ERCC1 Is a Predictor of Anthracycline Resistance and Taxane Sensitivity in Early Stage or Locally Advanced Breast Cancers

 ,
,  ,
, 

Abstract
1. Introduction
2. Results
2.1. ERCC1 Transcript Is a Predictor of Tumour Grade and Chromosomal Instability in Early Stage breast cancers (BCs)
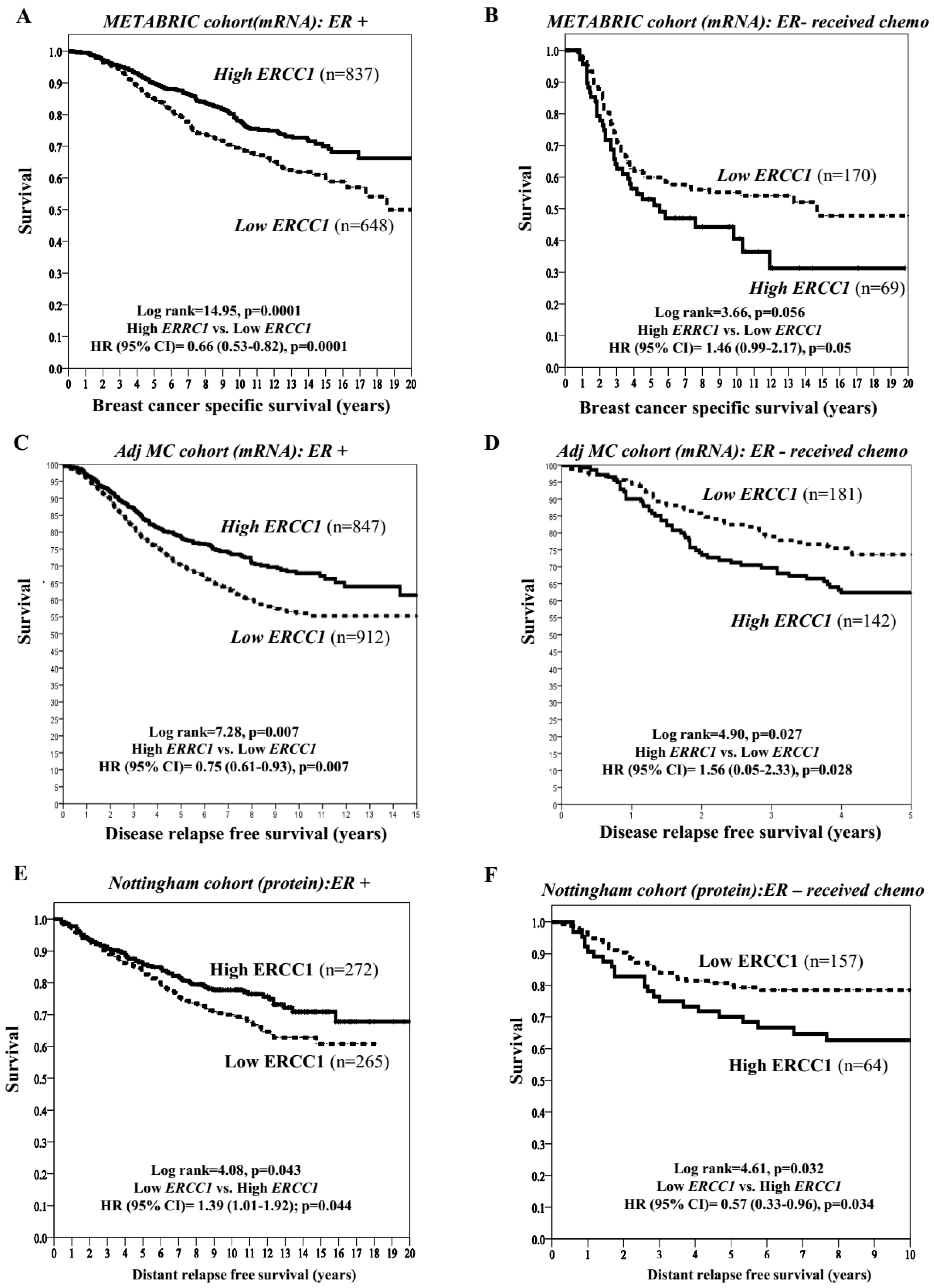
2.2. ERCC1 Transcript and Clinical Outcomes in Patients Receiving Adjuvant Therapy
2.3. ERCC1 Protein, Clinicopathological Features and Outcomes
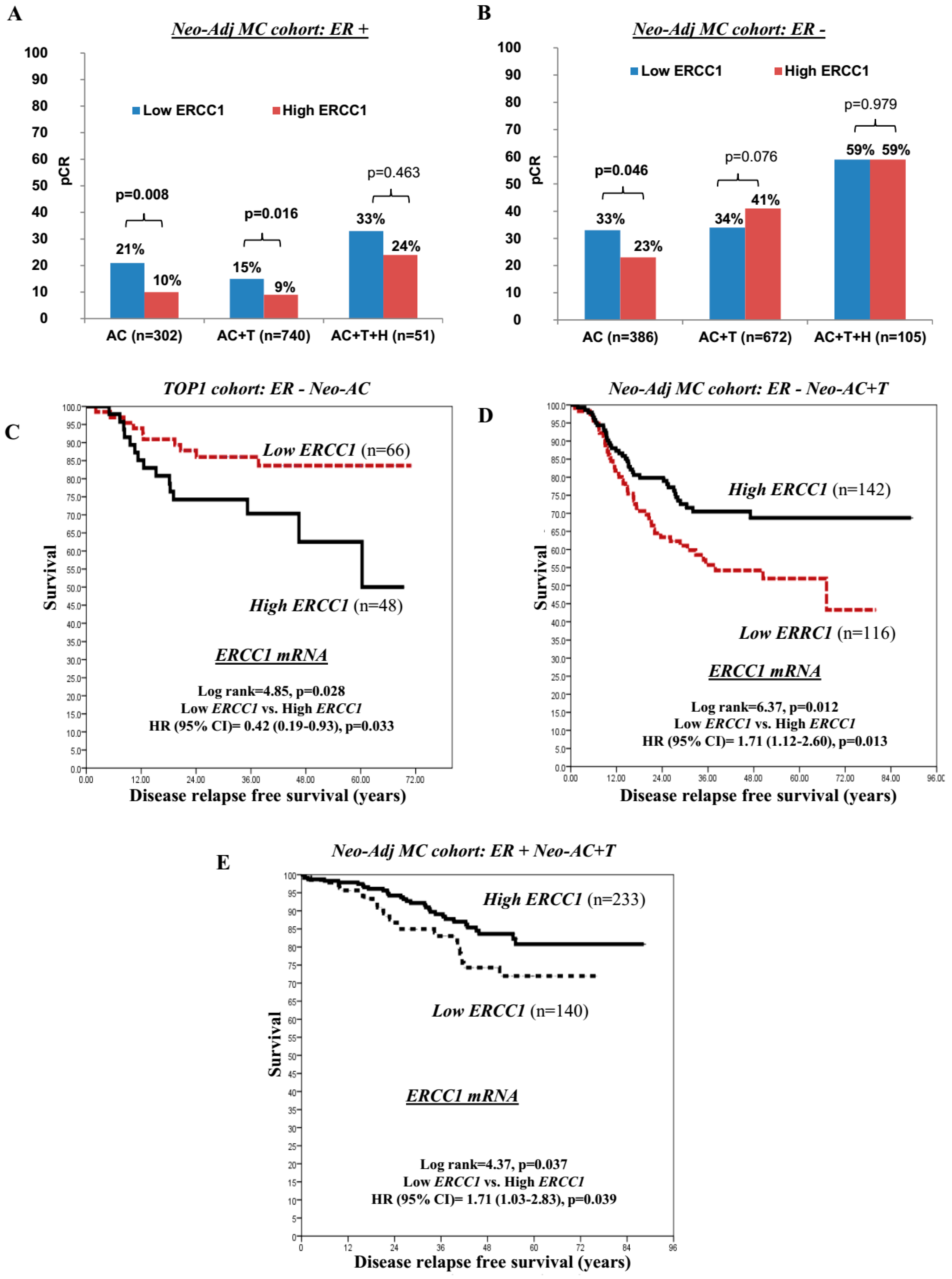
2.4. ERCC1 and Pathological Complete Response (pCR) to Neoadjuvant Chemotherapy
3. Discussion
4. Patients and Methods
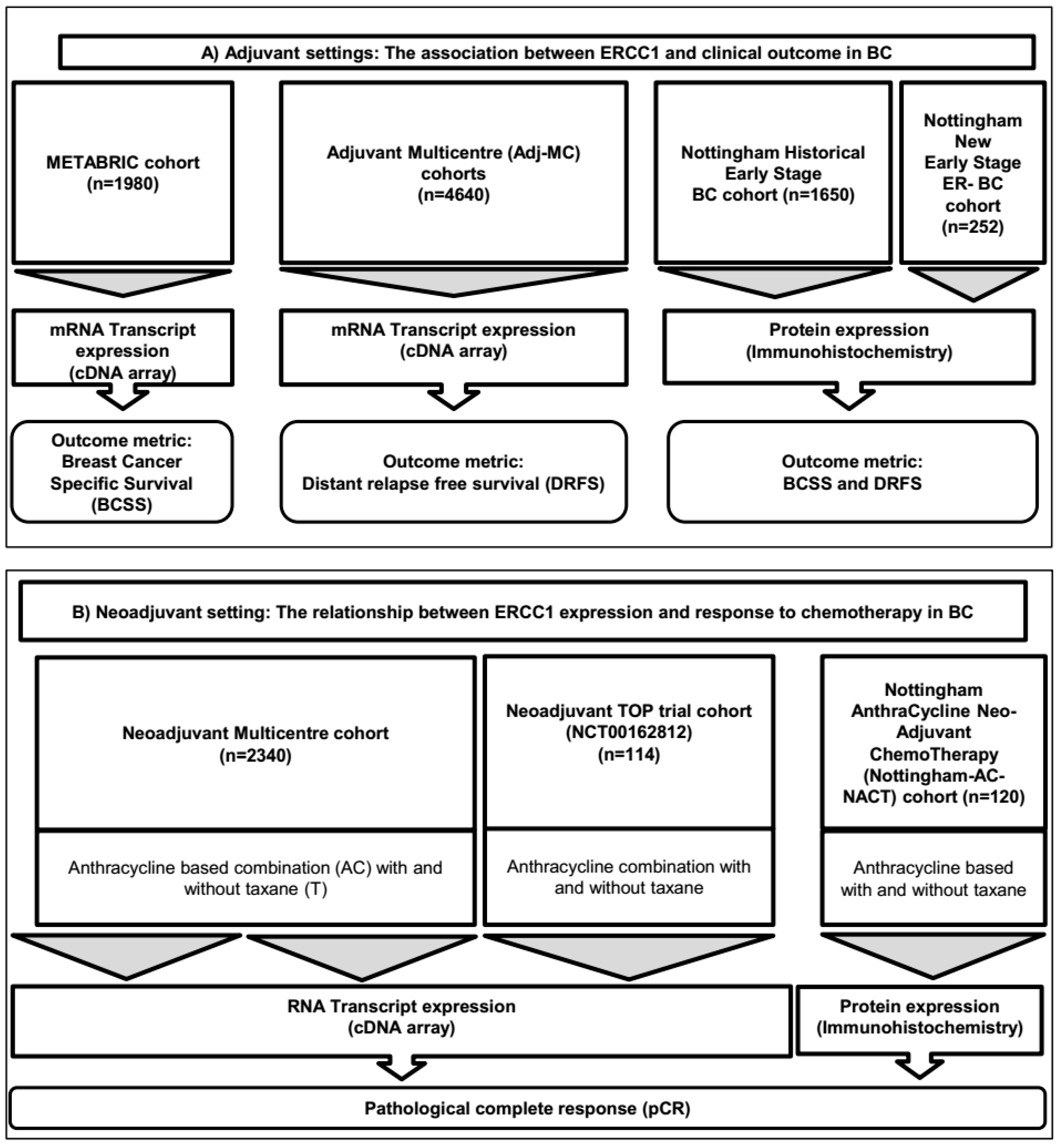
4.1. Study Design and Cohorts
4.2. Outcome Measurements and Patient Cohorts:
4.2.1. ERCC1 Transcript Expression Analysis
4.2.2. Protein Expression Association Analysis
4.3. Adjuvant Setting
4.4. Neo-Adjuvant Setting
4.5. Power Analysis
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgements
Conflicts of Interest
References
- Anampa, J.; Makower, D.; Sparano, J.A. Progress in adjuvant chemotherapy for breast cancer: An overview. BMC Med. 2015, 13, 195. [Google Scholar] [CrossRef] [PubMed]
- Denduluri, N.; Somerfield, M.R.; Giordano, S.H. Selection of Optimal Adjuvant Chemotherapy and Targeted Therapy for Early Breast Cancer: ASCO Clinical Practice Guideline Focused Update. J. Clin. Oncol. 2018, 14, 508–510. [Google Scholar]
- Fujii, T.; Le Du, F.; Xiao, L.; Kogawa, T.; Barcenas, C.H.; Alvarez, R.H.; Valero, V.; Shen, Y.; Ueno, N.T. Effectiveness of an Adjuvant Chemotherapy Regimen for Early-Stage Breast Cancer: A Systematic Review and Network Meta-analysis. JAMA. Oncol. 2015, 1, 1311–1318. [Google Scholar] [CrossRef] [PubMed]
- Krop, I.; Ismaila, N.; Andre, F.; Bast, R.C.; Barlow, W.; Collyar, D.E.; Hammond, M.E. Use of Biomarkers to Guide Decisions on Adjuvant Systemic Therapy for Women with Early-Stage Invasive Breast Cancer: American Society of Clinical Oncology Clinical Practice Guideline Focused Update. J. Clin. Oncol. 2017, 35, 2838–2847. [Google Scholar] [CrossRef] [PubMed]
