Should the Number of Metastatic Pelvic Lymph Nodes Be Integrated into the 2018 Figo Staging Classification of Early Stage Cervical Cancer?



 ,
,
Abstract
1. Introduction
2. Materials and Methods
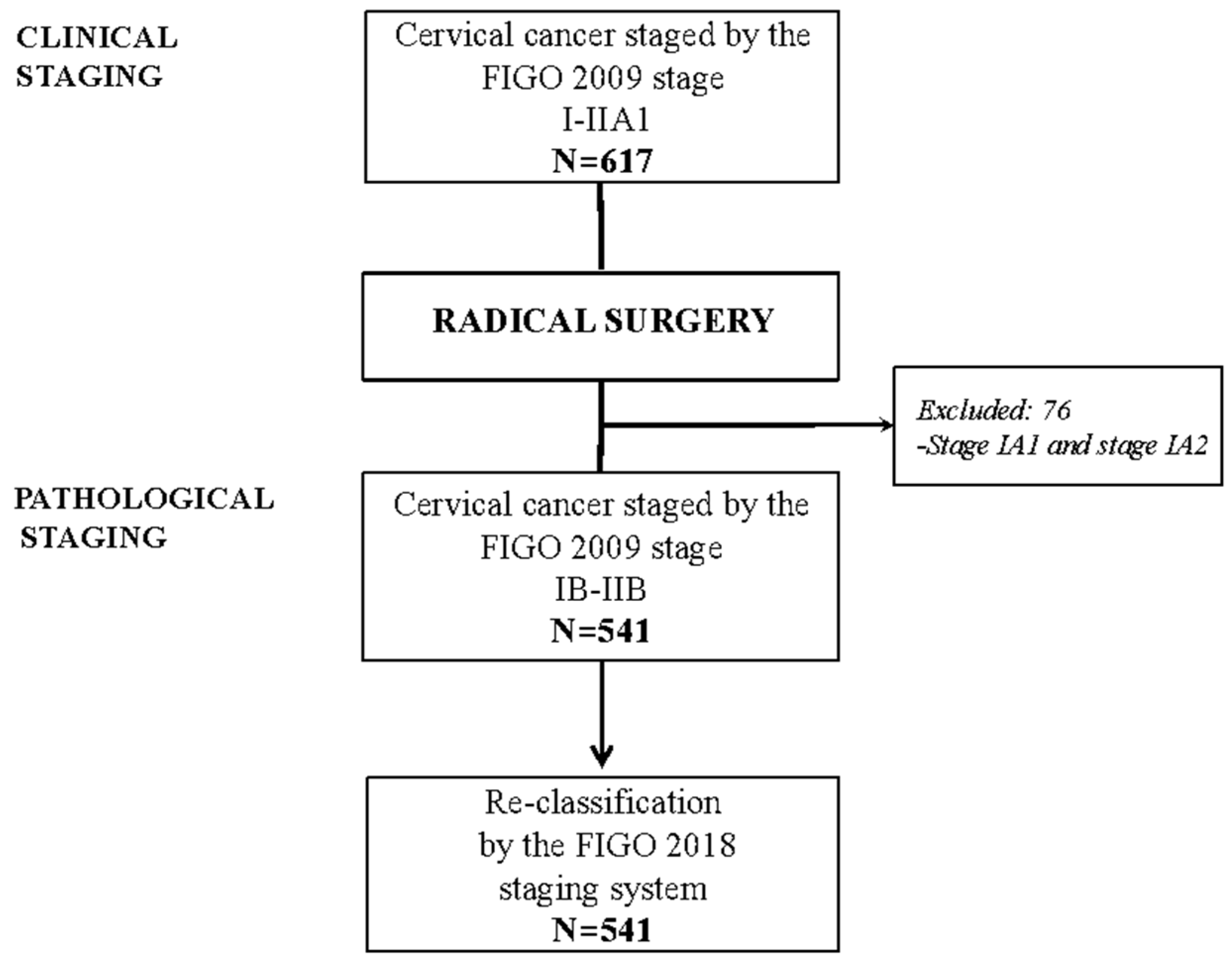
2.1. Study Design and Inclusion Criteria
2.2. Statistical Analysis
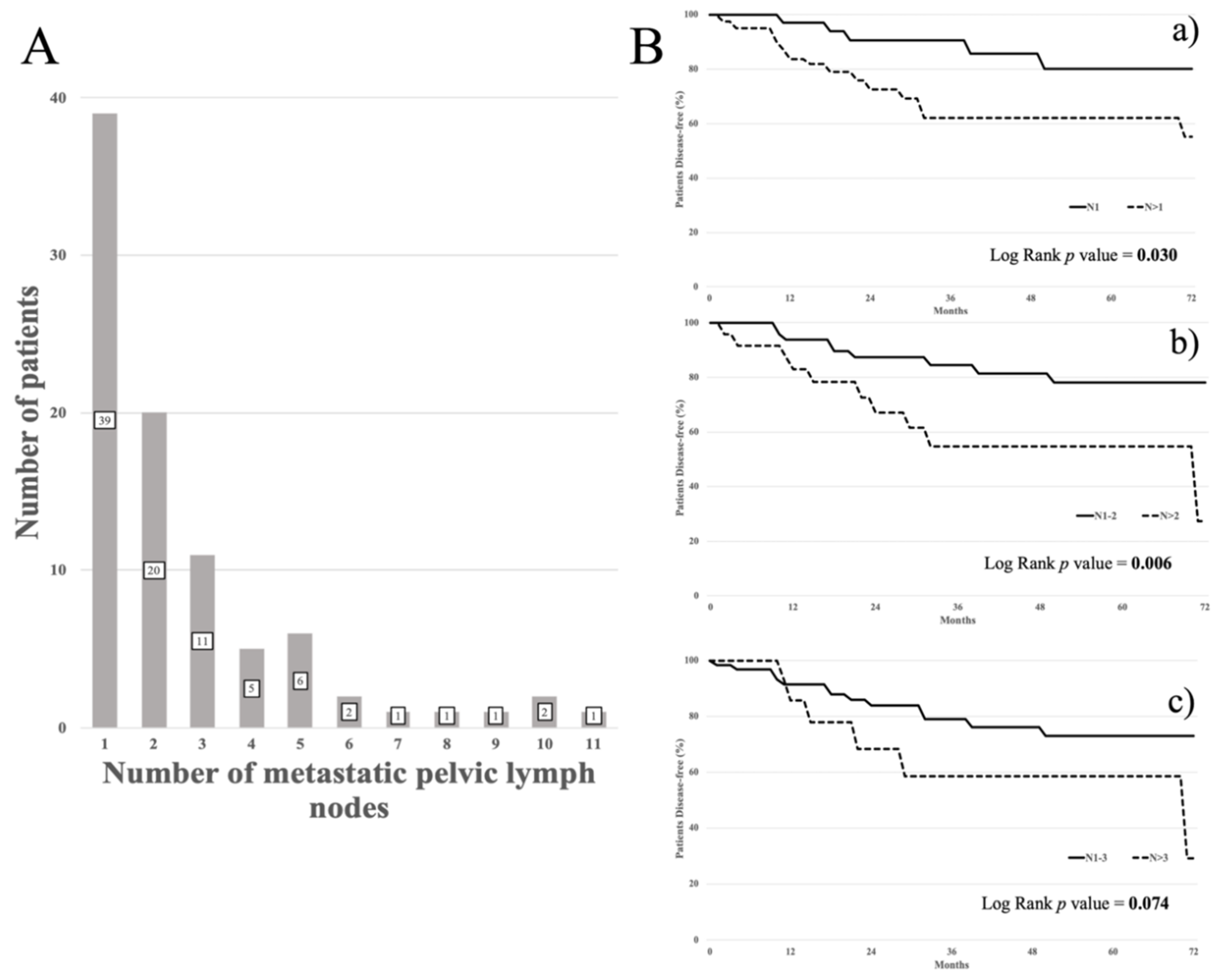
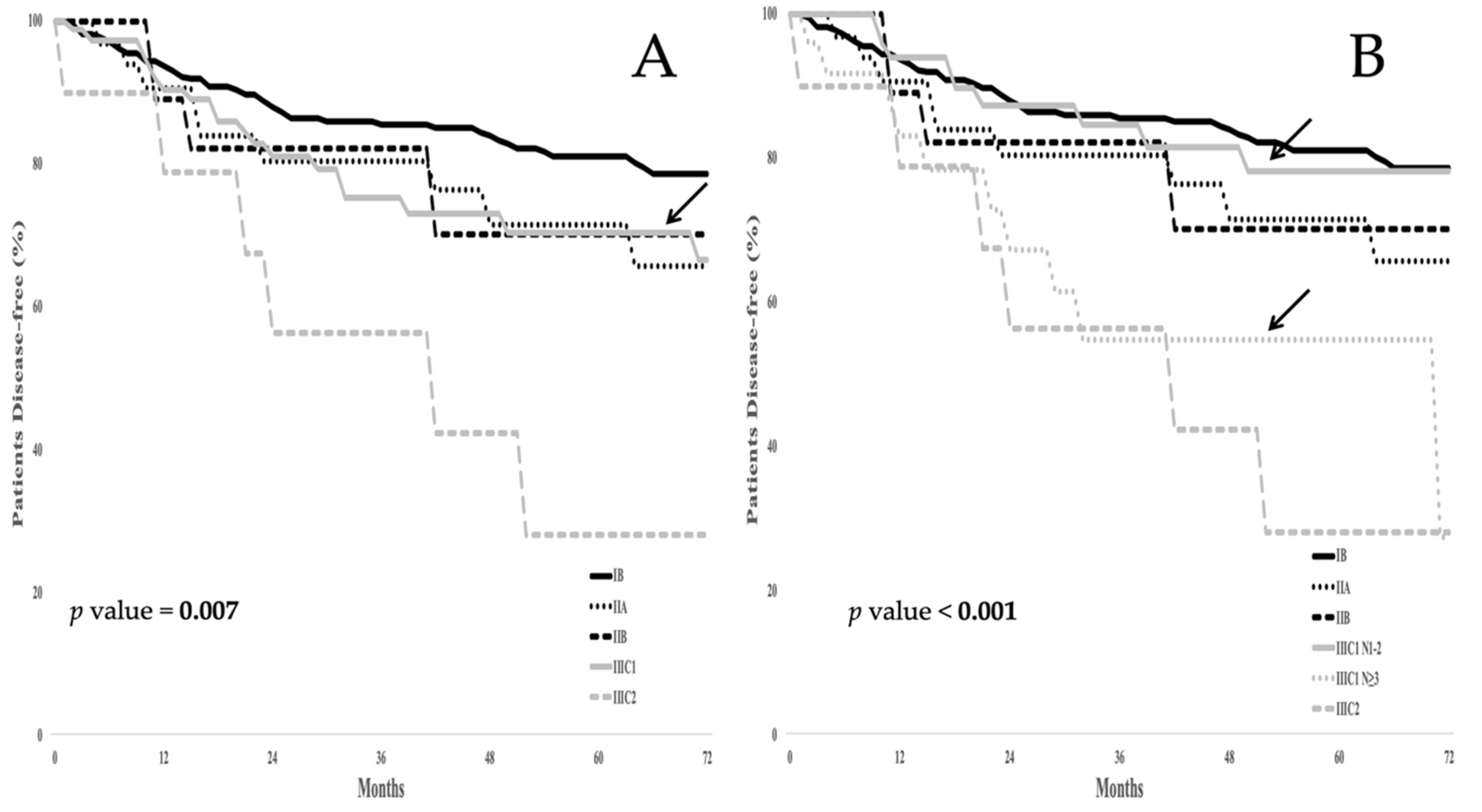
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Delgado, G.; Bundy, B.; Zaino, R.; Sevin, B.U.; Creasman, W.T.; Major, F. Prospective surgical-pathologic study of disease-free interval in patients with stage IB squamous cell carcinoma of the cervix: A Gynecologic Oncology Group study. Gynecol. Oncol. 1990, 38, 352–357. [Google Scholar] [CrossRef]
- Sakuragi, N. Up-to-date management of lymph node metastasis and the role of tailored lymphadenectomy in cervical cancer. Int. J. Clin. Oncol. 2007, 12, 165–175. [Google Scholar] [CrossRef]
- Bhatla, N.; Berek, J.S.; Cuello Fredes, M.; Denny, L.; Grenman, S.; Karunaratne, K.; Hehoe, S.T.; Konishi, I.; Olawaiye, A.B.; Prat, J.; et al. Revised FIGO staging for carcinoma of the cervix uteri. Int. J. Gynaecol. Obstet. 2019, 145, 129–135. [Google Scholar] [CrossRef]
- Yan, D.D.; Tang, Q.; Chen, J.H.; Tu, Y.Q.; Lv, X.J. Prognostic value of the 2018 FIGO staging system for cervical cancer patients with surgical risk factors. Cancer Manag. Res. 2019, 11, 5473–5480. [Google Scholar] [CrossRef]
- Matsuo, K.; Machida, H.; Mandelbaum, R.S.; Konishi, I.; Mikami, M. Validation of the 2018 FIGO cervical cancer staging system. Gynecol. Oncol. 2019, 152, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.X.; Fang, F. Progress in the study of lymph node metastasis in early-stage cervical cancer. Curr. Med. Sci. 2018, 38, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Ferrandina, G.; Pedone Anchora, L.; Gallotta, V.; Fagotti, A.; Vizza, E.; Chiantera, V.; De Iaco, P.; Ercoli, A.; Corrado, G.; Bottoni, C.; et al. Can we define the risk of lymph node metastasis in early stage cervical cancer patients? A large-scale, retrospective study. Ann. Surg. Oncol. 2017, 24, 2311–2318. [Google Scholar] [CrossRef]
