Lymph Node and Bone Marrow Micrometastases Define the Prognosis of Patients with pN0 Esophageal Cancer

 , ,
, , 
Abstract
1. Introduction
2. Methods
2.1. Patients, Study Design, and Inclusion Criteria
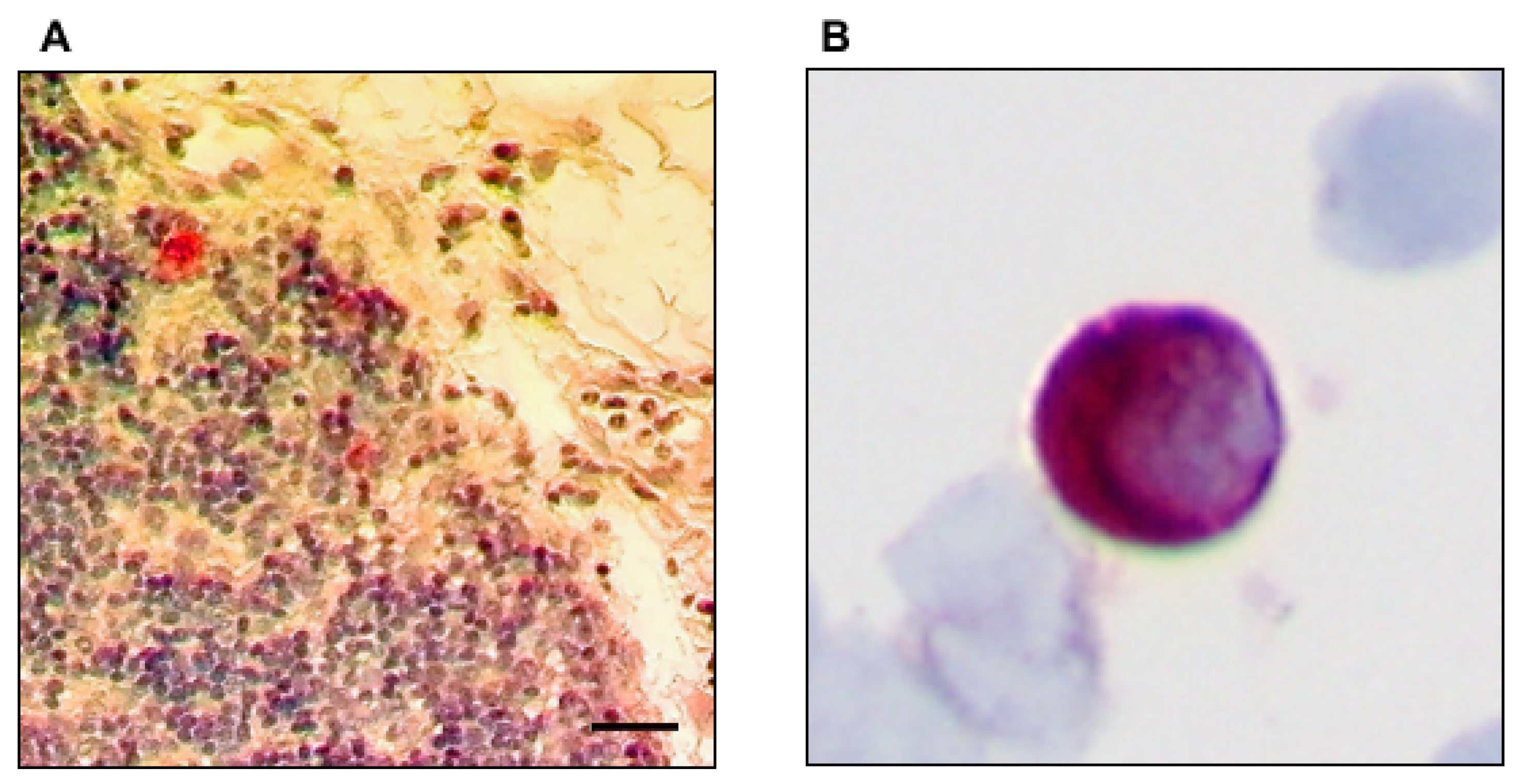
2.2. Preparation of the Surgical Specimen and Immunohistochemical Analysis
2.3. Statistical Analysis
2.4. Statement of Ethics
3. Results
3.1. Characteristics of Patients and Clinicopathological Parameters
3.2. Prevalence of Immunohistochemically Detectable Tumor Cells in Lymph Nodes and Bone Marrow
3.3. Association of Micrometastases in Lymph Nodes and Bone Marrow
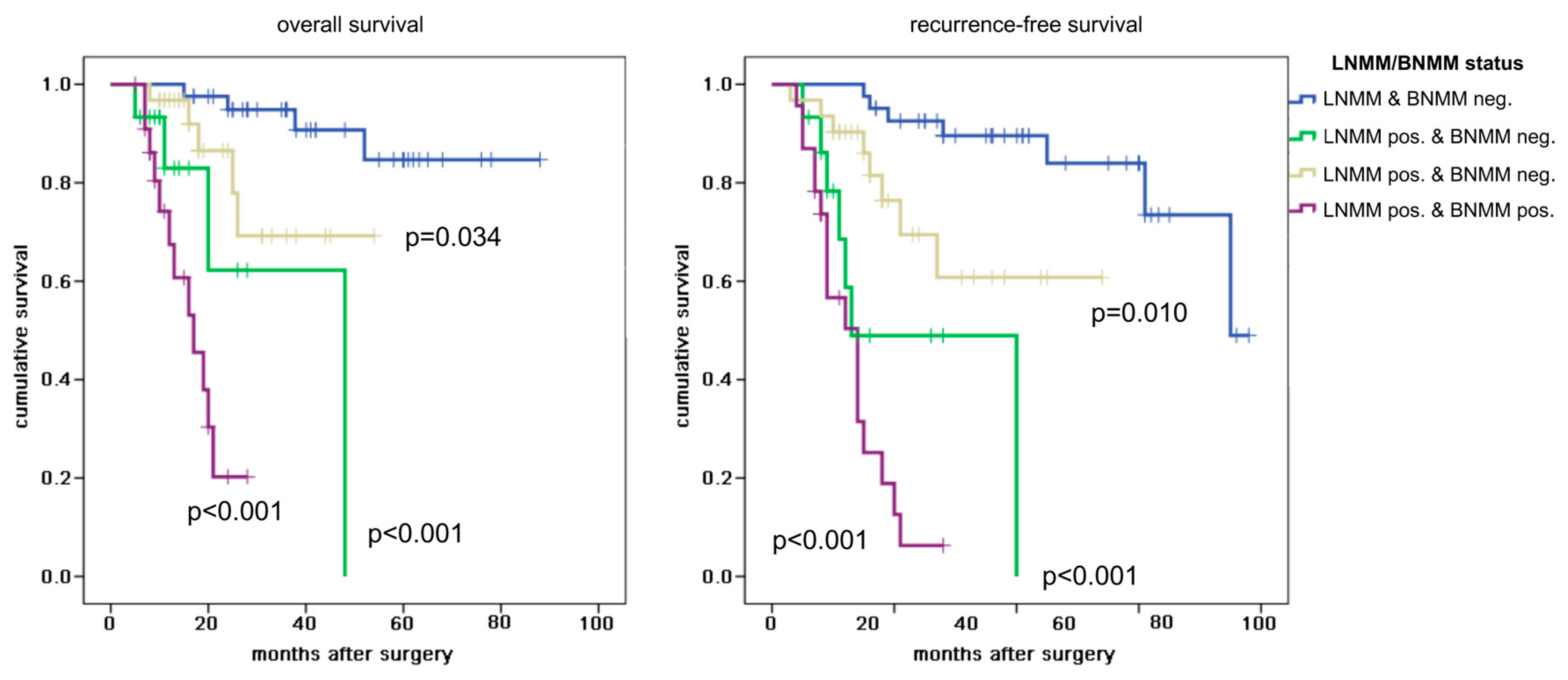
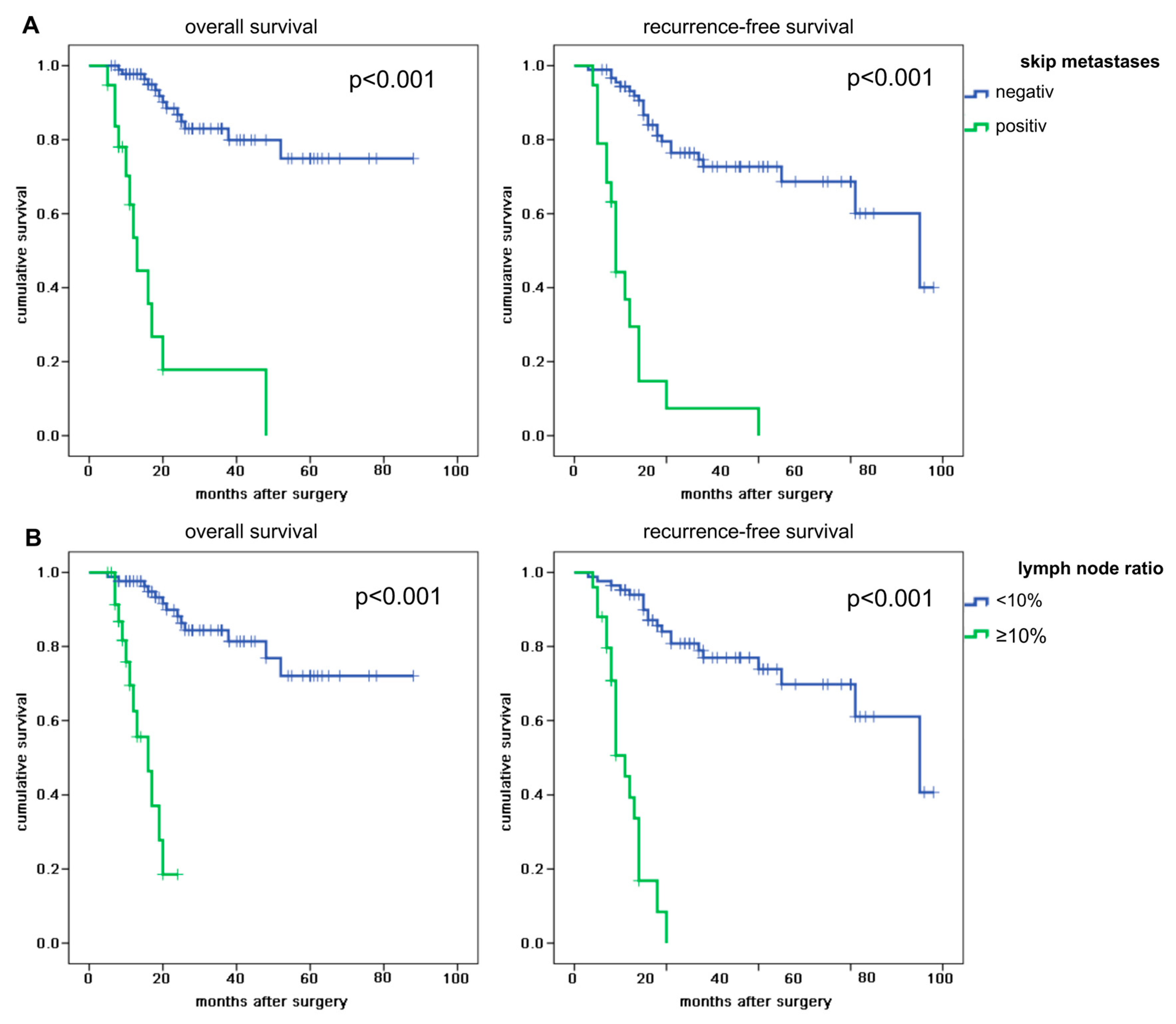
3.4. Survival Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Parry, K.; Visser, E.; van Rossum, P.S.N.; Mohammad, N.H.; Ruurda, J.P.; van Hillegersberg, R. Prognosis and Treatment After Diagnosis of Recurrent Esophageal Carcinoma Following Esophagectomy with Curative Intent. Ann. Surg. Oncol. 2015, 22, S1292–S1300. [Google Scholar] [CrossRef]
- Su, X.-D.; Zhang, D.-K.; Zhang, X.; Lin, P.; Long, H.; Rong, T.-H. Prognostic factors in patients with recurrence after complete resection of esophageal squamous cell carcinoma. J. Thorac. Dis. 2014, 6, 949–957. [Google Scholar]
- Lee, P.C.; Mirza, F.M.; Port, J.L.; Stiles, B.M.; Paul, S.; Christos, P.; Altorki, N.K. Predictors of recurrence and disease-free survival in patients with completely resected esophageal carcinoma. J. Thorac. Cardiovasc. Surg. 2011, 141, 1196–1206. [Google Scholar] [CrossRef][Green Version]
- Chen, M.-F.; Chen, P.-T.; Lu, M.-S.; Lee, C.-P.; Chen, W.-C. Survival benefit of surgery to patients with esophageal squamous cell carcinoma. Sci. Rep. 2017, 7, 46139. [Google Scholar] [CrossRef]
- Ovrebo, K.K.; Lie, S.A.; Laerum, O.D.; Svanes, K.; Viste, A. Long-term survival from adenocarcinoma of the esophagus after transthoracic and transhiatal esophagectomy. World J. Surg. Oncol. 2012, 10, 130. [Google Scholar] [CrossRef]
- Rice, T.W.; Ishwaran, H.; Ferguson, M.K.; Blackstone, E.H.; Goldstraw, P. Cancer of the Esophagus and Esophagogastric Junction: An Eighth Edition Staging Primer. J. Thorac. Oncol. 2017, 12, 36–42. [Google Scholar] [CrossRef]