- Sansregret, L.; Vanhaesebroeck, B.; Swanton, C. Determinants and clinical implications of chromosomal instability in cancer. Nat. Rev. Clin. Oncol. 2018, 15, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Thompson, S.L.; Bakhoum, S.F.; Compton, D.A. Mechanisms of chromosomal instability. Curr. Biol. 2010, 20, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Vargas-Rondon, N.; Villegas, V.E.; Rondon-Lagos, M. The Role of Chromosomal Instability in Cancer and Therapeutic Responses. Cancers (Basel) 2017, 28, 10. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, J.M.; Munro, A.F.; Dunn, J.A.; McConkey, C.; Jordan, S.; Twelves, C.J.; Cameron, D.A.; Thomas, J.; Campbell, F.M.; Rea, D.W.; et al. Predictive markers of anthracycline benefit: A prospectively planned analysis of the UK National Epirubicin Adjuvant Trial (NEAT/BR9601). Lancet Oncol. 2010, 11, 266–274. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group; Peto, R.; Davies, C.; Godwin, J.; Gray, R.; Pan, H.C.; Clarke, M.; Cutter, D.; Darby, S.; McGale, P.; et al. Comparisons between different polychemotherapy regimens for early breast cancer: Meta-analyses of long-term outcome among 100,000 women in 123 randomised trials. Lancet 2012, 379, 432–444. [Google Scholar]
- A’Hern, R.P.; Jamal-Hanjani, M.; Szász, A.M.; Johnston, S.R.; Reis-Filho, J.S.; Roylance, R.; Swanton, C.; et al. Taxane benefit in breast cancer: A role for grade and chromosomal stability. Nat. Rev. Clin. Oncol. 2013, 10, 357–364. [Google Scholar] [CrossRef]
- Swanton, C.; Barbara, N.; Marion, S. Chromosomal instability determines taxane response. Proc. Natl. Acad. Sci. USA 2009, 106, 8671–8676. [Google Scholar] [CrossRef] [PubMed]
- Helleday, T.; Petermann, E.; Lundin, C.; Hodgson, B.; Sharma, R.A. DNA repair pathways as targets for cancer therapy. Nat. Rev. Cancer 2008, 8, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Setton, J.; Lee, N.Y.; Riaz, N.; Powell, S.N. The therapeutic significance of mutational signatures from DNA repair deficiency in cancer. Nat. Commun. 2018, 9, 3292. [Google Scholar] [CrossRef] [PubMed]