- Fagotti, A.; Pedone Anchora, L.; Conte, C.; Chiantera, V.; Vizza, E.; Tortorella, L.; Surico, D.; De Iaco, P.; Corrado, G.; Fanfani, F.; et al. Beyond sentinel node algorithm. Toward a more tailored surgery for cervical cancer patients. Cancer Med. 2016, 5, 1725–1730. [Google Scholar] [CrossRef]
- Liu, Y.; Zhao, L.J.; Li, M.Z.; Li, M.X.; Wang, J.L.; Wei, L.H. The Number of Positive Pelvic Lymph Nodes and Multiple Groups of Pelvic Lymph Node Metastasis Influence Prognosis in Stage IA-IIB Cervical Squamous Cell Carcinoma. Chin. Med. J. (Engl.) 2015, 128, 2084–2089. [Google Scholar] [CrossRef]
- Park, J.Y.; Kim, D.J.; Kim, J.H.; Kim, Y.M.; Kim, Y.T.; Nam, J.H. Further stratification of risk groups in patients with lymph node metastasis after radical hysterectomy for early-stage cervical cancer. Gynecol. Oncol. 2010, 117, 53–58. [Google Scholar] [CrossRef]
- Park, J.W.; Bae, J.W. Prognostic significance of positive lymph node number in early cervical cancer. Mol. Clin. Oncol. 2016, 4, 1052–1056. [Google Scholar] [CrossRef]
- Zhou, J.; Wu, S.G.; Sun, J.Y.; Liao, X.L.; Li, F.Y.; Lin, H.X.; Yang, L.C.; He, Z.Y. Incorporation of the number of positive lymph nodes leads to better prognostic discrimination of node-positive early stage cervical cancer. Oncotarget 2017, 8, 26057–26065. [Google Scholar] [CrossRef]
- Kwon, J.; Eom, K.J.; Kim, Y.S.; Park, W.; Chun, M.; Lee, J.; Kim, Y.B.; Yoon, W.S.; Kim, J.H.; Choi, J.H.; et al. system for recurrence in early-stage cervical cancer with high risk factors: A multicenter cohort study (KROG 15-04). Cancer Res. Treat. 2018, 50, 964–974. [Google Scholar] [CrossRef] [PubMed]
- Polterauer, S.; Hefler, L.; Seebacher, V.; Rahhal, J.; Tempfer, C.; Horvat, R.; Reinthaller, A.; Grimm, C. The impact of lymph node density on survival of cervical cancer patients. Br. J. Cancer 2010, 103, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Joo, J.H.; Kim, Y.S.; Nam, J.H. Prognostic significance of lymph node ratio in node-positive cervical cancer patients. Medicine (Baltimore) 2018, 97, e11711. [Google Scholar] [CrossRef] [PubMed]
