Negative Impact of Wound Complications on Oncologic Outcome of Soft Tissue Sarcomas of the Chest Wall

 ,
, 
Abstract
:1. Introduction
2. Results
2.1. Predictors of Wound Complications
2.2. Follow-Up
2.3. Local Recurrence Free Survival (LRFS)
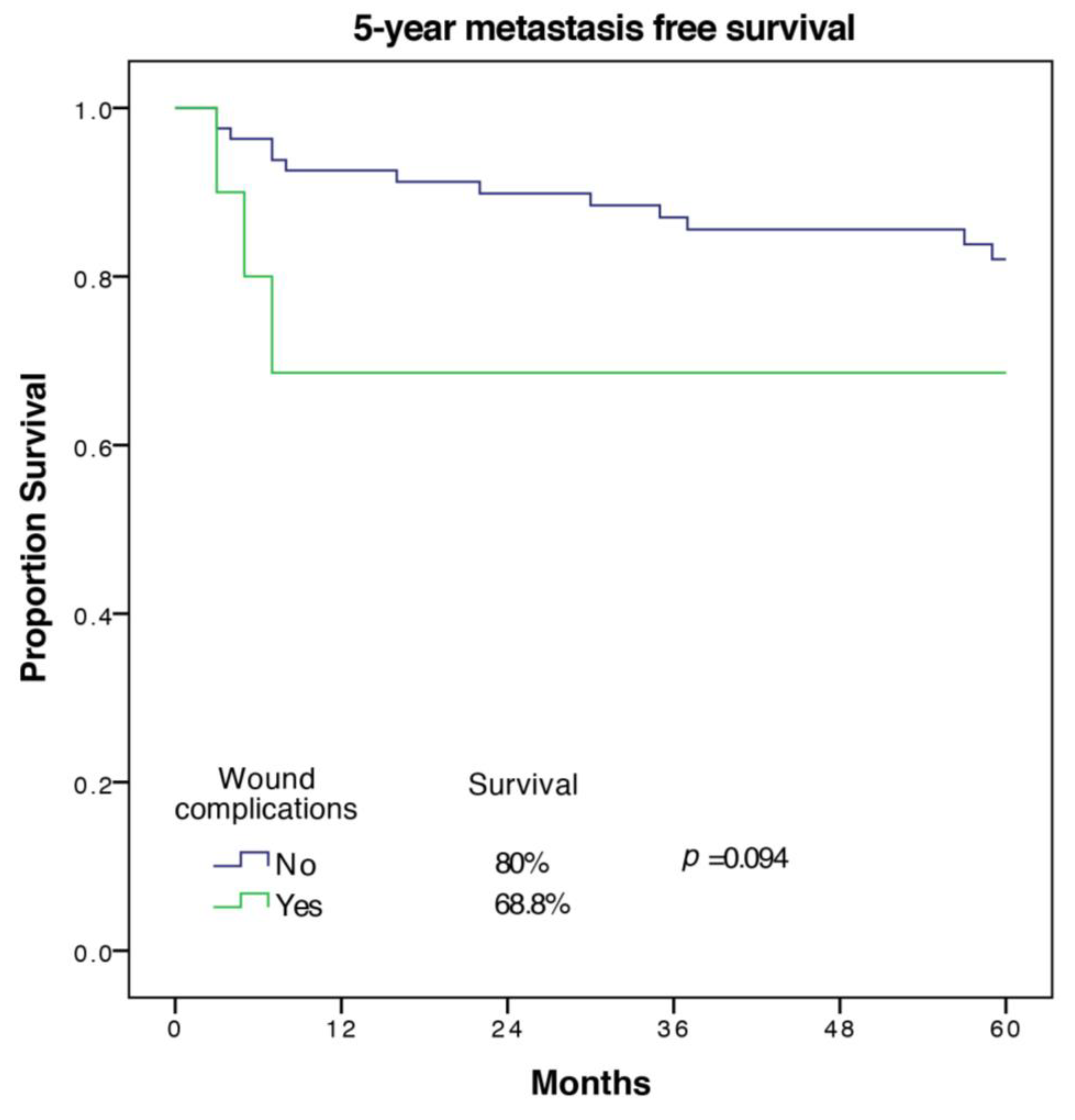
2.4. Metastasis Free Survival (MFS)
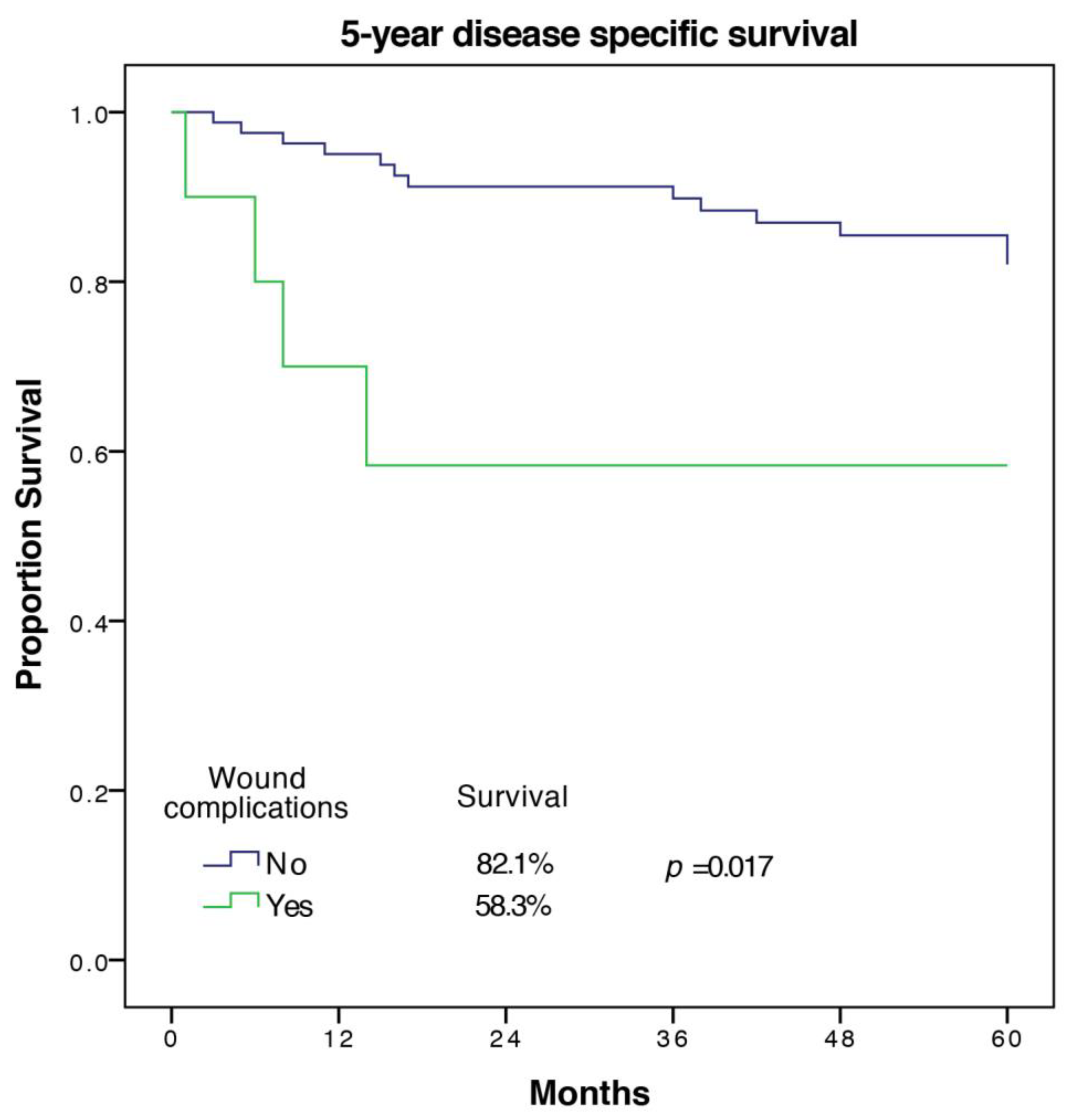
2.5. Disease Specific Survival (DSS)
3. Discussion
4. Materials and Methods
4.1. Treatment
4.2. Statistics
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jemal, A.; Siegel, R.; Xu, J.; Ward, E. Cancer statistics, 2010. CA A Cancer J. Clin. 2010, 60, 277–300. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.L.; Younes, R.N.; Haddad, F.J.; Deheinzelin, D.; Pinto, C.A.; Costa, M.L. Soft-tissue sarcomas of the chest wall: prognostic factors. Chest 2005, 127, 902–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, M.S.; Hajdu, S.I.; Bains, M.S.; Burt, M.E. Soft tissue sarcomas of the chest wall. Results of surgical resection. J. Thorac. Cardiovasc. Surg. 1991, 101, 843–854. [Google Scholar] [CrossRef]
- Harati, K.; Kolbenschlag, J.; Bohm, J.; Niggemann, H.; Joneidi-Jafari, H.; Stricker, I.; Lehnhardt, M.; Daigeler, A. Long-term outcomes of patients with soft tissue sarcoma of the chest wall: Analysis of the prognostic significance of microscopic margins. Oncol. Lett. 2018, 15, 2179–2187. [Google Scholar] [CrossRef] [PubMed]
- Salas, S.; Bui, B.; Stoeckle, E.; Terrier, P.; Ranchere-Vince, D.; Collin, F.; Leroux, A.; Guillou, L.; Michels, J.J.; Trassard, M.; et al. Soft tissue sarcomas of the trunk wall (STS-TW): a study of 343 patients from the French Sarcoma Group (FSG) database. Ann. Oncol. 2009, 20, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Soerensen, T.R.; Raedkjaer, M.; Jorgensen, P.H.; Hoejsgaard, A.; Safwat, A.; Baad-Hansen, T. Soft Tissue Sarcomas of the Thoracic Wall: More Prone to Higher Mortality, and Local Recurrence-A Single Institution Long-Term Follow-up Study. Int. J. Surg. Oncol. 2019, 2019, 2350157. [Google Scholar] [CrossRef] [Green Version]
- Baldini, E.H.; Lapidus, M.R.; Wang, Q.; Manola, J.; Orgill, D.P.; Pomahac, B.; Marcus, K.J.; Bertagnolli, M.M.; Devlin, P.M.; George, S.; et al. Predictors for major wound complications following preoperative radiotherapy and surgery for soft-tissue sarcoma of the extremities and trunk: importance of tumor proximity to skin surface. Ann. Surg. Oncol. 2013, 20, 1494–1499. [Google Scholar] [CrossRef]
- Davis, A.M.; O’Sullivan, B.; Turcotte, R.; Bell, R.; Catton, C.; Chabot, P.; Wunder, J.; Hammond, A.; Benk, V.; Kandel, R.; et al. Late radiation morbidity following randomization to preoperative versus postoperative radiotherapy in extremity soft tissue sarcoma. Radiother. Oncol. 2005, 75, 48–53. [Google Scholar] [CrossRef]
