Neoadjuvant Treatment in Locally Advanced Pancreatic Cancer (LAPC) Patients with FOLFIRINOX or Gemcitabine NabPaclitaxel: A Single-Center Experience and a Literature Review


 , ,
, , 
Abstract
:1. Introduction
2. Results
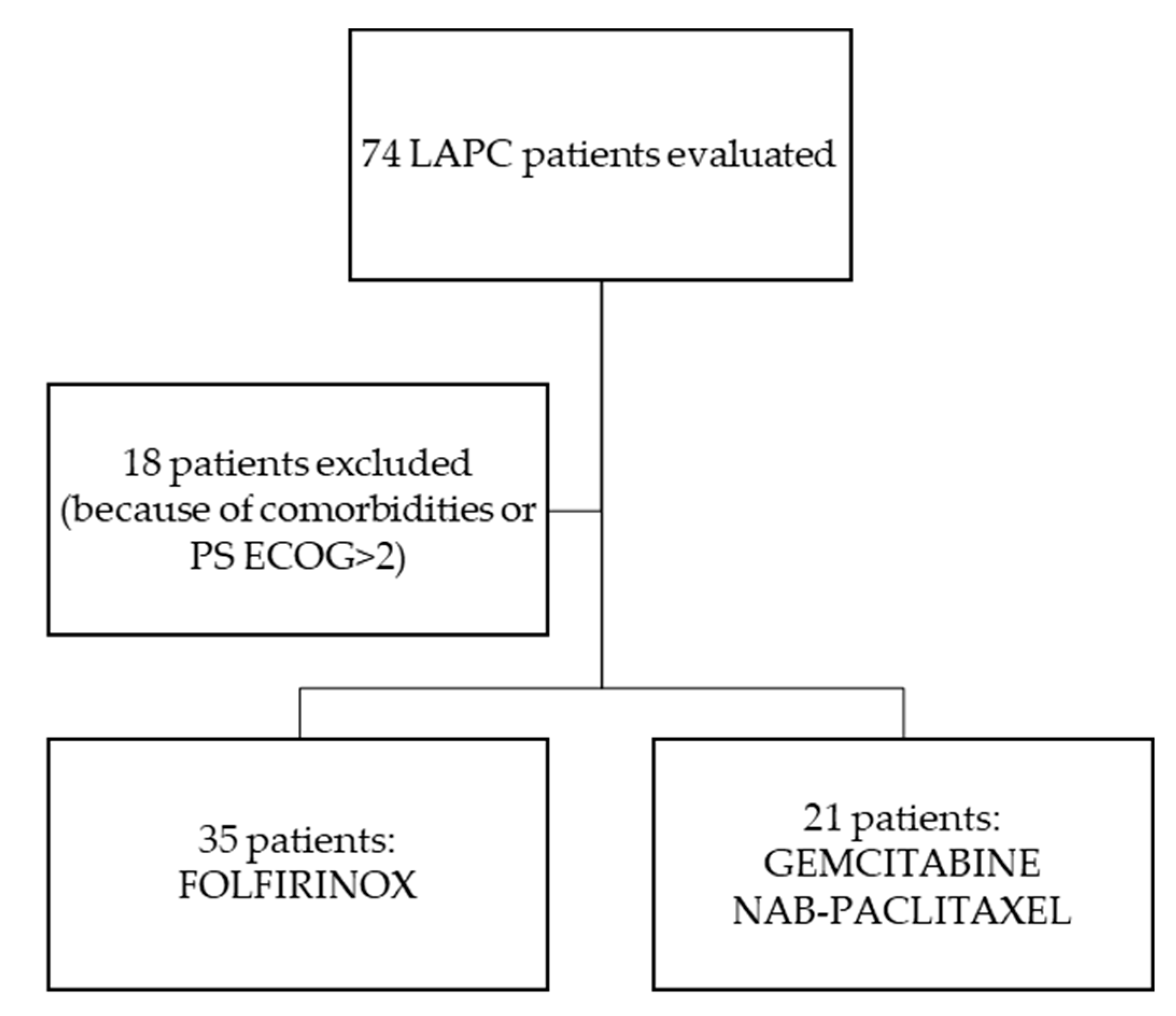
2.1. Patient Cohort
2.1.1. Characteristics of the Patients
2.1.2. Treatments
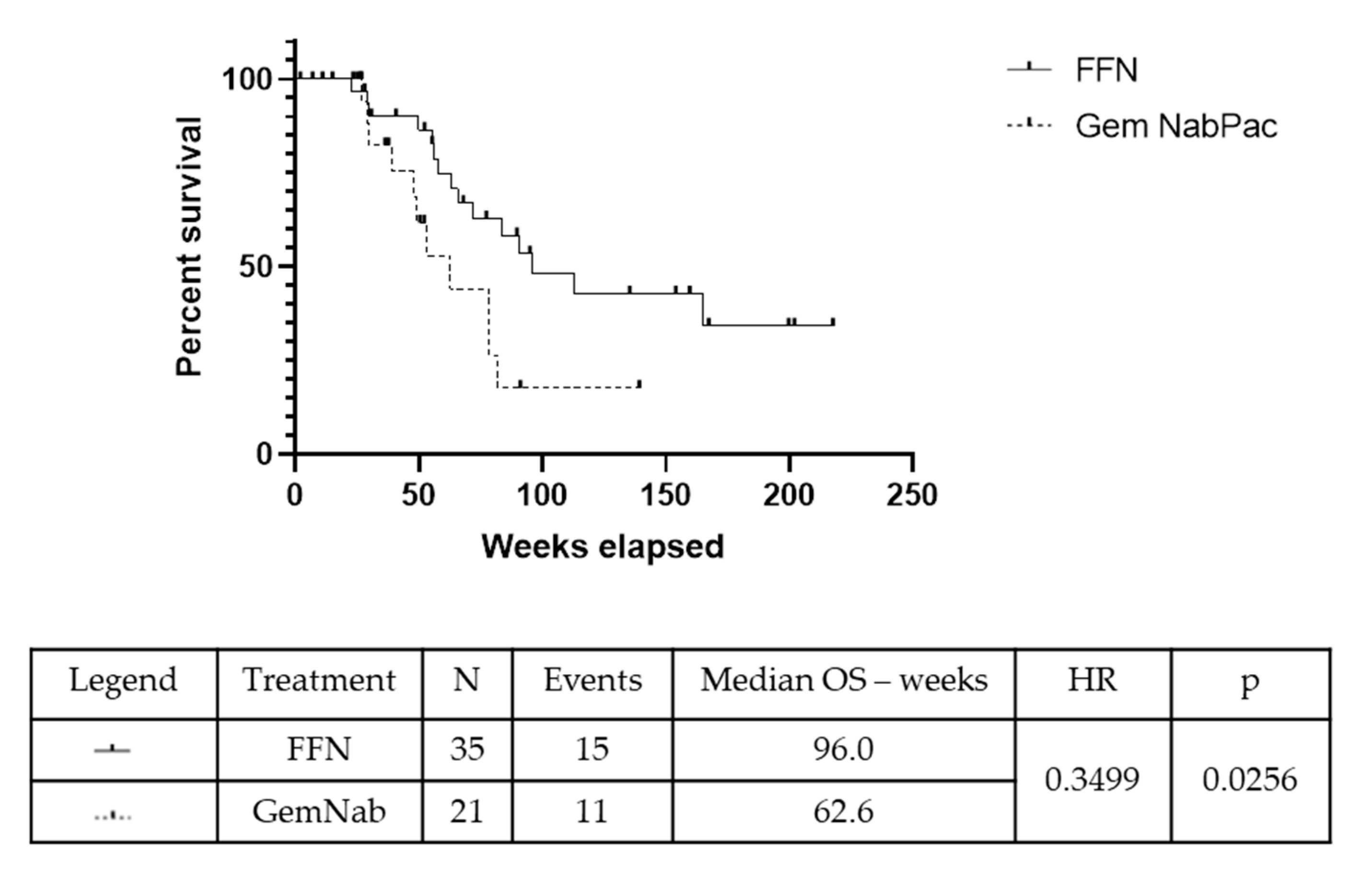
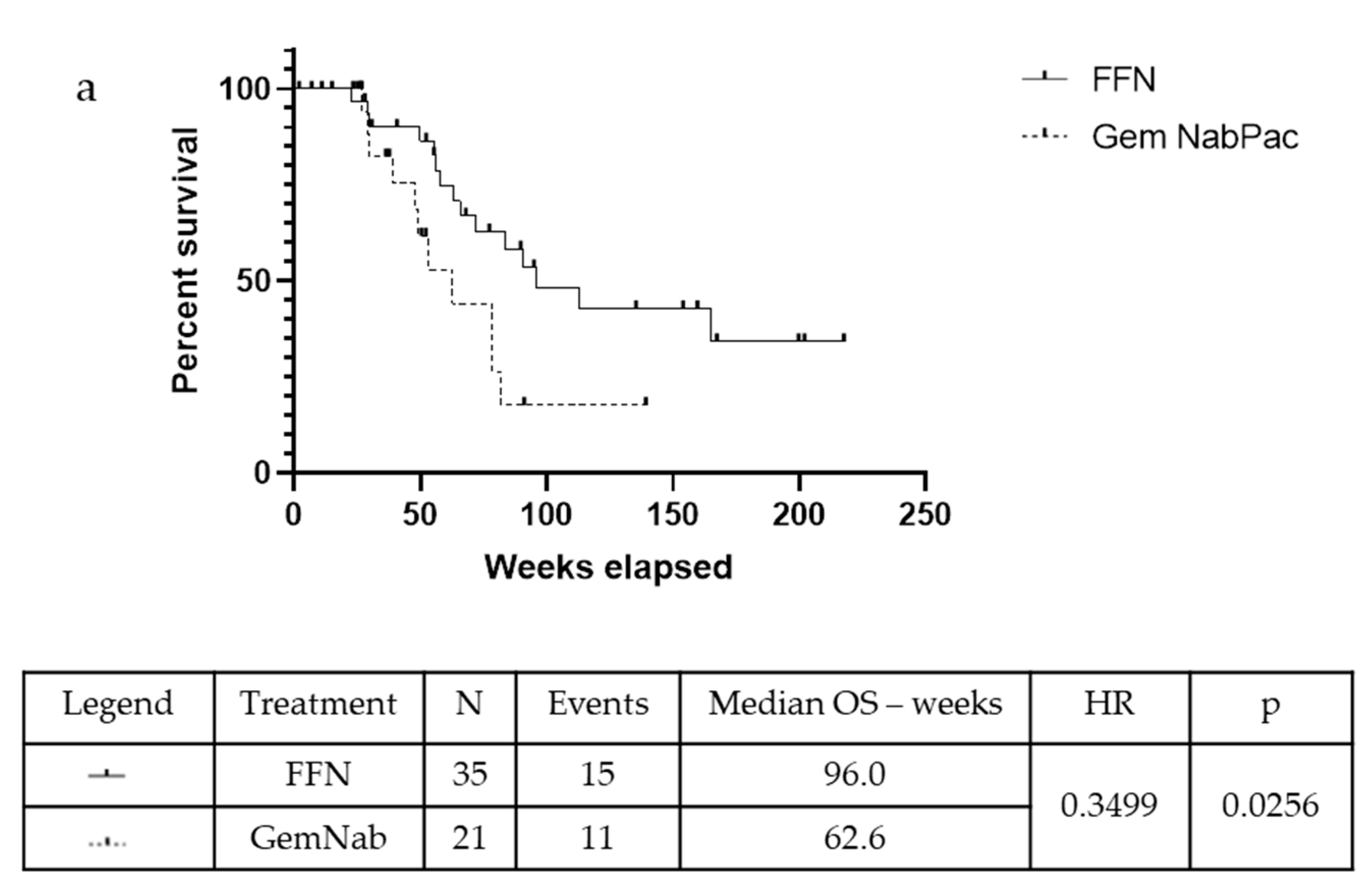
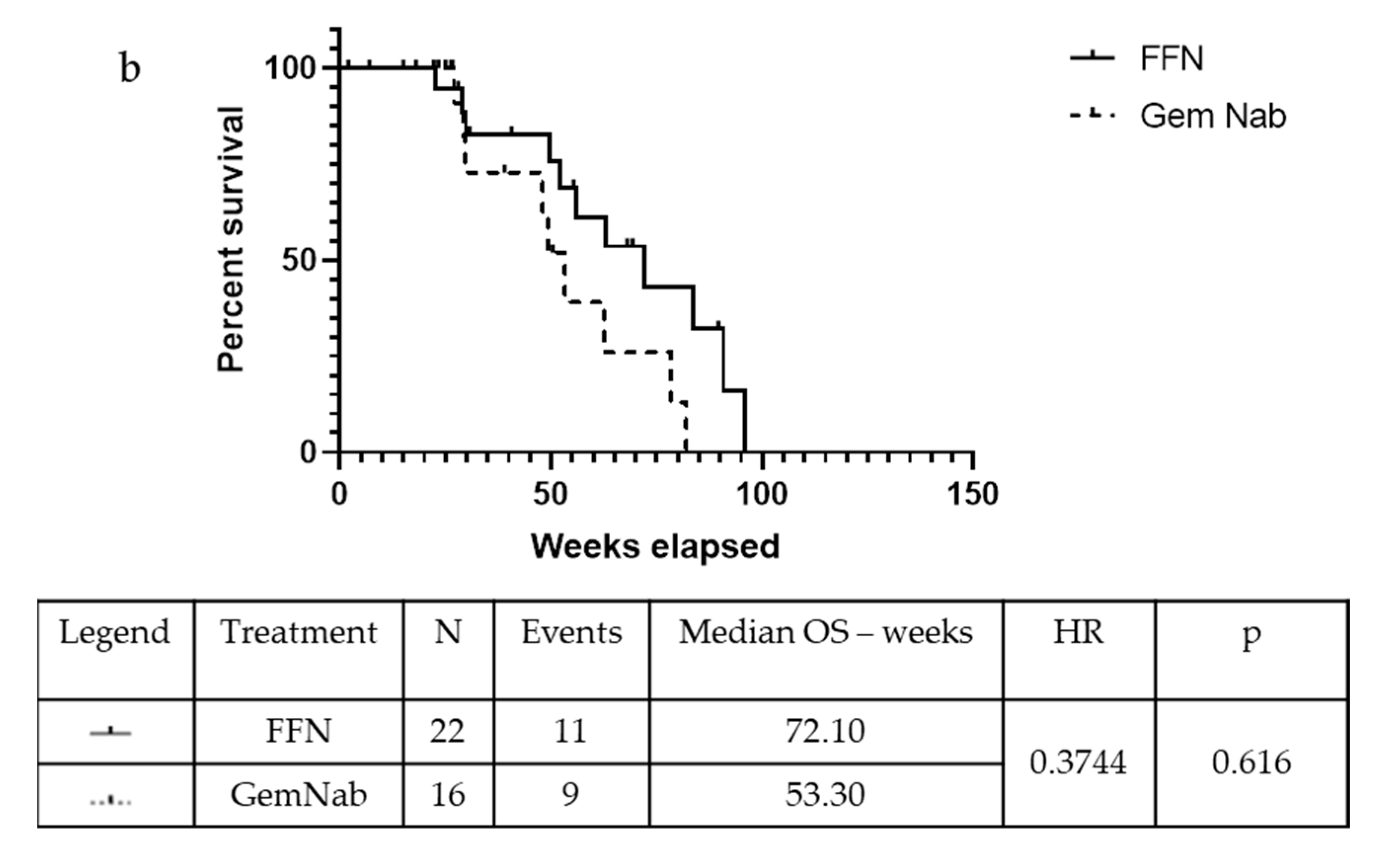
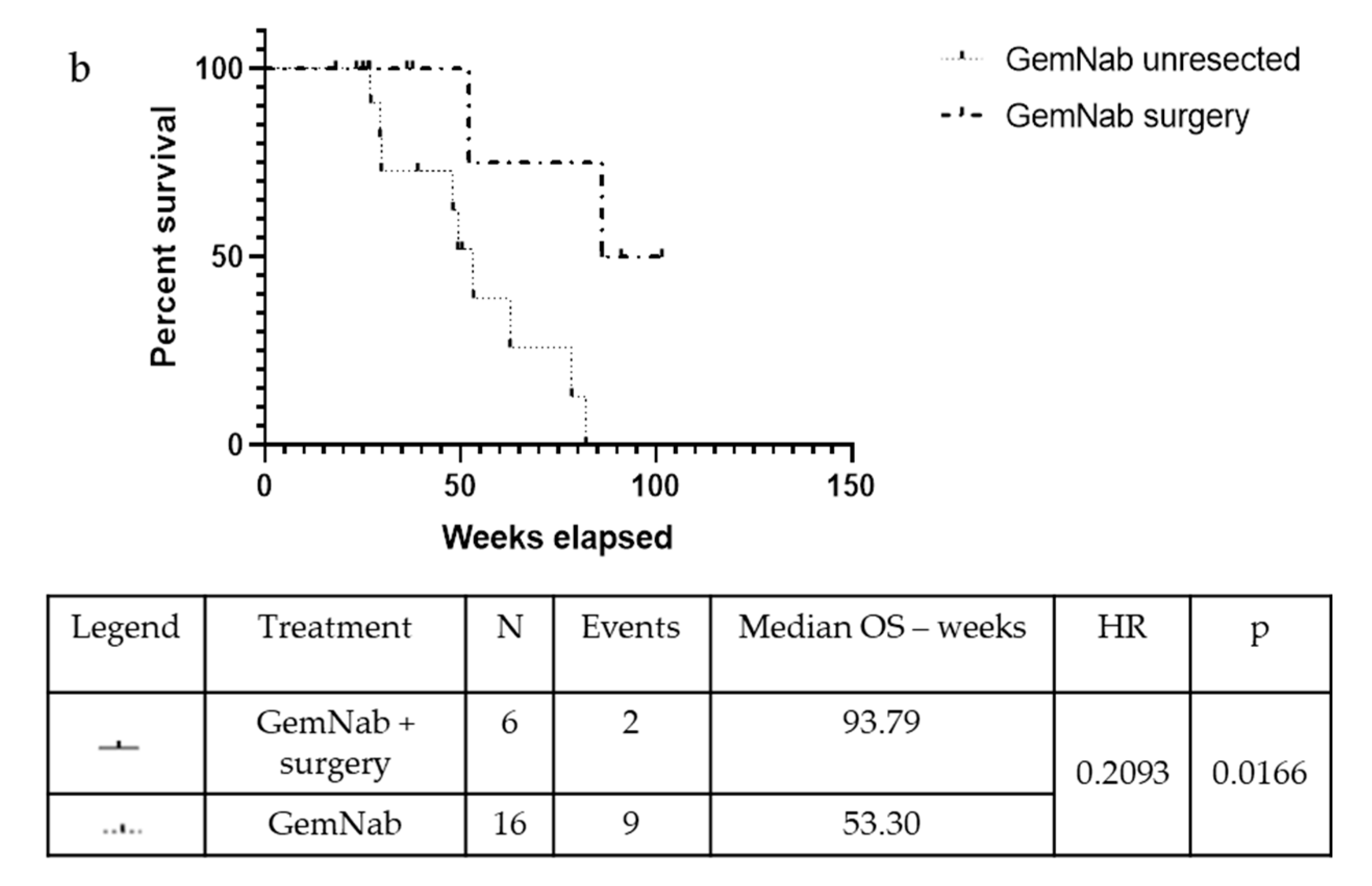
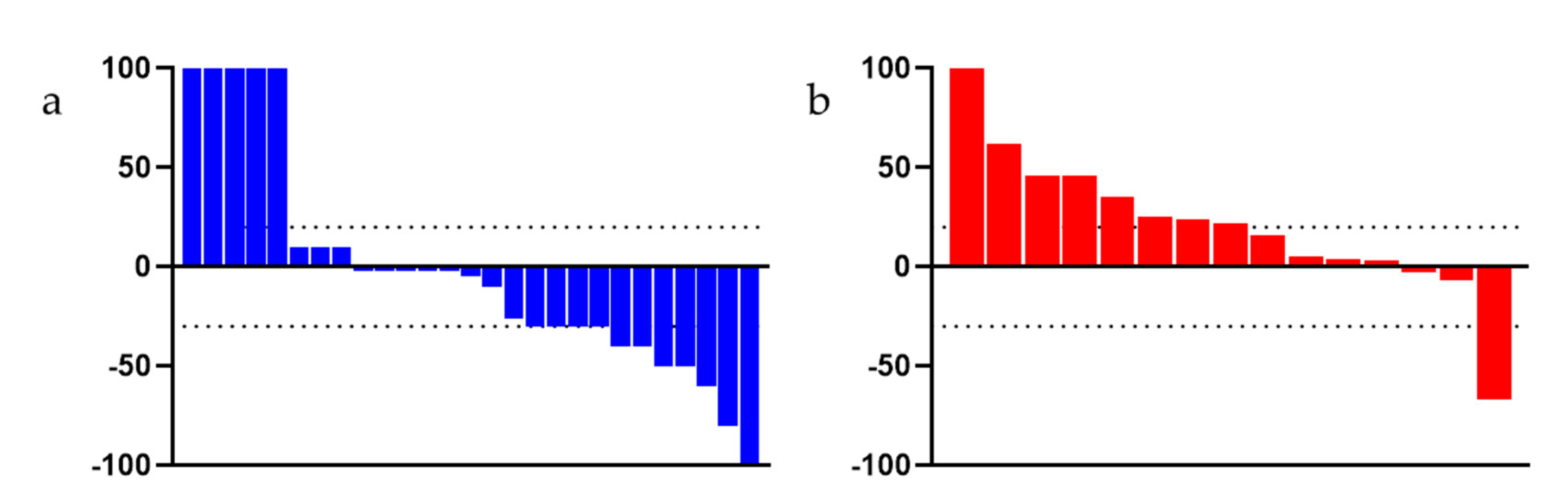
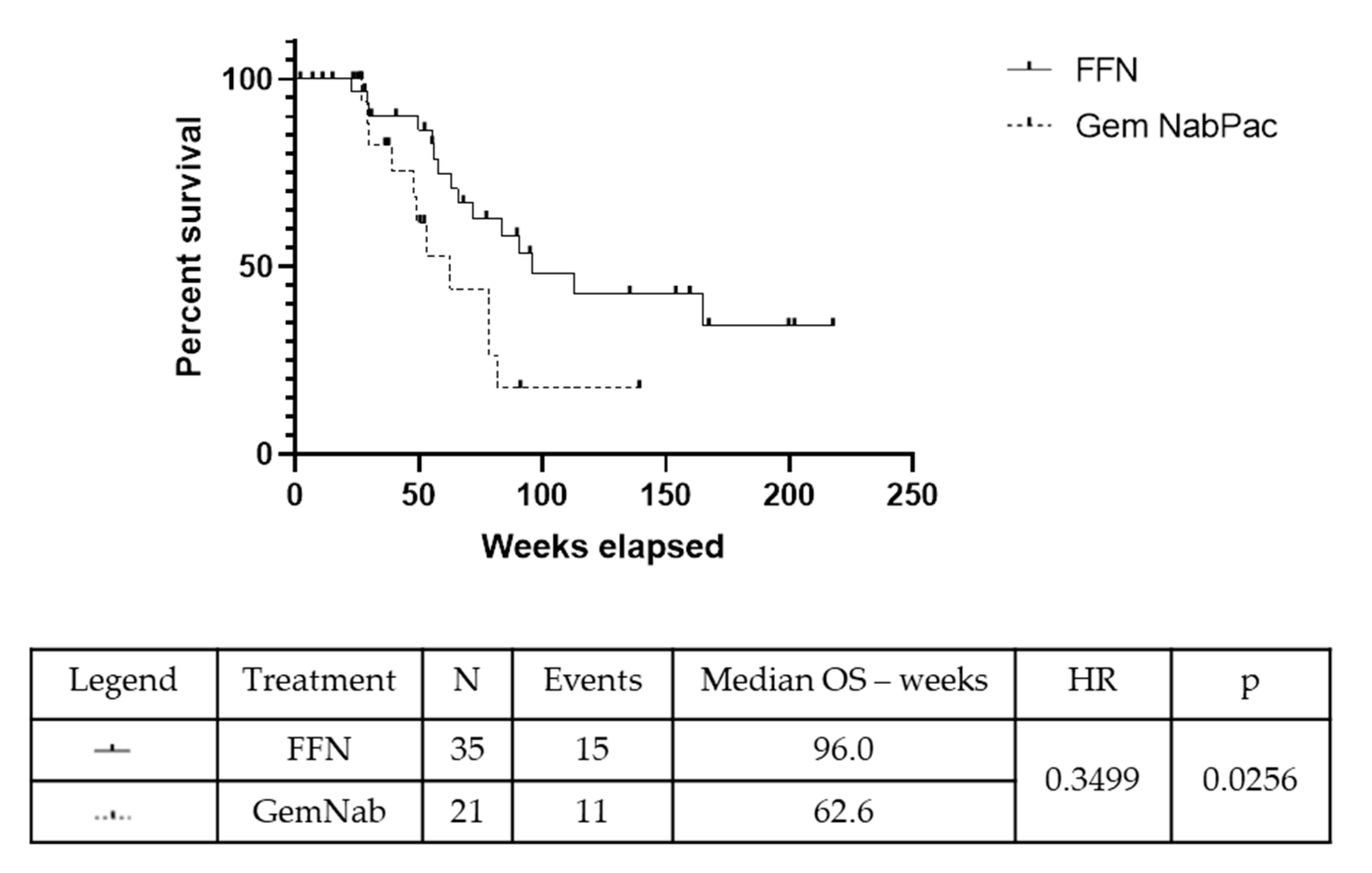
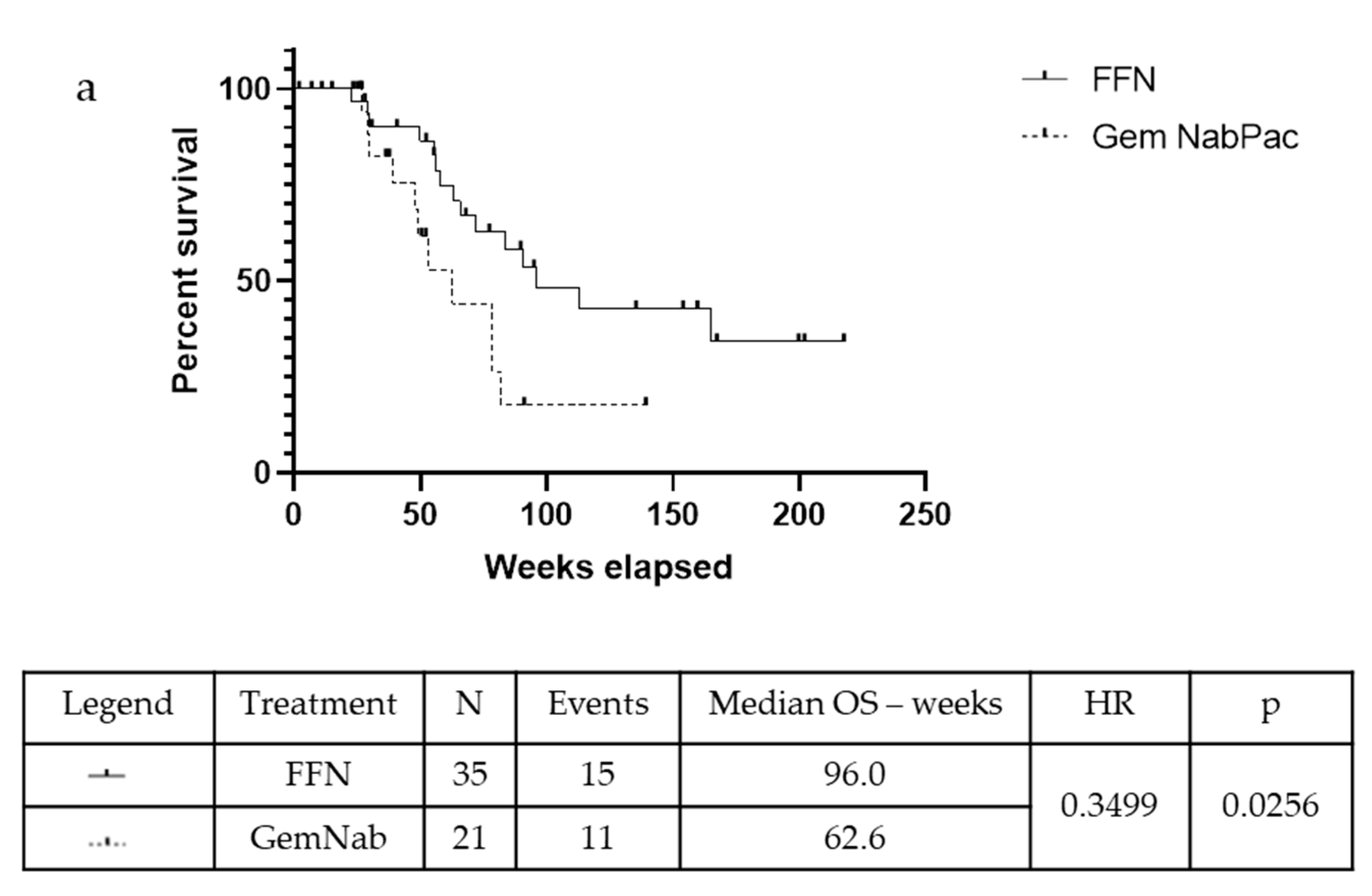
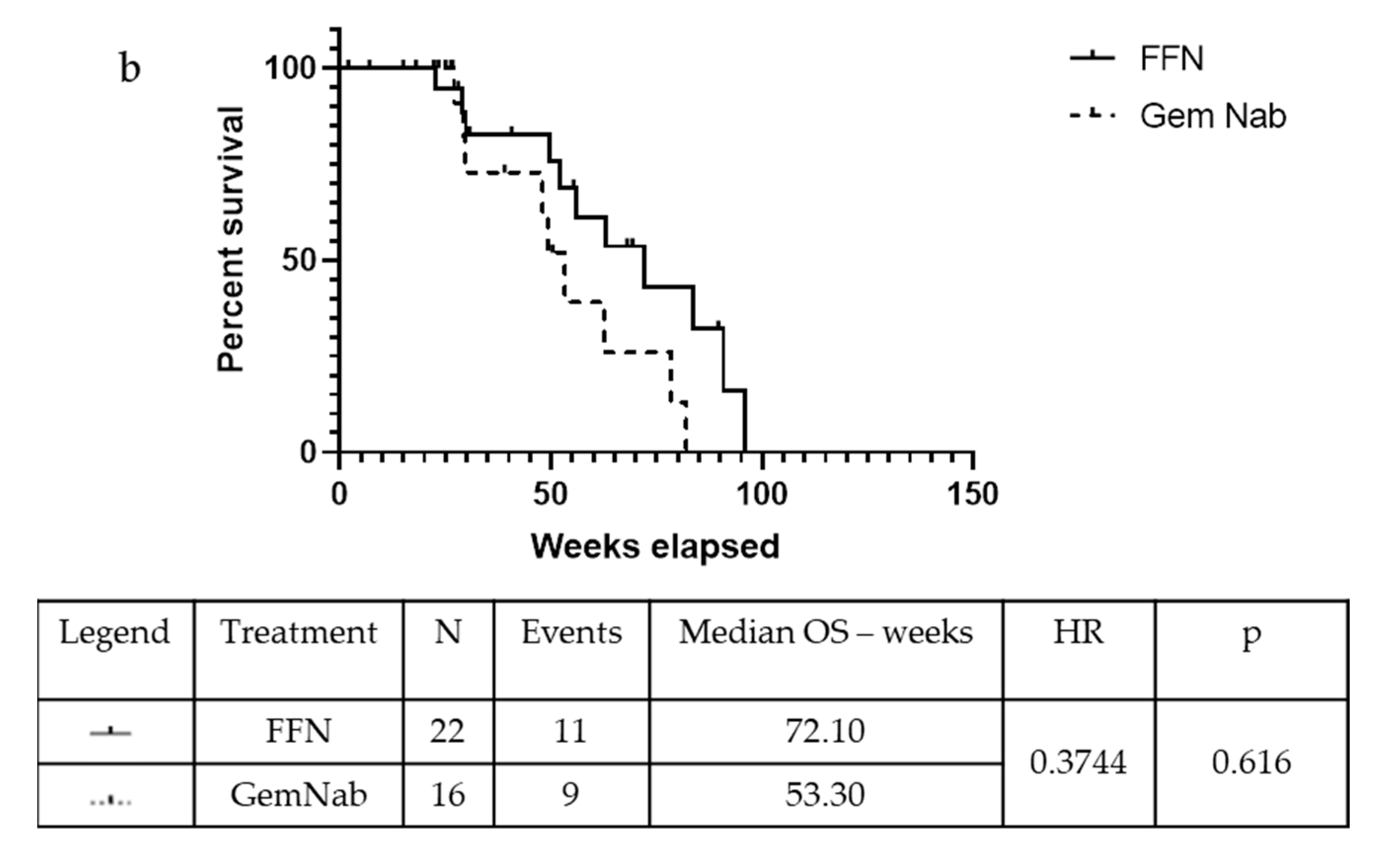
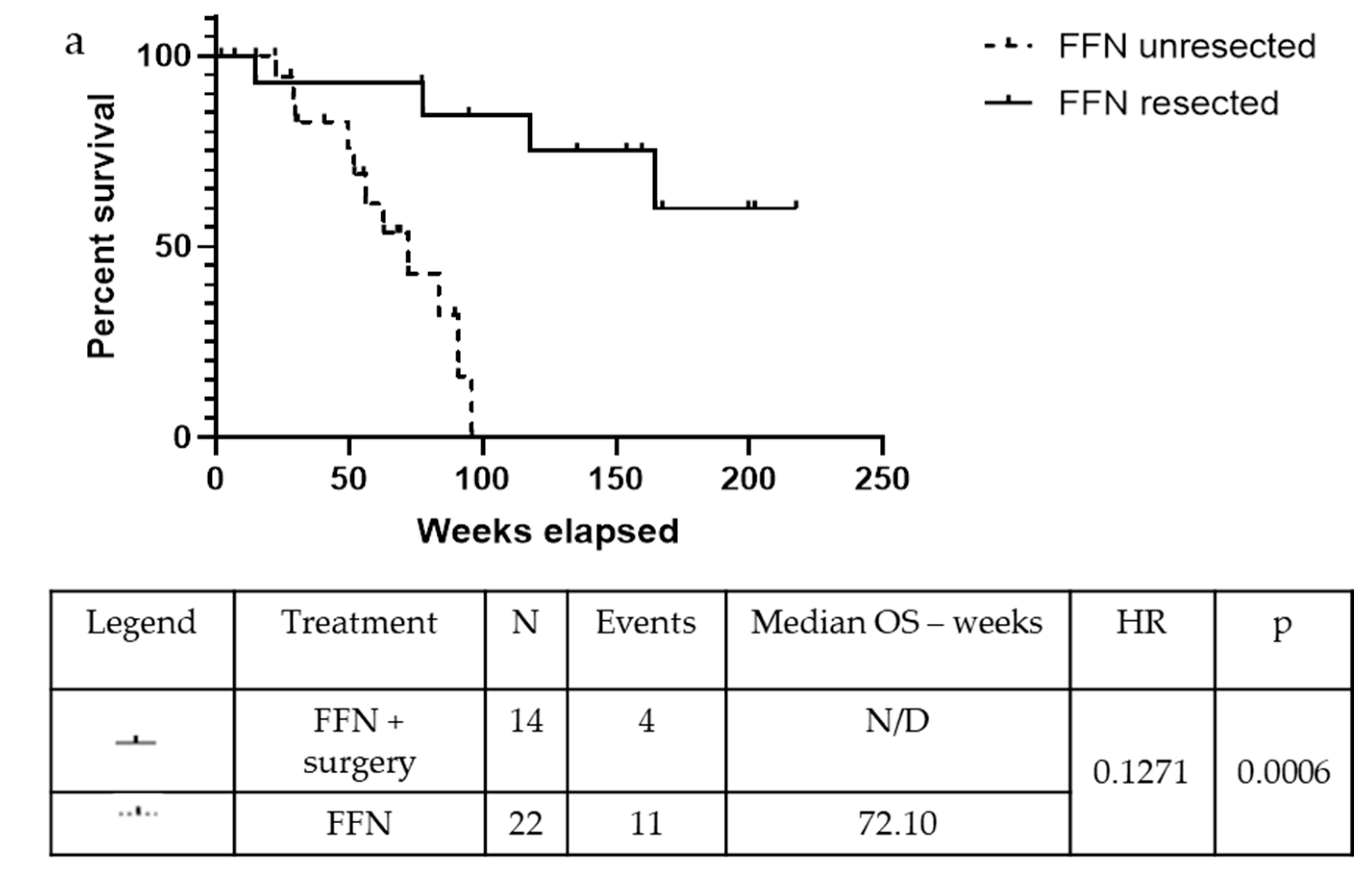
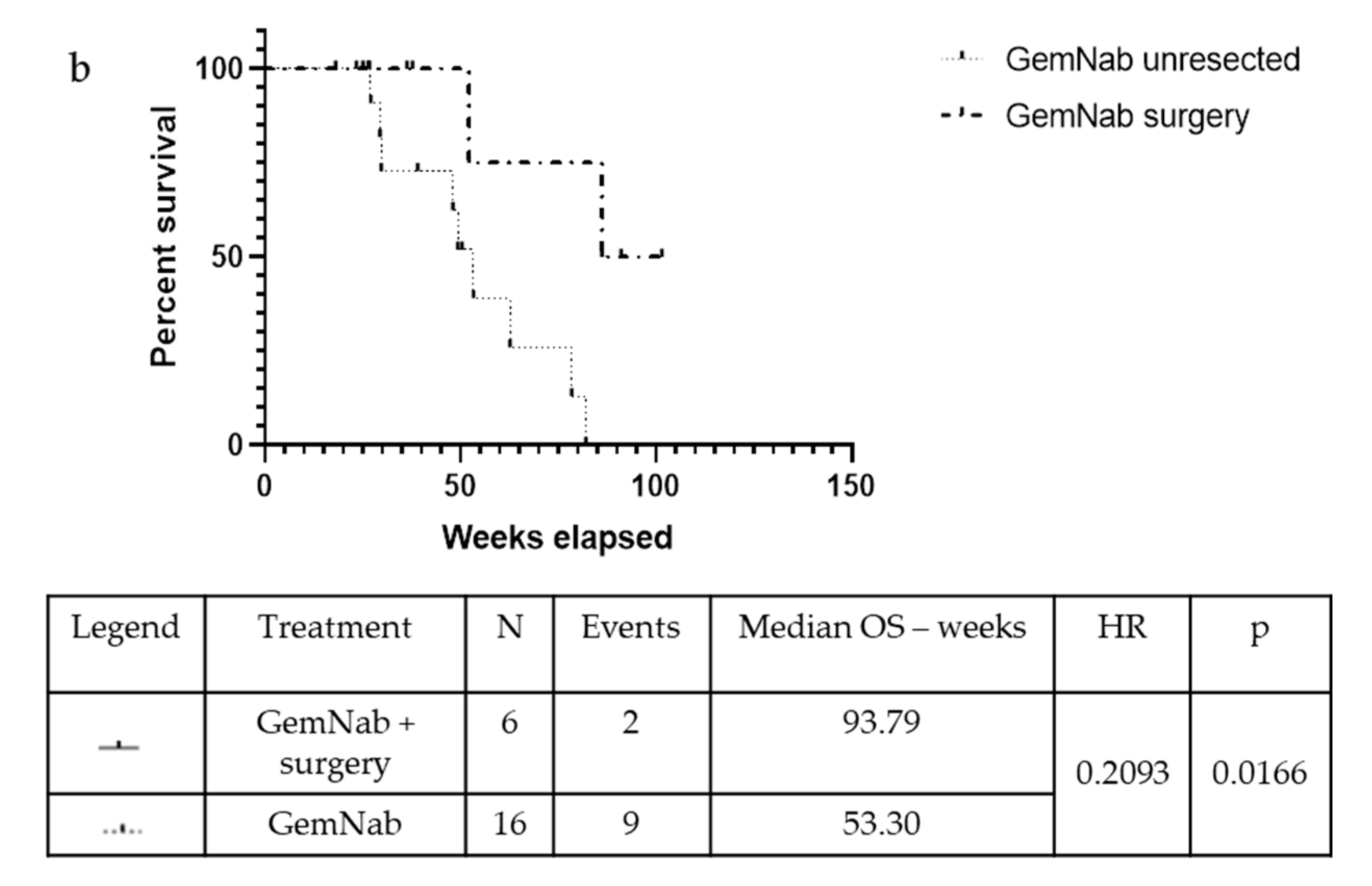
2.1.3. Efficacy
2.1.4. Prognostic Factors
2.1.5. Adverse Events
2.2. Review of the Literature
2.2.1. FOLFIRINOX
2.2.2. Gemcitabine-NabPaclitaxel
2.2.3. Studies Involving both FFN and GemNab
3. Discussion
4. Materials and Methods
4.1. Patients Selection
4.2. Study Design
4.3. Efficacy and Survival Outcomes
4.4. Statistical Analysis
4.5. Ethics
4.6. Literature Data
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef]
- Kamarajah, S.K.; Burns, W.R.; Frankel, T.L.; Cho, C.S.; Nathan, H. Validation of the American Joint Commission on Cancer (AJCC) 8th Edition Staging System for Patients with Pancreatic Adenocarcinoma: A Surveillance, Epidemiology and End Results (SEER) Analysis. Ann. Surg. Oncol. 2017, 24, 2023–2030. [Google Scholar] [CrossRef]
- Hidalgo, M. Pancreatic Cancer Medical Progress. N. Engl. J. Med. 2010, 362, 1605–1617. [Google Scholar] [CrossRef]
- Shaib, W.L.; Ip, A.; Cardona, K.; Alese, O.B.; Maithel, S.K.; Kooby, D.; Landry, J.; El-Rayes, B.F. Contemporary Management of Borderline Resectable and Locally Advanced Unresectable Pancreatic Cancer. Oncologist 2016, 21, 178–187. [Google Scholar] [CrossRef] [Green Version]
- Evans, D.B.; Ritch, P.S.; Erickson, B.A. Neoadjuvant Therapy for Localized Pancreatic Cancer. Ann. Surg. 2015, 261, 18–20. [Google Scholar] [CrossRef]
- Pawlik, T.M.; Laheru, D.; Hruban, R.H.; Coleman, J.A.; Wolfgang, C.L.; Campbell, K.; Ali, S.; Fishman, E.K.; Schulick, R.D.; Herman, J.M.; et al. Evaluating the Impact of a Single-Day Multidisciplinary Clinic on the Management of Pancreatic Cancer. Ann. Surg. Oncol. 2008, 15, 2081–2088. [Google Scholar] [CrossRef] [Green Version]
- Conroy, T.; Paillot, B.; François, E.; Bugat, R.; Jacob, J.H.; Stein, U.; Nasca, S.; Metges, J.P.; Rixe, O.; Michel, P.; et al. Irinotecan plus Oxaliplatin and Leucovorin-Modulated Fluorouracil in Advanced Pancreatic Cancer—A Groupe Tumeurs Digestives of the Fédération Nationale Des Centres de Lutte Contre le Cancer Study. J. Clin. Oncol. 2005, 23, 1228–1236. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.-L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. FOLFIRINOX versus Gemcitabine for Metastatic Pancreatic Cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [Green Version]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased Survival in Pancreatic Cancer with Nab-Paclitaxel plus Gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef]