- Sato, F.; Shimada, Y.; Li, Z.; Watanabe, G.; Maeda, M.; Imamura, M. Lymph node micrometastasis and prognosis in patients with oesophageal squamous cell carcinoma. Br. J. Surg. 2001, 88, 426–432. [Google Scholar] [CrossRef]
- Heeren, P.M.; Kelder, W.; Blondeel, I.; van Westreenen, H.L.; Hollema, H.; Plukker, J.T. Prognostic value of nodal micrometastases in patients with cancer of the gastro-oesophageal junction. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2005, 31, 270–276. [Google Scholar] [CrossRef]
- Buskens, C.J.; Ten Kate, F.J.W.; Obertop, H.; Izbicki, J.R.; van Lanschot, J.J.B. Analysis of micrometastatic disease in histologically negative lymph nodes of patients with adenocarcinoma of the distal esophagus or gastric cardia. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2008, 21, 488–495. [Google Scholar] [CrossRef]
- Izbicki, J.R.; Hosch, S.B.; Pichlmeier, U.; Rehders, A.; Busch, C.; Niendorf, A.; Passlick, B.; Broelsch, C.E.; Pantel, K. Prognostic value of immunohistochemically identifiable tumor cells in lymph nodes of patients with completely resected esophageal cancer. N. Engl. J. Med. 1997, 337, 1188–1194. [Google Scholar] [CrossRef]
- Vashist, Y.K.; Effenberger, K.E.; Vettorazzi, E.; Riethdorf, S.; Yekebas, E.F.; Izbicki, J.R.; Pantel, K. Disseminated tumor cells in bone marrow and the natural course of resected esophageal cancer. Ann. Surg. 2012, 255, 1105–1112. [Google Scholar] [CrossRef]
- Macadam, R.; Sarela, A.; Wilson, J.; MacLennan, K.; Guillou, P. Bone marrow micrometastases predict early post-operative recurrence following surgical resection of oesophageal and gastric carcinoma. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2003, 29, 450–454. [Google Scholar] [CrossRef]
- Konczalla, L.; Ghadban, T.; Effenberger, K.E.; Wöstemeier, A.; Riethdorf, S.; Uzunoglu, F.G.; Izbicki, J.R.; Pantel, K.; Bockhorn, M.; Reeh, M. Prospective Comparison of the Prognostic Relevance of Circulating Tumor Cells in Blood and Disseminated Tumor Cells in Bone Marrow of a Single Patient’s Cohort With Esophageal Cancer. Ann. Surg. 2019. [Google Scholar] [CrossRef]
- Ryan, P.; Furlong, H.; Murphy, C.G.; O’Sullivan, F.; Walsh, T.N.; Shanahan, F.; O’Sullivan, G.C. Prognostic significance of prospectively detected bone marrow micrometastases in esophagogastric cancer: 10-year follow-up confirms prognostic significance. Cancer Med. 2015, 4, 1281–1288. [Google Scholar] [CrossRef]