- O’Sullivan, B.; Davis, A.M.; Turcotte, R.; Bell, R.; Catton, C.; Chabot, P.; Wunder, J.; Kandel, R.; Goddard, K.; Sadura, A.; et al. Preoperative versus postoperative radiotherapy in soft-tissue sarcoma of the limbs: A randomised trial. Lancet 2002, 359, 2235–2241. [Google Scholar] [CrossRef]
- Schreiber, D.; Rineer, J.; Katsoulakis, E.; Sroufe, R.L.; Lange, C.S.; Nwokedi, E.; Schwartz, D.; Choi, K.; Rotman, M. Impact of postoperative radiation on survival for high-grade soft tissue sarcoma of the extremities after limb sparing radical resection. Am. J. Clin. Oncol. 2012, 35, 13–17. [Google Scholar] [CrossRef]
- Schütte, J.; Bauer, S.; Brodowicz, T.; Grünwald, V.; Hofer, S.; Hohenberger, P.; Jost, L.; Kasper, B.; Lindner, L.H.; Pritzkuleit, R.; et al. Onkopedia Leitlinie Weichgewebssarkome (maligne Weichgewebstumoren) des Erwachsenen. Ger. Soc. Haematol. Oncol. 2019. [Google Scholar]
- Andreou, A.; Biebl, M.; Dadras, M.; Struecker, B.; Sauer, I.M.; Thuss-Patience, P.C.; Chopra, S.; Fikatas, P.; Bahra, M.; Seehofer, D.; et al. Anastomotic leak predicts diminished long-term survival after resection for gastric and esophageal cancer. Surgery 2016, 160, 191–203. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Yoshikawa, T.; Aoyama, T.; Hasegawa, S.; Yamada, T.; Tsuchida, K.; Fujikawa, H.; Sato, T.; Ogata, T.; Cho, H.; et al. Impact of infectious complications on gastric cancer recurrence. Gastric Cancer 2015, 18, 368–374. [Google Scholar] [CrossRef] [PubMed]
- McArdle, C.S.; McMillan, D.C.; Hole, D.J. Impact of anastomotic leakage on long-term survival of patients undergoing curative resection for colorectal cancer. Br. J. Surg. 2005, 92, 1150–1154. [Google Scholar] [CrossRef] [PubMed]
- Jackson, R.M.; Rice, D.H. Wound infections and recurrence in head and neck cancer. Otolaryngol. Head Neck Surg. 1990, 102, 331–333. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, J.P.; Suarez, C. Prognostic significance of postoperative wound infection on head and neck cancer. Otolaryngol. Head Neck Surg. 1998, 118, 272–275. [Google Scholar] [CrossRef]
- Beecher, S.M.; O’Leary, D.P.; McLaughlin, R.; Sweeney, K.J.; Kerin, M.J. Influence of complications following immediate breast reconstruction on breast cancer recurrence rates. Br. J. Surg. 2016, 103, 391–398. [Google Scholar] [CrossRef]
- Murthy, B.L.; Thomson, C.S.; Dodwell, D.; Shenoy, H.; Mikeljevic, J.S.; Forman, D.; Horgan, K. Postoperative wound complications and systemic recurrence in breast cancer. Br. J. Cancer 2007, 97, 1211–1217. [Google Scholar] [CrossRef] [Green Version]
- Behnke, N.K.; Alamanda, V.K.; Song, Y.; Archer, K.R.; Halpern, J.L.; Schwartz, H.S.; Holt, G.E. Does postoperative infection after soft tissue sarcoma resection affect oncologic outcomes? J. Surg. Oncol. 2014, 109, 415–420. [Google Scholar] [CrossRef]
