Statin Use Decreases the Incidence of Hepatocellular Carcinoma: An Updated Meta-Analysis






Abstract
1. Introduction
2. Results
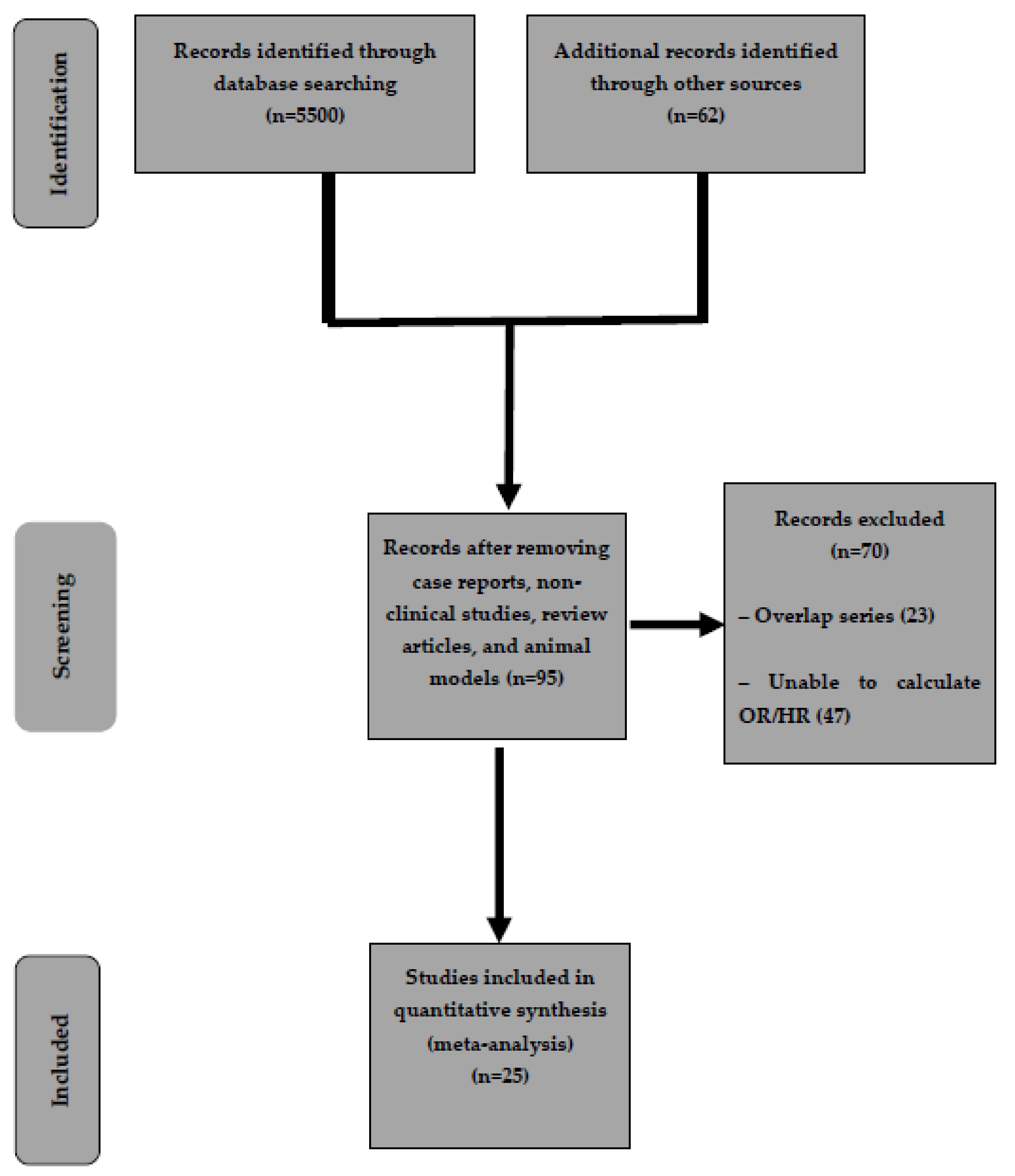
2.1. Characteristics of Included Studies
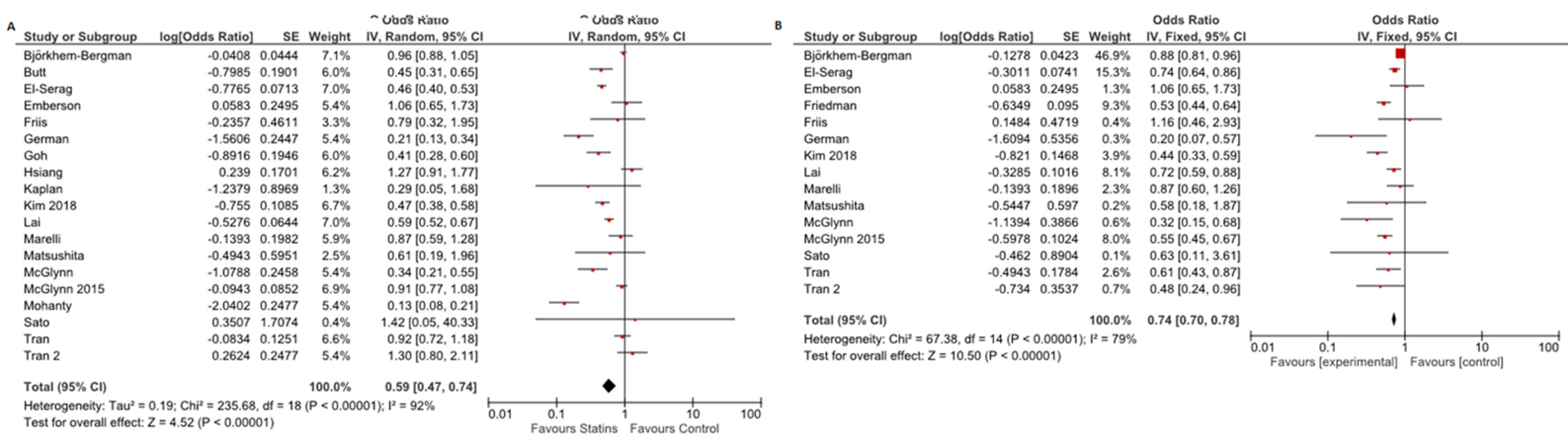
2.2. Risk of HCC
2.3. Subgroup Analysis
2.4. Sensitivity Analysis
3. Discussion
4. Methods
4.1. Inclusion and Exclusion Criteria
4.2. Search Strategy
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- El-Serag, H.B. Hepatocellular carcinoma. N. Engl. J. Med. 2011, 365, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed]
- Rognoni, C.; Ciani, O.; Sommariva, S.; Facciorusso, A.; Tarricone, R.; Bhoori, S.; Mazzaferro, V. Trans-arterial radioembolization in intermediate-advanced hepatocellular carcinoma: systematic review and meta-analyses. Oncotarget 2016, 7, 72343–72355. [Google Scholar] [CrossRef]
- Li, G.M.; Zhao, J.; Li, B.; Zhang, X.F.; Ma, J.X.; Ma, X.L.; Liu, J. The anti-inflammatory effects of statins on patients with rheumatoid arthritis: A systemic review and meta-analysis of 15 randomized controlled trials. Autoimmun. Rev. 2018, 17, 215–225. [Google Scholar] [CrossRef]
- Jain, M.K.; Ridker, P.M. Anti-inflammatory effects of statins: clinical evidence and basic mechanisms. Nat. Rev. Drug Discov. 2005, 4, 977–987. [Google Scholar] [CrossRef]
- Singh, S.; Singh, P.P.; Singh, A.G.; Murad, M.H.; Sanchez, W. Statins are associated with a reduced risk of hepatocellular cancer: a systematic review and meta-analysis. Gastroenterology 2013, 144, 323–332. [Google Scholar] [CrossRef]
- Bjorkhem-Bergman, L.; Backheden, M.; Soderberg Lofdal, K. Statin treatment reduces the risk of hepatocellular carcinoma but not colon cancer-results from a nationwide case-control study in Sweden. Pharmacoepidemiol. Drug Saf. 2014, 23, 1101–1106. [Google Scholar] [CrossRef]
- Butt, A.A.; Yan, P.; Bonilla, H.; Abou-Samra, A.B.; Shaikh, O.S.; Simon, T.G.; Chung, R.T.; Rogal, S.S. Effect of addition of statins to antiviral therapy in hepatitis C virus-infected persons: Results from ERCHIVES. Hepatology 2015, 62, 365–374. [Google Scholar] [CrossRef]
- Chang, F.M.; Wang, Y.P.; Lang, H.C.; Tsai, C.F.; Hou, M.C.; Lee, F.Y.; Lu, C.L. Statins decrease the risk of decompensation in hepatitis B virus- and hepatitis C virus-related cirrhosis: A population-based study. Hepatology 2017, 66, 896–907. [Google Scholar] [CrossRef]