- Pantel, K.; Alix-Panabières, C. Bone marrow as a reservoir for disseminated tumor cells: A special source for liquid biopsy in cancer patients. BoneKEy Rep. 2014, 3, 584. [Google Scholar] [CrossRef]
- Martini, N.; Flehinger, B.J.; Zaman, M.B.; Beattie, E.J. Results of resection in non-oat cell carcinoma of the lung with mediastinal lymph node metastases. Ann. Surg. 1983, 198, 386–397. [Google Scholar] [CrossRef]
- Casson, A.G.; Rusch, V.W.; Ginsberg, R.J.; Zankowicz, N.; Finley, R.J. Lymph node mapping of esophageal cancer. Ann. Thorac. Surg. 1994, 58, 1569–1570. [Google Scholar] [CrossRef]
- Raymond, W.A.; Leong, A.S. Immunoperoxidase staining in the detection of lymph node metastases in stage I breast cancer. Pathology (Phila) 1989, 21, 11–15. [Google Scholar] [CrossRef]
- Passlick, B.; Izbicki, J.R.; Kubuschok, B.; Nathrath, W.; Thetter, O.; Pichlmeier, U.; Schweiberer, L.; Riethmüller, G.; Pantel, K. Immunohistochemical assessment of individual tumor cells in lymph nodes of patients with non-small-cell lung cancer. J. Clin. Oncol. 2016. [Google Scholar] [CrossRef]
- Pantel, K.; Schlimok, G.; Angstwurm, M.; Weckermann, D.; Schmaus, W.; Gath, H.; Passlick, B.; Izbicki, J.R.; Riethmüller, G. Methodological analysis of immunocytochemical screening for disseminated epithelial tumor cells in bone marrow. J. Hematother. 1994, 3, 165–173. [Google Scholar] [CrossRef]
- Prenzel, K.; Bollschweiler, E.; Schröder, W.; Mönig, S.P.; Drebber, U.; Vallboehmer, D.; Hölscher, A.H. Prognostic Relevance of Skip Metastases in Esophageal Cancer. Ann. Thorac. Surg. 2010, 90, 1662–1667. [Google Scholar] [CrossRef]
- Waterman, T.A.; Hagen, J.A.; Peters, J.H.; DeMeester, S.R.; Taylor, C.R.; Demeester, T.R. The prognostic importance of immunohistochemically detected node metastases in resected esophageal adenocarcinoma. Ann. Thorac. Surg. 2004, 78, 1161–1169. [Google Scholar] [CrossRef]
- Kaifi, J.T.; Yekebas, E.F.; Schurr, P.; Obonyo, D.; Wachowiak, R.; Busch, P.; Heinecke, A.; Pantel, K.; Izbicki, J.R. Tumor-cell homing to lymph nodes and bone marrow and CXCR4 expression in esophageal cancer. J. Natl. Cancer Inst. 2005, 97, 1840–1847. [Google Scholar] [CrossRef]