- Broecker, J.S.; Ethun, C.G.; Monson, D.K.; Lopez-Aguiar, A.G.; Le, N.; McInnis, M.; Godette, K.; Reimer, N.B.; Oskouei, S.V.; Delman, K.A.; et al. The Oncologic Impact of Postoperative Complications Following Resection of Truncal and Extremity Soft Tissue Sarcomas. Ann. Surg. Oncol. 2017, 24, 3574–3586. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- McMillan, R.R.; Sima, C.S.; Moraco, N.H.; Rusch, V.W.; Huang, J. Recurrence patterns after resection of soft tissue sarcomas of the chest wall. Ann. Thorac. Surg. 2013, 96, 1223–1228. [Google Scholar] [CrossRef] [PubMed]
- Kuwahara, H.; Salo, J.; Nevala, R.; Tukiainen, E. Single-Institution, Multidisciplinary Experience of Soft Tissue Sarcomas in the Chest Wall. Ann. Plast. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Tsukushi, S.; Nishida, Y.; Sugiura, H.; Nakashima, H.; Ishiguro, N. Soft tissue sarcomas of the chest wall. J. Thorac. Oncol. 2009, 4, 834–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slump, J.; Ferguson, P.C.; Wunder, J.S.; Griffin, A.M.; Hoekstra, H.J.; Liu, X.; Hofer, S.O.P.; O’Neill, A.C. Patient, tumour and treatment factors affect complication rates in soft tissue sarcoma flap reconstruction in a synergistic manner. Eur. J. Surg. Oncol. 2017, 43, 1126–1133. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, C.; Harris, J.; Siegel, E.; Suva, L.; Wilson, M.; Morell, S.; Nicholas, R. Obesity is associated with larger soft-tissue sarcomas, more surgical complications, and more complex wound closures (obesity leads to larger soft-tissue sarcomas). J. Surg. Oncol. 2018, 118, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.D.; Mo, X.; Andonian, N.T.; Haglund, K.E.; Martin, D.D.; Liebner, D.A.; Chen, J.L.; Iwenofu, O.H.; Chakravarti, A.; Scharschmidt, T.J.; et al. Patterns of major wound complications following multidisciplinary therapy for lower extremity soft tissue sarcoma. J. Surg. Oncol. 2016, 114, 385–391. [Google Scholar] [CrossRef]
- Moore, J.; Isler, M.; Barry, J.; Mottard, S. Major wound complication risk factors following soft tissue sarcoma resection. Eur. J. Surg. Oncol. 2014, 40, 1671–1676. [Google Scholar] [CrossRef]
- Stevenson, M.G.; Ubbels, J.F.; Slump, J.; Huijing, M.A.; Bastiaannet, E.; Pras, E.; Hoekstra, H.J.; Been, L.B. Identification of predictors for wound complications following preoperative or postoperative radiotherapy in extremity soft tissue sarcoma. Eur. J. Surg. Oncol. 2018, 44, 816–822. [Google Scholar] [CrossRef]
- Slump, J.; Hofer, S.O.P.; Ferguson, P.C.; Wunder, J.S.; Griffin, A.M.; Hoekstra, H.J.; Bastiaannet, E.; O’Neill, A.C. Flap reconstruction does not increase complication rates following surgical resection of extremity soft tissue sarcoma. Eur. J. Surg. Oncol. 2018, 44, 251–259. [Google Scholar] [CrossRef]