- Chen, C.I.; Kuan, C.F.; Fang, Y.A.; Liu, S.H.; Liu, J.C.; Wu, L.L.; Chang, C.J.; Yang, H.C.; Hwang, J.; Miser, J.S.; et al. Cancer risk in HBV patients with statin and metformin use: a population-based cohort study. Medicine (Baltimore) 2015, 94, e462. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Johnson, M.L.; Hachem, C.; Morgana, R.O. Statins are associated with a reduced risk of hepatocellular carcinoma in a large cohort of patients with diabetes. Gastroenterology 2009, 136, 1601–1608. [Google Scholar] [CrossRef] [PubMed]
- Friedman, G.D.; Achacoso, N.; Fireman, B.; Habel, L.A. Statins and reduced risk of liver cancer: evidence for confounding. J. Natl. Cancer Inst. 2016, 108. [Google Scholar] [CrossRef] [PubMed]
- German, M.N.; Lutz, M.K.; Pickhardt, P.J.; Bruce, R.J.; Said, A. Statin use is protective against hepatocellular carcinoma in patients with nonalcoholic fatty liver disease: a case-control study. J. Clin. Gastroenterol. 2019, 17. [Google Scholar] [CrossRef] [PubMed]
- Goh, M.J.; Sinn, D.H.; Kim, S.; Woo, S.Y.; Cho, H.; Kang, W.; Gwak, G.Y.; Paik, Y.H.; Choi, M.S.; Lee, J.H.; et al. Statin use and the risk of hepatocellular carcinoma in patients with chronic hepatitis B. Hepatology 2019, 25. [Google Scholar] [CrossRef]
- Hsiang, J.C.; Wong, G.L.; Tse, Y.K.; Wong, V.W.; Yip, T.C.; Chan, H.L. Statin and the risk of hepatocellular carcinoma and death in a hospital-based hepatitis B-infected population: A propensity score landmark analysis. J. Hepatol. 2015, 63, 1190–1197. [Google Scholar] [CrossRef]
- Kaplan, D.E.; Serper, M.A.; Mehta, R.; Fox, R.; John, B.; Aytaman, A.; Baytarian, M.; Hunt, K.; Albrecht, J.; Njei, B.; et al. Effects of hypercholesterolemia and statin exposure on survival in a large national cohort of patients with cirrhosis. Gastroenterology 2019, 156, 1693–1706. [Google Scholar] [CrossRef]
- Kim, G.; Jang, S.Y.; Nam, C.M.; Kang, E.S. Statin use and the risk of hepatocellular carcinoma in patients at high risk: A nationwide nested case-control study. J. Hepatol. 2018, 68, 476–484. [Google Scholar] [CrossRef]
- King, L.; Khalili, H.; Huang, E.; Chung, R.; Chan, A. Statins are associated with a reduced risk of liver cancer: data from a large US prospective cohort study. Hepatology 2013, 58, 1216A. [Google Scholar] [CrossRef]
- Lai, S.W.; Liao, K.F.; Lai, H.C.; Muo, C.H.; Sung, F.C.; Chen, P.C. Statin use and risk of hepatocellular carcinoma. Eur. J. Epidemiol. 2013, 28, 485–492. [Google Scholar] [CrossRef]
- McGlynn, K.A.; Divine, G.W.; Sahasrabuddhe, V.V.; Engel, L.S.; VanSlooten, A.; Wells, K.; Yood, M.U.; Alford, S.H. Statin use and risk of hepatocellular carcinoma in a U.S. population. Cancer Epidemiol. 2014, 38, 523–527. [Google Scholar] [CrossRef] [PubMed]