- Fehm, D.M.T.; Braun, S.; Müller, V.; Janni, W.; Gebauer, G.; Marth, C.; Schindlbeck, C.; Wallwiener, D.; Borgen, E.; Naume, B.; et al. A concept for the standardized detection of disseminated tumor cells in bone marrow from patients with primary breast cancer and its clinical implementation. Cancer 2006, 107, 885–892. [Google Scholar] [CrossRef]
- MacGuill, M.J.; Barrett, C.; Ravi, N.; MacDonald, G.; Reynolds, J.V. Isolated tumour cells in pathological node-negative lymph nodes adversely affect prognosis in cancer of the oesophagus or oesophagogastric junction. J. Clin. Pathol. 2007, 60, 1108–1111. [Google Scholar] [CrossRef]
- Schurr, P.G.; Yekebas, E.F.; Kaifi, J.T.; Lasch, S.; Strate, T.; Kutup, A.; Cataldegirmen, G.; Bubenheim, M.; Pantel, K.; Izbicki, J.R. Lymphatic spread and microinvolvement in adenocarcinoma of the esophago-gastric junction. J. Surg. Oncol. 2006, 94, 307–315. [Google Scholar] [CrossRef]
- Vazquez-Sequeiros, E.; Wang, L.; Burgart, L.; Harmsen, W.; Zinsmeister, A.; Allen, M.; Jondal, M.; Wiersema, M.J. Occult lymph node metastases as a predictor of tumor relapse in patients with node-negative esophageal carcinoma. Gastroenterology 2002, 122, 1815–1821. [Google Scholar] [CrossRef]
- Morimoto, J.; Tanaka, H.; Ohira, M.; Kubo, N.; Muguruma, K.; Sakurai, K.; Yamashita, Y.; Maeda, K.; Sawada, T.; Hirakawa, K. The impact of the number of occult metastatic lymph nodes on postoperative relapse of resectable esophageal cancer. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2014, 27, 63–71. [Google Scholar] [CrossRef]
- Komukai, S.; Nishimaki, T.; Watanabe, H.; Ajioka, Y.; Suzuki, T.; Hatakeyama, K. Significance of immunohistochemically demonstrated micrometastases to lymph nodes in esophageal cancer with histologically negative nodes. Surgery 2000, 127, 40–46. [Google Scholar] [CrossRef]
- Zheng, B.; Ni, C.-H.; Chen, H.; Wu, W.-D.; Guo, Z.-H.; Zhu, Y.; Zheng, W.; Chen, C. New evidence guiding extent of lymphadenectomy for esophagogastric junction tumor: Application of Ber-Ep4 Joint with CD44v6 staining on the detection of lower mediastinal lymph node micrometastasis and survival analysis. Medicine (Baltimore) 2017, 96, e6533. [Google Scholar] [CrossRef]
