Evaluation of a Novel Prototype for Pressurized Intraperitoneal Aerosol Chemotherapy

 , , , , , ,
, , , , , ,  , and
, and 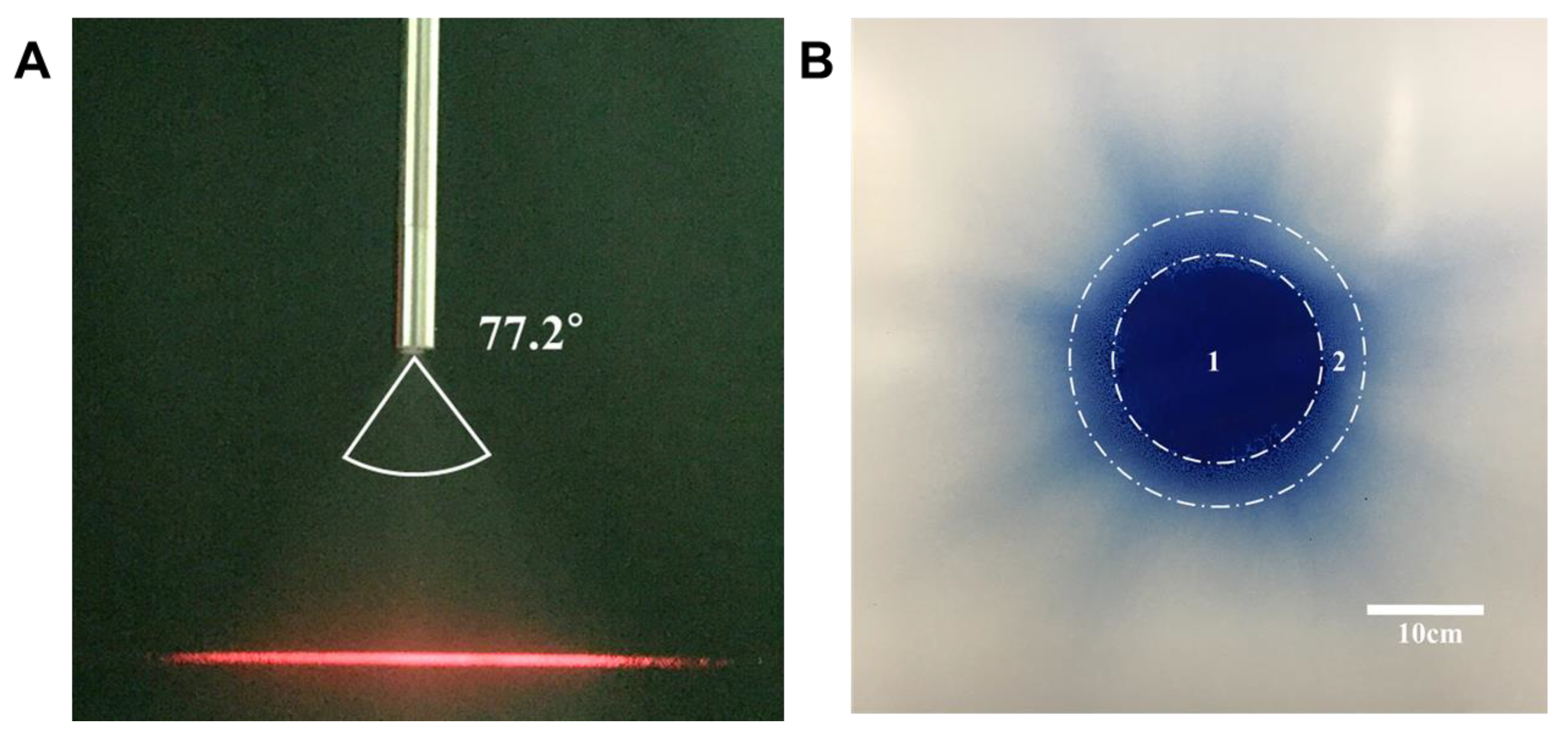{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
2.1. Granulometric Analysis and Spray Angle
2.2. Distribution Analysis with Methylene Blue Solution
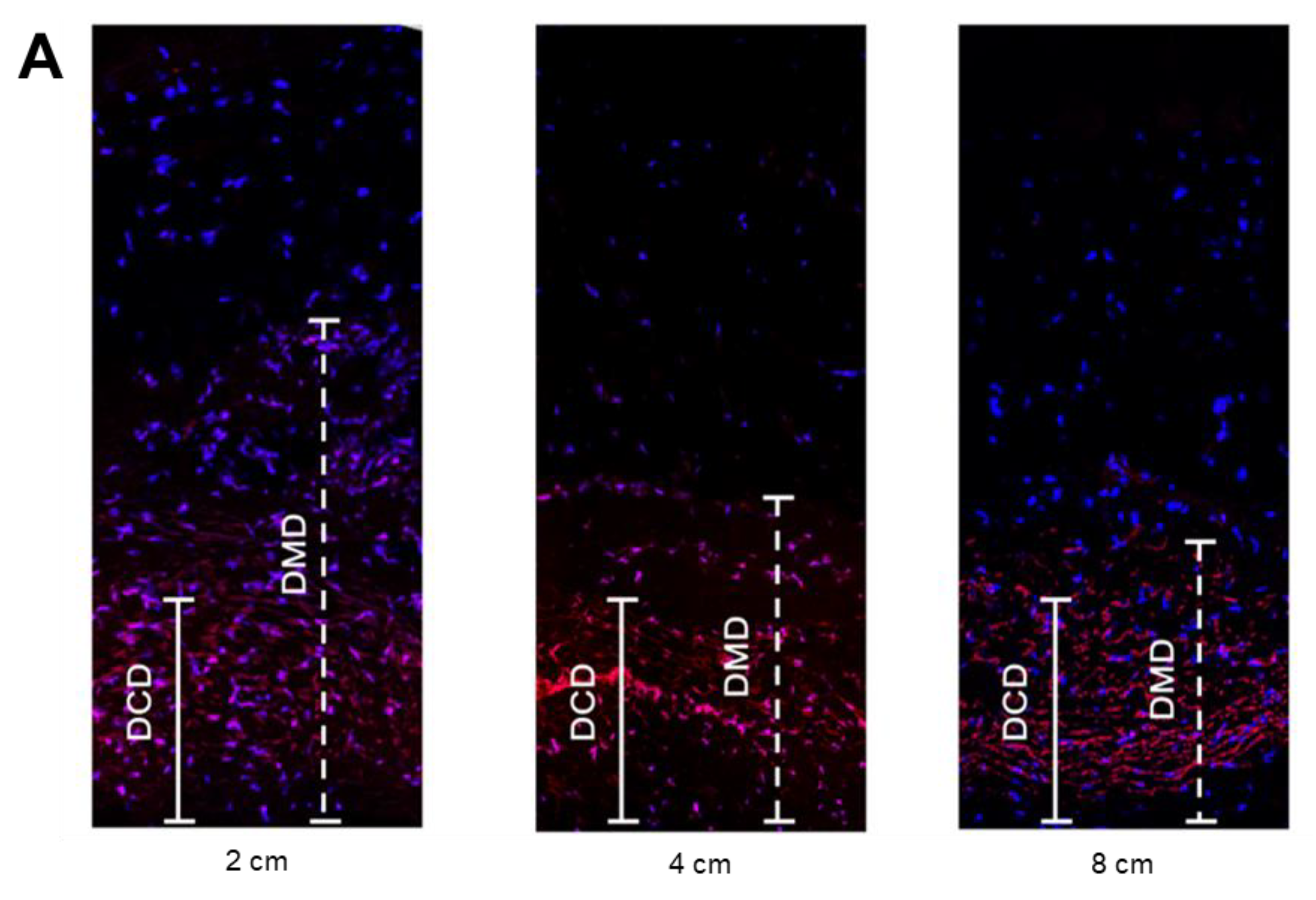
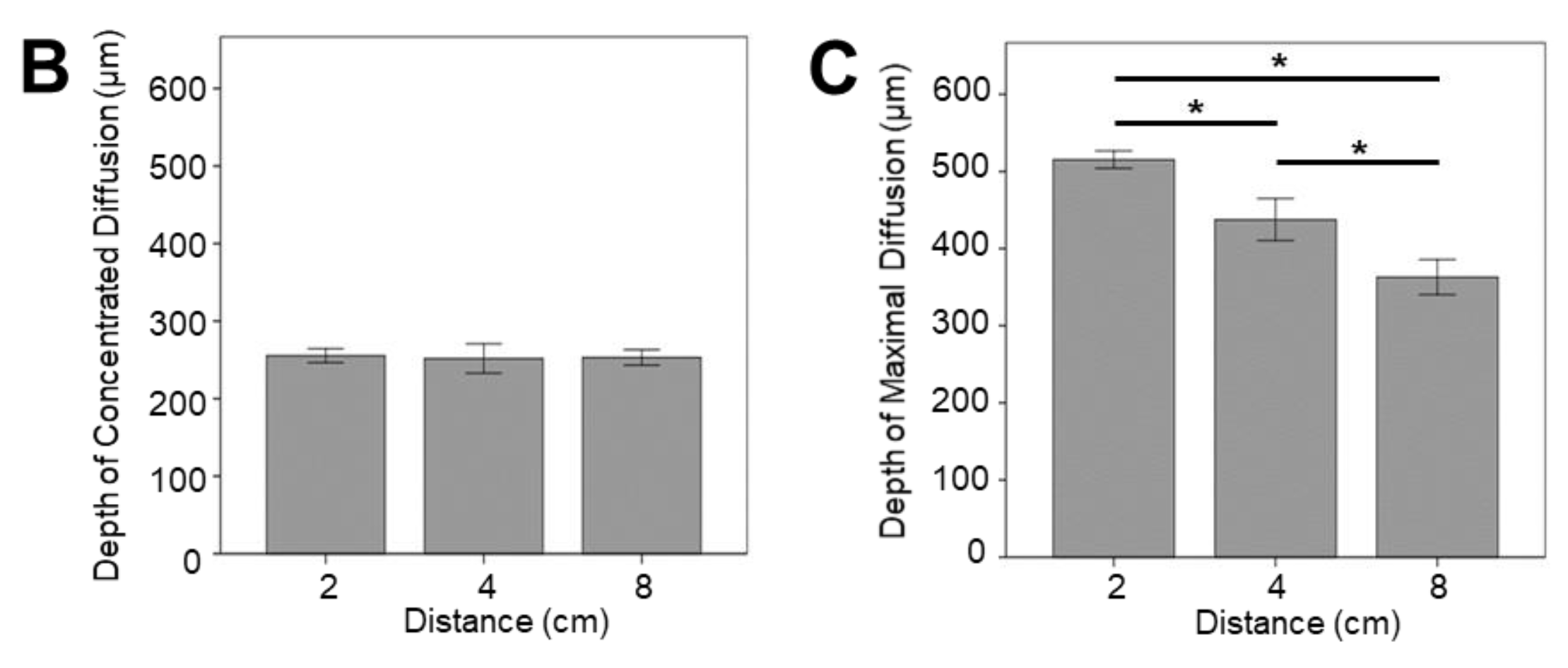
2.3. Ex-Vivo Experimental Analysis
3. Discussion
4. Materials and Methods
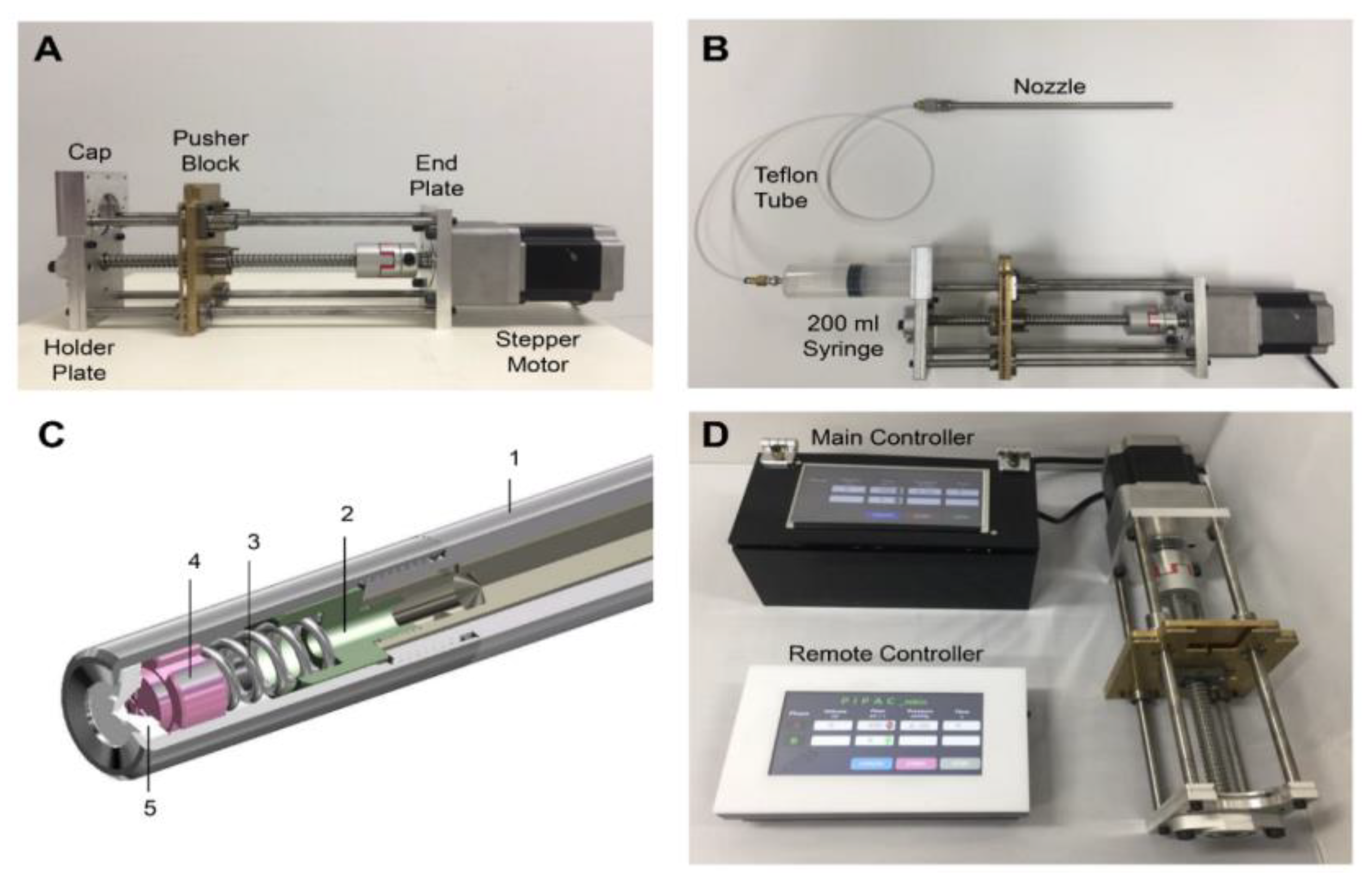
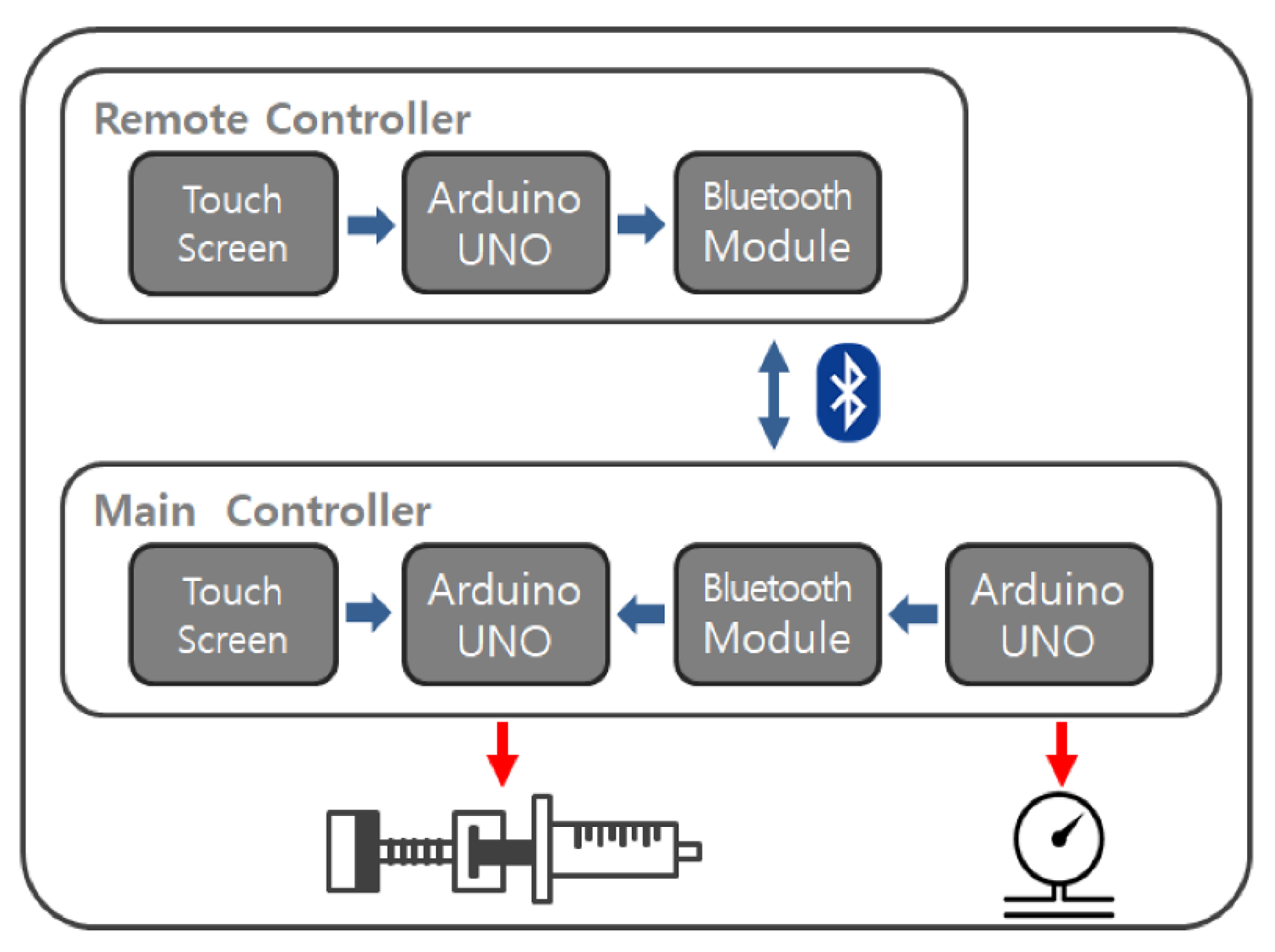
4.1. Prototype Development
4.2. Granulometric Analysis and Spray Angle
4.3. Distribution Analysis with Methylene Blue Solution
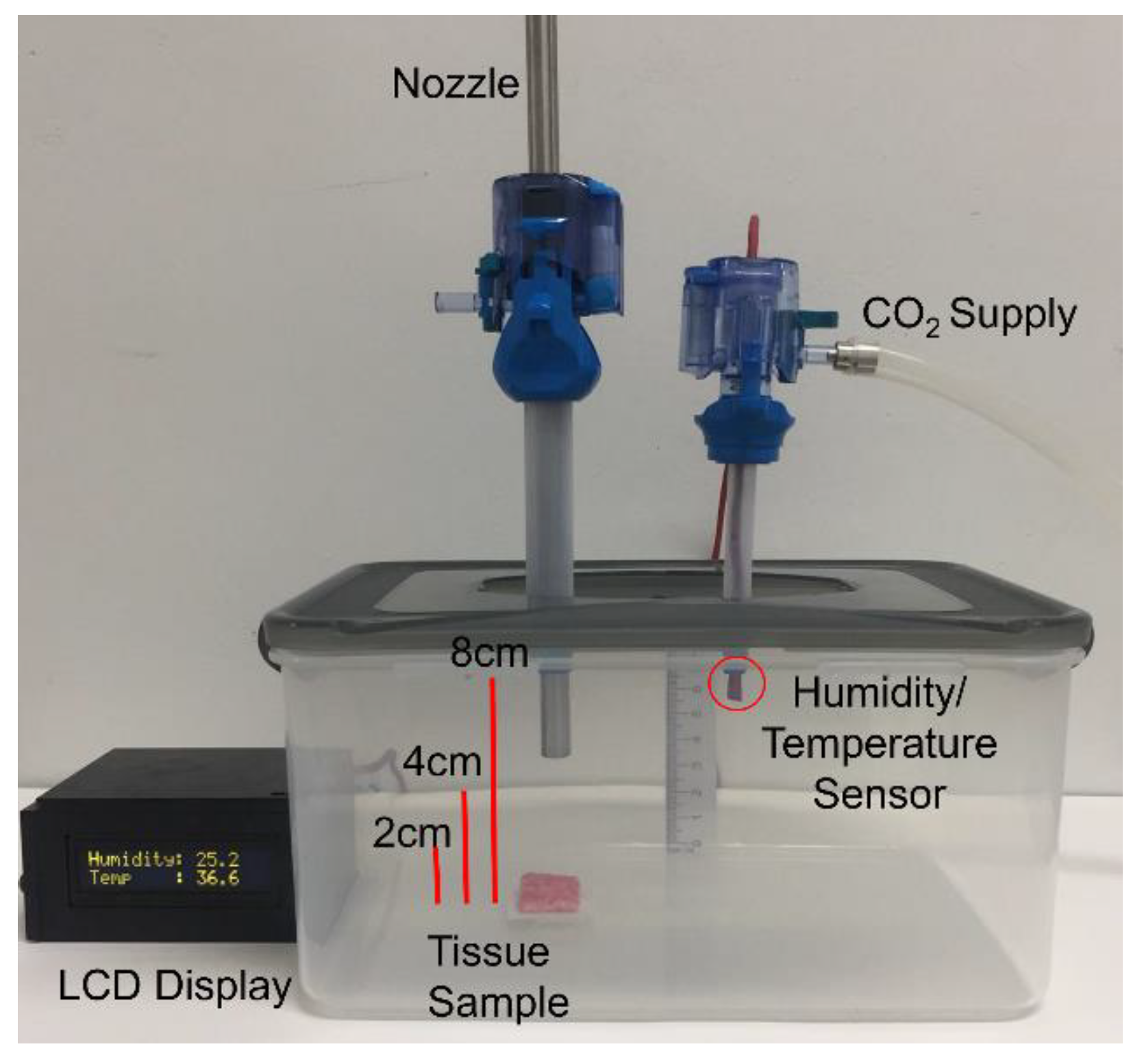
4.4. Ex-Vivo Experiment
4.5. Statistical Analysis
