The Current Status of Immune Checkpoint Inhibitors in Neuro-Oncology: A Systematic Review

 , , , and
, , , and
Abstract
1. Introduction
2. Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction and Statistical Analysis
3. Results
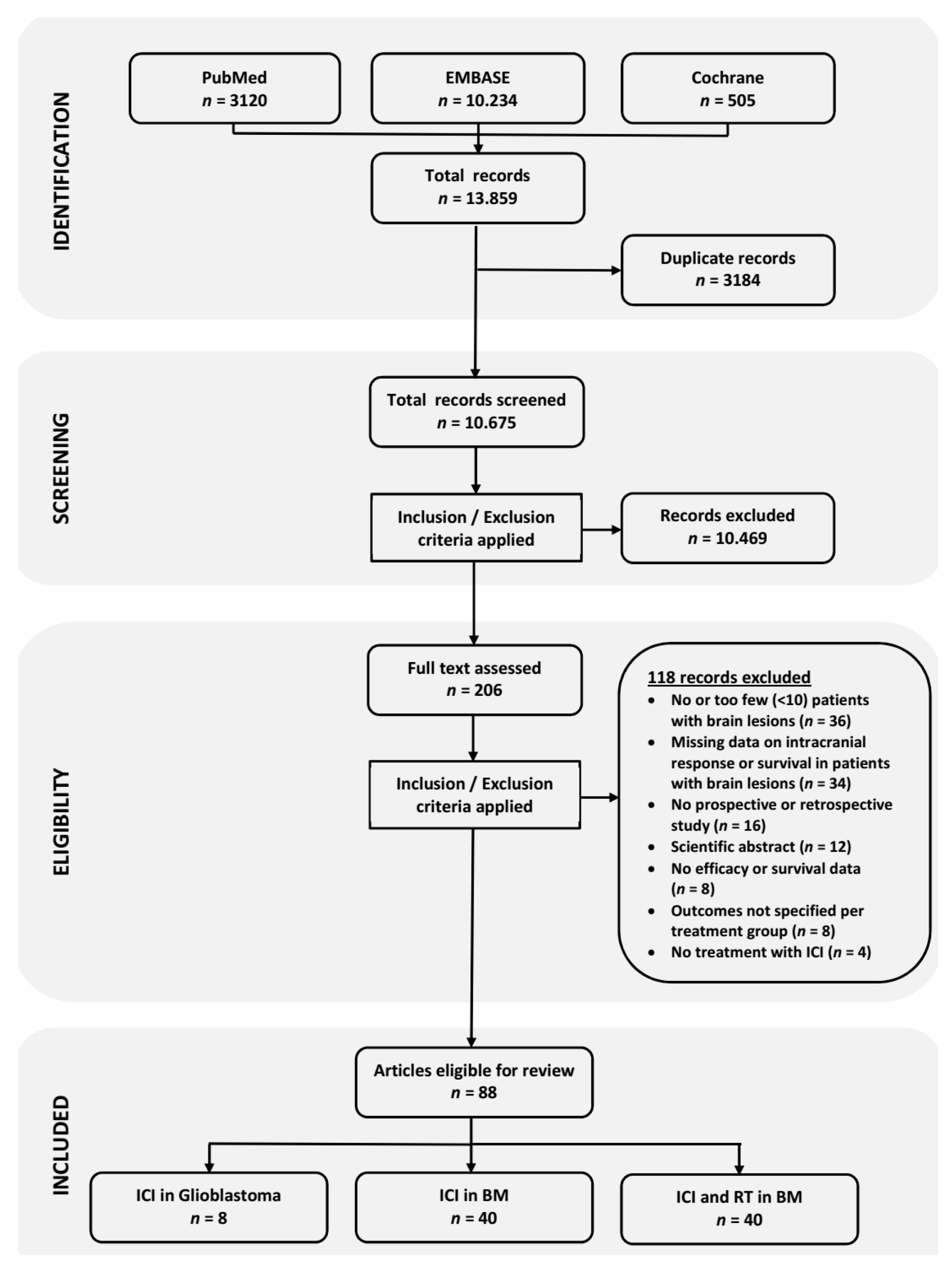
3.1. Literature Search Results
3.2. Overview of the Studies
3.3. Immune Checkpoint Inhibitors in Glioblastoma
3.4. Outcomes of Immune Checkpoint Inhibitors in Brain Metastases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Omidi, Y.; Barar, J. Impacts of blood-brain barrier in drug delivery and targeting of brain tumors. BioImpacts BI 2012, 2, 5–22. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Stupp, R.; Taillibert, S.; Kanner, A.; Read, W.; Steinberg, D.; Lhermitte, B.; Toms, S.; Idbaih, A.; Ahluwalia, M.S.; Fink, K.; et al. Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs Maintenance Temozolomide Alone on Survival in Patients with Glioblastoma: A Randomized Clinical Trial. Jama 2017, 318, 2306–2316. [Google Scholar] [CrossRef] [PubMed]
- Almeida, J.P.; Chaichana, K.L.; Rincon-Torroella, J.; Quinones-Hinojosa, A. The value of extent of resection of glioblastomas: Clinical evidence and current approach. Curr. Neurol. Neurosci Rep. 2015, 15, 517. [Google Scholar] [CrossRef]
- Romanelli, P.; Conti, A.; Pontoriero, A.; Ricciardi, G.K.; Tomasello, F.; De Renzis, C.; Innocenzi, G.; Esposito, V.; Cantore, G. Role of stereotactic radiosurgery and fractionated stereotactic radiotherapy for the treatment of recurrent glioblastoma multiforme. Neurosurg Focus 2009, 27, E8. [Google Scholar] [CrossRef]
- De Witt Hamer, P.C. Small molecule kinase inhibitors in glioblastoma: A systematic review of clinical studies. Neuro. Oncol. 2010, 12, 304–316. [Google Scholar] [CrossRef]
- Schouten, L.J.; Rutten, J.; Huveneers, H.A.; Twijnstra, A. Incidence of brain metastases in a cohort of patients with carcinoma of the breast, colon, kidney, and lung and melanoma. Cancer 2002, 94, 2698–2705. [Google Scholar] [CrossRef]
- Barnholtz-Sloan, J.S.; Sloan, A.E.; Davis, F.G.; Vigneau, F.D.; Lai, P.; Sawaya, R.E. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J. Clin. Oncol. 2004, 22, 2865–2872. [Google Scholar] [CrossRef]
- Cagney, D.N.; Martin, A.M.; Catalano, P.J.; Redig, A.J.; Lin, N.U.; Lee, E.Q.; Wen, P.Y.; Dunn, I.F.; Bi, W.L.; Weiss, S.E.; et al. Incidence and prognosis of patients with brain metastases at diagnosis of systemic malignancy: A population-based study. Neuro. Oncol. 2017, 19, 1511–1521. [Google Scholar] [CrossRef]
- Bafaloukos, D.; Gogas, H. The treatment of brain metastases in melanoma patients. Cancer Treat. Rev. 2004, 30, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Keir, M.E.; Butte, M.J.; Freeman, G.J.; Sharpe, A.H. PD-1 and its ligands in tolerance and immunity. Annu. Rev. Immunol. 2008, 26, 677–704. [Google Scholar] [CrossRef] [PubMed]
- Bour-Jordan, H.; Esensten, J.H.; Martinez-Llordella, M.; Penaranda, C.; Stumpf, M.; Bluestone, J.A. Intrinsic and extrinsic control of peripheral T-cell tolerance by costimulatory molecules of the CD28/ B7 family. Immunol. Rev. 2011, 241, 180–205. [Google Scholar] [CrossRef] [PubMed]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Perez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; Ahn, M.J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Tykodi, S.S.; Chow, L.Q.; Hwu, W.J.; Topalian, S.L.; Hwu, P.; Drake, C.G.; Camacho, L.H.; Kauh, J.; Odunsi, K.; et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N. Engl. J. Med. 2012, 366, 2455–2465. [Google Scholar] [CrossRef]
- Omuro, A.; Vlahovic, G.; Lim, M.; Sahebjam, S.; Baehring, J.; Cloughesy, T.F.; Voloschin, A.; Ramkissoon, S.H.; Ligon, K.L.; Latek, R.; et al. Nivolumab with or without ipilimumab in patients with recurrent glioblastoma: Results from exploratory phase i cohorts of CheckMate 143. Neuro-Oncol. 2018, 20, 674–686. [Google Scholar] [CrossRef]