- Chauffert, B.; Mornex, F.; Bonnetain, F.; Rougier, P.; Mariette, C.; Bouché, O.; Bosset, J.F.; Aparicio, T.; Mineur, L.; Azzedine, A.; et al. Phase III Trial Comparing Intensive Induction Chemoradiotherapy (60 Gy, Infusional 5-FU and Intermittent Cisplatin) Followed by Maintenance Gemcitabine with Gemcitabine Alone for Locally Advanced Unresectable Pancreatic Cancer. Definitive Results of the 2000-01 FFCD/SFRO study. Ann. Oncol. 2008, 19, 1592–1599. [Google Scholar] [CrossRef]
- Loehrer, P.J.; Feng, Y.; Cardenes, H.; Wagner, L.; Brell, J.M.; Cella, D.; Flynn, P.; Ramanathan, R.K.; Crane, C.H.; Alberts, S.R.; et al. Gemcitabine Alone versus Gemcitabine plus Radiotherapy in Patients with Locally Advanced Pancreatic Cancer: An Eastern Cooperative Oncology Group Trial. J. Clin. Oncol. 2011, 29, 4105–4112. [Google Scholar] [CrossRef]
- Mancini, B.R.; Stein, S.; Lloyd, S.; Rutter, C.E.; James, E.; Chang, B.W.; Lacy, J.; Johung, K.L. Chemoradiation after FOLFIRINOX for Borderline Resectable or Locally Advanced Pancreatic Cancer. J. Gastrointest. Oncol. 2018, 9, 982–988. [Google Scholar] [CrossRef]
- Rombouts, S.J.; Walma, M.S.; Vogel, J.A.; van Rijssen, L.B.; Wilmink, J.W.; Mohammad, N.H.; van Santvoort, H.C.; Molenaar, I.Q.; Besselink, M.G. Systematic Review of Resection Rates and Clinical Outcomes after FOLFIRINOX-Based Treatment in Patients with Locally Advanced Pancreatic Cancer. Ann. Surg. Oncol. 2016, 23, 4352–4360. [Google Scholar] [CrossRef]
- Tempero, M.A.; Malafa, M.P.; Chiorean, E.G.; Czito, B.; Scaife, C.; Narang, A.K.; Fountzilas, C.; Wolpin, B.M.; Al-Hawary, M.; Asbun, H.; et al. Guidelines Insights: Pancreatic Adenocarcinoma, Version 1.2019. J. Natl. Compr. Cancer Netw. 2019, 17, 202–210. [Google Scholar] [CrossRef]
- Gunturu, K.S.; Yao, X.; Cong, X.; Thumar, J.R.; Hochster, H.S.; Stein, S.M.; Lacy, J. FOLFIRINOX for Locally Advanced and Metastatic Pancreatic Cancer: Single Institution Retrospective Review of Efficacy and Toxicity. Med. Oncol. 2013, 30, 361. [Google Scholar] [CrossRef]
- Hosein, P.J.; Macintyre, J.; Kawamura, C.; Maldonado, J.C.; Ernani, V.; Loaiza-Bonilla, A.; Narayanan, G.; Ribeiro, A.; Portelance, L.; Merchan, J.R.; et al. A Retrospective Study of Neoadjuvant FOLFIRINOX in Unresectable or Borderline-Resectable Locally Advanced Pancreatic Adenocarcinoma. BMC Cancer 2012, 12, 199. [Google Scholar] [CrossRef]
- Ferrone, C.R.; Marchegiani, G.; Hong, T.S.; Ryan, D.P.; Deshpande, V.; McDonnell, E.I.; Sabbatino, F.; Santos, D.D.; Allen, J.N.; Blaszkowsky, L.S.; et al. Radiological and Surgical Implications of Neoadjuvant Treatment with FOLFIRINOX for Locally Advanced and Borderline Resectable Pancreatic Cancer. Ann. Surg. 2015, 261, 12–17. [Google Scholar] [CrossRef]
- Petrelli, F.; Coinu, A.; Borgonovo, K.; Cabiddu, M.; Ghilardi, M.; Lonati, V.; Aitini, E.; Barni, S. FOLFIRINOX-Based Neoadjuvant Therapy in Borderline Resectable or Unresectable Pancreatic Cancer: A Meta-Analytical Review of Published Studies. Pancreas 2015, 44, 515–521. [Google Scholar] [CrossRef]
- Nitsche, U.; Wenzel, P.; Siveke, J.T.; Braren, R.; Holzapfel, K.; Schlitter, A.M.; Stöß, C.; Kong, B.; Esposito, I.; Erkan, M.; et al. Resectability after First-Line FOLFIRINOX in Initially Unresectable Locally Advanced Pancreatic Cancer: A Single-Center Experience. Ann. Surg. Oncol. 2015, 22, 1212–1220. [Google Scholar] [CrossRef]
- Suker, M.; Beumer, B.R.; Sadot, E.; Marthey, L.; Faris, J.E.; Mellon, E.A.; El-Rayes, B.F.; Wang-Gillam, A.; Lacy, J.; Hosein, P.J.; et al. FOLFIRINOX for Locally Advanced Pancreatic Cancer: A Systematic Review and Patient-Level Meta-Analysis. Lancet Oncol. 2016, 17, 801–810. [Google Scholar] [CrossRef]