- Fleming, N.D.; Frumovitz, M.; Schmeler, K.M.; dos Reis, R.; Munsell, M.F.; Eifel, P.J.; Soliman, P.T.; Nick, A.M.; Westin, S.N.; Ramirez, P.T. Significance of lymph node ratio in defining risk category in node positive early stage cervical cancer. Gynecol. Oncol. 2015, 136, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Aslan, K.; Meydanli, M.M.; Oz, M.; Tohma, Y.A.; Haberal, A.; Ayhan, A. The prognostic value of lymph node ratio in stage IIIC cervical cancer patients triaged to primary treatment by radical hysterectomy with systematic pelvic and para-aortic lymphadenectomy. J Gynecol Oncol. 2020, 31, e1. [Google Scholar] [CrossRef]
- Guo, Q.; Zhu, J.; Wu, Y.; Wen, H.; Xia, L.; Ju, X.; Ke, G.; Wu, X. Validation of the prognostic value of various lymph node staging systems for cervical squamous cell carcinoma following radical surgery: A single-center analysis of 3,732 patients. Ann. Transl. Med. 2020, 8, 485. [Google Scholar] [CrossRef]
- Liu, Y.P.; Ma, L.; Wang, S.J.; Chen, Y.N.; Wu, G.X.; Han, M.; Wang, X.L. Prognostic value of lymph node metastases and lymph node ratio in esophageal squamous cell carcinoma. Eur. J. Surg. Oncol. 2009, 36, 155–159. [Google Scholar] [CrossRef]
- Hong, K.D.; Lee, S.I.; Moon, H.Y. Lymph node ratio as determined by the 7th edition of the AJCC staging system predicts survival in stage III colon cancer. J. Surg. Oncol. 2011, 103, 406–410. [Google Scholar] [CrossRef]
- Hwang, J.E.; Kim, H.; Shim, H.J.; Bae, W.K.; Hwang, E.C.; Jeong, O.; Ryu, S.Y.; Park, Y.K.; Cho, S.H.; Chung, I.J. Lymph-node ratio is an important clinical determinant for selecting the appropriate adjuvant chemotherapy regimen for curative D2-resected gastric cancer. J. Cancer Res. Clin. Oncol. 2019, 145, 2157–2166. [Google Scholar] [CrossRef]
- Pedone Anchora, L.; Turco, L.C.; Bizzarri, N.; Capozzi, V.A.; Lombisani, A.; Chiantera, V.; De Felice, F.; Gallotta, V.; Cosentino, F.; Fagotti, A.; et al. How to Select Early-Stage Cervical Cancer Patients Still Suitable for Laparoscopic Radical Hysterectomy: A Propensity-Matched Study. Ann. Surg. Oncol. 2020, 27, 1947–1955. [Google Scholar] [CrossRef] [PubMed]