- Lukas, R.V.; Rodon, J.; Becker, K.; Wong, E.T.; Shih, K.; Touat, M.; Fasso, M.; Osborne, S.; Molinero, L.; O’Hear, C.; et al. Clinical activity and safety of atezolizumab in patients with recurrent glioblastoma. J. Neurooncol. 2018, 140, 317–328. [Google Scholar] [CrossRef]
- Cloughesy, T.F.; Mochizuki, A.Y.; Orpilla, J.R.; Hugo, W.; Lee, A.H.; Davidson, T.B.; Wang, A.C.; Ellingson, B.M.; Rytlewski, J.A.; Sanders, C.M.; et al. Neoadjuvant anti-PD-1 immunotherapy promotes a survival benefit with intratumoral and systemic immune responses in recurrent glioblastoma. Nat. Med. 2019, 25, 477–486. [Google Scholar] [CrossRef]
- Schalper, K.A.; Rodriguez-Ruiz, M.E.; Diez-Valle, R.; Lopez-Janeiro, A.; Porciuncula, A.; Idoate, M.A.; Inoges, S.; de Andrea, C.; Lopez-Diaz de Cerio, A.; Tejada, S.; et al. Neoadjuvant nivolumab modifies the tumor immune microenvironment in resectable glioblastoma. Nat. Med. 2019, 25, 470–476. [Google Scholar] [CrossRef]
- Carter, T.; Shaw, H.; Cohn-Brown, D.; Chester, K.; Mulholland, P. Ipilimumab and Bevacizumab in Glioblastoma. Clin. Oncol. (R Coll Radiol) 2016, 28, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, D.T.; Yalon, M.; Vainer, G.W.; Lossos, A.; Yust, S.; Tzach, L.; Cagnano, E.; Limon, D.; Bokstein, F. Pembrolizumab: First experience with recurrent primary central nervous system (CNS) tumors. J. Neurooncol. 2016, 129, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, M.C.; Kim, B.T. Nivolumab for patients with recurrent glioblastoma progressing on bevacizumab: A retrospective case series. J. Neurooncol. 2017, 133, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Mantica, M.; Pritchard, A.; Lieberman, F.; Drappatz, J. Retrospective study of nivolumab for patients with recurrent high grade gliomas. J. Neurooncol. 2018, 139, 625–631. [Google Scholar] [CrossRef]
- Altomonte, M.; Di Giacomo, A.M.; Queirolo, P.; Ascierto, P.A.; Spagnolo, F.; Bajetta, E.; Calabrò, L.; Danielli, R.; De Rosa, F.; Maur, M.; et al. Clinical experience with ipilimumab 10 mg/kg in patients with melanoma treated at Italian centres as part of a European expanded access programme. J. Exp. Clin. Cancer Res. 2013, 32, 82. [Google Scholar] [CrossRef]
- Berrocal, A.; Arance, A.; Martin, J.A.L.; Soriano, V.; Muñoz, E.; Alonso, L.; Espinosa, E.; Criado, P.L.; Valdivia, J.; Algarra, S.M. Ipilimumab for advanced melanoma: Experience from the Spanish Expanded Access Program. Melanoma Res. 2014, 24, 577–583. [Google Scholar] [CrossRef]
- Bjørnhart, B.; Hansen, K.H.; Jørgensen, T.L.; Herrstedt, J.; Schytte, T. Efficacy and safety of immune checkpoint inhibitors in a Danish real life non-small cell lung cancer population: A retrospective cohort study. Acta Oncologica. 2019, 58, 953–961. [Google Scholar] [CrossRef]
- Chasset, F.; Pages, C.; Biard, L.; Roux, J.; Sidina, I.; Madelaine, I.; Basset-Seguin, N.; Viguier, M.; Madjlessi-Ezr, A.N.; Schneider, P.; et al. Single-center study under a French Temporary Authorization for Use (TAU) protocol for ipilimumab in metastatic melanoma: Negative impact of baseline corticosteroids. Eur. J. Dermatol. 2015, 25, 36–44. [Google Scholar] [CrossRef]
- Crino, L.; Bronte, G.; Bidoli, P.; Cravero, P.; Minenza, E.; Cortesi, E.; Garassino, M.C.; Proto, C.; Cappuzzo, F.; Grossi, F.; et al. Nivolumab and brain metastases in patients with advanced non-squamous non-small cell lung cancer. Lung Cancer 2019, 129, 35–40. [Google Scholar] [CrossRef]
- Di Giacomo, A.M.; Ascierto, P.A.; Pilla, L.; Santinami, M.; Ferrucci, P.F.; Giannarelli, D.; Marasco, A.; Rivoltini, L.; Simeone, E.; Nicoletti, S.V.; et al. Ipilimumab and fotemustine in patients with advanced melanoma (NIBIT-M1): An open-label, single-arm phase 2 trial. Lancet Oncol. 2012, 13, 879–886. [Google Scholar] [CrossRef]