- Sadot, E.; Doussot, A.; O’Reilly, E.M.; Lowery, M.A.; Goodman, K.A.; Do, R.K.G.; Tang, L.H.; Gönen, M.; D’Angelica, M.I.; DeMatteo, R.P.; et al. FOLFIRINOX Induction Therapy for Stage 3 Pancreatic Adenocarcinoma. Ann. Surg. Oncol. 2015, 22, 3512–3521. [Google Scholar] [CrossRef]
- Faris, J.E.; Blaszkowsky, L.S.; McDermott, S.; Guimaraes, A.R.; Szymonifka, J.; Huynh, M.A.; Ferrone, C.R.; Wargo, J.A.; Allen, J.N.; Dias, L.E.; et al. FOLFIRINOX in Locally Advanced Pancreatic Cancer: The Massachusetts General Hospital Cancer Center Experience. Oncologist 2013, 18, 543–548. [Google Scholar] [CrossRef] [Green Version]
- Kourie, H.; Auclin, E.; Cunha, A.S.; Gaujoux, S.; Bruzzi, M.; Sauvanet, A.; Lourenco, N.; Trouilloud, I.; Louafi, S.; El-Hajjar, A.; et al. Characteristic and Outcomes of Patients with Pathologic Complete Response after Preoperative Treatment in Borderline and Locally Advanced Pancreatic Adenocarcinoma: An AGEO Multicentric Retrospective Cohort. Clin. Res. Hepatol. Gastroenterol. 2019. [Google Scholar] [CrossRef]
- Yoo, C.; Shin, S.H.; Kim, K.P.; Jeong, J.H.; Chang, H.M.; Kang, J.H.; Lee, S.S.; Park, D.H.; Song, T.J.; Seo, D.W.; et al. Clinical Outcomes of Conversion Surgery after Neoadjuvant Chemotherapy in Patients with Borderline Resectable and Locally Advanced Unresectable Pancreatic Cancer: A Single-Center, Retrospective Analysis. Cancers 2019, 11, 278. [Google Scholar] [CrossRef]
- Li, X.; Guo, C.; Li, Q.; Wei, S.; Zhang, Q.; Chen, Y.; Shen, Y.; Ma, T.; Li, G.; Gao, S.; et al. Association of Modified-FOLFIRINOX-Regimen-Based Neoadjuvant Therapy with Outcomes of Locally Advanced Pancreatic Cancer in Chinese Population. Oncologist 2019, 24. [Google Scholar] [CrossRef]
- Matsumoto, I.; Kamei, K.; Omae, K.; Suzuki, S.; Matsuoka, H.; Mizuno, N.; Ozaka, M.; Ueno, H.; Kobayashi, S.; Uesugi, K.; et al. FOLFIRINOX for Locally Advanced Pancreatic Cancer: Results and Prognostic Factors of Subset Analysis from a Nation-Wide Multicenter Observational Study in Japan. Pancreatology 2019, 19, 296–301. [Google Scholar] [CrossRef]
- Pouypoudat, C.; Buscail, E.; Cossin, S.; Cassinotto, C.; Terrebonne, E.; Blanc, J.-F.; Smith, D.; Marty, M.; Dupin, C.; Laurent, C.; et al. FOLFIRINOX-Based Neoadjuvant Chemoradiotherapy for Borderline and Locally Advanced Pancreatic Cancer: A Pilot Study from a Tertiary Centre. Dig. Liver Dis. 2019, 51, 1043–1049. [Google Scholar] [CrossRef]
- Marchegiani, G.; Todaro, V.; Boninsegna, E.; Negrelli, R.; Sureka, B.; Bonamini, D.; Salvia, R.; Manfredi, R.; Pozzi Mucelli, R.; Bassi, C. Surgery after FOLFIRINOX Treatment for Locally Advanced and Borderline Resectable Pancreatic Cancer: Increase in Tumour Attenuation on CT Correlates with R0 Resection. Eur. Radiol. 2018, 28, 4265–4273. [Google Scholar] [CrossRef]
- Wagner, M.; Antunes, C.; Pietrasz, D.; Cassinotto, C.; Zappa, M.; Sa Cunha, A.; Lucidarme, O.; Bachet, J.B. CT Evaluation after Neoadjuvant FOLFIRINOX Chemotherapy for Borderline and Locally Advanced Pancreatic Adenocarcinoma. Eur. Radiol. 2017, 27, 3104–3116. [Google Scholar] [CrossRef]
- Barenboim, A.; Lahat, G.; Geva, R.; Nachmany, I.; Nakache, R.; Goykhman, Y.; Brazowski, E.; Rosen, G.; Isakov, O.; Wolf, I.; et al. Neoadjuvant FOLFIRINOX for Locally Advanced and Borderline Resectable Pancreatic Cancer: An Intention to Treat Analysis. Eur. J. Surg. Oncol. 2018, 44, 1619–1623. [Google Scholar] [CrossRef]