- Corrado, G.; Vizza, E.; Legge, F.; Pedone Anchora, L.; Sperduti, I.; Fagotti, A.; Mancini, E.; Gallotta, V.; Zampa, A.; Chiofalo, B.; et al. Comparison of Different Surgical Approaches for Stage IB1 Cervical Cancer Patients: A Multi-institution Study and a Review of the Literature. Int. J. Gynecol. Cancer 2018, 28, 1020–1028. [Google Scholar] [CrossRef]
- Gallotta, V.; Conte, C.; Federico, A.; Vizzielli, G.; Gueli Alletti, S.; Tortorella, L.; Pedone Anchora, L.; Cosentino, F.; Chiantera, V.; Fagotti, A.; et al. Robotic versus laparoscopic radical hysterectomy in early cervical cancer: A case matched control study. Eur. J. Surg. Oncol. 2018, 44, 754–759, Epub 13 Feburary 2018; PubMed. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E.L.; Meier, P. Nonparametric estimation from incomplete samples. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Mantel, N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother. Rep. 1966, 50, 163–170. [Google Scholar]
- Cox, D.R. Models and life-tables regression. J. R Stat. Soc. Ser. B (Methodol.) 1972, 34, 187–220. [Google Scholar] [CrossRef]
- Hosaka, M.; Watari, H.; Mitamura, T.; Konno, Y.; Odagiri, T.; Kato, T.; Takeda, M.; Sakuragi, N. Survival and prognosticators of node-positive cervical cancer patients treated with radical hysterectomy and systematic lymphadenectomy. Int. J. Clin. Oncol. 2011, 16, 33–38. [Google Scholar] [CrossRef]
- Okazawa, M.; Mabuchi, S.; Isohashi, F.; Suzuki, O.; Ohta, Y.; Fujita, M.; Yoshino, K.; Enomoto, T.; Kamiura, S.; Kimura, T. The prognostic significance of multiple pelvic node metastases in cervical cancer patients treated with radical hysterectomy plus adjuvant chemoradiotherapy. Int. J. Gynecol. Cancer 2012, 22, 490–497. [Google Scholar] [CrossRef]
- McComas, K.N.; Torgeson, A.M.; Ager, B.J.; Hellekson, C.; Burt, L.M.; Maurer, K.A.; Werner, T.L.; Gaffney, D.K. The variable impact of positive lymph nodes in cervical cancer: Implications of the new FIGO staging system. Gynecol. Oncol. 2020, 156, 85–92. [Google Scholar] [CrossRef]
