyfunctional and long-lasting CD4(+) T-cells. Oncoimmunology 2016, 5, e1178439. [Google Scholar] [CrossRef]
- Papassavas, E.C.; Spyropoulou-Vlachou, M.; Papassavas, A.C.; Schipper, R.F.; Doxiadis, I.N.; Stavropoulos-Giokas, C. MHC class I and class II phenotype, gene, and haplotype frequencies in Greeks using molecular typing data. Hum. Immunol. 2000, 61, 615–623. [Google Scholar] [CrossRef]
- Koo, K.C.; Park, S.U.; Kim, K.H.; Rha, K.H.; Hong, S.J.; Yang, S.C.; Chung, B.H. Prognostic Impacts of Metastatic Site and Pain on Progression to Castrate Resistance and Mortality in Patients with Metastatic Prostate Cancer. Yonsei Med. J. 2015, 56, 1206–1212. [Google Scholar] [CrossRef]
- Boeve, L.M.S.; Hulshof, M.; Vis, A.N.; Zwinderman, A.H.; Twisk, J.W.R.; Witjes, W.P.J.; Delaere, K.P.J.; Moorselaar, R.; Verhagen, P.; van Andel, G. Effect on Survival of Androgen Deprivation Therapy Alone Compared to Androgen Deprivation Therapy Combined with Concurrent Radiation Therapy to the Prostate in Patients with Primary Bone Metastatic Prostate Cancer in a Prospective Randomised Clinical Trial: Data from the HORRAD Trial. Eur. Urol. 2019, 75, 410–418. [Google Scholar]
- Sweeney, C.J. ECOG: CHAARTED--ChemoHormonal therapy versus androgen ablation randomized trial for extensive disease in prostate cancer. Clin. Adv. Hematol. Oncol. 2006, 4, 588–590. [Google Scholar]
- Fizazi, K.; Tran, N.; Fein, L.; Matsubara, N.; Rodriguez-Antolin, A.; Alekseev, B.Y.; Ozguroglu, M.; Ye, D.; Feyerabend, S.; Protheroe, A.; et al. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N. Engl. J. Med. 2017, 377, 352–360. [Google Scholar] [CrossRef]
- Patrikidou, A.; Loriot, Y.; Eymard, J.C.; Albiges, L.; Massard, C.; Ileana, E.; di Palma, M.; Escudier, B.; Fizazi, K. Who dies from prostate cancer? Prostate Cancer Prostatic Dis. 2014, 17, 348–352. [Google Scholar] [CrossRef]
- Campoli, M.; Ferrone, S. HLA antigen changes in malignant cells: Epigenetic mechanisms and biologic significance. Oncogene 2008, 27, 5869–5885. [Google Scholar] [CrossRef] [PubMed]
- Carretero, F.J.; del Campo, A.B.; Flores-Martin, J.F.; Mendez, R.; Garcia-Lopez, C.; Cozar, J.M.; Adams, V.; Ward, S.; Cabrera, T.; Ruiz-Cabello, F.; et al. Frequent HLA class I alterations in human prostate cancer: Molecular mechanisms and clinical relevance. Cancer Immunol. Immunother. 2016, 65, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Seliger, B.; Stoehr, R.; Handke, D.; Mueller, A.; Ferrone, S.; Wullich, B.; Tannapfel, A.; Hofstaedter, F.; Hartmann, A. Association of HLA class I antigen abnormalities with disease progression and early recurrence in prostate cancer. Cancer Immunol. Immunother. 2010, 59, 529–540. [Google Scholar] [CrossRef] [PubMed]
- Seliger, B. Novel insights into the molecular mechanisms of HLA class I abnormalities. Cancer Immunol. Immunother. 2012, 61, 249–254. [Google Scholar] [CrossRef]
- Edwards, J.; Krishna, N.S.; Witton, C.J.; Bartlett, J.M. Gene amplifications associated with the development of hormone-resistant prostate cancer. Clin. Cancer Res. 2003, 9, 5271–5281. [Google Scholar]
- Norell, H.; Carlsten, M.; Ohlum, T.; Malmberg, K.J.; Masucci, G.; Schedvins, K.; Altermann, W.; Handke, D.; Atkins, D.; Seliger, B.; et al. Frequent loss of HLA-A2 expression in metastasizing ovarian carcinomas associated with genomic haplotype loss and HLA-A2-restricted HER-2/neu-specific immunity. Cancer Res. 2006, 66, 6387–6394. [Google Scholar] [CrossRef]