- Stojadinovic, A.; Leung, D.H.; Hoos, A.; Jaques, D.P.; Lewis, J.J.; Brennan, M.F. Analysis of the prognostic significance of microscopic margins in 2084 localized primary adult soft tissue sarcomas. Ann. Surg. 2002, 235, 424–434. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.G.; Memos, N.; Thomas, J.M.; Smith, M.J.; Strauss, D.C.; Hayes, A.J. Patterns of disease relapse in primary extremity soft-tissue sarcoma. Br. J. Surg. 2016, 103, 1487–1496. [Google Scholar] [CrossRef] [PubMed]
- Radons, J. The role of inflammation in sarcoma. Adv. Exp. Med. Biol. 2014, 816, 259–313. [Google Scholar] [CrossRef] [PubMed]
- Hagi, T.; Nakamura, T.; Iino, T.; Matsubara, T.; Asanuma, K.; Matsumine, A.; Sudo, A. The diagnostic and prognostic value of interleukin-6 in patients with soft tissue sarcomas. Sci. Rep. 2017, 7, 9640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayatilaka, H.; Tyle, P.; Chen, J.J.; Kwak, M.; Ju, J.; Kim, H.J.; Lee, J.S.H.; Wu, P.H.; Gilkes, D.M.; Fan, R.; et al. Synergistic IL-6 and IL-8 paracrine signalling pathway infers a strategy to inhibit tumour cell migration. Nat. Commun. 2017, 8, 15584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tivari, S.; Lu, H.; Dasgupta, T.; De Lorenzo, M.S.; Wieder, R. Reawakening of dormant estrogen-dependent human breast cancer cells by bone marrow stroma secretory senescence. Cell Commun. Signal. 2018, 16, 48. [Google Scholar] [CrossRef] [Green Version]
- Voronov, E.; Reich, E.; Dotan, S.; Dransh, P.; Cohen, I.; Huszar, M.; Fogel, M.; Kleinman, H.K.; White, R.M.; Apte, R.N. Effects of IL-1 molecules on growth patterns of 3-MCA-induced cell lines: an interplay between immunogenicity and invasive potential. J. Immunotoxicol. 2010, 7, 27–38. [Google Scholar] [CrossRef] [Green Version]
- Libby, P. Inflammation in atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2045–2051. [Google Scholar] [CrossRef] [Green Version]
- Danesh, J.; Wheeler, J.G.; Hirschfield, G.M.; Eda, S.; Eiriksdottir, G.; Rumley, A.; Lowe, G.D.; Pepys, M.B.; Gudnason, V. C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N. Engl. J. Med. 2004, 350, 1387–1397. [Google Scholar] [CrossRef]
- Emerging Risk Factors, C.; Kaptoge, S.; Di Angelantonio, E.; Lowe, G.; Pepys, M.B.; Thompson, S.G.; Collins, R.; Danesh, J. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis. Lancet 2010, 375, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA A Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Complication | Clavien-Dindo Grade [21] | |||||
|---|---|---|---|---|---|---|
| I | II | IIIa | IIIb | IV | Total | |
| Respiratory tract infection | – | 1 | – | – | 1 | 2 |
| Urinary tract infection | – | 2 | – | – | – | 2 |
| Hemorrhage/Anemia | 8 | 5 | – | 2 | 2 | 17 |
| Wound complication | 2 | 2 | – | 9 | – | 13 |
| Seroma formation | 11 | – | – | 3 | – | 14 |
| Pneumothorax | – | – | 4 | – | – | 4 |
| All Patients (highest grade complication) | 20 | 7 | 4 | 11 | 3 | 45 |