- Zhang, X.; Chen, S.-B.; Chen, J.-X.; Wen, J.; Yang, H.; Xie, M.-R.; Zhang, Y.; Hu, Y.-Z.; Lin, P. CK19 mRNA expression in the bone marrow of patients with esophageal squamous cell carcinoma and its clinical significance. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2010, 23, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Thorban, S.; Rosenberg, R.; Busch, R.; Roder, R.J. Epithelial cells in bone marrow of oesophageal cancer patients: A significant prognostic factor in multivariate analysis. Br. J. Cancer 2000, 83, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Gray, R.T.; O’Donnell, M.E.; Verghis, R.M.; McCluggage, W.G.; Maxwell, P.; McGuigan, J.A.; Spence, G.M. Bone marrow micrometastases in esophageal carcinoma: A 10-year follow-up study. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2012, 25, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Aoyama, J.; Kawakubo, H.; Mayanagi, S.; Fukuda, K.; Irino, T.; Nakamura, R.; Wada, N.; Suzuki, T.; Kameyama, K.; Kitagawa, Y. Discrepancy Between the Clinical and Final Pathological Findings of Lymph Node Metastasis in Superficial Esophageal Cancer. Ann. Surg. Oncol. 2019, 26, 2874–2881. [Google Scholar] [CrossRef] [PubMed]
- Zingg, U.; Montani, M.; Busch, M.; Metzger, U.; Went, P.; Oertli, D. Prognostic influence of immunohistochemically detected lymph node micrometastasis and histological subtype in pN0 oesophageal cancer. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2009, 35, 593–599. [Google Scholar] [CrossRef]
- Parkinson, D.R.; Dracopoli, N.; Petty, B.G.; Compton, C.; Cristofanilli, M.; Deisseroth, A.; Hayes, D.F.; Kapke, G.F.; Kumar, P.; Lee, J.; et al. Considerations in the development of circulating tumor cell technology for clinical use. J. Transl. Med. 2012, 10, 138. [Google Scholar] [CrossRef]
- Joosse, S.A.; Hannemann, J.; Spötter, J.; Bauche, A.; Andreas, A.; Müller, V.; Pantel, K. Changes in keratin expression during metastatic progression of breast cancer: Impact on the detection of circulating tumor cells. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2012, 18, 993–1003. [Google Scholar] [CrossRef]
- Stoecklein, N.H.; Hosch, S.B.; Bezler, M.; Stern, F.; Hartmann, C.H.; Vay, C.; Siegmund, A.; Scheunemann, P.; Schurr, P.; Knoefel, W.T.; et al. Direct genetic analysis of single disseminated cancer cells for prediction of outcome and therapy selection in esophageal cancer. Cancer Cell 2008, 13, 441–453. [Google Scholar] [CrossRef]