- McGlynn, K.A.; Hagberg, K.; Chen, J.; Graubard, B.I.; London, W.T.; Jick, S.; Sahasrabuddhe, V.V. Statin use and risk of primary liver cancer in the Clinical Practice Research Datalink. J. Natl. Cancer Inst. 2015, 107. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, A.; Tate, J.P.; Garcia-Tsao, G. Statins are associated with a decreased risk of decompensation and death in veterans with hepatitis C-related compensated cirrhosis. Gastroenterology 2016, 150, 430–440.e431. [Google Scholar] [CrossRef] [PubMed]
- Simon, T.G.; Duberg, A.S.; Aleman, S.; Hagstrom, H.; Nguyen, L.H.; Khalili, H.; Chung, R.T.; Ludvigsson, J.F. Lipophilic statins and risk for hepatocellular carcinoma and death in patients with chronic viral hepatitis: results from a nationwide Swedish population. Ann. Intern. Med. 2019, 171, 318–327. [Google Scholar] [CrossRef]
- Tran, K.T.; McMenamin, U.C.; Coleman, H.G.; Cardwell, C.R.; Murchie, P.; Iversen, L.; Lee, A.J.; Thrift, A.P. Statin use and risk of liver cancer: Evidence from two population-based studies. Int. J. Cancer 2020, 146, 1250–1260. [Google Scholar] [CrossRef]
- Tsan, Y.T.; Lee, C.H.; Ho, W.C.; Lin, M.H.; Wang, J.D.; Chen, P.C. Statins and the risk of hepatocellular carcinoma in patients with hepatitis C virus infection. J. Clin. Oncol. 2013, 31, 1514–1521. [Google Scholar] [CrossRef]
- Tsan, Y.T.; Lee, C.H.; Wang, J.D.; Chen, P.C. Statins and the risk of hepatocellular carcinoma in patients with hepatitis B virus infection. J. Clin. Oncol. 2012, 30, 623–630. [Google Scholar] [CrossRef]
- Sato, S.; Ajiki, W.; Kobayashi, T.; Awata, N. Pravastatin use and the five-year incidence of cancer in coronary heart disease patients: from the prevention of coronary sclerosis study. J. Epidemiol. 2006, 16, 201–206. [Google Scholar] [CrossRef][Green Version]
- Marelli, C.; Gunnarsson, C.; Ross, S.; Haas, S.; Stroup, D.F.; Cload, P.; Clopton, P.; DeMaria, A.N. Statins and risk of cancer: a retrospective cohort analysis of 45,857 matched pairs from an electronic medical records database of 11 million adult Americans. J. Am. Coll. Cardiol. 2011, 58, 530–537. [Google Scholar] [CrossRef]
- Friis, S.; Poulsen, A.H.; Johnsen, S.P.; McLaughlin, J.K.; Fryzek, J.P.; Dalton, S.O.; Sorensen, H.T.; Olsen, J.H. Cancer risk among statin users: a population-based cohort study. Int. J. Cancer 2005, 114, 643–647. [Google Scholar] [CrossRef]
