Early Tumor Shrinkage and Depth of Response Evaluation in Metastatic Pancreatic Cancer Treated with First Line Chemotherapy: An Observational Retrospective Cohort Study

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Results
2.1. Patients Characteristics and Treatment Efficacy
2.2. ETS and DoR
2.3. Survival Analyses
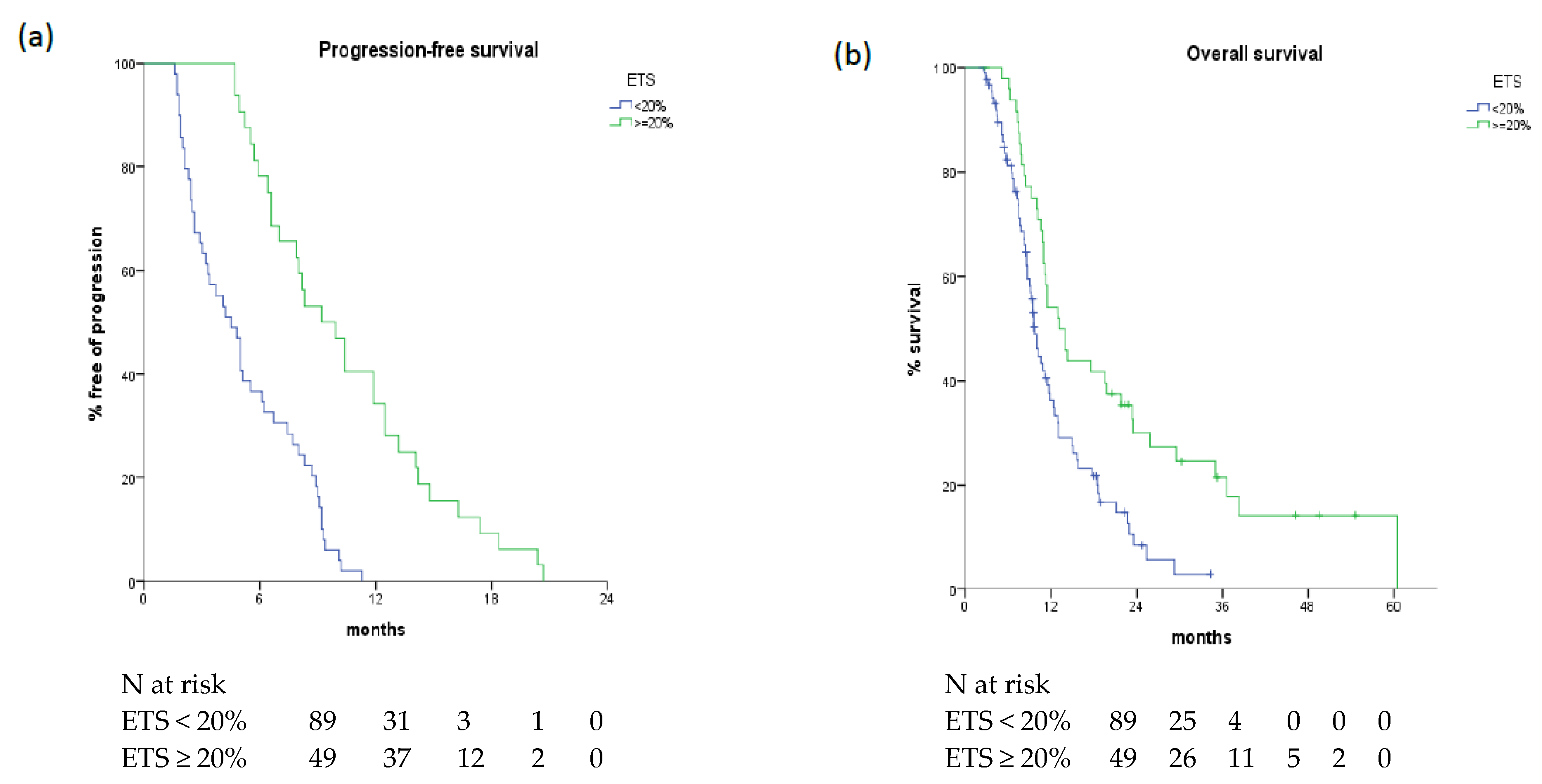
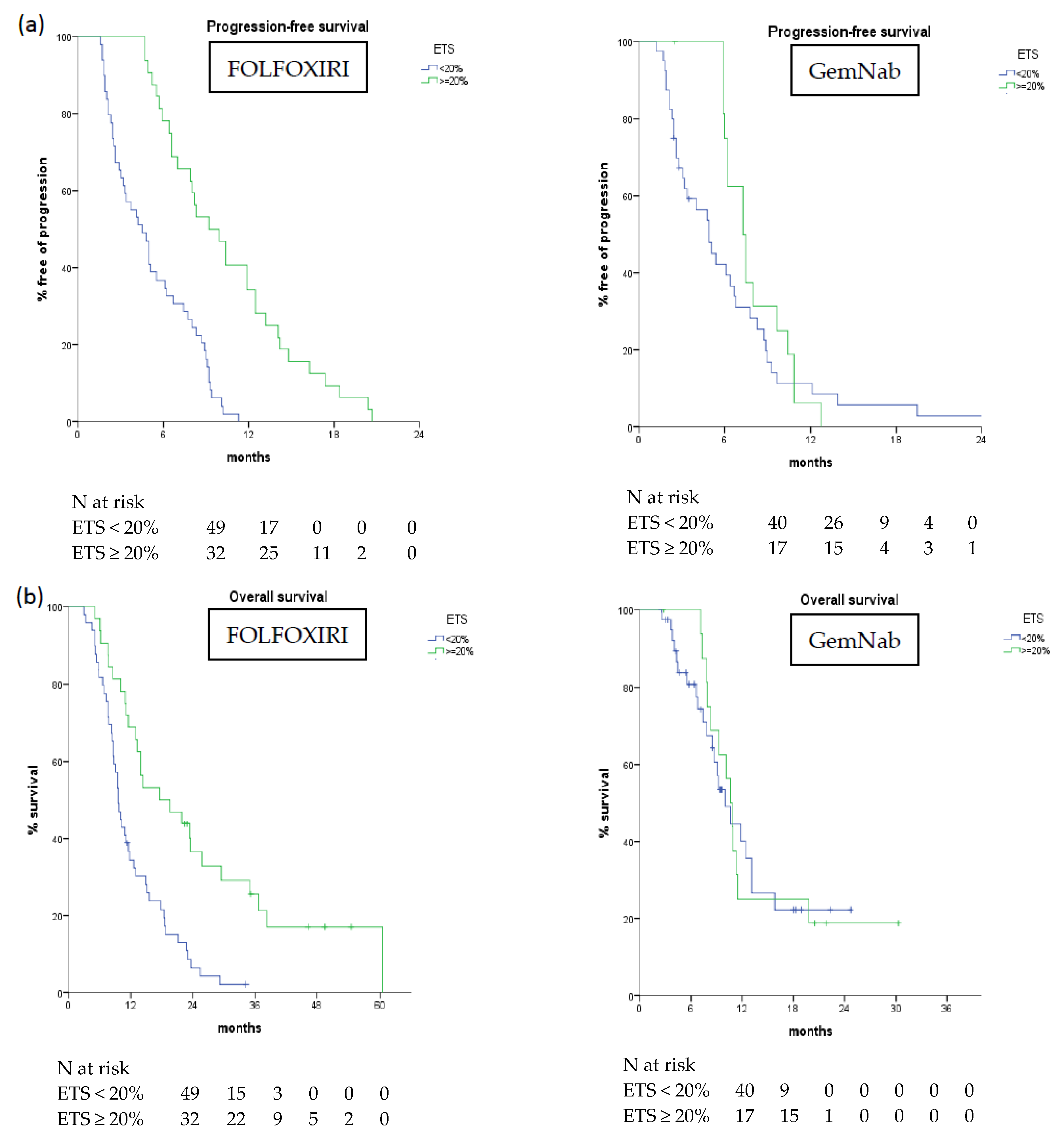
2.3.1. ETS: Correlation with Survival
