Association of miR-34a Expression with Quality of Life of Glioblastoma Patients: A Prospective Study


 , ,
, , 
Abstract
1. Introduction
2. Results
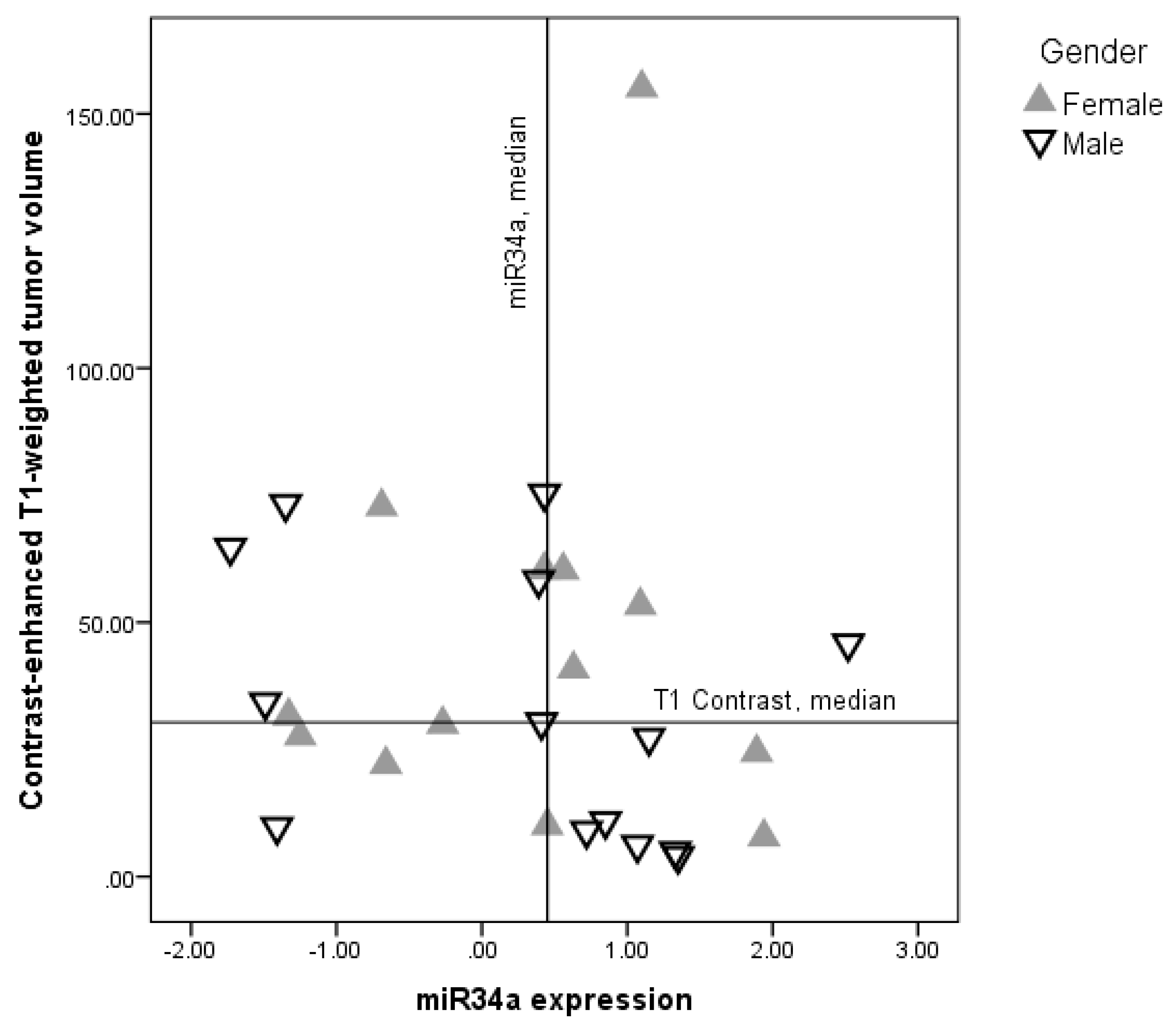
2.1. Demographic and Clinical Characteristics Relationship with miR-34a Expression Levels
2.2. Health Related Quality of Life and miR-34a Expression
2.3. Depression Correlation with miR-34a Expression
2.4. Functional Status
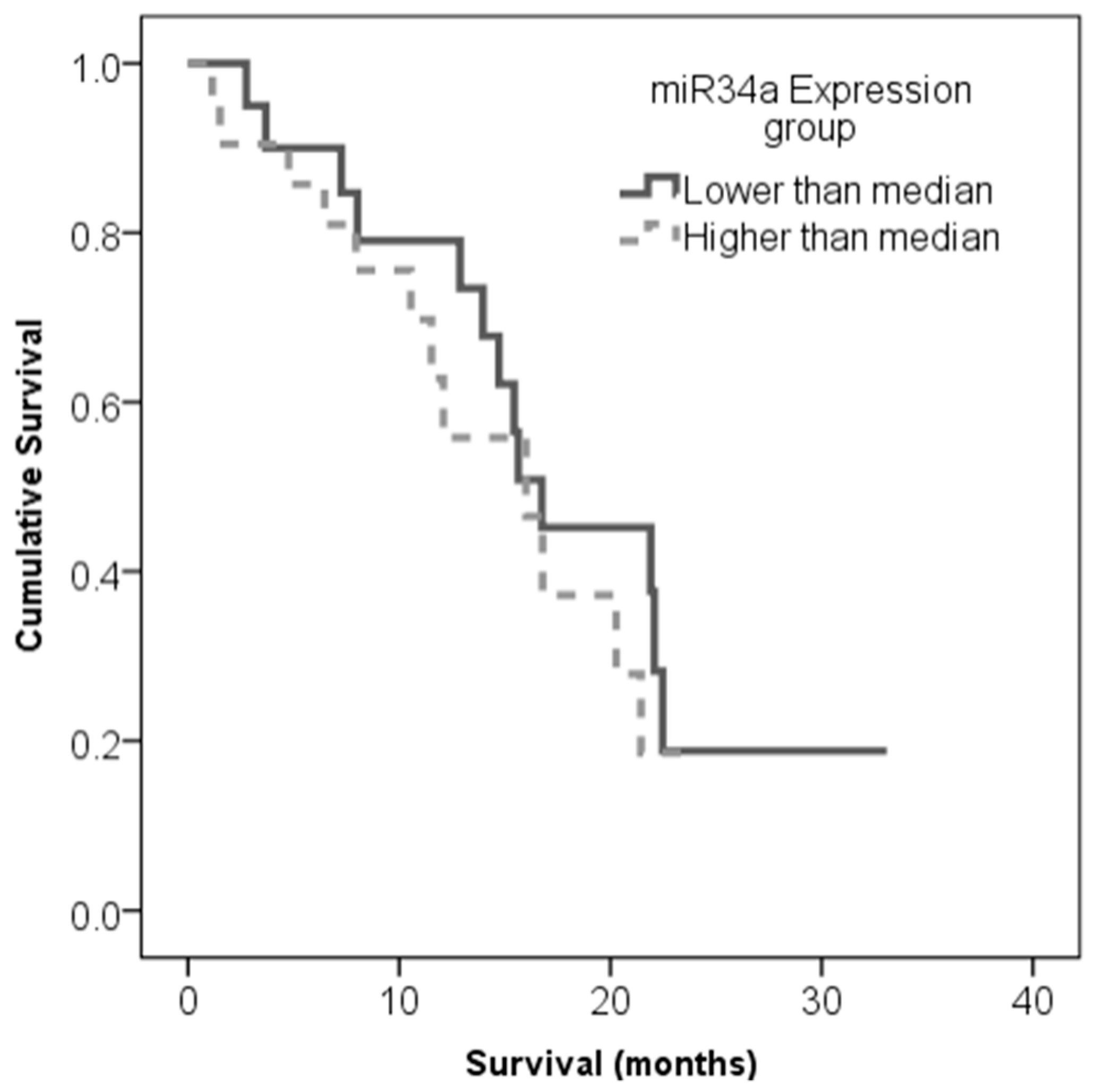
2.5. Correlation of miR-34a Expression and Patient Survival
3. Discussion
4. Materials and Methods
4.1. Procedures
4.2. Samples
4.3. Questionnaires
4.4. Tumour Volume Measurements
4.5. Small RNA Extraction, Micro RNA cDNA Synthesis and qPCR Performance
- 1)
- 2)
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Crocetti, E.; Trama, A.; Stiller, C.; Caldarella, A.; Soffietti, R.; Jaal, J.; Weber, D.C.; Ricardi, U.; Slowinski, J.; Brandes, A.; et al. Epidemiology of glial and non-glial brain tumours in Europe. Eur. J. Cancer 2012, 48, 1532–1542. [Google Scholar] [CrossRef] [PubMed]
- Porter, K.R.; McCarthy, B.J.; Freels, S.; Kim, Y.; Davis, F.G. Prevalence estimates for primary brain tumors in the United States by age, gender, behavior, and histology. Neuro. Oncol. 2010, 12, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Gately, L.; McLachlan, S.; Dowling, A.; Philip, J. Life beyond a diagnosis of glioblastoma: A systematic review of the literature. J. Cancer Surviv. 2017, 11, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Dirven, L.; Aaronson, N.K.; Heimans, J.J.; Taphoorn, M.J.B. Health-related quality of life in high-grade glioma patients. Chin. J. Cancer 2014, 33, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.-L.; Hou, P.-P.; Li, Y.-L.; Wang, D.-T.; Yuan, T.-W.; Wei, J.-L.; Zhao, B.-T.; Lou, J.-T.; Zhao, X.-T.; Jin, Y.; et al. MicroRNA-34a inhibits the proliferation and promotes the apoptosis of non-small cell lung cancer H1299 cell line by targeting TGFβR2. Tumor Biol. 2015, 36, 2481–2490. [Google Scholar] [CrossRef] [PubMed]
- Toraih, E.A.; Alghamdi, S.A.; El-Wazir, A.; Hosny, M.M.; Hussein, M.H.; Khashana, M.S.; Fawzy, M.S. Dual biomarkers long non-coding RNA GAS5 and microRNA-34a co-expression signature in common solid tumors. PLoS ONE 2018, 13, e0198231. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Brannon, A.R.; Reddy, A.R.; Alexe, G.; Seiler, M.W.; Arreola, A.; Oza, J.H.; Yao, M.; Juan, D.; Liou, L.S.; et al. Identifying mRNA targets of microRNA dysregulated in cancer: With application to clear cell Renal Cell Carcinoma. BMC Syst. Biol. 2010, 4, 51. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Qin, H.; Cui, Y. MiR-34a targets GAS1 to promote cell proliferation and inhibit apoptosis in papillary thyroid carcinoma via PI3K/Akt/Bad pathway. Biochem. Biophys. Res. Commun. 2013, 441, 958–963. [Google Scholar] [CrossRef] [PubMed]
- Marsh, E.E.; Lin, Z.; Yin, P.; Milad, M.; Chakravarti, D.; Bulun, S.E. Differential expression of microRNA species in human uterine leiomyoma versus normal myometrium. Fertil. Steril. 2008, 89, 1771–1776. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Zhang, Q.; Ma, X.; Wang, J.; Liang, T. miRNA and mRNA expression analysis reveals potential sex-biased miRNA expression. Sci. Rep. 2017, 7, 39812. [Google Scholar] [CrossRef] [PubMed]
- Bernardo, B.C.; Ooi, J.Y.Y.; Matsumoto, A.; Tham, Y.K.; Singla, S.; Kiriazis, H.; Patterson, N.L.; Sadoshima, J.; Obad, S.; Lin, R.C.Y.; et al. Sex differences in response to miRNA-34a therapy in mouse models of cardiac disease: Identification of sex-, disease- and treatment-regulated miRNAs. J. Physiol. 2016, 594, 5959–5974. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Jin, Z.; Chen, Y.; Xu, H.; Ma, C.; Hong, X.; Li, Y.; Zhao, G. Knockdown of long non-coding RNA ANRIL inhibits proliferation, migration, and invasion but promotes apoptosis of human glioma cells by upregulation of miR-34a. J. Cell. Biochem. 2018, 119, 2708–2718. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Zhao, H.; Xiang, W. Expression level of human miR-34a correlates with glioma grade and prognosis. J. Neurooncol. 2013, 113, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Guessous, F.; Zhang, Y.; DiPierro, C.; Kefas, B.; Johnson, E.; Marcinkiewicz, L.; Jiang, J.; Yang, Y.; Schmittgen, T.D.; et al. MicroRNA-34a Inhibits Glioblastoma Growth by Targeting Multiple Oncogenes. Cancer Res. 2009, 69, 7569–7576. [Google Scholar] [CrossRef] [PubMed]
- Genovese, G.; Ergun, A.; Shukla, S.A.; Campos, B.; Hanna, J.; Ghosh, P.; Quayle, S.N.; Rai, K.; Colla, S.; Ying, H.; et al. microRNA regulatory network inference identifies miR-34a as a novel regulator of TGF-β signaling in glioblastoma. Cancer Discov. 2012, 2, 736–749. [Google Scholar] [CrossRef] [PubMed]