- Matsushita, Y.; Sugihara, M.; Kaburagi, J.; Ozawa, M.; Iwashita, M.; Yoshida, S.; Saito, H.; Hattori, Y. Pravastatin use and cancer risk: a meta-analysis of individual patient data from long-term prospective controlled trials in Japan. Pharmacoepidemiol. Drug Saf. 2010, 19, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Emberson, J.R.; Kearney, P.M.; Blackwell, L.; Newman, C.; Reith, C.; Bhala, N.; Holland, L.; Peto, R.; Keech, A.; Collins, R.; et al. Lack of effect of lowering LDL cholesterol on cancer: meta-analysis of individual data from 175,000 people in 27 randomised trials of statin therapy. PLoS One 2012, 7, e29849. [Google Scholar]
- Sun, H.Y.; Singh, N. Antimicrobial and immunomodulatory attributes of statins: relevance in solid-organ transplant recipients. Clin. Infect Dis. 2009, 48, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Marrone, G.; Russo, L.; Rosado, E.; Hide, D.; Garcia-Cardena, G.; Garcia-Pagan, J.C.; Bosch, J.; Gracia-Sancho, J. The transcription factor KLF2 mediates hepatic endothelial protection and paracrine endothelial-stellate cell deactivation induced by statins. J. Hepatol. 2013, 58, 98–103. [Google Scholar] [CrossRef]
- Villani, R.; Navarese, E.P.; Cavallone, F.; Kubica, J.; Bellanti, F.; Facciorusso, A.; Vendemiale, G.; Serviddio, G. Risk of statin-induced hypertransaminasemia: A systematic review and meta-analysis of randomized controlled trials. Mayo Clin. Proc. Innov. Qual. Outcomes 2019, 3, 131–140. [Google Scholar] [CrossRef]
- Murakami, Y.; Saigo, K.; Takashima, H.; Minami, M.; Okanoue, T.; Brechot, C.; Paterlini-Brechot, P. Large scaled analysis of hepatitis B virus (HBV) DNA integration in HBV related hepatocellular carcinomas. Gut 2005, 54, 1162–1168. [Google Scholar] [CrossRef]
- Demierre, M.F.; Higgins, P.D.; Gruber, S.B.; Hawk, E.; Lippman, S.M. Statins and cancer prevention. Nat. Rev. Cancer 2005, 5, 930–942. [Google Scholar] [CrossRef]
- Facciorusso, A. The influence of diabetes in the pathogenesis and the clinical course of hepatocellular carcinoma: recent findings and new perspectives. Curr. Diabetes Rev. 2013, 9, 382–386. [Google Scholar] [CrossRef]
- Weis, M.; Heeschen, C.; Glassford, A.J.; Cooke, J.P. Statins have biphasic effects on angiogenesis. Circulation 2002, 105, 739–745. [Google Scholar] [CrossRef]
- Tatsuta, M.; Iishi, H.; Baba, M.; Iseki, K.; Yano, H.; Uehara, H.; Yamamoto, R.; Nakaizumi, A. Suppression by pravastatin, an inhibitor of p21ras isoprenylation, of hepatocarcinogenesis induced by N-nitrosomorpholine in Sprague-Dawley rats. Br. J. Cancer 1998, 77, 581–587. [Google Scholar] [CrossRef][Green Version]
- Hamelin, B.A.; Turgeon, J. Hydrophilicity/lipophilicity: relevance for the pharmacology and clinical effects of HMG-CoA reductase inhibitors. Trends Pharmacol. Sci. 1998, 19, 26–37. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 14 February 2020).