- Di Giacomo, A.M.; Ascierto, P.A.; Queirolo, P.; Pilla, L.; Ridolfi, R.; Santinami, M.; Testori, A.; Simeone, E.; Guidoboni, M.; Maurichi, A.; et al. Three-year follow-up of advanced melanoma patients who received ipilimumab plus fotemustine in the Italian Network for Tumor Biotherapy (NIBIT)-M1 phase II study. Ann. Oncol. 2015, 26, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Dumenil, C.; Massiani, M.A.; Dumoulin, J.; Giraud, V.; Labrune, S.; Chinet, T.; Giroux Leprieur, E. Clinical factors associated with early progression and grade 3-4 toxicity in patients with advanced non-small-cell lung cancers treated with nivolumab. PLoS ONE 2018, 13, e0195945. [Google Scholar] [CrossRef]
- Flippot, R.; Dalban, C.; Laguerre, B.; Borchiellini, D.; Gravis, G.; Negrier, S.; Chevreau, C.; Joly, F.; Geoffrois, L.; Ladoire, S.; et al. Safety and Efficacy of Nivolumab in Brain Metastases from Renal Cell Carcinoma: Results of the GETUG-AFU 26 NIVOREN Multicenter Phase II Study. J. Clin. Oncol. 2019, 37, 2008–2016. [Google Scholar] [CrossRef] [PubMed]
- Garde-Noguera, J.; Martorell, P.M.; De Julian, M.; Altozano, J.P.; Coloma, C.S.; Sanchez, J.G.; Molla, A.I.; Martin, M.; Rubio, X.M.; Liebana, S.M.; et al. Predictive and prognostic clinical and pathological factors of nivolumab efficacy in non-small-cell lung cancer patients. Clin. Transl. Oncol. 2018, 20, 1072–1079. [Google Scholar] [CrossRef] [PubMed]
- Gauvain, C.; Vauléon, E.; Chouaid, C.; Lerhun, E.; Jabot, L.; Scherpereel, A.; Vinas, F.; Cortot, A.B.; Monnet, I. Intracerebral efficacy and tolerance of nivolumab in non–small-cell lung cancer patients with brain metastases. Lung Cancer 2018, 116, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, S.B.; Gettinger, S.N.; Mahajan, A.; Chiang, A.C.; Herbst, R.S.; Sznol, M.; Tsiouris, A.J.; Cohen, J.; Vortmeyer, A.; Jilaveanu, L.; et al. Pembrolizumab for patients with melanoma or non-small-cell lung cancer and untreated brain metastases: Early analysis of a non-randomised, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 976–983. [Google Scholar] [CrossRef]
- Gonzalez-Cao, M.; Arance, A.; Piulats, J.M.; Marquez-Rodas, I.; Manzano, J.L.; Berrocal, A.; Crespo, G.; Rodriguez, D.; Perez-Ruiz, E.; Berciano, M.; et al. Pembrolizumab for advanced melanoma: Experience from the Spanish Expanded Access Program. Clin. Transl. Oncol. 2017, 19, 761–768. [Google Scholar] [CrossRef]
- Kluger, H.M.; Chiang, V.; Mahajan, A.; Zito, C.R.; Sznol, M.; Tran, T.; Weiss, S.A.; Cohen, J.V.; Yu, J.; Hegde, U.; et al. Long-Term Survival of Patients with Melanoma with Active Brain Metastases Treated With Pembrolizumab on a Phase II Trial. J. Clin. Oncol. 2019, 37, 52–60. [Google Scholar] [CrossRef]
- Konstantinou, M.P.; Dutriaux, C.; Gaudy-Marqueste, C.; Mortier, L.; Bedane, C.; Girard, C.; Thellier, S.; Jouary, T.; Grob, J.J.; Richard, M.A.; et al. Ipilimumab in melanoma patients with brain metastasis: A retro-spective multicentre evaluation of thirty-eight patients. Acta Derm. Venereol. 2014, 94, 45–49. [Google Scholar] [CrossRef]
- Long, G.V.; Atkinson, V.; Lo, S.; Sandhu, S.; Guminski, A.D.; Brown, M.P.; Wilmott, J.S.; Edwards, J.; Gonzalez, M.; Scolyer, R.A.; et al. Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: A multicentre randomised phase 2 study. Lancet Oncol. 2018, 19, 672–681. [Google Scholar] [CrossRef]
- Margolin, K.; Ernstoff, M.S.; Hamid, O.; Lawrence, D.; McDermott, D.; Puzanov, I.; Wolchok, J.D.; Clark, J.I.; Sznol, M.; Logan, T.F.; et al. Ipilimumab in patients with melanoma and brain metastases: An open-label, phase 2 trial. Lancet Oncol. 2012, 13, 459–465. [Google Scholar] [CrossRef]