- Mocquet, V.; Lainé, J.P.; Riedl, T.; Yajin, Z.; Lee, M.Y.; Egly, J.M. Sequential recruitment of the repair factors during NER: The role of XPG in initiating the resynthesis step. EMBO J. 2008, 27, 155–167. [Google Scholar] [CrossRef] [PubMed]
- George, R.S.; Roohi, I.K.; Gerold, B. Nuclear excision repair-based personalized therapy for non-small cell lung cancer: From hypothesis to reality. Int. J. Biochem. Cell Biol. 2017, 39, 1318–1328. [Google Scholar]
- Fousteri, M.; Mullenders, L.H. Transcription-coupled nucleotide excision repair in mammalian cells: Molecular mechanisms and biological effects. Cell Res. 2008, 18, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Kuraoka, I.; Kobertz, W.R.; Ariza, R.R.; Biggerstaff, M.; Essigmann, J.M.; Wood, R.D. Repair of an Interstrand DNA Cross-link Initiated by ERCC1-XPF Repair/Recombination Nuclease. J. Biol. Chem. 2000, 275, 26632–26636. [Google Scholar] [CrossRef] [PubMed]
- Clauson, C.; Schärer, O.D.; Niedernhofer, L. Advances in Understanding the Complex Mechanisms of DNA Interstrand Cross-Link Repair. Cold Spring Harb. Perspect Biol. 2013, 5, a012732. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Tillison, K.; Kalman, M.V. Downregulation of XPF-ERCC1 enhances cisplatin efficacy in cancer cells. DNA Repair 2010, 9, 745–753. [Google Scholar] [CrossRef]
- Chang, I.Y.; Kim, M.H.; Kim, H.B.; Lee, D.Y.; Kim, S.H.; Kim, H.Y.; You, H.J. Small interfering RNA-induced suppression of ERCC1 enhances sensitivity of human cancer cells to cisplatin. Biochem. Biophys. Res. Commun. 2005, 327, 225–233. [Google Scholar] [CrossRef]
- Song, L.; Ritchie, A.M.; McNeil, E.M.; Li, W.; Melton, D.W. Identification of DNA repair gene Ercc1 as a novel target in melanoma. Pigment Cell Melanoma Res. 2011, 24, 966–971. [Google Scholar] [CrossRef]
- Cimino, G.D.; Pan, C.X.; Henderson, P.T. Personalized medicine for targeted and platinum-based chemotherapy of lung and bladder cancer. Bioanalysis 2013, 5, 369–391. [Google Scholar] [CrossRef]
- Bahamon, B.N.; Gao, F.; Danaee, H. Development and Validation of an ERCC1 Immunohistochemistry Assay for Solid Tumors. Arch. Pathol. Lab. Med. 2016, 140, 1397–1403. [Google Scholar] [CrossRef]