- Quinn, M.A.; Benedet, J.L.; Odicino, F.; Maisonneuve, P.; Beller, U.; Creasman, W.T.; Heintz, A.P.M.; Ngan, H.Y.S.; Pecorelli, S. Carcinoma of the cervix uteri. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int. J. Gynaecol. Obstet. 2006, 95 (Suppl. 1), S43–S103. [Google Scholar] [CrossRef]
- Boussios, S.; Seraj, E.; Zarkavelis, G.; Petrakis, D.; Kollas, A.; Kafantari, A.; Assi, A.; Tatsi, K.; Pavlidis, N.; Pentheroudakis, G. Management of patients with recurrent/advanced cervical cancer beyond first line platinum regimens: Where do we stand? A literature review. Crit. Rev. Oncol. Hematol. 2016, 108, 164–174. [Google Scholar] [CrossRef]
- Dornhöfer, N.; Höckel, M. New developments in the surgical therapy of cervical carcinoma. Ann. N. Y. Acad. Sci. 2008, 1138, 233–252. [Google Scholar] [CrossRef]
- Gadducci, A.; Tana, R.; Cosio, S.; Cionini, L. Treatment options in recurrent cervical cancer (Review). Oncol. Lett. 2010, 1, 3–11. [Google Scholar] [CrossRef]
- Vizzielli, G.; Chiantera, V.; Tinelli, G.; Fagotti, A.; Gallotta, V.; Di Giorgio, A.; Gueli Alletti, S.; Scambia, G. Out-of-the-box pelvic surgery including iliopsoas resection for recurrent gynecological malignancies: Does that make sense? A single-institution case-series. Eur. J. Surg. Oncol. 2017, 43, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Nagao, S.; Shibutani, T.; Yamamoto, K.; Jimi, T.; Yano, H.; Kitai, M.; Shiozaki, T.; Matsuoka, K.; Yamaguchi, S. Phase II trial of paclitaxel, carboplatin, and bevacizumab for advanced or recurrent cervical cancer. Gynecol. Oncol. 2019, 154, 554–557. [Google Scholar] [CrossRef]
- Sniadecki, M.; Swierzko, A.; Dabkowski, M.; Orlowska-Volk, M.; Wycinka, E.; Klasa-Mazurkiewicz, D.; Milewska, A.; Poniewierza, P.; Liro, M.; Wydra, D. New therapeutic approaches in the treatment of node-positive cervical cancer patients based on molecular targets: A systematic review. Ginekol. Pol. 2019, 90, 336–345. [Google Scholar] [CrossRef]
- Yan, D.D.; Tang, Q.; Tu, Y.Q.; Chen, J.H.; Lv, X.J. A comprehensive analysis of the factors of positive pelvic lymph nodes on survival of cervical cancer patients with 2018 FIGO stage IIIC1p. Cancer Manag. Res. 2019, 11, 4223–4230. [Google Scholar] [CrossRef]