- Parakh, S.; Randhawa, M.; Nguyen, B.; Warburton, L.; Hussain, M.A.; Cebon, J.; Millward, M.; Yip, D.; Ali, S. Real-world efficacy and toxicity of combined nivolumab and ipilimumab in patients with metastatic melanoma. Asia Pac. J. Clin. Oncol 2019, 15, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Parakh, S.; Park, J.J.; Mendis, S.; Rai, R.; Xu, W.; Lo, S.; Drummond, M.; Rowe, C.; Wong, A.; McArthur, G.; et al. Efficacy of anti-PD-1 therapy in patients with melanoma brain metastases. Br. J. Cancer 2017, 116, 1558–1563. [Google Scholar] [CrossRef] [PubMed]
- Queirolo, P.; Spagnolo, F.; Ascierto, P.A.; Simeone, E.; Marchetti, P.; Scoppola, A.; Del Vecchio, M.; Di Guardo, L.; Maio, M.; Di Giacomo, A.M.; et al. Efficacy and safety of ipilimumab in patients with advanced melanoma and brain metastases. J. Neurooncol. 2014, 118, 109–116. [Google Scholar] [CrossRef]
- Sternberg, C.N.; Loriot, Y.; James, N.; Choy, E.; Castellano, D.; Lopez-Rios, F.; Banna, G.L.; De Giorgi, U.; Masini, C.; Bamias, A.; et al. Primary Results from SAUL, a Multinational Single-arm Safety Study of Atezolizumab Therapy for Locally Advanced or Metastatic Urothelial or Nonurothelial Carcinoma of the Urinary Tract. Eur. Urol. 2019, 76, 73–81. [Google Scholar] [CrossRef]
- Weber, J.S.; Amin, A.; Minor, D.; Siegel, J.; Berman, D.; O’Day, S.J. Safety and clinical activity of ipilimumab in melanoma patients with brain metastases: Retrospective analysis of data from a phase 2 trial. Melanoma Res. 2011, 21, 530–534. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Forsyth, P.A.; Algazi, A.; Hamid, O.; Hodi, F.S.; Moschos, S.J.; Khushalani, N.I.; Lewis, K.; Lao, C.D.; Postow, M.A.; et al. Combined Nivolumab and Ipilimumab in Melanoma Metastatic to the Brain. N. Engl. J. Med. 2018, 379, 722–730. [Google Scholar] [CrossRef]
- Alexander, M.; Mellor, J.D.; McArthur, G.; Kee, D. Ipilimumab in pretreated patients with unresectable or metastatic cutaneous, uveal and mucosal melanoma. Med. J. Aust. 2014, 201, 49–53. [Google Scholar] [CrossRef]
- Ahmad, S.S.; Qian, W.; Ellis, S.; Mason, E.; Khattak, M.A.; Gupta, A.; Shaw, H.; Quinton, A.; Kovarikova, J.; Thillai, K.; et al. Ipilimumab in the real world: The UK expanded access programme experience in previously treated advanced melanoma patients. Melanoma Res. 2015, 25, 432–442. [Google Scholar] [CrossRef]
- Ascierto, P.A.; Del Vecchio, M.; Robert, C.; Mackiewicz, A.; Chiarion-Sileni, V.; Arance, A.; Lebbe, C.; Bastholt, L.; Hamid, O.; Rutkowski, P.; et al. Ipilimumab 10 mg/kg versus ipilimumab 3 mg/kg in patients with unresectable or metastatic melanoma: A randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2017, 18, 611–622. [Google Scholar] [CrossRef]
- Dagogo-Jack, I.; Lanfranchi, M.; Gainor, J.F.; Giobbie-Hurder, A.; Lawrence, D.P.; Shaw, A.T.; Sullivan, R.J. A Retrospective Analysis of the Efficacy of Pembrolizumab in Melanoma Patients with Brain Metastasis. J. Immunother. 2017, 40, 108–113. [Google Scholar] [CrossRef] [PubMed]
- De Giorgi, U.; Carteni, G.; Giannarelli, D.; Basso, U.; Galli, L.; Cortesi, E.; Caserta, C.; Pignata, S.; Sabbatini, R.; Bearz, A.; et al. Safety and efficacy of nivolumab for metastatic renal cell carcinoma: Real-world results from an expanded access programme. BJU Int. 2019, 123, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Forschner, A.; Eichner, F.; Amaral, T.; Keim, U.; Garbe, C.; Eigentler, T.K. Improvement of overall survival in stage IV melanoma patients during 2011-2014: Analysis of real-world data in 441 patients of the German Central Malignant Melanoma Registry (CMMR). J. Cancer Res. Clin. Oncol. 2017, 143, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Gadgeel, S.M.; Pennell, N.A.; Fidler, M.J.; Halmos, B.; Bonomi, P.; Stevenson, J.; Schneider, B.; Sukari, A.; Ventimiglia, J.; Chen, W.; et al. Phase II Study of Maintenance Pembrolizumab in Patients with Extensive-Stage Small Cell Lung Cancer (SCLC). J. Thorac. Oncol. 2018, 13, 1393–1399. [Google Scholar] [CrossRef]