| Variable | All Patients (n = 102) | No Wound Complications (n = 91) | Wound Complications (n = 11) | Comparison, p-value | Logistic Multivariate Regression, p-value | Odds Ratio (95% CI) |
|---|---|---|---|---|---|---|
| Sex | 0.200 | |||||
| Male | 51 (50) | 43 (47.3) | 8 (72.7) | |||
| Female | 51 (50) | 48 (52.7) | 3 (27.3) | |||
| Age at operation, mean | 56.1 ± 18 | 56.7 ± 17,8 | 59.4 ± 20 | 0.508 | ||
| Obesity (BMI>30 kg/m2) | 0.033 | * | ||||
| Yes | 21 (20.6) | 16 (17.6) | 5 (45.4) | |||
| No | 81 (79.4) | 75 (82.4) | 6 (54.5) | |||
| ASA-Classification | 0.005 | * | ||||
| 1 | 20 (19.6) | 19 (20.9) | 1 (9.1) | |||
| 2 | 58 (56.9) | 55 (60.4) | 3 (27.3) | |||
| 3 | 22 (21.6) | 15 (16.5) | 7 (63.6) | |||
| 4 | 2 (2) | 2 (2.2) | 0 | |||
| Cardiovascular Morbidity | 0.026 | 0.036 | 5.07 (1.11–23.16) | |||
| Yes | 41 (40.2) | 33 (36.3) | 8 (72.7) | |||
| No | 61 (59.8) | 58 (63.7) | 3 (27.3) | |||
| Active Smoker | 0.219 | |||||
| Yes | 82 (80.4) | 75 (82.4) | 7 (63.6) | |||
| No | 20 (19.6) | 16 (17.6) | 4 (36.4) | |||
| Tumor depth | 0.497 | |||||
| Superficial | 31 (30.4) | 29 (31.9) | 2 (18.2) | |||
| Deep | 71 (69.6) | 62 (68.1) | 9 (81.8) | |||
| Tumor location (thorax region) | 0.704 | |||||
| Anterior | 11 (10.8) | 9 (9.9) | 2 (18.2) | |||
| Anterolateral | 32 (31.4) | 28 (30.8) | 4 (26.4) | |||
| Lateral | 28 (27.5) | 25 (27.5) | 3 (27.3) | |||
| Posterolateral | 19 (18.6) | 17 (18.7) | 2 (18.2) | |||
| Posterior | 12 (11.8) | 12 (13.2) | 0 | |||
| Tumor size | 0.389 | |||||
| ≤5 cm | 34 (33.3) | 32 (35.2) | 2 (18.2) | |||
| 5.1–10 cm | 40 (39.2) | 36 (39.6) | 4 (26.4) | |||
| 10.1–15 cm | 15 (14.7) | 13 (14.3) | 2 (18.2) | |||
| >15 cm | 13 (12.7) | 10 (11) | 3 (27.3) | |||
| Histologic Subtype | 0.233 | |||||
| Undifferentiated pleomorphic | 24 (23.5) | 21 (23.1) | 3 (27.3) | |||
| Liposarcoma | 17 (16.7) | 16 (17.6) | 1 (9.1) | |||
| Angiosarcoma | 10 (9.8) | 7 (7.7) | 3 (27.3) | |||
| Dermatofibrosarcoma | 8 (7.8) | 8 (8.8) | 0 | |||
| Fibrosarcoma | 7 (6.9) | 5 (5.5) | 2 (18.2) | |||
| Leiomyosarcoma | 7 (6.9) | 7 (7.7) | 0 | |||
| Myxofibrosarcoma | 6 (5.9) | 6 (6.6) | 0 | |||
| Other | 23 (22.6) | 21 (23.1) | 2 | |||
| UICC-Stage | 0.138 | |||||
| I | 33 (32.4) | 31 (34.1) | 2 (18.2) | |||
| II | 13 (12.7) | 13 (14.3) | 0 | |||
| III | 56 (54.9) | 47 (51.6) | 9 (81.8) | |||
| Tumor Grade | 0.425 | |||||
| G1 | 34 (33.3) | 32 (35.2) | 2 (18.2) | |||
| G2 | 29 (28.4) | 26 (28.6) | 3 (27.3) | |||
| G3 | 39 (38.2) | 33 (36.2) | 6 (54.5) | |||
| Prior external biopsy/incomplete resection | 0.980 | |||||
| Yes | 46 (45.1) | 41 (45.1) | 5 (45.5) | |||
| No | 56 (54.9) | 50 (54.9) | 6 (54.5) | |||
| Resection status | 0.515 | |||||
| R0 | 94 (92.2) | 84 (92.3) | 10 (90.1) | |||
| R1 | 4 (3.9) | 4 (4.4) | 0 | |||
| R2 | 4 (3.9) | 3 (3.3) | 1 (9.9) | |||
| Operative time in minutes, mean | 111.1 ± 72.5 | 105,5 ± 69.2 | 158.1 ± 86 | 0.029 | 0.025 | 1.01 (1.001–1.02) |