- Takekuma, M.; Kasamatsu, Y.; Kado, N.; Kuji, S.; Tanaka, A.; Takahashi, N.; Abe, M.; Hirashima, Y. Adjuvant chemotherapy versus concurrent chemoradiotherapy for high-risk cervical cancer after radical hysterectomy and systematic lymphadenectomy. Int. J. Clin. Oncol. 2016, 21, 741–747. [Google Scholar] [CrossRef]
- Matsuo, K.; Shimada, M.; Aoki, Y.; Sakamoto, M.; Takeshima, N.; Fujiwara, H.; Matsumoto, T.; Mikami, M.; Sugiyama, T. Comparison of adjuvant therapy for node-positive clinical stage IB-IIB cervical cancer: Systemic chemotherapy versus pelvic irradiation. Int. J. Cancer 2017, 141, 1042–1051. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.B.; Shim, S.H.; Lee, J.M. Comparison between adjuvant chemotherapy and adjuvant radiotherapy/chemoradiotherapy after radical surgery in patients with cervical cancer: A meta-analysis. J. Gynecol. Oncol. 2018, 29, e62. [Google Scholar] [CrossRef] [PubMed]
- Manders, D.B.; Sims, T.T.; Bailey, A.; Hwang, L.; Richardson, D.L.; Miller, D.S.; Kehoe, S.M.; Albuquerque, K.V.; Lea, J.S. The significance of para-aortic nodal size and the role of adjuvant systemic chemotherapy in cervical cancer: An institutional experience. Am. J. Clin. Oncol. 2018, 41, 1225–1230. [Google Scholar] [CrossRef]
- Zhong, M.L.; Wang, Y.N.; Liang, M.R.; Liu, H.; Zeng, S.Y. Consolidation chemotherapy in early-stage cervical cancer patients with lymph node metastasis after radical hysterectomy. Int. J. Gynecol. Cancer 2020, 30, 602–606. [Google Scholar] [CrossRef]
- Kim, H.; Cho, W.K.; Kim, Y.J.; Kim, Y.S.; Park, W. Significance of the number of high-risk factors in patients with cervical cancer treated with radical hysterectomy and concurrent chemoradiotherapy. Gynecol. Oncol. 2020, 157, 423–428. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients n. (%) |
|---|---|
| Patients | 541 |
| Age, yrs median (range) | 46 (19–85) |
| Histology | |
| Squamous | 345 (63.8) |
| Other | 196 (36.2) |
| Grading | |
| G1/G2 | 305 (56.3) |
| G3 | 236 (43.6) |
| Tumor Size | |
| ≤2 cm | 225 (41.6) |
| >2 cm ≤4 cm | 266 (49.2) |
| >4 cm | 50 (9.2) |
| LVSI * | |