- Jinga, D.C.; Ciuleanu, T.; Negru, S.; Aldea, C.; Gales, L.; Bacanu, F.; Oprean, C.; Manolache, M.; Zob, D.; Curescu, S.; et al. Effectiveness and safety profile of ipilimumab therapy in previously treated patients with unresectable or metastatic melanoma–The Romanian Patient Access Program. JBUON 2018, 22, 1287–1295. [Google Scholar]
- Juergens, R.A.; Mariano, C.; Jolivet, J.; Finn, N.; Rothenstein, J.; Reaume, M.N.; Faghih, A.; Labbe, C.; Owen, S.; Shepherd, F.A.; et al. Real-world benefit of nivolumab in a Canadian non-small-cell lung cancer cohort. Curr. Oncol. 2018, 25, 384–392. [Google Scholar] [CrossRef]
- Larkin, J.; Minor, D.; D’Angelo, S.; Neyns, B.; Smylie, M.; Miller, W.H., Jr.; Gutzmer, R.; Linette, G.; Chmielowski, B.; Lao, C.D.; et al. Overall Survival in Patients with Advanced Melanoma Who Received Nivolumab Versus Investigator’s Choice Chemotherapy in CheckMate 037: A Randomized, Controlled, Open-Label Phase III Trial. J. Clin. Oncol. 2018, 36, 383–390. [Google Scholar] [CrossRef]
- Mangana, J.; Cheng, P.F.; Kaufmann, C.; Amann, V.C.; Frauchiger, A.L.; Stogner, V.; Held, U.; von Moos, R.; Michielin, O.; Braun, R.P.; et al. Multicenter, real-life experience with checkpoint inhibitors and targeted therapy agents in advanced melanoma patients in Switzerland. Melanoma Res. 2017, 27, 358–368. [Google Scholar] [CrossRef]
- Milsch, L.; Gesierich, A.; Kreft, S.; Livingstone, E.; Zimmer, L.; Goebeler, M.; Schadendorf, D.; Schilling, B. Patterns of disease control and survival in patients with melanoma brain metastases undergoing immune-checkpoint blockade. Eur. J. Cancer 2018, 99, 58–65. [Google Scholar] [CrossRef]
- Spigel, D.R.; Chaft, J.E.; Gettinger, S.; Chao, B.H.; Dirix, L.; Schmid, P.; Chow, L.Q.M.; Hicks, R.J.; Leon, L.; Fredrickson, J.; et al. FIR: Efficacy, Safety, and Biomarker Analysis of a Phase II Open-Label Study of Atezolizumab in PD-L1-Selected Patients with NSCLC. J. Thorac. Oncol. 2018, 13, 1733–1742. [Google Scholar] [CrossRef]
- Schvartsman, G.; Ma, J.; Bassett, R.L., Jr.; Haydu, L.E.; Amaria, R.N.; Hwu, P.; Wong, M.K.; Hwu, W.J.; Diab, A.; Patel, S.P.; et al. Incidence, patterns of progression, and outcomes of preexisting and newly discovered brain metastases during treatment with anti-PD-1 in patients with metastatic melanoma. Cancer 2019, 125, 4193–4202. [Google Scholar] [CrossRef]
- Tamiya, M.; Tamiya, A.; Inoue, T.; Kimura, M.; Kunimasa, K.; Nakahama, K.; Taniguchi, Y.; Shiroyama, T.; Isa, S.I.; Nishino, K.; et al. Metastatic site as a predictor of nivolumab efficacy in patients with advanced non-small cell lung cancer: A retrospective multicenter trial. PLoS ONE 2018, 13, e0192227. [Google Scholar] [CrossRef] [PubMed]
- Vosoughi, E.; Lee, J.M.; Miller, J.R.; Nosrati, M.; Minor, D.R.; Abendroth, R.; Lee, J.W.; Andrews, B.T.; Leng, L.Z.; Wu, M.; et al. Survival and clinical outcomes of patients with melanoma brain metastasis in the era of checkpoint inhibitors and targeted therapies. BMC Cancer 2018, 18, 490. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.X.; Ou, W.; Diede, S.J.; Whitman, E.D. Real-world experience with pembrolizumab in patients with advanced melanoma: A large retrospective observational study. Medicine (Baltimore) 2019, 98, e16542. [Google Scholar] [CrossRef] [PubMed]
- Reardon, D.; Omuro, A.; Brandes, A.; Rieger, J.; Wick, A.; Sepulveda, J.; Phuphanich, S.; De Souza, P.; Ahluwalia, M.; Lim, M. OS10. 3 randomized phase 3 study evaluating the efficacy and safety of nivolumab vs bevacizumab in patients with recurrent glioblastoma: CheckMate 143. Neuro-oncology 2017, 19, iii21. [Google Scholar] [CrossRef]