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hanker, L.; Loibl, S.; Burchardi, N.; Pfisterer, J.; Meier, W.; Pujade-Lauraine, E.; Ray-Coquard, I.; Sehouli, J.; Harter, P.; du Bois, A. The impact of second to sixth line therapy on survival of relapsed ovarian cancer after primary taxane/platinum-based therapy. Ann. Oncol. 2012, 23, 2605–2612. [Google Scholar] [CrossRef] [PubMed]
- Elias, D.; Gilly, F.; Boutitie, F.; Quenet, F.; Bereder, J.-M.; Mansvelt, B.; Lorimier, G.; Dube, P.; Glehen, O. Peritoneal colorectal carcinomatosis treated with surgery and perioperative intraperitoneal chemotherapy: Retrospective analysis of 523 patients from a multicentric French study. J. Clin. Oncol. 2010, 28, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Ung, L.; Chua, T.C.; Morris, D.L. Cure for peritoneal metastases? An evidence-based review. ANZ J. Surg. 2013, 83, 821–826. [Google Scholar] [CrossRef] [PubMed]
- Gill, R.S.; Al-Adra, D.P.; Nagendran, J.; Campbell, S.; Shi, X.; Haase, E.; Schiller, D. Treatment of gastric cancer with peritoneal carcinomatosis by cytoreductive surgery and HIPEC: A systematic review of survival, mortality, and morbidity. J. Surgi. Oncol. 2011, 104, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Solass, W.; Kerb, R.; Mürdter, T.; Giger-Pabst, U.; Strumberg, D.; Tempfer, C.; Zieren, J.; Schwab, M.; Reymond, M.A. Intraperitoneal chemotherapy of peritoneal carcinomatosis using pressurized aerosol as an alternative to liquid solution: First evidence for efficacy. Ann. Surg. Oncol. 2014, 21, 553–559. [Google Scholar] [CrossRef]
- Flessner, M.F. The transport barrier in intraperitoneal therapy. Am. J. Physiol. Renal. Physiol. 2005, 288, F433–F442. [Google Scholar] [CrossRef] [PubMed]