- Li, X.J.; Ren, Z.J.; Tang, J.H. MicroRNA-34a: A potential therapeutic target in human cancer. Cell Death Dis. 2014, 5, e1327. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Lam, M.; Iorns, E.; Gunn, W.; Tan, F.; Lomax, J.; Errington, T. Registered report: The microRNA miR-34a inhibits prostate cancer stem cells and metastasis by directly repressing CD44. Elife 2015, 4, e06434. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Wu, Y.; Wang, Z.; Liu, X.; Wang, S.; Qin, C. MicroRNA-34a expression is predictive of recurrence after radiofrequency ablation in early hepatocellular carcinoma. Tumor Biol. 2015, 36, 3887–3893. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, J.P.; Dolecek, T.A.; Horbinski, C.; Ostrom, Q.T.; Lightner, D.D.; Barnholtz-Sloan, J.S.; Villano, J.L. Epidemiologic and molecular prognostic review of glioblastoma. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 1985–1996. [Google Scholar] [CrossRef] [PubMed]
- Brodbelt, A.; Greenberg, D.; Winters, T.; Williams, M.; Vernon, S.; Collins, V.P.; (UK) National Cancer Information Network Brain Tumour Group. Glioblastoma in England: 2007–2011. Eur. J. Cancer 2015, 51, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Chen, Z.; Liang, H.; Li, Z.; Zou, X.; Luo, H.; Guo, W.; Xu, L. Thyroid hormone inhibits TGFβ1 induced renal tubular epithelial to mesenchymal transition by increasing miR34a expression. Cell. Signal. 2013, 25, 1949–1954. [Google Scholar] [CrossRef] [PubMed]
- Bunevicius, A.; Laws, E.R.; Deltuva, V.; Tamasauskas, A. Association of thyroid hormone concentrations with quality of life of primary brain tumor patients: A pilot study. J. Neurooncol. 2017, 131, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Bunevicius, A.; Deltuva, V.P.; Tamasauskas, S.; Smith, T.; Laws, E.R.; Bunevicius, R.; Iervasi, G.; Tamasauskas, A. Preoperative low tri-iodothyronine concentration is associated with worse health status and shorter five year survival of primary brain tumor patients. Oncotarget 2017, 8, 8648–8656. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.; Guo, J.; Li, D.; Jia, C.; Yin, W.; Sun, R.; Lv, Z.; Cong, X. MicroRNA-34a suppresses cell proliferation by targeting LMTK3 in human breast cancer mcf-7 cell line. DNA Cell Biol. 2013, 32, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Mainio, A.; Tuunanen, S.; Hakko, H.; Niemelä, A.; Koivukangas, J.; Räsänen, P. Decreased quality of life and depression as predictors for shorter survival among patients with low-grade gliomas: A follow-up from 1990 to 2003. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Mugge, L.; Mansour, T.R.; Crippen, M.; Alam, Y.; Schroeder, J. Depression and glioblastoma, complicated concomitant diseases: A systemic review of published literature. Neurosurg. Rev. 2018, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, J.A.; Carter, B.S.; Meng, F.; Turner, D.L.; Dai, M.; Schatzberg, A.F.; Barchas, J.D.; Jones, E.G.; Bunney, W.E.; Myers, R.M.; et al. The microRNA network is altered in anterior cingulate cortex of patients with unipolar and bipolar depression. J. Psychiatr. Res. 2016, 82, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Andolina, D.; Di Segni, M.; Ventura, R. MiRNA-34 and stress response. Oncotarget 2017, 8, 5658–5659. [Google Scholar] [CrossRef] [PubMed]
- Andolina, D.; Di Segni, M.; Bisicchia, E.; D’Alessandro, F.; Cestari, V.; Ventura, A.; Concepcion, C.; Puglisi-Allegra, S.; Ventura, R. Effects of lack of microRNA-34 on the neural circuitry underlying the stress response and anxiety. Neuropharmacology 2016, 107, 305–316. [Google Scholar] [CrossRef] [PubMed]
- Fayers, P.; Aaronson, N.; Bjordal, K.; Groenvold, M.; Curran, D.; Bottomley, A. EORTC QLQ-C30 Scoring Manual, 3rd ed.; EORTC Data Center: Brussels, Belgium, 2001; Volume 30. [Google Scholar]
- Taphoorn, M.J.B.; Claassens, L.; Aaronson, N.K.; Coens, C.; Mauer, M.; Osoba, D.; Stupp, R.; Mirimanoff, R.O.; van den Bent, M.J.; Bottomley, A.; et al. An international validation study of the EORTC brain cancer module (EORTC QLQ-BN20) for assessing health-related quality of life and symptoms in brain cancer patients. Eur. J. Cancer 2010, 46, 1033–1040. [Google Scholar] [CrossRef] [PubMed]
- Osoba, D.; Aaronson, N.K.; Muller, M.; Sneeuw, K.; Hsu, M.; Yung, W.K.A.; Brada, M.; Newlands, E. The development and psychometric validation of a brain cancer quality-of-life questionnaire for use in combination with general cancer-specific questionnaires. Qual. Life Res. 1996, 5, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Bunevičius, A.; Tamašauskas, Š.; Tamašauskas, A.; Deltuva, V. Evaluation of health-related quality of life in Lithuanian brain tumor patients using the EORTC brain cancer module. Medicina (Kaunas) 2012, 48, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Pranckeviciene, A.; Bunevicius, A. Depression screening in patients with brain tumors: A review. CNS Oncol. 