| Full thickness resection | 0.239 | |||||
| Yes | 39 (38.2) | 33 (36.3) | 6 (54.5) | |||
| No | 63 (61.8) | 58 (63.7) | 5 (45.5) | |||
| Soft tissue reconstruction | 0.279 | |||||
| Primary Closure | 70 (68.6) | 64 (70.3) | 6 (54.5) | |||
| Skin graft | 7 (6.9) | 7 (7.7) | 0 | |||
| Local flap | 24 (23.5) | 19 (20.9) | 5 (45.5) | |||
| Free flap | 1 (1) | 1 (1.1) | 0 | |||
| Neoadjuvant Treatment | 1.000 | |||||
| Yes | 5 (4.9) | 5 (5.5) | 0 | |||
| No | 97 (95.1) | 86 (94.5) | 11 (100) | |||
| Adjuvant radiotherapy | 0.744 | |||||
| Yes | 35 (34.3) | 32 (35.2) | 3 (27.3) | |||
| No | 67 (65.7) | 59 (64.8) | 8 (72.7) | |||
| Length of stay in days, mean | 13.4 ± 10.4 | 11.4 ± 5.8 | 29.5 ± 21.6 | <0.001 |
| Variable | n | 5-y-LRFS | p-value (Log Rank) | 5-y-MFS | p-value (Log Rank) | 5-y-DSS | p-value (Log Rank) |
|---|---|---|---|---|---|---|---|
| All patients | 94 | 67.8 ± 5 | 80.3 ± 4.5 | 79.5 ± 4.5 | |||
| Sex | 0.005 | 0.550 | 0.189 | ||||
| Male | 45 | 81.4 ± 5.9 | 83.9 ± 5.6 | 84.9 ± 5.7 | |||
| Female | 49 | 55.1 ± 7.4 | 76.1 ± 7.2 | 74.1 ± 6.8 | |||
| Age at operation | 0.057 | 0.036 | 0.023 | ||||
| ≤39 | 19 | 89.5 ± 7 | 94.7 ± 5.1 | - | |||
| 40–64 | 38 | 68 ± 7.6 | 83.8 ± 6.8 | 77.6 ± 7.7 | |||
| ≥65 | 37 | 55.3 ± 8.8 | 66.4 ± 9.1 | 69.0 ± 8.3 | |||
| Obesity (BMI>30 kg/m2) | 0.732 | 0.874 | 0.336 | ||||
| Yes | 18 | 72.2 ± 10.6 | 83.3 ± 8.8 | 88.9 ± 7.4 | |||
| No | 76 | 66.7 ± 5.6 | 79.1 ± 5.3 | 76.8 ± 5.3 | |||
| ASA-Classification | 0.009 | 0.208 | 0.238 | ||||
| 1 | 20 | 95 ± 4.9 | 90 ± 6.7 | 89.7 ± 6.9 | |||
| 2 | 51 | 62.4 ± 7.1 | 80.8 ± 6.2 | 78.3 ± 6.5 | |||
| 3 | 21 | 52.4 ± 10.9 | 69.3 ± 11.9 | 75.9 ± 9.4 | |||
| 4 | 2 | - | 50 ± 35.4 | 50 ± 35.4 | |||
| Cardiovascular Morbidity | 0.005 | 0.011 | 0.001 | ||||
| Yes | 36 | 48.9 ± 9.1 | 62.5 ± 10.3 | 59.7 ± 9.5 | |||
| No | 58 | 78.6 ± 5.5 | 88.7 ± 4.4 | 90.5 ± 4.1 | |||
| Active Smoker | 0.921 | 0.947 | 0.641 | ||||
| Yes | 19 | 68.4 ± 10.7 | 81.5 ± 9.8 | 78.6 ± 9.5 | |||
| No | 75 | 67.7 ± 5.6 | 80 ± 5.1 | 79.9 ± 5.1 | |||
| Tumor depth | 0.150 | 0.064 | 0.158 | ||||
| Superficial | 29 | 77.9 ± 8 | 91.3 ± 5.9 | 87.9 ± 6.6 | |||
| Deep | 65 | 63.4 ± 6.1 | 75.4 ± 5.9 | 75.8 ± 5.7 | |||
| Tumor location (thorax region) | 0.773 | 0.837 | 0.174 | ||||
| Anterior | 11 | 72.7 ± 13.4 | 90.9 ± 8.7 | 90.9 ± 8.7 | |||
| Anterolateral | 27 | 61.4 ± 9.7 | 80.9 ± 8.8 | 75.7 ± 8.7 | |||
| Lateral | 26 | 67.2 ± 9.6 | 79.9 ± 8.1 | 64.6 ± 10.4 | |||
| Posterolateral | 19 | 68.4 ± 10.7 | 80.7 ± 10.3 | 90.9 ± 8.7 | |||
| Posterior | 11 | 80 ± 12.6 | 70 ± 14.5 | 88.9 ± 10.5 | |||
| Tumor size | 0.001 | 0.003 | 0.019 | ||||
| ≤5 cm | 33 | 74.5 ± 7.9 | 81.9 ± 7.5 | 83 ± 7 | |||
| 5.1–10 cm | 35 | 76.2 ± 7.4 | 84.3 ± 6.5 | 83.1 ± 7 | |||
| 10.1–15 cm | 15 | 66.7 ± 12.2 | 92.9 ± 6.9 | 86.2 ± 9.1 | |||