- Pei, D.; Yifeng, W.; Liquan, C.; Yaping, G.; Qinian, W. High ERCC1 expression is associated with platinum-resistance, but not survival in patients with epithelial ovarian cancer. Oncol. Lett. 2016, 12, 857–862. [Google Scholar]
- Steffensen, K.D.; Waldstrøm, M.; Jakobsen, A. The relationship of platinum resistance and ERCC1 protein expression in epithelial ovarian cancer. Int. J. Gynecol. Cancer 2009, 19, 820–825. [Google Scholar] [CrossRef]
- Mesquita, K.A.; Alabdullah, M.; Griffin, M. ERCC1-XPF deficiency is a predictor of olaparib induced synthetic lethality and platinum sensitivity in epithelial ovarian cancers. Gynecol. Oncol. 2019, 153, 416–424. [Google Scholar] [CrossRef]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P. Pathological complete response and long-term clinical benefit in breast cancer: The CTNeoBC pooled analysis. Lancet. 2014, 384, 164–172. [Google Scholar] [CrossRef]
- Pennisi, A.; Kieber-Emmons, T.; Makhoul, I.; Hutchins, L. Relevance of Pathological Complete Response after Neoadjuvant Therapy for Breast Cancer. Breast Cancer (Auckl) 2016, 10, 103–106. [Google Scholar] [CrossRef]
- Rahn, J.J.; Adair, G.M.; Nairn, R.S. Multiple roles of ERCC1-XPF in mammalian interstrand crosslink repair. Environ. Mol. Mutagen. 2010, 51, 567–581. [Google Scholar] [CrossRef]
- Miyoshi, Y.; Kurosumi, M.; Kurebayashi, J.; Matsuura, N.; Takahashi, M.; Tokunaga, E.; Egawa, C. Predictive factors for anthracycline-based chemotherapy for human breast cancer. Breast Cancer (Auckl) 2010, 17, 103–109. [Google Scholar] [CrossRef]
- Pei, X.H.; Yang, Z.; Lv, X.Q.; Li, H.X. Genetic variation in ERCC1 and XPF genes and breast cancer risk. Genet. Mol. Res. 2014, 13, 2259–2267. [Google Scholar] [CrossRef]
- EL Baiomy, M.A.; EI Kashef, W.F. ERCC1 Expression in Metastatic Triple Negative Breast Cancer Patients Treated with Platinum-Based Chemotherapy. Asian. Pac. J. Cancer Prev. 2017, 18, 507–513. [Google Scholar] [CrossRef]
- Ozkan, C.; Gumuskaya, B.; Yaman, S.; Aksoy, S.; Guler, G.; Altundag, K. ERCC1 expression in triple negative breast cancer. J. BUON. 2012, 17, 271–276. [Google Scholar] [CrossRef]