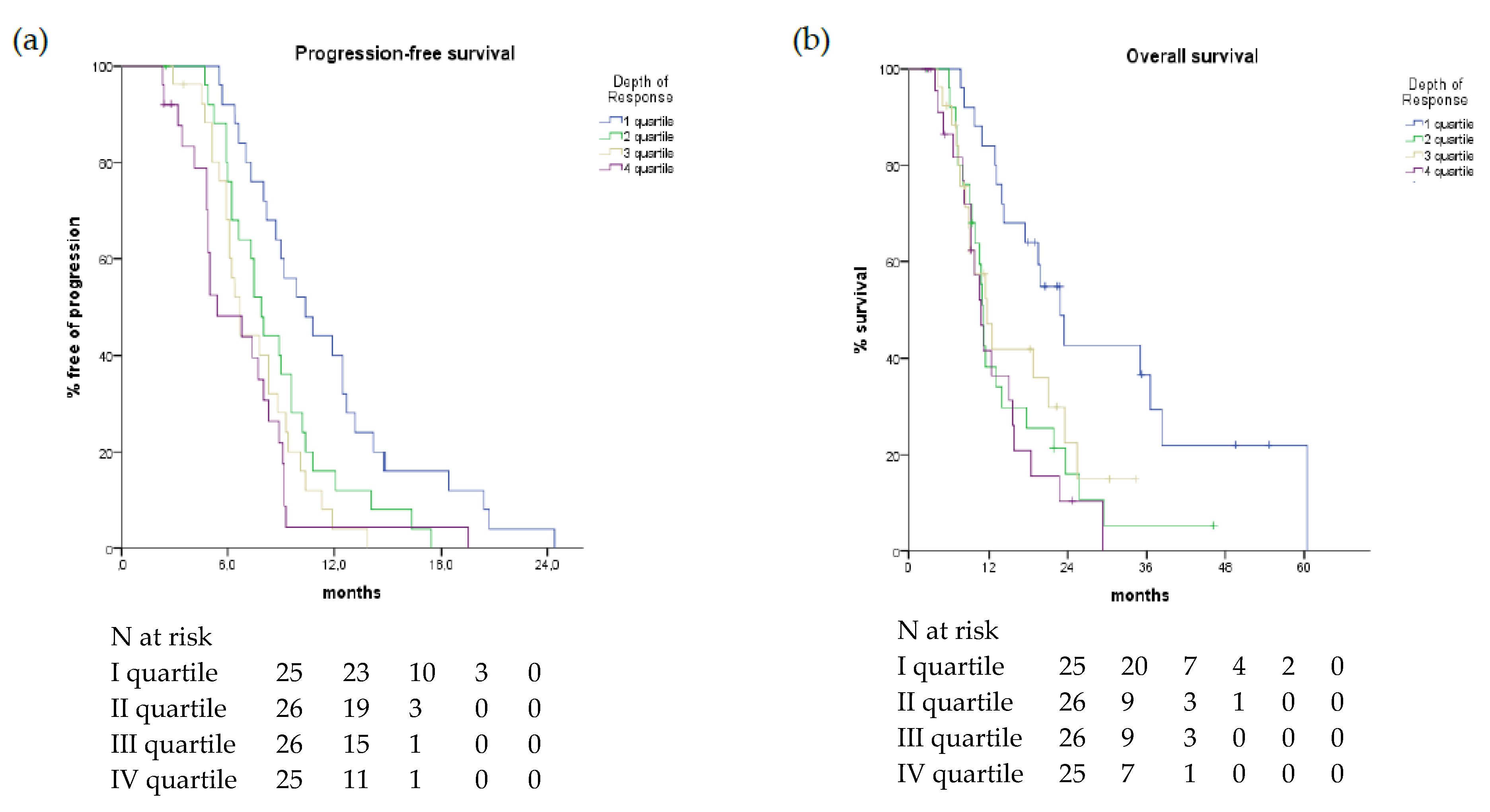
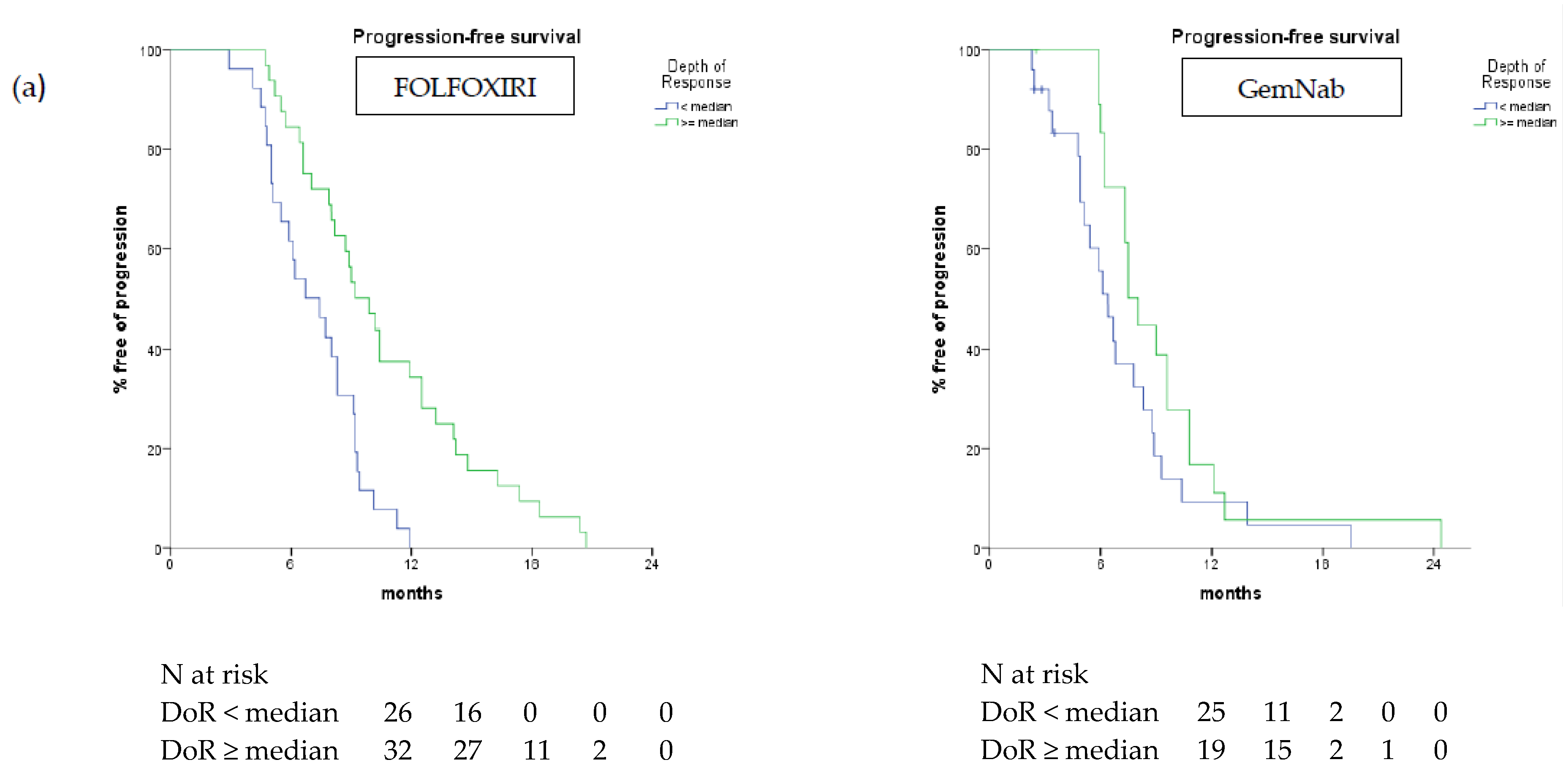
2.3.2. DoR: Correlation with Survival
2.3.3. Multivariate Analysis
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. Review World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef] [PubMed]
- United States National Cancer Institute. Pancreatic Cancer: Statistics 2018. Available online: https://www.cancer.net/cancer-types/pancreatic-cancer/statistics (accessed on 11 May 2019).