2015, 4, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Rooney, A.G.; McNamara, S.; Mackinnon, M.; Fraser, M.; Rampling, R.; Carson, A.; Grant, R. Screening for major depressive disorder in adults with cerebral glioma: An initial validation of 3 self-report instruments. Neuro. Oncol. 2013, 15, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Karnofsky, D.A.; Abelmann, W.H.; Craver, L.F.; Burchenal, J.H. The use of the nitrogen mustards in the palliative treatment of carcinoma.With particular reference to bronchogenic carcinoma. Cancer 1948, 1, 634–656. [Google Scholar] [CrossRef]
- Jennett, B.; Bond, M. Assessment of outcome after severe brain damage. Lancet (London, England) 1975, 1, 480–484. [Google Scholar] [CrossRef]
- Egger, J.; Kapur, T.; Fedorov, A.; Pieper, S.; Miller, J.V.; Veeraraghavan, H.; Freisleben, B.; Golby, A.J.; Nimsky, C.; Kikinis, R. GBM Volumetry using the 3D Slicer Medical Image Computing Platform. Sci. Rep. 2013, 3, 1364. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Total Sample | Lower than Median miR34 Expression | Equal or Higher than Median miR34 Expression |
|---|---|---|---|
| N (%) | |||
| Gender Females Males | 23 (56.1%) 18 (43.9%) | 13 (56.5%) 7 (38.9%) | 10 (43.5%) 11 (61.1%) |
| Marital status Living alone With partner | 6 (14.6%) 35 (85.4%) | 3 (50.0%) 17 (48.6%) | 3 (50.0%) 18 (51.4%) |
| Education Lower than university University degree | 18 (43.9%) 23 (56.1%) | 8 (44.4%) 12 (52.2%) | 10 (55.6%) 11 (47.8%) |
| Tumor location Frontal Temporal Parietal Occipital Two or three lobes | 14 (34.1%) 8 (19.5%) 6 (14.6%) - 13 (31.7%) | 10 (71.4%) 3 (37.5%) 3 (50.0%) - 4 (30.8%) | 4 (28.6%) 5 (62.5%) 3 (50.0%) - 9 (69.2%) |
| Tumor side Right Left Bilateral | 19 (46.3%) 19 (46.3%) 3 (7.3%) | 10 (52.6%) 9 (47.4%) 1 (33.3%) | 9 (47.4%) 10 (52.6%) 2 (66.7%) |
| Lesion Solitary Multifocal | 34 (82.9%) 7 (17.1%) | 19 (55.9%) 1 (14.3%) | 15 (44.1%) 6 (85.7%) |
| Median | |||
| Volume T1 Contrast enhanced T2 FLAIR weighted | 31.0 116.7 | 58.3 144.3 | 24.4* 114.2 |
| Scales and Domains | miR-34 Expression | |||||
|---|---|---|---|---|---|---|
| Total Sample | Females | Males | ||||
| rho | Sig. | rho | Sig. | rho | Sig. | |
| Health-related Quality of life | ||||||
| EORTC QLQ-C30 A | ||||||
| Global evaluation of health | −0.05 | 0.76 | −0.11 | 0.62 | 0.05 | 0.86 |
| Physical functioning | 0.30 | 0.06 | 0.18 | 0.40 | 0.66 | 0.01 |
| Role functioning | 0.05 | 0.78 | −0.13 | 0.56 | 0.27 | 0.32 |