- Suker, M.; Nuyttens, J.J.; Groot Koerkamp, B.; Eskens, F.A.L.M.; van Eijck, C.H.J. FOLFIRINOX and Radiotherapy for Locally Advanced Pancreatic Cancer: A Cohort Study. J. Surg. Oncol. 2018, 118, 1021–1026. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.C.; Gromski, M.A.; Kim, H.W.; Kim, J.; Kim, J.; Hwang, J.H. Clinical Outcomes of FOLFIRINOX in Locally Advanced Pancreatic Cancer: A Single Center Experience. Medicine 2018, 97, e13592. [Google Scholar] [CrossRef]
- Blazer, M.; Wu, C.; Goldberg, R.M.; Phillips, G.; Schmidt, C.; Muscarella, P.; Wuthrick, E.; Williams, T.M.; Reardon, J.; Christopher Ellison, E.; et al. Neoadjuvant Modified (m) FOLFIRINOX for Locally Advanced Unresectable (LAPC) and Borderline Resectable (BRPC) Adenocarcinoma of the Pancreas. Ann. Surg. Oncol. 2015, 22, 1153–1159. [Google Scholar] [CrossRef]
- Hackert, T.; Sachsenmaier, M.; Hinz, U.; Schneider, L.; Michalski, C.W.; Springfeld, C.; Strobel, O.; Jäger, D.; Ulrich, A.; Büchler, M.W. Locally Advanced Pancreatic Cancer: Neoadjuvant Therapy with Folfirinox Results in Resectability in 60% of the Patients. Ann. Surg. 2016, 264, 457–463. [Google Scholar] [CrossRef]
- Vogel, J.A.; Rombouts, S.J.; de Rooij, T.; van Delden, O.M.; Dijkgraaf, M.G.; van Gulik, T.M.; van Hooft, J.E.; van Laarhoven, H.W.; Martin, R.C.; Schoorlemmer, A.; et al. Induction Chemotherapy Followed by Resection or Irreversible Electroporation in Locally Advanced Pancreatic Cancer (IMPALA): A Prospective Cohort Study. Ann. Surg. Oncol. 2017, 24, 2734–2743. [Google Scholar] [CrossRef]
- Nanda, R.H.; El-Rayes, B.; Maithel, S.K.; Landry, J. Neoadjuvant Modified FOLFIRINOX and Chemoradiation Therapy for Locally Advanced Pancreatic Cancer Improves Resectability. J. Surg. Oncol. 2015, 111, 1028–1034. [Google Scholar] [CrossRef]
- Stein, S.M.; James, E.S.; Deng, Y.; Cong, X.; Kortmansky, J.S.; Li, J.; Staugaard, C.; Indukala, D.; Boustani, A.M.; Patel, V.; et al. Final Analysis of a Phase II Study of Modified FOLFIRINOX in Locally Advanced and Metastatic Pancreatic Cancer. Br. J. Cancer 2016, 114, 737–743. [Google Scholar] [CrossRef]
- Lakatos, G.; Petranyi, A.; Szűcs, A.; Nehéz, L.; Harsanyi, L.; Hegyi, P.; Bodoky, G. Efficacy and Safety of FOLFIRINOX in Locally Advanced Pancreatic Cancer. A Single Center Experience. Pathol. Oncol. Res. 2017, 23, 753–759. [Google Scholar] [CrossRef]
- Khushman, M.; Dempsey, N.; Cudris Maldonado, J.; Loaiza-Bonilla, A.; Velez, M.; Carcas, L.; Dammrich, D.; Hurtado-Cordovi, J.; Parajuli, R.; Pollack, T.; et al. Full Dose Neoadjuvant FOLFIRINOX Is Associated with Prolonged Survival in Patients with Locally Advanced Pancreatic Adenocarcinoma. Pancreatology 2015, 15, 667–673. [Google Scholar] [CrossRef]
- Rangelova, E.; Wefer, A.; Persson, S.; Valente, R.; Tanaka, K.; Orsini, N.; Segersvärd, R.; Arnelo, U.; Del Chiaro, M. Surgery Improves Survival after Neoadjuvant Therapy for Borderline and Locally Advanced Pancreatic Cancer. Ann. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Cavanna, L.; Stroppa, E.M.; Citterio, C.; Mordenti, P.; Di Nunzio, C.; Peveri, S.; Orlandi, E.; Vecchia, S. Modified FOLFIRINOX for Unresectable Locally Advanced/Metastatic Pancreatic Cancer. A Real-World Comparison of an Attenuated with a Full Dose in a Single Center Experience. Onco Targets Ther. 2019, 12, 3077–3085. [Google Scholar] [CrossRef] [PubMed]