- Pantel, K.; Brakenhoff, R.H.; Brandt, B. Detection, clinical relevance and specific biological properties of disseminating tumour cells. Nat. Rev. Cancer 2008, 8, 329–340. [Google Scholar] [CrossRef]
- Braun, S.; Pantel, K.; Müller, P.; Janni, W.; Hepp, F.; Kentenich, C.R.; Gastroph, S.; Wischnik, A.; Dimpfl, T.; Kindermann, G.; et al. Cytokeratin-positive cells in the bone marrow and survival of patients with stage I, II, or III breast cancer. N. Engl. J. Med. 2000, 342, 525–533. [Google Scholar] [CrossRef]
- Bostick, P.J.; Chatterjee, S.; Chi, D.D.; Huynh, K.T.; E Giuliano, A.; Cote, R.; Hoon, D. Limitations of specific reverse-transcriptase polymerase chain reaction markers in the detection of metastases in the lymph nodes and blood of breast cancer patients. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1998, 16, 2632–2640. [Google Scholar] [CrossRef] [PubMed]
- Zippelius, A.; Kufer, P.; Honold, G.; Köllermann, M.W.; Oberneder, R.; Schlimok, G.; Riethmüller, G.; Pantel, K. Limitations of reverse-transcriptase polymerase chain reaction analyses for detection of micrometastatic epithelial cancer cells in bone marrow. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1997, 15, 2701–2708. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, G.C.; Sheehan, D.; Clarke, A.; Stuart, R.; Kelly, J.; Kiely, M.D.; Walsh, T.; Collins, J.K.; Shanahan, F. Micrometastases in esophagogastric cancer: High detection rate in resected rib segments. Gastroenterology 1999, 116, 543–548. [Google Scholar] [CrossRef]
- Bonavina, L.; Soligo, D.; Quirici, N.; Bossolasco, P.; Cesana, B.; Deliliers, G.L.; Peracchia, A. Bone marrow-disseminated tumor cells in patients with carcinoma of the esophagus or cardia. Surgery 2001, 129, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, S.; D’Ovidio, F.; Tazzari, P.; Pilotti, V.; Daddi, N.; Bandini, G.; Piccioli, M.; Pileri, S. Iliac crest biopsy versus rib segment resection for the detection of bone marrow isolated tumor cells from lung and esophageal cancer. Eur. J. Cardio Thorac. Surg. Off. J. Eur. Assoc. Cardio Thorac. Surg. 2001, 19, 576–579. [Google Scholar] [CrossRef][Green Version]
- Yanagi, M.; Sasaki, K.; Uchikado, Y.; Omoto, I.; Arigami, T.; Kurahara, H.; Uenosono, Y.; Sakoda, M.; Maemura, K.; Natsugoe, S. Effect of Neoadjuvant Chemoradiotherapy on Lymph Node Micrometastases in Thoracic Esophageal Cancer. Anticancer Res. 2018, 38, 893–900. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | All | LNMM and BNMM Negative | LNMM Positive and BNMM Negative | p Value | LNMM Negative and BNMM Positive | p Value | LNMM and BNMM Positive | p Value |