| No | 297 (54.9) |
| Yes | 244 (45.1) |
| Involvement of the upper third of vagina | |
| No | 482 (89.1) |
| Yes | 59 (10.9) |
| Parametrial involvement | |
| No | 499 (92.2) |
| Yes | 42 (7.8) |
| Radicality of surgery | |
| Type A | 52 (9.6) |
| Type B | 226 (41.8) |
| Type C | 263 (48.6) |
| Surgical approach | |
| Open | 258 (47.7) |
| Laparoscopy | 201 (37.2) |
| Robotic | 82 (15.2) |
| Lymphadenectomy | |
| Pelvic | 425 (78.6) |
| Pelvic and aortic | 116 (21.4) |
| n. of pelvic lymph nodes removed, median (range) | 27 (7–92) |
| n. of aortic lymph nodes removed, median (range) | 11 (2–38) |
| Adjuvant treatment | |
| No | 249 (46.0) |
| Radiotherapy | 137 (25.3) |
| Chemotherapy | 22 (4.1) |
| Concomitant chemoradiotherapy | 133 (24.6) |
| FIGO Staging Systems | Pathological FIGO Stage 2018 n. (%) | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| IB1 | IB2 | IB3 | IIA1 | IIA2 | IIB | IIIC1 | IIIC2 | |||
| Pathological FIGO stage 2009 n. (%) | IB1 | 209 (50.0) | 148 (35.4) | 0 | 0 | 0 | 0 | 54 (12.9) | 7 (1.7) |
418 (100) |
| IB2 | 0 | 0 | 22 (73.3) | 0 | 0 | 0 | 6 (20.0) | 2 (6.7) |
30 (100) | |
| IIA1 | 0 | 0 | 0 | 30 (71.4) | 0 | 0 | 11 (26.2) | 1 (2.4) |
42 (100) | |
| IIA2 | 0 | 0 | 0 | 0 | 8 (88.9) | 0 | 1 (11.1) | 0 |
9 (100) | |
| IIB | 0 | 0 | 0 | 0 | 0 | 22 (52.4) | 17 (40.5) | 3 (7.1) |
42 (100) | |
| Total | 209 (38.6) | 148 (27.4) | 22 (4.1) | 30 (5.5) | 8 (1.5) | 22 (4.1) | 89 (16.5) | 13 (2.4) |
541 (100) | |
| Analyses of Each Variable of the Models and of the Whole Models | Current FIGO 2018 | Revisited FIGO 2018 | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||||||
| Patients n. (%) | β | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | ||
| Variables of the model | Tumor size | |||||||
| <2 cm | 223 (42.2) | |||||||
| 2–4 cm | 257 (48.7) | 0.718 | 2.00 (1.20–3.33) | 2.05 (1.23–3.41) | ||||
| >4 cm | 48 (9.1) | 0.430 | 0.019 | 1.44 (0.60–3.44) | 0.028 | 1.27 (0.53–3.08) | 0.018 | |
| Involvement ofthe upper thirdof vagina | ||||||||
| No | 472 (89.4) | |||||||
| Yes | 56 (10.6) | 0.404 | 0.179 | 1.40 (0.74–2.66) | 0.306 | 1.40 (0.74–2.67) | 0.302 | |