- Montes, A.; Villarroel, P.; Ayerbes, M.; Gómez, J.C.; Aldana, G.; Tuñas, L.; Fernández, M.; Fernández, M. Prognostic and Predictive Markers of Response to Treatment in Patients with Locally Advanced Unresectable and Metastatic Pancreatic Adenocarcinoma Treated with Gemcitabine/Nab-Paclitaxel: Results of a Retrospective Analysis. J. Cancer Res. Ther. 2017, 13, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Peterson, S.; Loaiza-Bonilla, A.; Ben-Josef, E.; Drebin, J.A.; Westendorf-Overley, C.; Anthony, L.B.; DeSimone, P.A.; Goel, G.; Kudrimoti, M.R.; Dineen, S.P.; et al. Neoadjuvant Nab -Paclitaxel and Gemcitabine (AG) in Borderline Resectable (BR) or Unresectable (UR) Locally Advanced Pancreatic Adenocarcinoma (LAPC) in Patients Ineligible for FOLFIRINOX. J. Clin. Oncol. 2017. [Google Scholar] [CrossRef]
- Yamada, S.; Fujii, T.; Yokoyama, Y.; Kawashima, H.; Maeda, O.; Suzuki, K.; Okada, T.; Ono, E.; Yamaguchi, J.; Takano, N.; et al. Phase I Study of Chemoradiotherapy Using Gemcitabine plus Nab-Paclitaxel for Unresectable Locally Advanced Pancreatic Cancer. Cancer Chemother. Pharmacol. 2018, 81, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Shabason, J.E.; Chen, J.; Apisarnthanarax, S.; Damjanov, N.; Giantonio, B.; Loaiza-Bonilla, A.; O’Dwyer, P.J.; O’Hara, M.; Reiss, K.A.; Teitelbaum, U.; et al. A Phase I Dose Escalation Trial of Nab-Paclitaxel and Fixed Dose Radiation in Patients with Unresectable or Borderline Resectable Pancreatic Cancer. Cancer Chemother. Pharmacol. 2018, 81, 609–614. [Google Scholar] [CrossRef]
- Saito, T.; Ishido, K.; Kudo, D.; Kimura, N.; Wakiya, T.; Nakayama, Y.; Hakamada, K. Combination Therapy with Gemcitabine and Nab-Paclitaxel for Locally Advanced Unresectable Pancreatic Cancer. Mol. Clin. Oncol. 2017, 6, 963–967. [Google Scholar] [CrossRef]
- Hammel, P.; Lacy, J.; Portales, F.; Sobrero, A.F.; Pazo Cid, R.A.; Manzano Mozo, J.L.; Terrebonne, E.; Dowden, S.D.; Shiansong Li, J.; Ong, T.J.; et al. Phase II LAPACT Trial of Nab -Paclitaxel ( Nab -P) plus Gemcitabine (G) for Patients with Locally Advanced Pancreatic Cancer (LAPC). J. Clin. Oncol. 2019, 36, 204. [Google Scholar] [CrossRef]
- Gemenetzis, G.; Groot, V.P.; Blair, A.B.; Laheru, D.A.; Zheng, L.; Narang, A.K.; Fishman, E.K.; Hruban, R.H.; Yu, J.; Burkhart, R.A.; et al. Survival in Locally Advanced Pancreatic Cancer after Neoadjuvant Therapy and Surgical Resection. Ann. Surg. 2019. [Google Scholar] [CrossRef]
- Burris, H.A.; Moore, M.J.; Andersen, J.; Green, M.R.; Rothenberg, M.L.; Modiano, M.R.; Cripps, M.C.; Portenoy, R.K.; Storniolo, A.M.; Tarassoff, P.; et al. Improvements in Survival and Clinical Benefit with Gemcitabine as First- Line Therapy for Patients with Advanced Pancreas Cancer: A Randomized Trial. J. Clin. Oncol. 1997, 15, 2403–2413. [Google Scholar] [CrossRef]
- Gudjonsson, B. Cancer of the Pancreas: 50 Years of Surgery. Cancer 1987, 60, 2284–2303. [Google Scholar] [CrossRef]