- Dumont, A.; Pannier, D.; Ducoulombier, A.; Tresch, E.; Chen, J.; Kramar, A.; Révillion, F.; Peyrat, J.P.; Bonneterre, J. ERCC1 and CYP1B1 polymorphisms as predictors of response to neoadjuvant chemotherapy in estrogen positive breast tumors. Springerplus 2015, 4, 327. [Google Scholar] [CrossRef][Green Version]
- Mathilde, G.B.; Pierre, R.; Anne, C. ERCC1 and telomere status in breast tumours treated with neoadjuvant chemotherapy and their association with patient prognosis. J. Pathol. Clin. Res. 2016, 2, 234–246. [Google Scholar]
- Fareed, K.R.; Al-Attar, A.; Soomro, I.N.; Kaye, P.V.; Patel, J.; Lobo, D.N.; Parsons, S.L.; Madhusudan, S. Tumour regression and ERCC1 nuclear protein expression predict clinical outcome in patients with gastro-oesophageal cancer treated with neoadjuvant chemotherapy. Br. J. Cancer 2010, 102, 1600–1607. [Google Scholar] [CrossRef]
- Gossage, L.; Madhusudan, S. Current status of excision repair cross complementing-group 1 (ERCC1) in cancer. Cancer Treat Rev. 2007, 33, 565–577. [Google Scholar] [CrossRef]
- Kirschner, K.; Melton, D.W. Multiple roles of the ERCC1-XPF endonuclease in DNA repair and resistance to anticancer drugs. Anticancer Res. 2010, 30, 3223–3232. [Google Scholar]
- McNeil, E.M.; Melton, D.W. DNA repair endonuclease ERCC1-XPF as a novel therapeutic target to overcome chemoresistance in cancer therapy. Nucleic Acids Res. 2012, 40, 9990–10004. [Google Scholar] [CrossRef]
- Friboulet, L.; Olaussen, K.A.; Pignon, J.P. ERCC1 isoform expression and DNA repair in non-small-cell lung cancer. N. Engl. J. Med. 2013, 368, 1101–1110. [Google Scholar] [CrossRef]
- Smith, D.H.; Fiehn, A.M.; Fogh, L.; Christensen, I.J.; Hansen, T.P.; Stenvang, J.; Nielsen, H.J.; Nielsen, K.V.; Hasselby, J.P.; Brünner, N.; et al. Measuring ERCC1 protein expression in cancer specimens: validation of a novel antibody. Sci. Rep. 2014, 4, 4313. [Google Scholar] [CrossRef]
- Abdel-Fatah, T.M.A.; Agarwal, D.; Liu, D.X.; Russell, R.; Rueda, O.M.; Liu, K.; Xu, B. SPAG5 as a prognostic biomarker and chemotherapy sensitivity predictor in breast cancer: a retrospective, integrated genomic, transcriptomic, and protein analysis. Lancet Oncol. 2016, 17, 1004–1018. [Google Scholar] [CrossRef]