| Parametrial involvement | ||||||||
| No | 489 (92.6) | |||||||
| Yes | 39 (7.4) | 0.328 | 0.377 | 1.12 (0.49–2.53) | 0.794 | 1.03 (0.45–2.37) | 0.949 | |
| Pelvic lymphnode metastasis | ||||||||
| No | (83.1) | |||||||
| Yes | 89 (16.9) | 0.319 | 0.218 | 1.06 (0.60–1.89) | 0.836 | |||
| Pelvic lymph node metastasis | - | - | ||||||
| No | 439 (83.1) | |||||||
| N1-2 | 59 (11.2) | 0.164 | 0.60 (0.30–1.33) | |||||
| n>2 | 30 (5.7) | 1.144 | 0.003 | 2.78 (1.33–5.85) | 0.006 | |||
| Global analysis of the models | χ2 | 9.456 | 21.922 | |||||
| Degrees of freedom | 5 | 6 | ||||||
| p value | 0.092 | 0.006 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pedone Anchora, L.; Carbone, V.; Gallotta, V.; Fanfani, F.; Cosentino, F.; Turco, L.C.; Fedele, C.; Bizzarri, N.; Scambia, G.; Ferrandina, G. Should the Number of Metastatic Pelvic Lymph Nodes Be Integrated into the 2018 Figo Staging Classification of Early Stage Cervical Cancer? Cancers 2020, 12, 1552. https://doi.org/10.3390/cancers12061552
Pedone Anchora L, Carbone V, Gallotta V, Fanfani F, Cosentino F, Turco LC, Fedele C, Bizzarri N, Scambia G, Ferrandina G. Should the Number of Metastatic Pelvic Lymph Nodes Be Integrated into the 2018 Figo Staging Classification of Early Stage Cervical Cancer? Cancers. 2020; 12(6):1552. https://doi.org/10.3390/cancers12061552
Chicago/Turabian StylePedone Anchora, Luigi, Vittoria Carbone, Valerio Gallotta, Francesco Fanfani, Francesco Cosentino, Luigi Carlo Turco, Camilla Fedele, Nicolò Bizzarri, Giovanni Scambia, and Gabriella Ferrandina. 2020. "Should the Number of Metastatic Pelvic Lymph Nodes Be Integrated into the 2018 Figo Staging Classification of Early Stage Cervical Cancer?" Cancers 12, no. 6: 1552. https://doi.org/10.3390/cancers12061552
APA StylePedone Anchora, L., Carbone, V., Gallotta, V., Fanfani, F., Cosentino, F., Turco, L. C., Fedele, C., Bizzarri, N., Scambia, G., & Ferrandina, G. (2020). Should the Number of Metastatic Pelvic Lymph Nodes Be Integrated into the 2018 Figo Staging Classification of Early Stage Cervical Cancer? Cancers, 12(6), 1552. https://doi.org/10.3390/cancers12061552