- Dedrick, R.L.; Myers, C.E.; Bungay, P.M.; DeVita, V. Pharmacokinetic rationale for peritoneal drug administration. Cancer Treat. Rep. 1978, 62, 1–13. [Google Scholar] [PubMed]
- Los, G.; Mutsaers, P.H.; van der Vijgh, W.J.; Baldew, G.S.; de Graaf, P.W.; McVie, J.G. Direct diffusion of cis-diamminedichloroplatinum (II) in intraperitoneal rat tumors after intraperitonal chemotherapy: A comparison with systemic chemotherapy. Cancer Res. 1989, 49, 3380–3384. [Google Scholar] [PubMed]
- Hendrix, R.J.; Kassira, J.P.; Lambert, L.A. Elevated Maximum Core Body Temperature During Hyperthermic Intraperitoneal Chemoperfusion (HIPEC) is Associated with Increased Postoperative Complications. Ann. Surg. Oncol. 2019, 27, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Reymond, M.A.; Hu, B.; Garcia, A.; Reck, T.; Köckerling, F.; Hess, J.; Morel, P. Feasibility of therapeutic pneumoperitoneum in a large animal model using a microvaporisator. Surg. Endosc. 2000, 14, 51. [Google Scholar] [CrossRef] [PubMed]
- Göhler, D.; Khosrawipour, V.; Khosrawipour, T.; Diaz-Carballo, D.; Falkenstein, T.A.; Zieren, J.; Stintz, M.; Giger-Pabst, U. Technical description of the microinjection pump (MIP®) and granulometric characterization of the aerosol applied for pressurized intraperitoneal aerosol chemotherapy (PIPAC). Surg. Endosc. 2017, 31, 1778–1784. [Google Scholar] [CrossRef] [PubMed]
- Demtröder, C.; Solass, W.; Zieren, J.; Strumberg, D.; Giger-Pabst, U.; Reymond, M.A. Pressurized intraperitoneal aerosol chemotherapy with oxaliplatin in colorectal peritoneal metastasis. Colorectal Dis. 2016, 18, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Tempfer, C.B.; Celik, I.; Solass, W.; Buerkle, B.; Pabst, U.G.; Zieren, J.; Strumberg, D.; Reymond, M.