- Gnoni, A.; Licchetta, A.; Scarpa, A.; Azzariti, A.; Brunetti, A.E.; Simone, G.; Nardulli, P.; Santini, D.; Aieta, M.; Delcuratolo, S.; et al. Carcinogenesis of pancreatic adenocarcinoma: Precursor lesions. Int. J. Mol. Sci. 2013, 14, 19731–19762. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [PubMed]
- Vivaldi, C.; Caparello, C.; Musettini, G.; Pasquini, G.; Catanese, S.; Fornaro, L.; Lencioni, M.; Falcone, A.; Vasile, E. First-line treatment with FOLFOXIRI for advanced pancreatic cancer in clinical practice: Patients’ outcome and analysis of prognostic factors. Int. J. Cancer 2016, 139, 938–945. [Google Scholar] [CrossRef] [PubMed]
- NCCN Guidelines. Available online: https://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdf (accessed on 11 May 2019).
- Ryan, D.P.; Hong, T.S.; Bardeesy, N. Pancreatic adenocarcinoma. N. Engl. J. Med. 2014, 371, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Cremolini, C.; Loupakis, F.; Antoniotti, C.; Lonardi, S.; Masi, G.; Salvatore, L.; Cortesi, E.; Tomasello, G.; Spadi, R.; Zaniboni, A.; et al. Early tumor shrinkage and depth of response predict long-term outcome in metastatic colorectal cancer patients treated with first-line chemotherapy plus bevacizumab: results from phase III TRIBE trial by the Gruppo Oncologico del Nord Ovest. Ann. Oncol. 2015, 26, 1188–1194. [Google Scholar] [CrossRef] [PubMed]
- Stintzing, S.; Modest, D.P.; Fischer von Weikersthal, L.; Decker, T.; Kiani, A.; Vehling-Kaiser, U.; Al-Batran, S.; Heintges, T.; Lerchenmueller, C.; Kahl, C.; et al. LBA11 Independent Radiological Evaluation of Objective Response Early Tumor Shrinkage, and Depth of Response In FIRE-3 (AIO KRK-0306) in the Final RAS Evaluable Population. Ann. Oncol. 2014, 25 (Suppl. 4). [Google Scholar] [CrossRef]
- Heinemann, V.; Stintzing, S.; Modest, D.P.; Giessen-Jung, C.; Michl, M.; Mansmann, U.R. Early tumour shrinkage (ETS) and depth of response (DpR) in the treatment of patients with metastatic colorectal cancer (mCRC). Eur. J. Cancer 2015, 51, 1927–1936. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, T.; Isayama, H.; Nakai, Y.; Togawa, O.; Kogure, H.; Ito, Y.; Yamamoto, K.; Mizuno, S.; Yagioka, H.; Yashima, Y.; et al. Prognostic factors in patients with advanced biliary tract cancer receiving chemotherapy. Cancer Chemother. Pharmacol. 2011, 67, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Kaga, Y.; Sunakawa, Y.; Kubota, Y.; Tagawa, T.; Yamamoto, T.; Ikusue, T.; Uto, Y.; Miyashita, K.; Toshima, H.; Kobayashi, K.; et al. Early tumor shrinkage as a predictor of favorable outcomes in patients with advanced pancreatic cancer treated with FOLFIRINOX. Oncotarget 2016, 7, 67314–67320. [Google Scholar] [CrossRef] [PubMed]