| Emotional functioning | 0.14 | 0.39 | 0.15 | 0.49 | 0.27 | 0.32 |
| Cognitive functioning | 0.11 | 0.52 | −0.09 | 0.68 | 0.44 | 0.09 |
| Social functioning | 0.26 | 0.12 | 0.09 | 0.67 | 0.44 | 0.09 |
| QLQ C30 Total Score | 0.31 | 0.06 | 0.26 | 0.25 | 0.24 | 0.36 |
| EORTC QLQ-BN20 B | ||||||
| Future uncertainty | −0.11 | 0.50 | −0.14 | 0.52 | −0.07 | 0.81 |
| Visual difficulties | 0.06 | 0.74 | 0.25 | 0.25 | −0.22 | 0.43 |
| Communication | 0.15 | 0.38 | 0.18 | 0.42 | −0.14 | 0.62 |
| Motor difficulties | 0.13 | 0.42 | 0.23 | 0.30 | −0.17 | 0.52 |
| Headaches | −0.08 | 0.64 | 0.07 | 0.70 | −0.19 | 0.49 |
| Seizures | 0.15 | 0.36 | −0.16 | 0.46 | 0.42 | 0.12 |
| Drowsiness | −0.34 | 0.03 | −0.20 | 0.37 | −0.49 | 0.05 |
| Hair loss | −0.01 | 0.97 | 0.33 | 0.13 | −0.42 | 0.11 |
| Itchy skin | −0.06 | 0.71 | 0.13 | 0.54 | −0.27 | 0.32 |
| Leg weakness | −0.26 | 0.11 | −0.17 | 0.45 | −0.42 | −0.11 |
| Bladder control | 0.19 | 0.24 | 0.37 | 0.08 | −0.01 | 0.98 |
| Depression | ||||||
| PHQ-9 C | −0.36 | 0.03 | −0.36 | 0.09 | −0.37 | 0.16 |
| Level of functioning | ||||||
| KPS at time of admission D | 0.36 | 0.03 | 0.19 | 0.41 | 0.34 | 0.22 |
| GOS at time of discharge E | 0.17 | 0.30 | 0.11 | 0.62 | 0.09 | 0.74 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaitkiene, P.; Pranckeviciene, A.; Stakaitis, R.; Steponaitis, G.; Tamasauskas, A.; Bunevicius, A. Association of miR-34a Expression with Quality of Life of Glioblastoma Patients: A Prospective Study. Cancers 2019, 11, 300. https://doi.org/10.3390/cancers11030300
Vaitkiene P, Pranckeviciene A, Stakaitis R, Steponaitis G, Tamasauskas A, Bunevicius A. Association of miR-34a Expression with Quality of Life of Glioblastoma Patients: A Prospective Study. Cancers. 2019; 11(3):300. https://doi.org/10.3390/cancers11030300
Chicago/Turabian StyleVaitkiene, Paulina, Aiste Pranckeviciene, Rytis Stakaitis, Giedrius Steponaitis, Arimantas Tamasauskas, and Adomas Bunevicius. 2019. "Association of miR-34a Expression with Quality of Life of Glioblastoma Patients: A Prospective Study" Cancers 11, no. 3: 300. https://doi.org/10.3390/cancers11030300
APA StyleVaitkiene, P., Pranckeviciene, A., Stakaitis, R., Steponaitis, G., Tamasauskas, A., & Bunevicius, A. (2019). Association of miR-34a Expression with Quality of Life of Glioblastoma Patients: A Prospective Study. Cancers, 11(3), 300. https://doi.org/10.3390/cancers11030300