- Colli, L.M.; Machiela, M.J.; Myers, T.A.; Jessop, L.; Yu, K.; Chanock, S.J. Burden of Nonsynonymous Mutations among TCGA Cancers and Candidate Immune Checkpoint Inhibitor Responses. Cancer Res. 2016, 76, 3767–3772. [Google Scholar] [CrossRef]
- Hodges, T.R.; Ott, M.; Xiu, J.; Gatalica, Z.; Swensen, J.; Zhou, S.; Huse, J.T.; de Groot, J.; Li, S.; Overwijk, W.W.; et al. Mutational burden, immune checkpoint expression, and mismatch repair in glioma: Implications for immune checkpoint immunotherapy. Neuro. Oncol. 2017, 19, 1047–1057. [Google Scholar] [CrossRef]
- Schumacher, T.N.; Schreiber, R.D. Neoantigens in cancer immunotherapy. Science 2015, 348, 69–74. [Google Scholar] [CrossRef]
- Lim, M.; Xia, Y.; Bettegowda, C.; Weller, M. Current state of immunotherapy for glioblastoma. Nat. reviews. Clin. Oncol. 2018, 15, 422–442. [Google Scholar] [CrossRef]
- Berghoff, A.S.; Lassmann, H.; Preusser, M.; Hoftberger, R. Characterization of the inflammatory response to solid cancer metastases in the human brain. Clin. Exp. Metastasis 2013, 30, 69–81. [Google Scholar] [CrossRef]
- Berghoff, A.S.; Fuchs, E.; Ricken, G.; Mlecnik, B.; Bindea, G.; Spanberger, T.; Hackl, M.; Widhalm, G.; Dieckmann, K.; Prayer, D.; et al. Density of tumor-infiltrating lymphocytes correlates with extent of brain edema and overall survival time in patients with brain metastases. Oncoimmunology 2016, 5, e1057388. [Google Scholar] [CrossRef] [PubMed]
- Reardon, D.A.; Neuberg, D.S.; Keskin, D.B.; Tirosh, I.; Anandappa, A.; Mathewson, N.D.; Sun, J.; Shukla, S.A.; Gjini, E.; Li, S. Effect of dexamethasone in glioblastoma (GBM) patients on systemic and intratumoral T-cell responses induced by personalized neoantigen-targeting vaccine. J. Clin. Oncol. 2018, 36, 2020. [Google Scholar] [CrossRef]
- Arbour, K.C.; Mezquita, L.; Long, N.; Rizvi, H.; Auclin, E.; Ni, A.; Martinez-Bernal, G.; Ferrara, R.; Lai, W.V.; Hendriks, L.E.L.; et al. Impact of Baseline Steroids on Efficacy of Programmed Cell Death-1 and Programmed Death-Ligand 1 Blockade in Patients with Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36, 2872–2878. [Google Scholar] [CrossRef] [PubMed]
- Horvat, T.Z.; Adel, N.G.; Dang, T.O.; Momtaz, P.; Postow, M.A.; Callahan, M.K.; Carvajal, R.D.; Dickson, M.A.; D’Angelo, S.P.; Woo, K.M.; et al. Immune-Related Adverse Events, Need for Systemic Immunosuppression, and Effects on Survival and Time to Treatment Failure in Patients With Melanoma Treated with Ipilimumab at Memorial Sloan Kettering Cancer Center. J. Clin. Oncol. 2015, 33, 3193–3198. [Google Scholar] [CrossRef] [PubMed]
- Zagni, C.; Floresta, G.; Monciino, G.; Rescifina, A. The Search for Potent, Small-Molecule HDACIs in Cancer Treatment: A Decade After Vorinostat. Med. Res. Rev. 2017, 37, 1373–1428. [Google Scholar] [CrossRef] [PubMed]
- Briere, D.; Sudhakar, N.; Woods, D.M.; Hallin, J.; Engstrom, L.D.; Aranda, R.; Chiang, H.; Sodre, A.L.; Olson, P.; Weber, J.S.; et al. The class I/IV HDAC inhibitor mocetinostat increases tumor antigen presentation, decreases immune suppressive cell types and augments checkpoint inhibitor therapy. Cancer Immunol. Immunother. CII 2018, 67, 381–392. [Google Scholar] [CrossRef]
- Fukumoto, T.; Fatkhutdinov, N.; Zundell, J.A.; Tcyganov, E.N.; Nacarelli, T.; Karakashev, S.; Wu, S.; Liu, Q.; Gabrilovich, D.I.; Zhang, R. HDAC6 Inhibition Synergizes with Anti-PD-L1 Therapy in ARID1A-Inactivated Ovarian Cancer. Cancer Res. 2019, 79, 5482–5489. [Google Scholar] [CrossRef]
- Chiocca, E.A.; Yu, J.S.; Lukas, R.V.; Solomon, I.H.; Ligon, K.L.; Nakashima, H.; Triggs, D.A.; Reardon, D.A.; Wen, P.; Stopa, B.M.; et al. Regulatable interleukin-12 gene therapy in patients with recurrent high-grade glioma: Results of a phase 1 trial. Sci. Transl. Med. 2019, 11, eaaw5680. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Study Design | Tumor Type | Setting | Agent | No. of Patients | ORR | PFS | OS |