{kind=link}
{kind=link}
{kind=link}
| Study, Year | Design, Period | Country | Sample Size | Age | Men, n (%) | Liver Disease Etiology (HBV/HCV/alcohol/NASH) | Follow-Up Period | Statin Use Period or Dose | Outcome Measure | Variables Adjusted for |
|---|---|---|---|---|---|---|---|---|---|---|
| Björkhem-Bergman, 2014 [8] | Case–control, July 2006 to December 2010 | Swedish Cancer Register | HCC group: 3994 patients (of which 687 statin users) Control (non-HCC), 19970 patients (of which 3598 statin users) | Mean age NR | 52% | NR | 4 years | At least 9 months | OR, aOR | Age, sex, diabetes, education, other drugs, liver disease etiology |
| ERCHIVES: Butt, 2015 [9] | Retrospective cohort, between 2002 and 2013 | USA | Statin users: 3347 Non-users: 3901 | Statin users: 53 (Non-statin users: 52 | Statin Users: 3226 (96.4%) Non-users: 3702 (94.9%) | HCV all patients | 10 years | Mean (IQR) months: Statin users: 31.7 (13.3–58.5) | HR, aHR | Baseline FIB-4 |
| Chang, 2017 [10] | Nested case–control (propensity score matching retrospective study), 1 January 2000 to 31 December 2013 | Taiwan NHIRD database (Taiwan’s National Health Insurance) | Statin users: 675 Non-users: 675 | 56.5±11.2 57.5 (14.1) | Statin users: 492 (73%) Non-users: 476 (71%) | 313 (46%)/146 (22%)/219 (32%), 292 (43%)/152 (23%)/231 (34%) | Statin users: 5.5 years (3.5) Non-users: 5.4 years (3.6) | Patient with cDDDs >28 were considered as statin user | aHR | Age, sex, diabetes, comorbidities, other drugs, liver disease etiology |
| Chen, 2014 [11] | Propensity score matching retrospective cohort, 1 January 2000 to 31 December 2008 | Taiwan’s National Health Insurance (NHI) Research Database (NHIRD) | Statin users: 8861 Statin + metformin: 5152 Non-users: 53037 | Mean NR | Statin users: 4869 (54.95%) Statin + metformin: 2650 (51.44%) Non-users: 30726 (57.93%) | All patients HBV | 9 years | Patients who used statins for <28 cDDDs were defined as statin non-users | aHR | Age, sex, comorbidities, other drugs |
| El-Serag, 2009 [12] | Nested case–control, 1997–2002 | Department of Veterans Affairs (VA) National Databases, USA | HCC group: 1303 patients of which 447 statin users Control (non-HCC): 5212 patients of which 2766 non-users | HCC group: 72 years Control (non-HCC): 72 years | HCC group: 1286 (99%) Control (non-HCC): 5144(99%) | HCC group: 25 (1.9%)/192 (14.7%)/215 (16.5%)/ Control (non-HCC): 11 (0.2%)/93 (1.8%)/60 (1.2%) | 5 years | Statin use defined as >3 prescriptions | OR, aOR | Etiology of liver disease, cirrhosis, race, other drugs |
| Friedman, 2016 [13] | Case–control, 1 January 1996 to 30 June 2014 | Kaiser Permanente Northern California, USA | HCC group: 2877 patients of which 701 statin users Control group (non-HCC): 142850 patients of which 44953 statin users | NR | NR | NR | 18 years | NR | aOR | Liver disease etiology, comorbidities, other drugs, BMI |
| German, 2019 [14] | Case–control, 2002–2016 | Wisconsin (USA) | HCC group: 34 patients of which 6 statin users Control group (non-HCC): 68 patients of which 34 statin users | HCC group: 68.9±11.4 Control group (non-HCC): 69.4±7.5 | HCC group: 22 Control group (non-HCC): 44 | NAFLD all patients | 14 years | NR | OR, aOR | Age, sex, other drugs |