| >15 cm | 11 | 20.5 ± 12.9 | 46.7 ± 16.6 | 48.0 ± 16.4 | |||
| Histologic Subtype | 0.013 | 0.321 | 0.96 | ||||
| Undifferentiated pleomorphic | 23 | 59.1 ± 10.6 | 64.7 ± 11 | 66.9 ± 10.4 | |||
| Liposarcoma | 14 | 92.3 ± 7.4 | 90.9 ± 8.7 | 90.9 ± 8.7 | |||
| Angiosarcoma | 8 | 25 ± 15.3 | 66.7 ± 27.2 | 53.6 ± 20.1 | |||
| Dermatofibrosarcoma | 8 | - | - | - | |||
| Fibrosarcoma | 7 | 57.1 ± 18.7 | 85.7 ± 13.2 | 83.3 ± 15.2 | |||
| Leiomyosarcoma | 6 | 83.3 ± 15.2 | 83.3 ± 15.2 | 66.7 ± 19.2 | |||
| Myxofibrosarcoma | 5 | 60 ± 21.9 | - | - | |||
| Other | 23 | 67.8 ± 10.1 | 76.4 ± 9.3 | 85 ± 8 | |||
| UICC-Stage | 0.005 | 0.022 | 0.046 | ||||
| I | 32 | 90.3 ± 5.3 | 96.7 ± 3.3 | 92 ± 5.4 | |||
| II | 12 | 53.3 ± 16.1 | 59.5 ± 16.2 | 70.7 ± 14.6 | |||
| III | 50 | 56.3 ± 7.2 | 74.5 ± 6.8 | 73.3 ± 6.7 | |||
| Tumor Grade | 0.002 | 0.015 | 0.045 | ||||
| G1 | 33 | 90.6 ± 5.2 | 96.8 ± 3.2 | 92.4 ± 5.2 | |||
| G2 | 26 | 60.4 ± 9.8 | 75.6 ± 8.7 | 71.9 ± 9 | |||
| G3 | 35 | 51.4 ± 9 | 65.2 ± 9.9 | 72.3 ± 8.6 | |||
| Prior external biopsy/incomplete resection | 0.306 | 0.704 | 0.728 | ||||
| Yes | 42 | 73.1 ± 7 | 81.4 ± 6.4 | 76.6 ± 6.9 | |||
| No | 52 | 63.3 ± 7 | 79.8 ± 6.2 | 82.9 ± 5.6 | |||
| Full thickness resection | 0.101 | 0.916 | 0.146 | ||||
| Yes | 36 | 59.6 ± 8.4 | 80.9 ± 7.2 | 73 ± 7.7 | |||
| No | 58 | 72.9 ± 6 | 80 ± 5.8 | 83.4 ± 5.5 | |||
| Soft tissue reconstruction | 0.305 | 0.159 | 0.673 | ||||
| Primary Closure | 63 | 71.5 ± 5.9 | 80.2 ± 5.4 | 78.5 ± 5.6 | |||
| Skin graft | 7 | 42.9 ± 18.7 | 83.3 ± 15.2 | - | |||
| Local flap | 23 | 64.5 ± 10.1 | 86.5 ± 7.2 | 78 ± 8.7 | |||
| Free flap | 1 | - | - | - | |||
| Wound complication CD ≥ 2 | <0.001 | 0.094 | 0.017 | ||||
| Yes | 10 | 30 ± 14.5 | 68.8 ± 15.1 | 58.3 ± 16.1 | |||
| No | 84 | 72.6 ± 5 | 82 ± 4.6 | 82.1 ± 4.6 | |||
| Other complication CD ≥ 2 | 0.315 | 0.555 | 0.051 | ||||
| Yes | 15 | 56.9 ± 13.4 | 77 ± 12 | 66 ± 12.4 | |||
| No | 79 | 69.7 ± 5.3 | 80.9 ± 4.9 | 82.2 ± 4.7 | |||
| Neoadjuvant Treatment | 0.761 | 0.385 | 0.723 | ||||
| Yes | 4 | 75 ± 21.7 | - | 75 ± 21.7 | |||
| No | 90 | 67.5 ± 5.1 | 79.5 ± 4.7 | 79.9 ± 4.6 | |||
| Adjuvant radiotherapy | 0.036 | 0.114 | 0.762 | ||||
| Yes | 30 | 81.7 ± 7.5 | 72 ± 8.5 | 81.3 ± 7.6 | |||
| No | 64 | 61.2 ± 6.7 | 84.4 ± 5.2 | 78.6 ± 5.6 |
| Variable | Hazard Ratio 5-y-LRFS | p-value (MVA) | Hazard Ratio 5-y-MFS | p-value (MVA) | Hazard Ratio 5-y-DSS | p-value (MVA) |
|---|---|---|---|---|---|---|
| Sex | ||||||
| Male | 0.93 (0.34–2.58) | 0.893 | 2 (0.55–7.25) | 0.289 | 1.75 (0.43–7.13) | 0.432 |
| Female | Ref. | Ref. | Ref. | |||
| Age at operation | ||||||
| ≤39 | Ref. | Ref. | Ref. | |||
| 40–64 | 1.73 (0.31–9.73) | 0.533 | 1.27 (0.85–19.11) | 0.861 | – | 0.935 |
| ≥65 | 1.62 (0.25–10.52) | 0.612 | 3.26 (0.17–62.36) | 0.433 | – | 0.935 |
| ASA-Classification | ||||||