- Crist, D.W.; Sitzmann, J.V.; Cameron, J.L. Improved Hospital Morbidity, Mortality, and Survival after the Whipple Procedure. Ann. Surg. 1987, 206, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Del Chiaro, M.; Rangelova, E.; Halimi, A.; Ateeb, Z.; Scandavini, C.; Valente, R.; Segersvärd, R.; Arnelo, U.; Verbeke, C.S. Pancreatectomy with Arterial Resection Is Superior to Palliation in Patients with Borderline Resectable or Locally Advanced Pancreatic Cancer. HPB 2019, 21, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Bilimoria, K.Y.; Talamonti, M.S.; Sener, S.F.; Bilimoria, M.M.; Stewart, A.K.; Winchester, D.P.; Ko, C.Y.; Bentrem, D.J. Effect of Hospital Volume on Margin Status after Pancreaticoduodenectomy for Cancer. J. Am. Coll. Surg. 2008, 207, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Winter, J.M.; Cameron, J.L.; Campbell, K.A.; Arnold, M.A.; Chang, D.C.; Coleman, J.; Hodgin, M.B.; Sauter, P.K.; Hruban, R.H.; Riall, T.S.; et al. 1423 Pancreaticoduodenectomies for Pancreatic Cancer: A Single-Institution Experience. J. Gastrointest. Surg. 2006, 10, 1199–1210. [Google Scholar] [CrossRef] [PubMed]
- Zervos, E.E.; Rosemurgy, A.S.; Al-Saif, O.; Durkin, A.J. Surgical Management of Early-Stage Pancreatic Cancer. Cancer Control. 2004, 11, 23–31. [Google Scholar] [CrossRef]
- Imamura, M.; Doi, R. Treatment of Locally Advanced Pancreatic Cancer: Should We Resect When Resectable? Pancreas 2004, 28, 293–295. [Google Scholar] [CrossRef]
- Dholakia, A.S.; Hacker-Prietz, A.; Wild, A.T.; Raman, S.P.; Wood, L.D.; Huang, P.; Laheru, D.A.; Zheng, L.; De Jesus-Acosta, A.; Le, D.T.; et al. Resection of Borderline Resectable Pancreatic Cancer after Neoadjuvant Chemoradiation Does Not Depend on Improved Radiographic Appearance of Tumor–Vessel Relationships. J. Radiat. Oncol. 2013, 2, 413–425. [Google Scholar] [CrossRef]
- Waddell, N.; Pajic, M.; Patch, A.M.; Chang, D.K.; Kassahn, K.S.; Bailey, P.; Johns, A.L.; Miller, D.; Nones, K.; Quek, K.; et al. Whole Genomes Redefine the Mutational Landscape of Pancreatic Cancer. Nature 2015, 518, 495–501. [Google Scholar] [CrossRef]
- Golan, T.; Kanji, Z.S.; Epelbaum, R.; Devaud, N.; Dagan, E.; Holter, S.; Aderka, D.; Paluch-Shimon, S.; Kaufman, B.; Gershoni-Baruch, R.; et al. Overall Survival and Clinical Characteristics of Pancreatic Cancer in BRCA Mutation Carriers. Br. J. Cancer 2014, 111, 1132–1138. [Google Scholar] [CrossRef]
- Golan, T.; Oh, D.-Y.; Reni, M.; Macarulla, T.M.; Tortora, G.; Hall, M.J.; Reinacher-Schick, A.C.; Borg, C.; Hochhauser, D.; Walter, T.; et al. POLO: A Randomized Phase III Trial of Olaparib Maintenance Monotherapy in Patients (Pts) with Metastatic Pancreatic Cancer (MPC) Who Have a Germline BRCA1/2mutation (gBRCAm). J. Clin. Oncol. 2018, 33. [Google Scholar] [CrossRef]
- Van Der Sijde, F.; Vietsch, E.E.; Mustafa, D.A.M.; Besselink, M.G.; Koerkamp, B.G.; Van Eijck, C.H.J. Circulating Biomarkers for Prediction of Objective Response to Chemotherapy in Pancreatic Cancer Patients. Cancers 2019, 11, 93. [Google Scholar] [CrossRef] [PubMed]
- Azzariti, A.; Brunetti, O.; Porcelli, L.; Graziano, G.; Iacobazzi, R.M.; Signorile, M.; Scarpa, A.; Lorusso, V.; Silvestris, N. Potential Predictive Role of Chemotherapy-Induced Changes of Soluble CD40 Ligand in Untreated Advanced Pancreatic Ductal Adenocarcinoma. Onco. Targets. Ther. 2016, 9, 4681–4686. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.W.; Lim, J.B. Clinical Significance of Elevated Serum Soluble CD40 Ligand Levels as a Diagnostic and Prognostic Tumor Marker for Pancreatic Ductal Adenocarcinoma. J. Transl. Med. 2014, 12, 102. [Google Scholar] [CrossRef] [PubMed]