- Wang, Z.; Marincola, F.M.; Rivoltini, L.; Parmiani, G.; Ferrone, S. Selective histocompatibility leukocyte antigen (HLA)-A2 loss caused by aberrant pre-mRNA splicing in 624MEL28 melanoma cells. J. Exp. Med. 1999, 190, 205–215. [Google Scholar] [CrossRef]
- Serrano, A.; Brady, C.S.; Jimenez, P.; Duggan-Keen, M.F.; Mendez, R.; Stern, P.; Garrido, F.; Ruiz-Cabello, F. A mutation determining the loss of HLA-A2 antigen expression in a cervical carcinoma reveals novel splicing of human MHC class I classical transcripts in both tumoral and normal cells. Immunogenetics 2000, 51, 1047–1052. [Google Scholar] [CrossRef]
- Brady, C.S.; Bartholomew, J.S.; Burt, D.J.; Duggan-Keen, M.F.; Glenville, S.; Telford, N.; Little, A.M.; Davidson, J.A.; Jimenez, P.; Ruiz-Cabello, F.; et al. Multiple mechanisms underlie HLA dysregulation in cervical cancer. Tissue Antigens 2000, 55, 401–411. [Google Scholar] [CrossRef]
- Shukla, S.A.; Rooney, M.S.; Rajasagi, M.; Tiao, G.; Dixon, P.M.; Lawrence, M.S.; Stevens, J.; Lane, W.J.; Dellagatta, J.L.; Steelman, S.; et al. Comprehensive analysis of cancer-associated somatic mutations in class I HLA genes. Nat. Biotechnol. 2015, 33, 1152–1158. [Google Scholar] [CrossRef]
- Hayashi, S.; Moriyama, T.; Yamaguchi, R.; Mizuno, S.; Komura, M.; Miyano, S.; Nakagawa, H.; Imoto, S. ALPHLARD-NT: Bayesian Method for Human Leukocyte Antigen Genotyping and Mutation Calling through Simultaneous Analysis of Normal and Tumor Whole-Genome Sequence Data. J. Comput. Biol. 2019, 26, 923–937. [Google Scholar] [CrossRef] [PubMed]
- Balachandran, V.P.; Gonen, M.; Smith, J.J.; DeMatteo, R.P. Nomograms in oncology: More than meets the eye. Lancet Oncol. 2015, 16, e173–e180. [Google Scholar] [CrossRef]
- Bandini, M.; Fossati, N.; Briganti, A. Nomograms in urologic oncology, advantages and disadvantages. Curr. Opin. Urol. 2019, 29, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Sun, G.; Liao, B.; Zhang, X.; Armstrong, C.M.; Yin, X.; Liu, J.; Chen, J.; Yang, Y.; Zhao, P.; et al. Novel nomograms for castration-resistant prostate cancer and survival outcome in patients with de novo bone metastatic prostate cancer. BJU Int. 2018, 122, 994–1002. [Google Scholar] [CrossRef]
- Iacovelli, R.; Ciccarese, C.; Schinzari, G.; Maiorano, B.A.; Rossi, E.; Pierconti, F.; Bassi, P.F.; Bria, E.; Tortora, G. Going towards a precise definition of the therapeutic management of de-novo metastatic castration sensitive prostate cancer patients: How prognostic classification impact treatment decisions. Crit. Rev. Oncol. Hematol. 2019, 139, 83–86. [Google Scholar] [CrossRef]
- Miyake, H.; Matsushita, Y.; Watanabe, H.; Tamura, K.; Motoyama, D.; Ito, T.; Sugiyama, T.; Otsuka, A. Prognostic Significance of Time to Castration Resistance in Patients with Metastatic Castration-sensitive Prostate Cancer. Anticancer Res. 2019, 39, 1391–1396. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Univariate | CR | OS | ||||
| p | Hazard Ratio | 95.0% CI for Exp(B) (Range) | p | Hazard Ratio | 95.0% CI for Exp(B) (Range) | |
| Age | 0.978 | 0.992 | 0.573–1.719 | 0.701 | 0.888 | 0.483–1.630 |
| PSA | 0.495 | 1.000 | 0.999–1.001 | 0.798 | 1.000 | 0.999–1.001 |
| ISUP Grade group | 0.181 | 1.215 | 0.913–1.6177 | 0.034 | 1.507 | 1.032–2.200 |
| PCa burden | 0.258 | 1.393 | 0.784–2.473 | 0.822 | 1.077 | 0.565–2.052 |