| Goh, 2019 [15] | Retrospective cohort, January 2008 to December 2012 | Single institution in Seoul, Republic of Korea | Statin users: 713 Non-users: 7000 | Statin users: 50 (44–56) Non-users: 47 (39–54) | Statin users: 482 (67.6%) Non-users: 4624 (66.1%) | HBV (all patients) | 7.2 years (0.5–9.7) | cDDD >28 was considered as statin use | HR, aHR | Age, sex, liver cirrhosis, comorbidities, viral level, other drugs, liver function tests |
| Hsiang, 2015 [16] | Propensity score matching retrospective cohort, January 2000 to December 2012 | Hospital Authority (HA) registry database, Hong Kong | Statin users: 1176 Non-users: 52337 | Statin users: 58.7±12.4 Non-users: 58.9±12.9 | NR | HBV (all patients) | Statin users: 1.6 years (0.7–3.9) Non-users: 2.6 years (1–5.1) | cDDD: 291.5 | aHR | – |
| Kaplan, 2019 [17] | Propensity score matching retrospective cohort, 1 January 2008 through 30 June 2016 | Veterans’ Health Administration | Statin users: 21921 Non-users: 51023 | Statin users: 64 (60–69) Non-users: 63 (58–68) | Statin users: 21373 (97.5%) Non-users: 12602 (98%) | Statin users: NR/2457 (11.2%)/8471 (38.6%)/5158 (23.5%) Non-users: NR/2065 (14.9%)/4876 (35.2%)/2159 (15.6%) | Statin users: 900 days (478–1546) Non-users: 1970 days (1234–2736) | 270 days (0–827) | aHR | Race, liver disease etiology, liver function tests, cirrhosis, comorbidities, BMI |
| Kim, 2018 [18] | Nested case–control study, 2002–2013 | National Health Insurance Service Physical Health Examination in the Republicof Korea. | HCC group: 1642 patients of which 111 statin users Non-HCC group: 8210 patients of which 1047 statin users | HCC group: 61.8±9.2 Non-HCC group: 61.8±9.2 | HCC group: 1372 (83.6%) Non-HCC group: 6860 (83.6%) | HCC group: 755 (46%)/NR/277 (16.9%)/NR Non-HCC group: 232 (2.8%)/NR/418 (5.1%)/NR | NR | OR, aOR | Comorbidities, cirrhosis, BMI, other drugs, household income level | |
| King, 2013 [19] | Prospective cohort | USA | 136178 | NR | NR | NR | >20 years | aHR | Age, BMI, comorbidities, other drugs | |
| Lai, 2013 [20] | Case–Control study, 2000–2009 | Taiwan National Health Insurance program | HCC group: 3480 patients of which 255 statin users Non-HCC: 13920 patients of which 1635 statin users | HCC group: 62.7±13.4 Non-HCC: 62.2±13.7 | HCC group: 2525 (72.6%) Non-HCC: 10100 (72.6%) | HCC group: 1295 (37.2%)/1005 (28.9%)/66 (1.90%)/72 (2.07%) Non-HCC: 424 (3.05%)/274 (1.97%)/75 (0.54%)/86 (0.62%) | 9 years | HCC group: 16.7 months Non-HCC: 18.6 months | OR, aOR | Age, sex, comorbidities, cirrhosis, etiology of liver disease, other drugs |
| McGlynn, 2014 [21] | Nested case–control, between 1999 and 2010 | Population of the Health Alliance Plan HMO of the Henry FordHealth System (HFHS), a single integrated health system. USA | HCC group: 94 patients of which 25 statin users Non-HCC group: 468 patients of which 233 statin users | Mean NR | HCC group: 70 (74.47%) Non-HCC group: 348 (74.36%) | HCC group: 1 (1.06%)/46 (48.94%)/24 (25.53%)/NR Non-HCC group: 1 (0.21%)/8 (1.71%)/4 (0.85%)/NR | NR | ≤2 years: HCC group: 13 Control group: 105 > 2 years use of statin: HCC group: 12 Control: 128 | OR, aOR | Race, etiology of liver disease, comorbidities |