- Abdel-Fatah, T.M.; McArdle, S.E.; Agarwal, D. HAGE in Triple-Negative Breast Cancer Is a Novel Prognostic, Predictive, and Actionable Biomarker: A Transcriptomic and Protein Expression Analysis. Clin. Cancer Res. 2016, 22, 905–914. [Google Scholar] [CrossRef]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M. Reporting recommendations for tumor marker prognostic studies (REMARK). Nature Clinical Practice Oncology 2005, 2, 416–422. [Google Scholar]
- Holm, S. A simple sequentially rejective multiple test procedure. Scand J. Stat. 1979, 6, 65–70. [Google Scholar]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M.; Statistics Subcommittee of the NCI-EORTC Working Group on Cancer Diagnostics. Reporting recommendations for tumor marker prognostic studies (REMARK). J. Natl. Cancer Inst. 2005, 97, 1180–1184. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ERCC1 mRNA Expression | p-Value | * p-Value(Adjusted) | ||
|---|---|---|---|---|
| Low | High | |||
| (A) Pathological Parameters | ||||
| Tumour Size | ||||
| ≤1cm | 43 (4.5%) | 43 (4.4%) | 0.481 | 5.2910 |
| >1–2cm | 247 (25.7%) | 279 (28.8%) | ||
| >2–4cm | 620 (64.5%) | 601 (62.0%) | ||
| >4cm | 51 (5.3%) | 46 (4.7%) | ||
| Tumour Grade | ||||
| 1 | 35 (3.7%) | 130 (14.1%) | 4.4 × 10−37 | <0.00001 |
| 2 | 305 (32.0%) | 460 (49.8%) | ||
| 3 | 612 (64.3%) | 334 (36.1%) | ||
| Lymph Node Group | ||||
| Negative | 486 (49.8%) | 528 (54.2%) | 0.051 | 0.0623 |
| Positive | 490 (50.2%) | 446 (45.8%) | ||
| Histological Types | ||||
| IDC-NST | 837 (85.8%) | 704 (72.3%) | 1.33 × 10−15 | <0.00001 |
| Medullary Carcinoma | 20 (2.0%) | 12 (1.2%) | ||
| Invasive special type | 104 (10.7%) | 247 (25.4%) | ||
| Invasive others | 15 (1.5%) | 11 (1.1%) | ||
| Ki67 Expression | ||||
| Negative | 375 (38.4%) | 600 (61.6%) | 1.37 × 10−24 | <0.00001 |
| Positive | 601 (61.6%) | 374 (38.4%) | ||
| P53 Mutation | ||||
| Wild type | 325 (82.9%) | 383 (92.3%) | 4.9 × 10−5 | <0.00001 |
| Mutant | 67 (17.1%) | 32 (7.7%) | ||
| ER Expression | ||||
| Negative | 332 (34.0%) | 126 (12.9%) | 4.8 × 10−28 | <0.00001 |
| Positive | 644 (66.0%) | 848 (87.1%) | ||