| Metastases | 0.955 | 1.011 | 0.690–1.481 | 0.777 | 0.940 | 0.615–1.438 |
| Pain | 0.005 | 2.333 | 1.286–4.232 | 0.000 | 3.937 | 1.964–7.893 |
| ECOG PS | 0.003 | 2.433 | 1.346–4.397 | 0.003 | 2.745 | 1.418–5.314 |
| HLA-A allele | 0.007 | 1.675 | 1.150–2.438 | 0.065 | 1.521 | 0.975–2.372 |
| Multivariate | CR | OS | ||||
| p | Hazard Ratio | 95.0% CI for Exp(B) (Range) | p | Hazard Ratio | 95.0% CI for Exp(B) (Range) | |
| Model before Stepwise Selection | ||||||
| Age | 0.651 | 1.181 | 0.574–2.431 | 0.347 | 1.440 | 0.673–3.079 |
| PSA | 0.914 | 1.000 | 0.999–1.001 | 0.404 | 1.001 | 0.999–1.002 |
| ISUP Grade group | 0.351 | 1.140 | 0.865–1.501 | 0.103 | 1.332 | 0.943–1.882 |
| PCa burden | 0.944 | 0.967 | 0.374–2.499 | 0.986 | 1.008 | 0.423–2.399 |
| Metastases | 0.654 | 1.124 | 0.674–1.875 | 0.910 | 1.033 | 0.586–1.823 |
| Pain | 0.140 | 2.333 | 0.757–7.190 | 0.006 | 1.889 | 1.544–13.399 |
| ECOG PS | 0.978 | 1.012 | 0.428–2.395 | 0.597 | 0.777 | 0.298–2.007 |
| HLA-A allele | 0.008 | 2.029 | 1.205–3.414 | 0.051 | 2.035 | 0.998–4.150 |
| Model after Stepwise Selection | ||||||
| HLA-A allele | 0.001 | 2.052 | 1.355–3.108 | 0.016 | 1.889 | 1.126–3.169 |
| Pain | 0.013 | 2.222 | 1.181–4.179 | 0.002 | 3.116 | 1.512–6.424 |
| PCa Patients with de novo metastatic disease | |
| Characteristic (Initial PCa Staging) | No. (%) of PCa (N = 56) |
| Median age at diagnosis (years) (range) | 70.14 (49–88%) |
| PSA (median 75.9 ng/mL; range 2.38–6806) | |
| ≤100 | 30 (53.6%) |
| >100 | 23 (41.1%) |
| Missing | 3 (5.4%) |
| Gleason Score | |
| ≤7 | 10 (17.9%) |
| 8 | 14 (25%) |
| ≥9 | 27 (48.2%) |
| Missing | 5 (8.9%) |
| ISUP Grade group | |
| 1 | 2 (3.6%) |
| 2 | 2 (3.6%) |
| 3 | 6 (10.7%) |
| 4 | 14 (25%) |
| 5 | 27 (48.2%) |
| Missing | 5 (8.9%) |
| Nodal Status a | |
| Positive | 29 (51.9%) |
| Negative | 24 (42.9%) |
| Missing | 3 (5.4%) |
| Bone Metastasis b | |
| Positive | 46 (82.1%) |
| Negative | 7 (12.5%) |
| Missing | 3 (5.4%) |
| High-Volume PCa (visceral metastases and/or 4 or more bone metastases) | |
| Positive | 28 (50%) |
| Negative | 25 (44.6%) |
| Missing | 3 (5%) |
| ECOG PS | |
| 0 | 31 (55.4%) |
| ≥1 | 25 (44.6%) |
| PAIN | |
| Present | 33 (58.9%) |
| Absent | 23 (41.1%) |
| Ethnicity | |
| Caucasian | 54 (96.4%) |
| African American | 1 (1.8%) |
| Asian | 1 (1.8%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stokidis, S.; Fortis, S.P.; Kogionou, P.; Anagnostou, T.; Perez, S.A.; Baxevanis, C.N. HLA Class I Allele Expression and Clinical Outcome in De Novo Metastatic Prostate Cancer. Cancers 2020, 12, 1623. https://doi.org/10.3390/cancers12061623
Stokidis S, Fortis SP, Kogionou P, Anagnostou T, Perez SA, Baxevanis CN. HLA Class I Allele Expression and Clinical Outcome in De Novo Metastatic Prostate Cancer. Cancers. 2020; 12(6):1623. https://doi.org/10.3390/cancers12061623
Chicago/Turabian StyleStokidis, Savvas, Sotirios P. Fortis, Paraskevi Kogionou, Theodoros Anagnostou, Sonia A. Perez, and Constantin N. Baxevanis. 2020. "HLA Class I Allele Expression and Clinical Outcome in De Novo Metastatic Prostate Cancer" Cancers 12, no. 6: 1623. https://doi.org/10.3390/cancers12061623
APA StyleStokidis, S., Fortis, S. P., Kogionou, P., Anagnostou, T., Perez, S. A., & Baxevanis, C. N. (2020). HLA Class I Allele Expression and Clinical Outcome in De Novo Metastatic Prostate Cancer. Cancers, 12(6), 1623. https://doi.org/10.3390/cancers12061623