|---|---|---|---|---|---|---|---|---|
| % | Months | Months | ||||||
| Carter (2016) [21] | Retrospective | Glioblastoma | Recurrent | IPI + BEV | 16 | 31.0 | N.A. | N.A. |
| Blumenthal (2016) [22] | Retrospective | Glioma | Recurrent | PEMBRO | 17 (10 GBM) | 0.0 | N.A. | 2.6 [range 0.4–11.6] |
| Chamberlain (2017) [23] | Retrospective | Glioblastoma | Recurrent | NIVO | 16 | 0.0 | 2.0 (95% CI 1.3–2.7) | 3.5 (95% CI 2.8–4.2) |
| Omuro (2018) Cohort A [17] | I | Glioblastoma | Recurrent | NIVO | 10 | 11.0 | 1.9 (95% CI 1.3–4.6) | 10.4 (95% CI 4.1–22.8) |
| Omuro (2018) Cohort B | I | Glioblastoma | Recurrent | NIVO + IPI | 10 | 0.0 | 1.5 (95% CI 0.5–2.8) | 9.2 (95% CI 3.9–12.7) |
| Omuro (2018) Cohort C | I | Glioblastoma | Recurrent | NIVO + IPI | 20 | 10.0 | 2.1 (95% CI 1.4–2.8) | 7.3 (95% CI 4.7–12.9) |
| Mantica (2018) [24] | Retrospective | Glioblastoma | Recurrent | NIVO (+ BEV) | 37 | 0.0 | 4.6 [range 0.5–15.0] | 6.5 [range 0.8–19.5] |
| Lukas (2018) [18] | I | Glioblastoma | Recurrent | ATEZO | 16 | 6.0 | 1.2 [range 0.7–10.7] | 4.2 [range 1.2–18.8+] |
| Cloughesy (2019) Cohort A [19] | II | Glioblastoma | Recurrent | PEMBRO | 16 | N.A. | 3.3 | 13.7 |
| Cloughesy (2019) Cohort B [19] | II | Glioblastoma | Recurrent | PEMBRO | 16 | N.A. | 2.4 | 7.5 |
| Schalper (2019) [20] | II | Glioblastoma | Newly diagnosed and Recurrent | NIVO | 29 | N.A. | 4.1 (95% CI 2.8–5.5) | 7.3 (95% CI 5.4–7.9) |
| Author | Study Design | Tumor Type | Agent | No. of Patients | ORR | PFS | OS |
|---|---|---|---|---|---|---|---|
| % | Months | Months | |||||
| Altomonte (2013) [25] | EAP (Retrospective) | Melanoma | IPI | 11 | 0 | 3.0 (95% CI 2.4–3.6) | 4.0 (95% CI 2.4–5.6) |
| Berrocal (2014) [26] | EAP (Retrospective) | Melanoma | IPI | 29 | 10.8 | N.A. | 3.9 (95% CI 1.1–6.8) |
| Chasset (2015) [28] | EAP (Retrospective) | Melanoma | IPI | 23 | 17 | N.A. | 7.0 (95% CI 4.0–12.0) |
| Di Giacomo (2012)(2014) [30,31] | II | Melanoma | IPI + Fotemustine | 20 | 40.0 | 3.0 † (95% CI 2.9–3.1) | 12.7 (95% CI 2.7–22.7) |
| Goldberg (2016) [36] | II | Melanoma | PEMBRO | 18 | 22.0 * (95% CI 7.0–48.0) | N.A. | N.R. |
| González-Cao (2017) [37] | EAP (Retrospective) | Melanoma | PEMBRO | 10 | 40.0 * | N.A. | N.A. |
| Kluger (2019) [38] | II | Melanoma | PEMBRO | 23 | 26.0 * (95% CI 10.0–48.0) | 2.0 (95% CI, 2.0–N.R.) | 17.0 (95% CI 10.0–N.R.) |
| Konstantinou (2014) [39] | EAP (Retrospective) | Melanoma | IPI | 38 | 5.3 * | N.A. | 3.3 |
| Long (2018) Cohort A [40] | II | Melanoma | NIVO + IPI | 35 | 46.0 * (95% CI 29.0–63.0) | N.R. † (95% CI 2.9–N.R) | N.R. (95% CI 8.5–N.R.) |
| Long (2018) Cohort B [40] | II | Melanoma | NIVO | 25 | 20.0 * (95% CI 7.0–41.0) | 2.5 † (95% CI 1.7–2.8) | 18.5 (95% CI 6.9–N.R.) |
| Long (2018) Cohort C [40] | II | Melanoma | NIVO | 16 | 6.0 * (95% CI 0.0–30.0) | 2.3 † (95% CI 1.4–4.3) | 5.1 (95% CI 1.8–N.R.) |
| Margolin (2012) Cohort A [41] | II | Melanoma | IPI | 51 | 16.0 * (95% CI 7.0–29.0) | 1.5 † (95% CI 1.2–2.5) | 7.0 (95% CI 4.1–10.8) |
| Margolin (2012) Cohort B [41] | II | Melanoma | IPI | 21 | 5.0 * (95% CI 0.1–24.0) | 1.2 † (95% CI 1.2–1.3) | 3.7 (95% CI 1.6–7.3) |
| Parakh (2017) [43] | Retrospective | Melanoma | NIVO or PEMBRO | 66 | 21.0 * | 5.3 † (95% CI 3.3–8.2) | 9.9 (95% CI 6.9–17.7) |
| Parakh (2019) [42] | Retrospective | Melanoma | NIVO + IPI | 11 | 18.0 * | 2.9 (95% CI 0.6–7.1) | 17.4 (95% CI 7.1–N.R.) |
| Queirolo (2014) [44] | EAP (Retrospective) | Melanoma | IPI | 145 | 12.0 | 3.1 (95% CI 2.7–3.5) | 4.3 (95% CI 3.4–5.2) |
| Tawbi (2018) [47] | II | Melanoma | NIVO + IPI | 94 | 55.0 * (95% CI 45–66) | N.R. | N.R. |