| PAM 50 Luminal A | ||||
| Negative | 770 (78.9%) | 466 (48.1%) | 4.45 × 10−45 | <0.00001 |
| Positive | 206 (21.1%) | 502 (51.9%) | ||
| PAM 50 Luminal B | ||||
| Negative | 684 (70.1%) | 775 (80.1%) | 3.68 × 10−7 | <0.00001 |
| Positive | 292 (29.9%) | 193 (19.9%) | ||
| PAM 50 Her2 | ||||
| Negative | 799 (81.9%) | 909 (93.9%) | 4.39 × 10−16 | <0.00001 |
| Positive | 177 (18.1%) | 59 (6.1%) | ||
| PAM 50 Basal | ||||
| Negative | 751 (76.9%) | 871 (90.0%) | 1.089 × 10−14 | <0.00001 |
| Positive | 225 (23.1%) | 97 (10.0%) | ||
| Integrative Molecular Clusters | ||||
| Int Clust 1 | 101 (10.3%) | 35 (3.6%) | 1.163 × 10−60 | <0.00001 |
| Int Clust 2 | 41 (4.2%) | 30 (3.1%) | ||
| Int Clust 3 | 78 (8.0%) | 210 (21.6%) | ||
| Int Clust 4 | 144 (14.8%) | 187 (19.2%) | ||
| Int Clust 5 | 139 (14.2%) | 46 (4.7%) | ||
| Int Clust 6 | 52 (5.3%) | 33 (3.4%) | ||
| Int Clust 7 | 74 (7.6%) | 112 (11.5%) | ||
| Int Clust 8 | 77 (7.9%) | 221 (22.7%) | ||
| Int Clust 9 | 108 (11.1%) | 38 (3.9%) | ||
| Int Clust 10 | 162 (16.6%) | 62 (6.4%) | ||
| Genufu Sub-Types | ||||
| ER−/Her-2− | 104 (21.4%) | 44 (8.8%) | 7.43 × 10−37 | <0.00001 |
| ER+/Her-2– (high proliferation) | 212 (43.7%) | 148 (29.7%) | ||
| ER+/Her-2– (low proliferation) | 85 (17.5%) | 281 (56.3%) | ||
| Her-2 + | 84 (17.3%) | 26 (5.2%) | ||
| Variables | HR | 95.0% CI | p Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| ERCC1 mRNA expression (+) | 1.43 | 1.02 | 2.01 | 0.039 * |
| ER (+) | 0.75 | 0.38 | 1.49 | 0.411 |
| PR (+) | 0.91 | 0.63 | 1.32 | 0.624 |
| HER2 overexpression | 0.82 | 0.36 | 1.85 | 0.63 |
| TP53 mutation | 1.81 | 1.24 | 2.63 | 0.002 * |
| Tumour Size (continuous) | 1.01 | 1.01 | 1.02 | 0.001* |
| Lymph node (LN) stage | 1.2 × 10−6 * | |||
| Negative | 1 | |||
| 1–3 positive LNs | 1.87 | 1.25 | 2.79 | |
| > 3 positive LNs | 3.33 | 2.12 | 5.23 | |
| Histological grade | 0.563 | |||
| Low | 1 | |||
| Intermediate | 0.98 | 0.46 | 2.09 | |
| High | 1.2 | 0.55 | 2.62 | |
| PAM-50 subtypes | 0.049 * | |||
| PAM-50-LUM A | 1 | 0.97 | 2.16 | |
| PAM-50-LUM B | 1.44 | 0.43 | 2.16 | |
| PAM-50-LUM HER2 | 0.96 | 0.5 | 3.04 | |