|---|---|---|---|---|---|---|---|---|
| Patients | 110 (100.0%) | 41 (37.3%) | 15 (13.6%) | n.a. | 31 (28.2%) | n.a. | 23 (20.9%) | n.a. |
| Age (years) | ||||||||
| ≤60 | 53 (48.2%) | 21 (51.2%) | 8 (53.3%) | 0.999 | 13 (41.9%) | 0.868 | 11 (47.8%) | 0.994 |
| >60 | 57 (51.8%) | 20 (48.8%) | 7 (46.7%) | 18 (58.1%) | 12 (52.2%) | |||
| Sex | ||||||||
| Male | 83 (75.5%) | 33 (80.5%) | 9 (60.0%) | 0.398 | 22 (71.0%) | 0.790 | 19 (82.6%) | 0.998 |
| Female | 27 (24.5%) | 8 (19.5%) | 6 (40.0%) | 9 (29.0%) | 4 (17.4%) | |||
| pT category | ||||||||
| pT1 | 24 (21.8%) | 13 (31.7%) | 2 (13.3%) | 0.112 | 8 (25.8%) | 0.938 | 1 (4.3%) | 0.017 |
| pT2 | 35 (31.8%) | 13 (31.7%) | 3 (20.0%) | 12 (38.7%) | 7 (30.4%) | |||
| pT3 | 37 (33.6%) | 13 (31.7%) | 7 (46.7%) | 7 (22.6%) | 10 (43.5%) | |||
| pT4 | 14 (12.7%) | 2 (4.9%) | 3 (20.0%) | 4 (12.9%) | 5 (21.7%) | |||
| UICC stage | ||||||||
| I | 24 (21.8%) | 13 (31.7%) | 2 (13.3%) | 0.175 | 8 (25.8%) | 0.975 | 1 (4.3%) | 0.011 |
| II | 72 (65.5%) | 28 (63.4%) | 10 (66.7%) | 19 (61.3%) | 17 (73.9%) | |||
| III | 14 (12.7%) | 2 (4.9%) | 3 (20.0%) | 4 (12.9%) | 5 (21.7%) | |||
| Grading | ||||||||
| G1 | 11 (10.0%) | 6 (14.6%) | 1 (6.7%) | 0.516 | 2 (6.5%) | 0.988 | 2 (8.7%) | 0.970 |
| G2 | 65 (59.1%) | 23 (56.1%) | 7 (46.7%) | 21 (67.7%) | 14 (60.9%) | |||
| G3 | 34 (30.9%) | 12 (29.3%) | 7 (46.7%) | 8 (25.8%) | 7 (30.4%) | |||
| Histology | 0.351 | |||||||
| AC | 66 (60.0%) | 20 (48.8%) | 13 (86.7%) | 0.050 | 17 (54.8%) | 0.952 | 16 (69.6%) | |
| SCC | 44 (40.0%) | 21 (51.2%) | 2 (13.3%) | 14 (45.2%) | 7 (30.4%) | |||
| Recurrence | ||||||||
| Negative | 71 (64.5%) | 34 (82.9%) | 8 (53.3%) | 0.113 | 23 (74.2%) | 0.832 | 6 (26.1%) | <0.001 |
| Positive | 39 (35.5%) | 7 (17.1%) | 7 (46.7%) | 8 (25.8%) | 17 (73.9%) | |||
| Survival | ||||||||
| Alive | 85 (77.3%) | 37 (90.2%) | 11 (73.3%) | 0.489 | 26 (83.9%) | 0.905 | 11 (47.8%) | <0.001 |
| Deceased | 25 (22.7%) | 4 (9.8%) | 4 (26.7%) | 5 (16.1%) | 12 (52.2%) | |||
| Variables | BNMM | p Value | |
|---|---|---|---|
| Negative | Positive | ||
| LNMM | |||