- Beatty, G.L.; Chiorean, E.G.; Fishman, M.P.; Saboury, B.; Teitelbaum, U.R.; Sun, W.; Huhn, R.D.; Song, W.; Li, D.; Sharp, L.L.; et al. CD40 Agonists Alter Tumor Stroma and Show Efficacy against Pancreatic Carcinoma in Mice and Humans. Science 2011, 331, 1612–1616. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, M.H.; O’Reilly, E.M.; Rosemarie, M.; Varadhachary, G.; Wainberg, Z.A.; Ko, A.; Fisher, G.A., Jr.; Rahma, O.; Lyman, J.P.; Cabanski, C.R.; et al. A phase Ib study of CD40 agonistic monoclonal antibody APX005M together with gemcitabine and nab-paclitaxel with or without nivolumab in untreated metastatic ductal pancreatic adenocarcinoma patients. In Proceedings of the AACR Annual Meeting 2019, Atlanta, GA, USA, 29 March–3 April 2019. [Google Scholar]
- Von Ahrens, D.; Bhagat, T.D.; Nagrath, D.; Maitra, A.; Verma, A. The Role of Stromal Cancer-Associated Fibroblasts in Pancreatic Cancer. J. Hematol. Oncol. 2017, 10, 76. [Google Scholar] [CrossRef] [PubMed]
- Porcelli, L.; Iacobazzi, R.M.; Di Fonte, R.; Serratì, S.; Intini, A.; Solimando, A.G.; Brunetti, O.; Calabrese, A.; Leonetti, F.; Azzariti, A.; et al. CAFs and TGF-β Signaling Activation by Mast Cells Contribute to Resistance to Gemcitabine/Nabpaclitaxel in Pancreatic Cancer. Cancers 2019, 11, 330. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FOLFIRINOX (n = 35) | Gemcitabine NabPaclitaxel (n = 21) | p | |
|---|---|---|---|
| Median Age years (range) | 59.2 (42–70) | 65.4 (44–79) | 0.042 * |
| Male/Female | 17/18 | 13/8 | 0.12 |
| Site (n): | |||
| Head Body/Tail | 20 15 | 16 5 | 0.46 |
| PS ECOG: | |||
| 0 1 | 30 5 | 17 9 | 0.007 * |
| Median CA19.9 UI/mL at diagnosis (range) | 841.95 (1–10694) | 2125.58 (0.8–18801) | 0.20 |
| T classification: | |||
| T4 T3 | 27 8 | 19 2 | 0.96 |
| N classification: | |||
| N0 N+ | 14 21 | 7 14 | 0.34 |
| FOLFIRINOX (n = 18) | Gemcitabine NabPaclitaxel (n = 11) | |
|---|---|---|
| Local Relapse Only | 7 | 5 |
| Distant Relapse: | 11 | 6 |
| Carcinosis | 4 | 1 |
| Lung | 2 | 1 |
| Liver | 1 | 1 |
| ≥2 sites | 4 | 3 |
| Total Number of relapse—n (%) | 29 (51.79%) | |
| FOLFIRINOX n = 35 (%) | Gemcitabine NabPaclitaxel n = 21 (%) | |||
|---|---|---|---|---|
| G1/2 | G3/4 | G1/2 | G3/4 | |
| Anemia | 20 (57.14) | 0 (0) | 17 (80.95) | 1 (4.76) |
| Neutropenia | 11 (31.43) | 10 (28.57) | 6 (28.57) | 1 (4.76) |
| Decreased Platelet Count | 15 (42.86) | 1 (2.86) | 6 (28.57) | 1 (4.76) |
| Increased Transaminases | 13 (37.14) | 1 (2.86) | 13 (61.90) | 1 (4.76) |
| Oral Mucositis | 6 (17.14) | 0 (0) | 2 (9.52) | 0 (0) |
| Diarrhoea | 16 (45.71) | 2 (5.71) | 8 (38.10) | 2 (9.52) |
| Nausea | 19 (54.29) | 1 (2.86) | 10 (47.62) | 0 (0) |
| Vomiting | 9 (25.71) | 0 (0) | 7 (33.33) | 0 (0) |
| Fatigue | 21 (60) | 0 (0) | 17 (80.95) | 0 (0) |
| Parestesia | 24 (68.57) | 0 (0) | 5 (23.81) | 1 (4.76) |
| Total | 91.12% | 8.88% | 92.86% | 7.14% |
| Author | Year | Treatment | N° of Patients Treated | Resection Rate (RR %) | R0 Resection (n/Total Resected Patients) | Reference |
|---|---|---|---|---|---|---|
| Barenboim | 2018 | FFN | 30 | 3 (10%) | N/A | 31 |
| Blazer | 2015 | FFN | 25 | 11 (44%) | 10/11 | 34 |
| Cavanna | 2019 | mFFN | 13 | N/A | N/A | 42 |
| Faris * | 2013 | FFN | 22 | 5 (23%) | 5/5 | 23 |
| Ferrone * | 2015 | FFN | 25 | N/A | NA | 18 |
| Gunturu | 2015 | FFN | 16 | 2 (12.5%) | N/A | 16 |
| Hackert | 2016 | FFN | 125 | 76 (61%) | 31/76 | 35 |
| Hosein | 2012 | FFN | 14 | 6 (43%) | 5/6 | 17 |
| Khushman | 2015 | FFN | 40 | N/A | 6 | 40 |
| Kourie | 2019 | FFN | 14 | 14 (100%) | 14/14 | 24 |