- Kunzmann, V.; Ramanathan, R.K.; Goldstein, D.; Liu, H.; Ferrara, S.; Lu, B.; Renschler, M.F.; Von Hoff, D.D. Tumor Reduction in Primary and Metastatic Pancreatic Cancer Lesions with nab-Paclitaxel and Gemcitabine: An Exploratory Analysis from a Phase 3 Study. Pancreas 2017, 46, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Hammel, P.; Lacy, J.; Portales, F.; Sobrero, A.F.; Pazo Cid, R.A.; Manzano Mozo, J.L.; Terrebonne, E.; Dowden, S.D.; Li, J.S.; Ong, T.J.; et al. Phase II LAPACT trial of nabpaclitaxel (nab-P) plus gemcitabine (G) for patients with locally advanced pancreatic cancer (LAPC). J. Clin. Oncol. 2018, 36 (Suppl. 4), 204. [Google Scholar] [CrossRef]
- Tabernero, J.; Chiorean, E.G.; Infante, J.R.; Hingorani, S.R.; Ganju, V.; Weekes, C.; Scheithauer, W.; Ramanathan, R.K.; Goldstein, D.; Penenberg, D.N.; et al. Prognostic factors of survival in a randomized phase III trial (MPACT) of weekly nab-paclitaxel plus gemcitabine versus gemcitabine alone in patients with metastatic pancreatic cancer. Oncologist 2016, 20, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Taieb, J.; Rinaldi, Y.; Pointet, A.L.; Barbier, E.; Khemissa, F.; Gratet, A.; Miglianico, L.; Laharie-Mineur, H.; Bouhier-Leporrier, K.; Ghiringhelli, F.; et al. Gemcitabine plus nab-paclitaxel until progression or given sequentially with 5-fluorouracile plus irinotecan (FOLFIRI.3) for first-line treatment of metastatic pancreatic ductal adenocarcinoma (mPDAC): A randomized phase II study (PRODIGE 37-FIRGEMAX). J. Clin. Oncol. 2018, 36 (Suppl. 15), 4107. [Google Scholar] [CrossRef]
- Dahan, L.; Phelip, J.M.; Le Malicot, K.; Williet, N.; Desrame, J.; Volet, J.; Petorin, C.; Malka, D.; Rebischung, C.; Aparicio, T.; et al. FOLFIRINOX until progression, FOLFIRINOX with maintenance treatment, or sequential treatment with gemcitabine and FOLFIRI.3 for first-line treatment of metastatic pancreatic cancer: A randomized phase II trial (PRODIGE 35-PANOPTIMOX). J. Clin. Oncol. 2018, 36 (Suppl. 15), 4000. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients | FOLFOXIRI Cohort | GemNab Cohort | |||
|---|---|---|---|---|---|---|
| n = 138 | % | n = 81 | % | n = 57 | % | |
| Age years, median (range) | 64 (41–76) | - | 62 (41–75) | - | 68 (47–76) | |
| Age (years) | ||||||
| <65 | 80 | 58 | 60 | 74 | 20 | 35 |
| ≥65 | 58 | 42 | 21 | 26 | 37 | 65 |
| Gender | ||||||
| Male | 71 | 51.4 | 40 | 49.4 | 31 | 54.4 |
| Female | 67 | 48.6 | 41 | 50.6 | 26 | 45.6 |
| ECOG Performance Status | ||||||
| 0 | 84 | 68.4 | 62 | 76.5 | 22 | 38.6 |
| 1 | 54 | 39.2 | 19 | 23.5 | 35 | 61.4 |
| Histology: Adenocarcinoma | ||||||
| Ductal | 123 | 89.1 | 74 | 91.4 | 49 | 86 |
| On IPMN | 12 | 8.7 | 6 | 7.4 | 6 | 10.6 |
| Acinar | 2 | 1.4 | 1 | 1.2 | 1 | 1.7 |
| Squamous | 1 | 0.7 | - | - | 1 | 1.7 |
| Site of primitive tumor | ||||||
| Head/uncinate process | 65 | 47.1 | 39 | 48.1 | 26 | 45.6 |