| Weber (2011) [46] | II | Melanoma | IPI (+ Budesonide) | 12 | 16.7 | N.A. | 14.0 |
| Bjørnhart (2019) [27] | Retrospective | NSCLC | NIVO or PEMBRO | 21 | 4.8 * | 4.2 (95%CI 2.5–5.9) | 8.2 (95% CI 1.0–15.5) |
| Crinò (2019) [29] | EAP | NSCLC | NIVO | 409 | 17.0 | 3.0 (95% CI 2.7–3.3) | 8.6 (95% CI 6.4–10.8) |
| Dumenil (2018) [32] | Retrospective | NSCLC | NIVO | 10 | 0 | N.A. | 3.1 |
| Garde-Noguera (2018) [34] | Retrospective | NSCLC | NIVO | 38 | 17.2 | 1.6 | 3.1 |
| Gauvain (2018) [35] | Retrospective | NSCLC | NIVO | 30 | 9.0 * (95% CI 3.0–23.0) | 3.9 † (95% CI 2.8–11.1) | N.R. |
| Goldberg (2016) [36] | II | NSCLC | PEMBRO | 18 | 33.0 * (95% CI 14.0–59.0) | N.A. | 7.7 (95% CI 3.5–N.R.) |
| Spigel (2018) Cohort 3 [60] | II | NSCLC | ATEZO | 13 | 23.0 (95% CI 5.0–54.0) | 2.5 | 6.8 (95% CI 3.2–19.5) |
| Flippot (2019) Cohort A [33] | II | RCC | NIVO | 39 | 11.8 * (95% CI 3.3–27.5) | 2.7 † (95% CI 2.3–4.6) | N.A. |
| Flippot (2019) Cohort B [33] | II | RCC | NIVO + Local Tx | 34 | N.A. | 4.8 † (95% CI 3.0–8.0) | N.A. |
| Sternberg (2019) [45] | III | UTC | ATEZO | 14 | 0 (95% CI 0–23.0) | 2.0 (95% CI 1.5–2.3) | 3.7 (95% CI 1.5–7.0) |
| Variable | Glioblastoma | Brain Metastases | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Melanoma | NSCLC | All | |||||||
| IPI | NIVO | PEMBRO | IPI + NIVO | PEMBRO | NIVO | ATEZO | All | ||
| Median Intracranial PFS | 2.1 mo | 1.2–3.0 mo | 2.3–2.5 mo | N.A. | N.A. | N.A. | 3.9 mo | N.A. | 2.7 mo |
| Median PFS | - | 3.0–3.1 mo | N.A. | 2.0–5.2 mo | 2.9 mo | N.A. | 1.6–3.0 mo | 2.5 mo | 3.0 mo |
| Median OS | 7.3 mo | 3.3–14.0 mo | 5.1–18.5 mo | 17.0–20.4 mo | 17.4 mo | 7.7 mo | 2.8–9.0 mo | 6.8 mo | 8.0 mo |
| NCT Number | Official Trial Name | Phase | Primary Endpoint | Endpoint Status |
|---|---|---|---|---|
| NCT02017717 | A Study of the Effectiveness and Safety of Nivolumab Compared to Bevacizumab and of Nivolumab With or Without Ipilimumab in Glioblastoma Patients (CheckMate-143) | III | Overall survival | Endpoint not met |
| NCT02617589 | An Investigational Immuno-therapy Study of Nivolumab Compared to Temozolomide, Each Given With Radiation Therapy, for Newly-diagnosed Patients With Glioblastoma (GBM, a Malignant Brain Cancer) (CheckMate-498) | III | Overall survival | Endpoint not met |
| NCT02667587 | An Investigational Immuno-therapy Study of Temozolomide Plus Radiation Therapy With Nivolumab or Placebo, for Newly Diagnosed Patients With Glioblastoma (GBM, a Malignant Brain Cancer) (CheckMate-548) | III | Progression-free survival Overall survival | Endpoint not met Endpoint in progress |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brahm, C.G.; van Linde, M.E.; Enting, R.H.; Schuur, M.; Otten, R.H.J.; Heymans, M.W.; Verheul, H.M.W.; Walenkamp, A.M.E. The Current Status of Immune Checkpoint Inhibitors in Neuro-Oncology: A Systematic Review. Cancers 2020, 12, 586. https://doi.org/10.3390/cancers12030586
Brahm CG, van Linde ME, Enting RH, Schuur M, Otten RHJ, Heymans MW, Verheul HMW, Walenkamp AME. The Current Status of Immune Checkpoint Inhibitors in Neuro-Oncology: A Systematic Review. Cancers. 2020; 12(3):586. https://doi.org/10.3390/cancers12030586
Chicago/Turabian StyleBrahm, Cyrillo G., Myra E. van Linde, Roelien H. Enting, Maaike Schuur, René H.J. Otten, Martijn W. Heymans, Henk M.W. Verheul, and Annemiek M.E. Walenkamp. 2020. "The Current Status of Immune Checkpoint Inhibitors in Neuro-Oncology: A Systematic Review" Cancers 12, no. 3: 586. https://doi.org/10.3390/cancers12030586
APA StyleBrahm, C. G., van Linde, M. E., Enting, R. H., Schuur, M., Otten, R. H. J., Heymans, M. W., Verheul, H. M. W., & Walenkamp, A. M. E. (2020). The Current Status of Immune Checkpoint Inhibitors in Neuro-Oncology: A Systematic Review. Cancers, 12(3), 586. https://doi.org/10.3390/cancers12030586