| McGlynn, 2015 [22] | Nested case–control, 1988 and 2011 | UK’s Clinical Practice Research Datalink (CPRD). | HCC group: 1195 patients of which 302 statin users Non-HCC group: 4640 patients of which 1242 statin users | HCC group: 97.2±12.1 Non-HCC group: 67±12.1 | HCC group: 856 (71.6%) Non-HCC group: 3322 (71.6%) | HCC group: 74 (6.2%)/189 (15.8%)/170 (14.2%) Non-HCC group: 23/(0.5%)/189 (4%)/9 (0.2%) | NR | Cumulative dose: <8120) HCC: 168 (14.1%) Control: 642 (13.2%) >(21 281 HCC: 152 (12.7%) Control: 649 (14%) | OR, aOR | BMI, etiology of liver disease, comorbidities, other drugs used |
| Mohanty, 2016 [23] | Propensity score matching retrospective cohort, January 1996 through December 2009 | Veteran Affairs Clinical Case Registry, which contains nationwide data from veterans infected with the HCV | Statin users: 685 Non-users: 685 | Statin users: 56 (52–59) Non-users: 56 (52–60) | Statin users: 677 (98.8%) Non-users: 671 (97.9%) | All had HCV and compensated cirrhosis | NR | NR | HR | – |
| Simon, 2019 [24] | Propensity score matching cohort study, 2005–2013 | Swedish registers | Statin users: 16668 Non-users: 8334 | Statin users: 47.3±11 Non-users: 47.5±13.7 | Statin users: 65.2% Non-users: 65.6% | Statin users: 1540 (23.5%)/5014/6554 (76.5%)/NR Non-users: 1953 (23.4%)/6381/76.6% | 8 years | NR | aHR | Age, sex, duration of viral infection, cirrhosis, comorbidities, other drugs used |
| Tran, 2019 [25] | Nested case–control, 1999-2011 | Scottish Primary Care Clinical Informatics Unit (PCCIU) database. | HCC group: 434 patients of which 111 statin users Non-HCC group: 2103 patients of which 571 statin users | Mean NR | HCC group: 292 (67.3%) Non-HCC group: 1412 (67.1%) | NR | NR | HCC group: 4.88 years (3.1–7.29) Non-HCC group: 4.83 years (3.1–7.24) | OR, aOR | Age, sex, obesity, comorbidities, other drugs used, alcohol |
| Tran, 2019 (II) [25] | Prospective cohort | UK Biobank | Statin users: 395301 Non-users: 76550 | Mean NR | NR | NR | NR | NR | OR | Age, sex, body mass index, alcohol, comorbidities, other drugs used |
| Tsan, 2012 [27] | Retrospective cohort, 1997–2008 | Taiwan National Health Insurance Research Database | Statin users: 2785 Non-users: 30628 | Statin users: 34.7 (26.6–43.8) Non-users: 46.3 (38.9–55.3) | Statin users: 1590 (57.1%) Non-users: 17852 (58.3%) | All patients have HBV | NR | 28–90 cDDD: 933 (33.5%) 91–356 cDDD: 1279 (45.9%) >365 cDDDs: 573 (20.6%) | HR, aHR | Age, sex, income, diabetes, and liver cirrhosis |
| Tsan, 2013 [26] | Retrospective cohort, 1 January 1999 to 31 December 2010 | Taiwan National Health Insurance Research Database | Statin users: 35023 Non-users: 225841 | Statin users: 53.9 (45.4–62.1) Non-users: 49.8 (38.9–62) | Statin users: 14973 (42.8%) Non-users: 113290 (50.2%) | All patients had HCV | Statin users: 12 years (12.0–12.0) Non-users: 12 years (10.9–12) | 179.6 CDD (80.0–414.7) | HR, aHR | Age, sex, urbanization, income, liver cirrhosis, and diabetes |
| Sato, 2006 [28] | RCT 28 September 1991 and 31 March 1995 | Japan | Statin users: 179 Non-users: 84 | NR | NR | NR | NR | All patients used pravastatin | OR, aOR | – |
| Marelli, 2011 [29] | Retrospective cohort, propensity score matching, 1990–2009 | General Electric Centricity electronic medical records database | Statin users: 45857 Non-users: 45857 | Statin users: 64.2±10.44 Non-users: 64.19±9.45 | Statin users: 23953 (52.23%) Non-users: 24106 (52.57%) | Viral 28 (0.06%) | Statin users: 8.43 years Non-users: 8.43 years | NR | OR, aOR | – |