-A. Activity of pressurized intraperitoneal aerosol chemotherapy (PIPAC) with cisplatin and doxorubicin in women with recurrent, platinum-resistant ovarian cancer: Preliminary clinical experience. Gynecol. Oncol. 2014, 132, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Khosrawipour, V.; Khosrawipour, T.; Falkenstein, T.A.; Diaz-Carballo, D.; Foerster, E.; Osma, A.; Adamietz, I.A.; Zieren, J.; Fakhrian, K. Evaluating the effect of Micropump© position, internal pressure and doxorubicin dosage on efficacy of pressurized intra-peritoneal aerosol chemotherapy (PIPAC) in an ex vivo model. Anticancer Res. 2016, 36, 4595–4600. [Google Scholar] [CrossRef] [PubMed]
- Alyami, M.; Hübner, M.; Grass, F.; Bakrin, N.; Villeneuve, L.; Laplace, N.; Passot, G.; Glehen, O.; Kepenekian, V. Pressurised intraperitoneal aerosol chemotherapy: Rationale, evidence, and potential indications. Lancet. Oncol. 2019, 20, e368–e377. [Google Scholar] [CrossRef]
- Solaß, W.; Giger-Pabst, U.; Zieren, J.; Reymond, M.A. Pressurized intraperitoneal aerosol chemotherapy (PIPAC): Occupational health and safety aspects. Ann. Surg. Oncol. 2013, 20, 3504–3511. [Google Scholar] [CrossRef] [PubMed]
- Khosrawipour, V.; Khosrawipour, T.; Diaz-Carballo, D.; Förster, E.; Zieren, J.; Giger-Pabst, U. Exploring the spatial drug distribution pattern of pressurized intraperitoneal aerosol chemotherapy (PIPAC). Ann. Surg. Oncol. 2016, 23, 1220–1224. [Google Scholar] [CrossRef] [PubMed]






© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.S.; Kim, J.; Lee, E.J.; Park, S.J.; Mun, J.; Paik, H.; Oh, S.H.; Park, S.; Ryu, S.; Lim, W.; et al. Evaluation of a Novel Prototype for Pressurized Intraperitoneal Aerosol Chemotherapy. Cancers 2020, 12, 633. https://doi.org/10.3390/cancers12030633
Lee HS, Kim J, Lee EJ, Park SJ, Mun J, Paik H, Oh SH, Park S, Ryu S, Lim W, et al. Evaluation of a Novel Prototype for Pressurized Intraperitoneal Aerosol Chemotherapy. Cancers. 2020; 12(3):633. https://doi.org/10.3390/cancers12030633
Chicago/Turabian StyleLee, Hee Su, Junsik Kim, Eun Ji Lee, Soo Jin Park, Jaehee Mun, Haerin Paik, Soo Hyun Oh, Sunwoo Park, Soomin Ryu, Whasun Lim, and et al. 2020. "Evaluation of a Novel Prototype for Pressurized Intraperitoneal Aerosol Chemotherapy" Cancers 12, no. 3: 633. https://doi.org/10.3390/cancers12030633
APA StyleLee, H. S., Kim, J., Lee, E. J., Park, S. J., Mun, J., Paik, H., Oh, S. H., Park, S., Ryu, S., Lim, W., Song, G., Kim, H. S., & Lee, J. C. (2020). Evaluation of a Novel Prototype for Pressurized Intraperitoneal Aerosol Chemotherapy. Cancers, 12(3), 633. https://doi.org/10.3390/cancers12030633