| PAM-50-LUM Basal | 1.24 | 1.17 | 4.56 | |
| PAM-50-Normal like | 2.31 | |||
| IntClust Members | 0.189 | |||
| IntClust 1 | 1 | |||
| IntClust 2 | 1.28 | 0.59 | 2.8 | |
| IntClust 3 | 0.56 | 0.25 | 1.24 | |
| IntClust 4 | 0.8 | 0.4 | 1.59 | |
| IntClust 5 | 2.47 | 0.94 | 6.53 | |
| IntClust 6 | 1.15 | 0.5 | 2.64 | |
| IntClust 7 | 1.08 | 0.49 | 2.38 | |
| IntClust 8 | 1.03 | 0.52 | 2.05 | |
| IntClust 9 | 1.31 | 0.66 | 2.58 | |
| IntClust 10 | 0.81 | 0.38 | 1.76 | |
| Hormone therapy | 0.64 | 0.43 | 0.96 | 0.031 * |
| Chemotherapy | 0.93 | 0.62 | 1.41 | 0.741 |
| Interaction term | 2.86 | 1.1 | 7.42 | 0.09 |
| Hormone therapy * ER (IHC) | ||||
| Interaction term | 2.11 | 1.23 | 3.95 | 0.020 * |
| Chemotherapy * ERCC1 | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdel-Fatah, T.M.A.; Ali, R.; Sadiq, M.; Moseley, P.M.; Mesquita, K.A.; Ball, G.; Green, A.R.; Rakha, E.A.; Chan, S.Y.T.; Madhusudan, S. ERCC1 Is a Predictor of Anthracycline Resistance and Taxane Sensitivity in Early Stage or Locally Advanced Breast Cancers. Cancers 2019, 11, 1149. https://doi.org/10.3390/cancers11081149
Abdel-Fatah TMA, Ali R, Sadiq M, Moseley PM, Mesquita KA, Ball G, Green AR, Rakha EA, Chan SYT, Madhusudan S. ERCC1 Is a Predictor of Anthracycline Resistance and Taxane Sensitivity in Early Stage or Locally Advanced Breast Cancers. Cancers. 2019; 11(8):1149. https://doi.org/10.3390/cancers11081149
Chicago/Turabian StyleAbdel-Fatah, Tarek M. A., Reem Ali, Maaz Sadiq, Paul M. Moseley, Katia A. Mesquita, Graham Ball, Andrew R. Green, Emad A. Rakha, Stephen Y. T. Chan, and Srinivasan Madhusudan. 2019. "ERCC1 Is a Predictor of Anthracycline Resistance and Taxane Sensitivity in Early Stage or Locally Advanced Breast Cancers" Cancers 11, no. 8: 1149. https://doi.org/10.3390/cancers11081149
APA StyleAbdel-Fatah, T. M. A., Ali, R., Sadiq, M., Moseley, P. M., Mesquita, K. A., Ball, G., Green, A. R., Rakha, E. A., Chan, S. Y. T., & Madhusudan, S. (2019). ERCC1 Is a Predictor of Anthracycline Resistance and Taxane Sensitivity in Early Stage or Locally Advanced Breast Cancers. Cancers, 11(8), 1149. https://doi.org/10.3390/cancers11081149