| Negative | 41 (73.2%) | 31 (57.4%) | 0.109 |
| Positive | 15 (26.8%) | 23 (42.6%) | |
| Skip metastases | |||
| Negative | 50 (89.3%) | 41 (75.9%) | 0.080 |
| Positive | 6 (10.7%) | 13 (24.1%) | |
| Lymph node ratio | |||
| <10% | 49 (87.5%) | 36 (66.7%) | 0.012 |
| ≥10% | 7 (12.5%) | 18 (33.3%) | |
| Variables | OR | 95% CI | p Value |
|---|---|---|---|
| Age | 1.011 | 0.963–1.062 | 0.778 |
| pT category | 1.284 | 0.440–3.742 | 0.647 |
| UICC stage | 2.144 | 0.366–12.201 | 0.403 |
| Grading | 1.347 | 0.610–2.975 | 0.461 |
| Skip metastases | 7.953 | 2.376–26.617 | 0.001 |
| Lymph node ratio | 1.204 | 0.246–5.887 | 0.819 |
| LNMM/BNMM status | 1.925 | 1.126–3.289 | 0.017 |
| Variables | OR | 95% CI | p Value |
|---|---|---|---|
| Age | 0.991 | 0.952–1.031 | 0.642 |
| pT category | 1.319 | 0.560–3.103 | 0.527 |
| UICC stage | 2.119 | 0.524–8.580 | 0.292 |
| Grading | 1.092 | 0.597–1.997 | 0.775 |
| Skip metastases | 3.702 | 1.297–10.571 | 0.014 |
| Lymph node ratio | 2.686 | 0.758–9.524 | 0.126 |
| LNMM/BNMM status | 1.624 | 1.085–2.431 | 0.019 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karstens, K.-F.; Ghadban, T.; Effenberger, K.; Sauter, G.; Pantel, K.; Izbicki, J.R.; Vashist, Y.; König, A.; Reeh, M. Lymph Node and Bone Marrow Micrometastases Define the Prognosis of Patients with pN0 Esophageal Cancer. Cancers 2020, 12, 588. https://doi.org/10.3390/cancers12030588
Karstens K-F, Ghadban T, Effenberger K, Sauter G, Pantel K, Izbicki JR, Vashist Y, König A, Reeh M. Lymph Node and Bone Marrow Micrometastases Define the Prognosis of Patients with pN0 Esophageal Cancer. Cancers. 2020; 12(3):588. https://doi.org/10.3390/cancers12030588
Chicago/Turabian StyleKarstens, Karl-F., Tarik Ghadban, Katharina Effenberger, Guido Sauter, Klaus Pantel, Jakob R. Izbicki, Yogesh Vashist, Alexandra König, and Matthias Reeh. 2020. "Lymph Node and Bone Marrow Micrometastases Define the Prognosis of Patients with pN0 Esophageal Cancer" Cancers 12, no. 3: 588. https://doi.org/10.3390/cancers12030588
APA StyleKarstens, K.-F., Ghadban, T., Effenberger, K., Sauter, G., Pantel, K., Izbicki, J. R., Vashist, Y., König, A., & Reeh, M. (2020). Lymph Node and Bone Marrow Micrometastases Define the Prognosis of Patients with pN0 Esophageal Cancer. Cancers, 12(3), 588. https://doi.org/10.3390/cancers12030588