| Friis, 2005 [30] | Population-based cohort study, 1989–2002 | The Prescription Database of North Jutland County and the Danish Cancer Registry | Statin users: 12251 Non-users: 322503 | Statin users: 60.7 Non-users: 53.9 | 6935 (57%) 707 (56%) | NR | 3.3 years (0–14) | Number of statin prescriptions: 2–4: 2392 (20%) 5–9: 2516 (21%) 10–19: 3282 (27%) 20+: 4061 (33%) | aOR | Age, gender, other drugs used |
| Matsushita, 2010 [31] | Individual patient meta-analysis of RCT | Multicenter | Statin users: 7375 Non-users: 6349 | Statin users: 57.9±8.3 Non-users: 57.1±8.7 | Statin users: 47.4% Non-users: 49.5% | NR | 5.3 years | All patients used pravastatin | OR, aOR | – |
| Emberson, 2012 [32] | Individual patient meta-analysis from RCTs | International | Statin users: 67258 Non-users: 67279 | 63 | 46675 (27%) | NR | 4.9 years | NR | OR, aOR | – |
| Variable | Subgroup | Studies (n) | Summary Estimate (95% CI) | Within-Group Heterogeneity (I2) |
|---|---|---|---|---|
| Etiology of liver disease | HBV | 2 | 0.46 (0.36–0.60) | 0% |
| HCV | 2 | 0.68 (0.30–1.55) | 66% | |
| Diabetes | Yes | 5 | 0.52 (0.46–0.58) | 0% |
| No | 4 | 0.43 (0.31–0.61) | 58% | |
| Cumulative defined daily dose | ≤365 | 3 | 0.51 (0.30–0.88) | 78% |
| >365 | 3 | 0.27 (0.11–0.67) | 81% | |
| Molecule | Lipophilic | 2 | 0.49 (0.39–0.62) | 19% |
| Hydrophilic | 2 | 0.73 (0.40–1.34) | 83% | |
| Simvastatin | 2 | 0.69 (0.42–1.15) | 55% | |
| Atorvastatin | 2 | 0.43 (0.28–0.65) | 17% | |
| Fluvastatin | 2 | 1.02 (0.08–13.25) | 83% | |
| Pravastatin | 1 | 0.80 (0.46–1.39) | NA | |
| Rosuvastatin | 2 | 0.53 (0.04–6.38) | 86% |
| Variable | Subgroup | Studies (n) | Summary Estimate (95% CI) | Within-Group Heterogeneity (I2) |
|---|---|---|---|---|
| Study design | Observational | 16 | 0.52 (0.41–0.73) | 87% |
| RCT | 3 | 0.98 (0.76–1.32) | 45% | |
| Study location | Asia | 8 | 0.51 (0.43–0.65) | 44% |
| Western | 8 | 0.59 (0.45–0.81) | 34% | |
| Study quality | High | 13 | 0.54 (0.44–0.89) | 39.4% |
| Low | 3 | 0.57 (0.41–0.98) | 55% | |
| Abbreviations: CI, Confidence Interval; RCT, Randomized-Controlled Trial | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Facciorusso, A.; Abd El Aziz, M.A.; Singh, S.; Pusceddu, S.; Milione, M.; Giacomelli, L.; Sacco, R. Statin Use Decreases the Incidence of Hepatocellular Carcinoma: An Updated Meta-Analysis. Cancers 2020, 12, 874. https://doi.org/10.3390/cancers12040874
Facciorusso A, Abd El Aziz MA, Singh S, Pusceddu S, Milione M, Giacomelli L, Sacco R. Statin Use Decreases the Incidence of Hepatocellular Carcinoma: An Updated Meta-Analysis. Cancers. 2020; 12(4):874. https://doi.org/10.3390/cancers12040874
Chicago/Turabian StyleFacciorusso, Antonio, Mohamed A Abd El Aziz, Siddharth Singh, Sara Pusceddu, Massimo Milione, Luca Giacomelli, and Rodolfo Sacco. 2020. "Statin Use Decreases the Incidence of Hepatocellular Carcinoma: An Updated Meta-Analysis" Cancers 12, no. 4: 874. https://doi.org/10.3390/cancers12040874
APA StyleFacciorusso, A., Abd El Aziz, M. A., Singh, S., Pusceddu, S., Milione, M., Giacomelli, L., & Sacco, R. (2020). Statin Use Decreases the Incidence of Hepatocellular Carcinoma: An Updated Meta-Analysis. Cancers, 12(4), 874. https://doi.org/10.3390/cancers12040874