| Body/tail | 73 | 52.9 | 42 | 51.9 | 31 | 54.4 |
| Number of metastatic sites | ||||||
| Median (range) | 2 (1–5) | - | 2 (1–5) | 2 (1–4) | ||
| Synchronous disease | ||||||
| Yes | 101 | 73.2 | 58 | 71.6 | 43 | 75.4 |
| No | 37 | 26.8 | 23 | 28.4 | 14 | 24.6 |
| Metastatic sites | ||||||
| Liver | 108 | 78.3 | 65 | 80.2 | 43 | 75.4 |
| Peritoneum | 41 | 29.7 | 27 | 33.3 | 14 | 24.6 |
| Lung | 32 | 23.2 | 14 | 17.3 | 18 | 31.6 |
| Bones | 4 | 2.9 | 2 | 2.5 | 2 | 3.5 |
| Local recurrence | 7 | 5.1 | 3 | 3.7 | 4 | 7 |
| Lymph nodes | 20 | 14.4 | 4 | 4.8 | 16 | 28 |
| Previous treatments | ||||||
| Curative-intent surgery | 37 | 26.9 | 24 | 29.6 | 13 | 22.8 |
| Adjuvant chemotherapy | 25 | 18.1 | 18 | 22.2 | 7 | 12.3 |
| Ca 19.9 [KU/L] | ||||||
| Normal value | 27 | 19.5 | 15 | 18.5 | 13 | 22.8 |
| <59 ULN | 60 | 43.4 | 39 | 48.1 | 22 | 38.6 |
| ≥59 ULN | 42 | 30.4 | 20 | 24.7 | 20 | 35.1 |
| Not evaluable | 9 | 6.5 | 7 | 8.6 | 2 | 3.5 |
| ETS and DoR Cut-Offs | All Patients n (%) | FOLFOXIRI n (%) | GemNab n (%) | p-Value |
|---|---|---|---|---|
| ETS | ||||
| ≥20% | 49 (35.5) | 32 (39.5) | 17 (29.8) | 0.28 |
| <20% | 89 (64.5) | 49 (60.5) | 40 (70.2) | |
| DoR | ||||
| I quartile (−81.81%–−44.87%) | 25 | 20 (34.5) | 5 (11.3) | 0.039 |
| II quartile (−44.87%–−27.52%) | 26 | 12 (20.7) | 14 (31.8) | |
| III quartile (−27.52%–−7.34%) | 26 | 15 (25.8) | 11 (25) | |
| IV quartile (−7.33%–+48%) | 25 | 11 (18.9) | 14 (31.8) | |
| ≥median | 51 | 32 (55.2) | 19 (43.2) | 0.23 |
| <median | 51 | 26 (44.8) | 25 (56.8) |
| Clinical and Pathological Features | PFS | OS | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| ECOG performance status | ||||
| 0 vs. 1 | 1.655 (1.160–2.361) | 0.005 | 2.216 (1.479–3.320) | <0.001 |
| Gender | ||||
| male vs. female | 1.020 (0.725–1.435) | 0.907 | 1.124 (0.769–1.643) | 0.547 |
| Sites of metastases, yes vs. no | ||||
| Liver | 0.774 (0.513–1.166) | 0.22 | 0.606 (0.375–0.980) | 0.041 |
| Lung | 1.221 (0.899–1.994) | 0.165 | 1.416 (0.868–2.311) | 0.164 |
| Peritoneum | 0.974 (0.670–1.417) | 0.891 | 0.942 (0.622–1.425) | 0.776 |
| Number of metastatic sites | ||||
| 1–2 vs. 3–5 | 0.905 (0.622–1.316) | 0.6 | 1.324 (0.811–1.882) | 0.324 |
| Primary site | ||||
| head-uncinate process vs. body-tail | 0.718 (0.509–1.013) | 0.059 | 0.844 (0.577–1.235) | 0.382 |
| Previous surgery on primary tumour | ||||
| yes vs. no | 1.026 (0.694–1.516) | 0.897 | 1.422 (0.912–2.218) | 0.12 |
| Ca19.9 level | ||||
| <ULN vs. ≥ULN | 0.803 (0.523–1.235) | 0.318 | 1.332 (0.798–2.224) | 0.273 |
| ETS | ||||
| ≥20% vs. <20% | 0.444 (0.308–0.640) | <0.001 | 0.493 (0.324–0.750) | 0.001 |
| As a continuous variable | 1.029 (1.023–1.035) | <0.001 | 1.012 (1.008–1.016) | <0.001 |
| DoR | ||||