| 1 | Ref. | Ref. | Ref. | |||
| 2 | 4.26 (0.44–41.2) | 0.21 | 0.73 (0.09–5.9) | 0.765 | 0.58 (0.07–4.6) | 0.607 |
| 3 | 4.9 (0.47–50.87) | 0.183 | 0.62 (0.07–5.85) | 0.676 | 0.68 (0.08–5.38) | 0.711 |
| 4 | – | 0.985 | 3.93 (0.13–122.81) | 0.436 | 2.39 (0.1–55) | 0.587 |
| Cardiovascular Morbidity | ||||||
| Yes | 4.07 (1.43–11.59) | 0.009 | 3.17 (0.72–13.91) | 0.127 | 11.55 (2.23–59.82) | 0.004 |
| No | Ref. | Ref. | Ref. | |||
| Tumor depth | ||||||
| Superficial | Ref. | Ref. | Ref. | |||
| Deep | 1.46 (0.48–4.42) | 0.508 | 1.88 (0.3–11.93) | 0.503 | 1.5 (0.33–6.91) | 0.600 |
| Tumor size | ||||||
| ≤ 5 cm | Ref. | Ref. | Ref. | |||
| 5.1–10 cm | 1.02 (0.33–3.16) | 0.976 | 0.43 (0.09–2.13) | 0.301 | 0.65 (0.13–3.12) | 0.590 |
| 10.1–15 cm | 0.94 (0.27–3.18) | 0.916 | 0.08 (0.004–1.7) | 0.105 | 0.52 (0.08–3.37) | 0.496 |
| > 15 cm | 2.06 (0.63–6.74) | 0.234 | 3.13 (0.59–16.64) | 0.181 | 1.81 (0.35–9.35) | 0.480 |
| Tumor Grade | ||||||
| G1 | Ref. | Ref. | Ref. | |||
| G2 | 18.76 (4.11–85.49) | <0.001 | 9.05 (0.63–129.2) | 0.104 | 11.96 (1.55–92.4) | 0.017 |
| G3 | 10 (2.59–38.62) | 0.001 | 14.35 (1.31–157.35) | 0.029 | 6.95 (1.04–46.35) | 0.045 |
| Histologic Subtype | 0.307 | 0.607 | ||||
| Wound complication CD ≥ 2 | ||||||
| Yes | 3.83 (1.24–11.85) | 0.02 | 3.4 (0.66–17.43) | 0.142 | 5.31 (1.1–25.62) | 0.037 |
| No | Ref. | Ref. | Ref. | |||
| Other complication CD ≥ 2 | ||||||
| Yes | 1.15 (0.35–3.77) | 0.822 | 1.22 (0.18–8.35) | 0.839 | 2.94 (0.6–14.46) | 0.184 |
| No | Ref. | Ref. | Ref. | |||
| Adjuvant radiotherapy | ||||||
| Yes | 0.09 (0.03–0.31) | <0.001 | 1.1 (0.28–4.32) | 0.893 | 0.22 (0.05–1.02) | 0.052 |
| No | Ref. | Ref. | Ref. | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dadras, M.; Koepp, P.; Wagner, J.M.; Wallner, C.; Sacher, M.; Lehnhardt, M.; Behr, B.; Harati, K. Negative Impact of Wound Complications on Oncologic Outcome of Soft Tissue Sarcomas of the Chest Wall. Cancers 2020, 12, 101. https://doi.org/10.3390/cancers12010101
Dadras M, Koepp P, Wagner JM, Wallner C, Sacher M, Lehnhardt M, Behr B, Harati K. Negative Impact of Wound Complications on Oncologic Outcome of Soft Tissue Sarcomas of the Chest Wall. Cancers. 2020; 12(1):101. https://doi.org/10.3390/cancers12010101
Chicago/Turabian StyleDadras, Mehran, Pascal Koepp, Johannes Maximilian Wagner, Christoph Wallner, Maxi Sacher, Marcus Lehnhardt, Björn Behr, and Kamran Harati. 2020. "Negative Impact of Wound Complications on Oncologic Outcome of Soft Tissue Sarcomas of the Chest Wall" Cancers 12, no. 1: 101. https://doi.org/10.3390/cancers12010101
APA StyleDadras, M., Koepp, P., Wagner, J. M., Wallner, C., Sacher, M., Lehnhardt, M., Behr, B., & Harati, K. (2020). Negative Impact of Wound Complications on Oncologic Outcome of Soft Tissue Sarcomas of the Chest Wall. Cancers, 12(1), 101. https://doi.org/10.3390/cancers12010101