| Lakatos | 2017 | mFFN | 32 | 2 (6.3%) | 2/2 | 39 |
| Lee | 2018 | FFN | 64 | 15 (23.4%) | 11/15 | 33 |
| Li | 2019 | FFN | 41 | 14 (34.15%) | N/A | 26 |
| Mancini | 2018 | FFN | 23 | 1 (4%) | 1/1 | 13 |
| Marchegiani * | 2018 | FFN | 46 | N/A | N/A | 29 |
| Matsumoto | 2019 | FFN | 66 | N/A | N/A | 27 |
| Nanda | 2015 | mFFN | 29 | 12 (41.9%) | 10/12 | 37 |
| Nitsche | 2015 | FFN | 14 | 4 (29%) | 3/4 | 20 |
| Petrelli ° | 2015 | FFN | N/A | (26.1%) | (22.5%) | 19 |
| Pouypoudat | 2019 | FFN | 38 | 13 (34.2%) | 12/13 | 28 |
| Rombouts # | 2016 | FFN | 365 | 103 (28%) | 72/103 | 14 |
| Sadot | 2015 | FFN | 101 | 31 (31%) | 16/31 | 22 |
| Stein | 2016 | FFN | 31 | 13 (41.9%) | 13/13 | 38 |
| Suker ° | 2016 | FFN | 355 | 91 (25.9%) | 60/81 | 21 |
| Wagner * | 2017 | FFN | 13 | 13 (100%) | 11/13 | 30 |
| Yoo | 2019 | FFN | 70 | 66 (94.29%) | N/A | 25 |
| Author | Year | Treatment | N° of Patients Treated | Resection Rate (RR %) | R0 Resection (n/Total Resected Patients) | Reference |
|---|---|---|---|---|---|---|
| Yamada | 2018 | GemNab | 12 | 6 (50%) | N/A | 45 |
| Montes | 2017 | GemNab | 9 | N/A | N/A | 43 |
| Peterson | 2018 | GemNab | 10 | N/A | N/A | 44 |
| Saito | 2017 | GemNab | 7 | 2 (28,6%) | 2/2 | 47 |
| Shabason | 2018 | GemNab | 5 | 2 (40%) | 2/2 | 46 |
| Hammel | 2018 | GemNab | 107 | 16 (15%) | 7/16 | 48 |
| Author | Year | Treatment | N° of Patients Treated | Resection Rate (RR %) | R0 Resection (n/Total Resected Patients) | Reference |
|---|---|---|---|---|---|---|
| Gemenetzis | 2018 | FFN | 187 | 51 (63%) | N/A | 49 |
| GemNab | 16 | N/A | N/A | |||
| Rangelova | 2019 | FFN | 54 | N/A | N/A | 41 |
| GemNab | 21 | N/A | N/A |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Napolitano, F.; Formisano, L.; Giardino, A.; Girelli, R.; Servetto, A.; Santaniello, A.; Foschini, F.; Marciano, R.; Mozzillo, E.; Carratù, A.C.; et al. Neoadjuvant Treatment in Locally Advanced Pancreatic Cancer (LAPC) Patients with FOLFIRINOX or Gemcitabine NabPaclitaxel: A Single-Center Experience and a Literature Review. Cancers 2019, 11, 981. https://doi.org/10.3390/cancers11070981
Napolitano F, Formisano L, Giardino A, Girelli R, Servetto A, Santaniello A, Foschini F, Marciano R, Mozzillo E, Carratù AC, et al. Neoadjuvant Treatment in Locally Advanced Pancreatic Cancer (LAPC) Patients with FOLFIRINOX or Gemcitabine NabPaclitaxel: A Single-Center Experience and a Literature Review. Cancers. 2019; 11(7):981. https://doi.org/10.3390/cancers11070981
Chicago/Turabian StyleNapolitano, Fabiana, Luigi Formisano, Alessandro Giardino, Roberto Girelli, Alberto Servetto, Antonio Santaniello, Francesca Foschini, Roberta Marciano, Eleonora Mozzillo, Anna Chiara Carratù, and et al. 2019. "Neoadjuvant Treatment in Locally Advanced Pancreatic Cancer (LAPC) Patients with FOLFIRINOX or Gemcitabine NabPaclitaxel: A Single-Center Experience and a Literature Review" Cancers 11, no. 7: 981. https://doi.org/10.3390/cancers11070981
APA StyleNapolitano, F., Formisano, L., Giardino, A., Girelli, R., Servetto, A., Santaniello, A., Foschini, F., Marciano, R., Mozzillo, E., Carratù, A. C., Cascetta, P., De Placido, P., De Placido, S., & Bianco, R. (2019). Neoadjuvant Treatment in Locally Advanced Pancreatic Cancer (LAPC) Patients with FOLFIRINOX or Gemcitabine NabPaclitaxel: A Single-Center Experience and a Literature Review. Cancers, 11(7), 981. https://doi.org/10.3390/cancers11070981