| <median value vs. ≥median value | 0.461 (0.304–0.669) | <0.001 | 0.601 (0.376–0.960) | 0.033 |
| As a continuous variable | 1.025 (1.016–1.034) | <0.001 | 1.019 (1.008–1.029) | <0.001 |
| PFS and OS in Treatment Groups | ETS | DoR | ||||
|---|---|---|---|---|---|---|
| ≥20% | <20% | p-Value | ≥Median | <Median | p-Value | |
| median PFS (months) | ||||||
| FOLFOXIRI | 9.2 | 4.5 | <0.001 | 9.2 | 6.7 | <0.001 |
| GemNab | 7.3 | 4.9 | 0.209 | 7.5 | 6.4 | 0.093 |
| median OS (months) | ||||||
| FOLFOXIRI | 17.5 | 9.6 | <0.001 | 19.5 | 11.5 | 0.005 |
| GemNab | 10.6 | 10 | 0.853 | 10.9 | 10.6 | 0.818 |
| Variables | PFS | OS | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| ECOG performance status | ||||
| 1 vs. 0 | 1.902 (1.235–2.929) | 0.004 | 3.074 (1.843–5.125) | <0.0001 |
| Presence of liver metastases | - | - | ||
| no vs. yes | 0.428 (0.244–0.750) | 0.003 | ||
| ETS | ||||
| <20% vs. ≥20% | 1.890 (1.054–3.389) | 0.033 | 2.349 (1.126–4.897) | 0.023 |
| DoR | ||||
| continuous variable | 1.035 (1.022–1.049) | <0.0001 | 1.038 (1.022–1.055) | <0.0001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vivaldi, C.; Fornaro, L.; Cappelli, C.; Pecora, I.; Catanese, S.; Salani, F.; Cacciato Insilla, A.; Kauffmann, E.; Donati, F.; Pasquini, G.; et al. Early Tumor Shrinkage and Depth of Response Evaluation in Metastatic Pancreatic Cancer Treated with First Line Chemotherapy: An Observational Retrospective Cohort Study. Cancers 2019, 11, 939. https://doi.org/10.3390/cancers11070939
Vivaldi C, Fornaro L, Cappelli C, Pecora I, Catanese S, Salani F, Cacciato Insilla A, Kauffmann E, Donati F, Pasquini G, et al. Early Tumor Shrinkage and Depth of Response Evaluation in Metastatic Pancreatic Cancer Treated with First Line Chemotherapy: An Observational Retrospective Cohort Study. Cancers. 2019; 11(7):939. https://doi.org/10.3390/cancers11070939
Chicago/Turabian StyleVivaldi, Caterina, Lorenzo Fornaro, Carla Cappelli, Irene Pecora, Silvia Catanese, Francesca Salani, Andrea Cacciato Insilla, Emanuele Kauffmann, Francescamaria Donati, Giulia Pasquini, and et al. 2019. "Early Tumor Shrinkage and Depth of Response Evaluation in Metastatic Pancreatic Cancer Treated with First Line Chemotherapy: An Observational Retrospective Cohort Study" Cancers 11, no. 7: 939. https://doi.org/10.3390/cancers11070939
APA StyleVivaldi, C., Fornaro, L., Cappelli, C., Pecora, I., Catanese, S., Salani, F., Cacciato Insilla, A., Kauffmann, E., Donati, F., Pasquini, G., Massa, V., Napoli, N., Lencioni, M., Boraschi, P., Campani, D., Boggi, U., Caramella, D., Falcone, A., & Vasile, E. (2019). Early Tumor Shrinkage and Depth of Response Evaluation in Metastatic Pancreatic Cancer Treated with First Line Chemotherapy: An Observational Retrospective Cohort Study. Cancers, 11(7), 939. https://doi.org/10.3390/cancers11070939