Indoleamine 2,3-dioxygenase 1 and Programmed Cell Death-ligand 1 Co-expression Predicts Poor Pathologic Response and Recurrence in Esophageal Squamous Cell Carcinoma after Neoadjuvant Chemoradiotherapy

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Quantitative Reverse Transcription Polymerase Chain Reaction
2.3. Correlation of Indoleamine 2,3-Dioxygenase 1 and Programmed Cell Death-Ligand 1 Expression with Clinicopathologic Characteristics
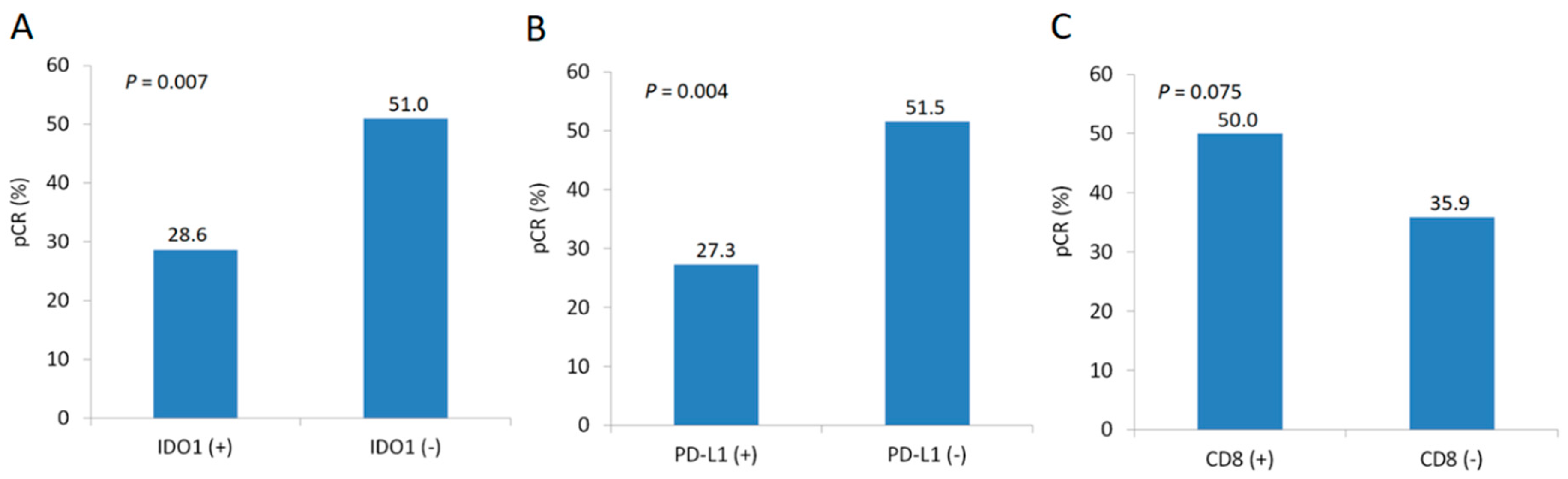
2.4. Factors Associated with Pathologic Complete Response
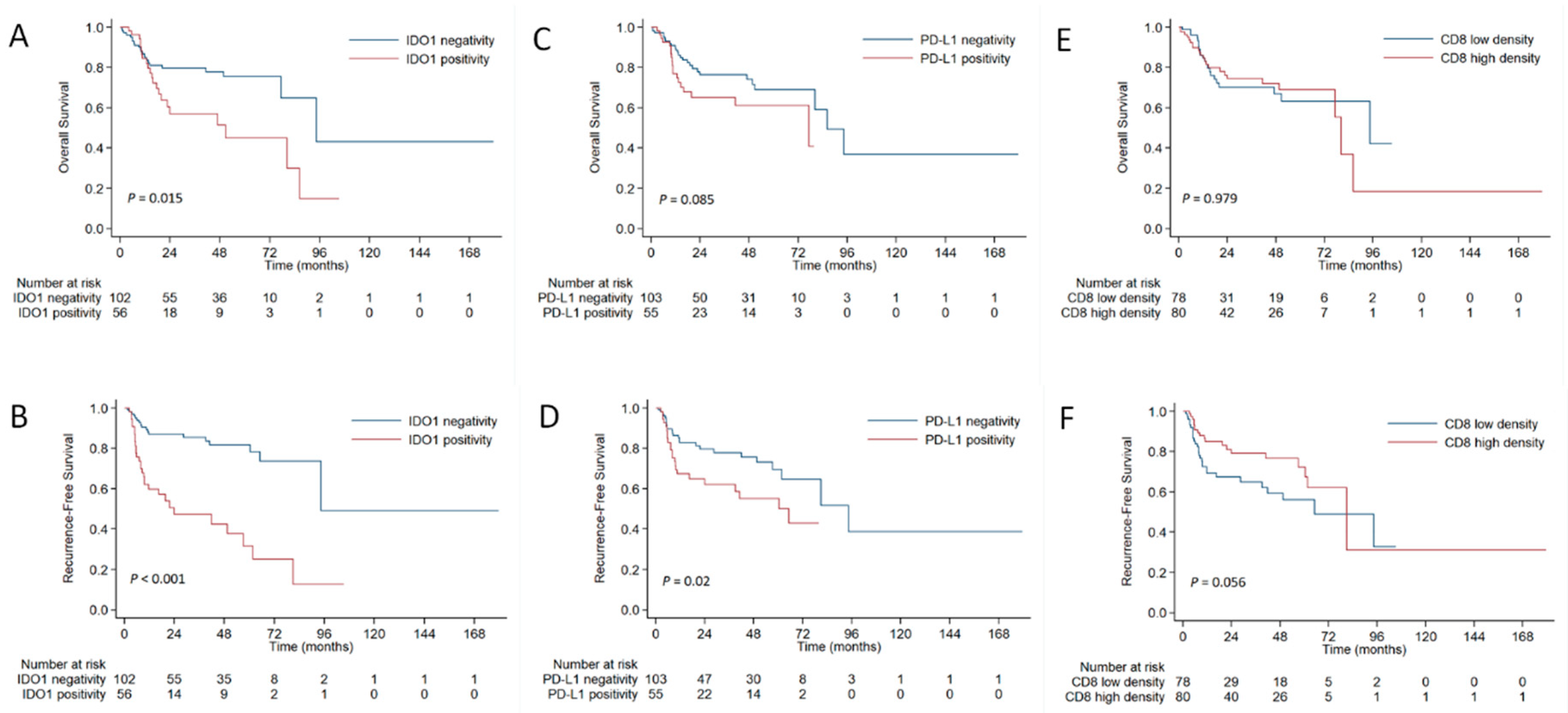
2.5. Survival Analysis
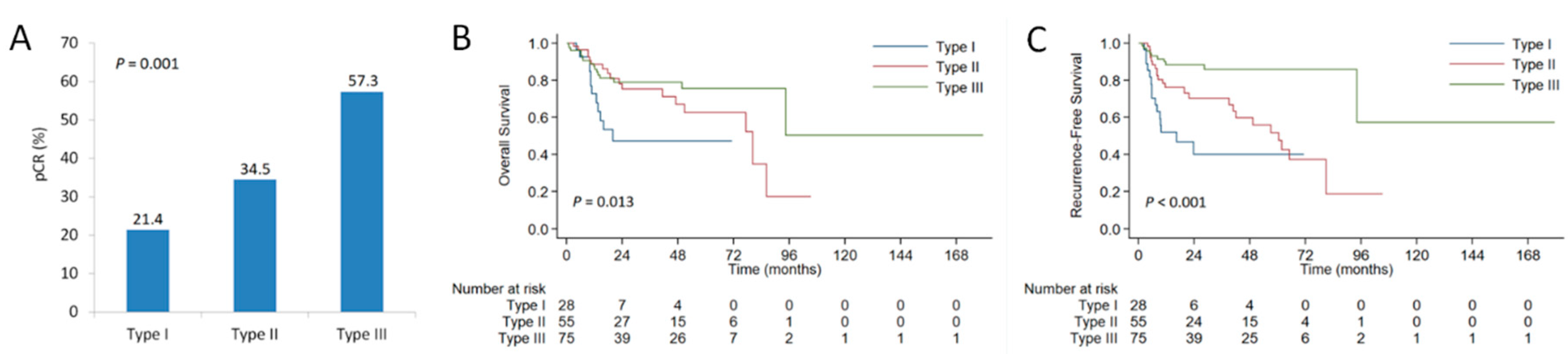
2.6. Stratification Analysis
3. Discussion
4. Patients and Methods
4.1. Patients
4.2. Quantitative Reverse Transcription Polymerase Chain Reaction
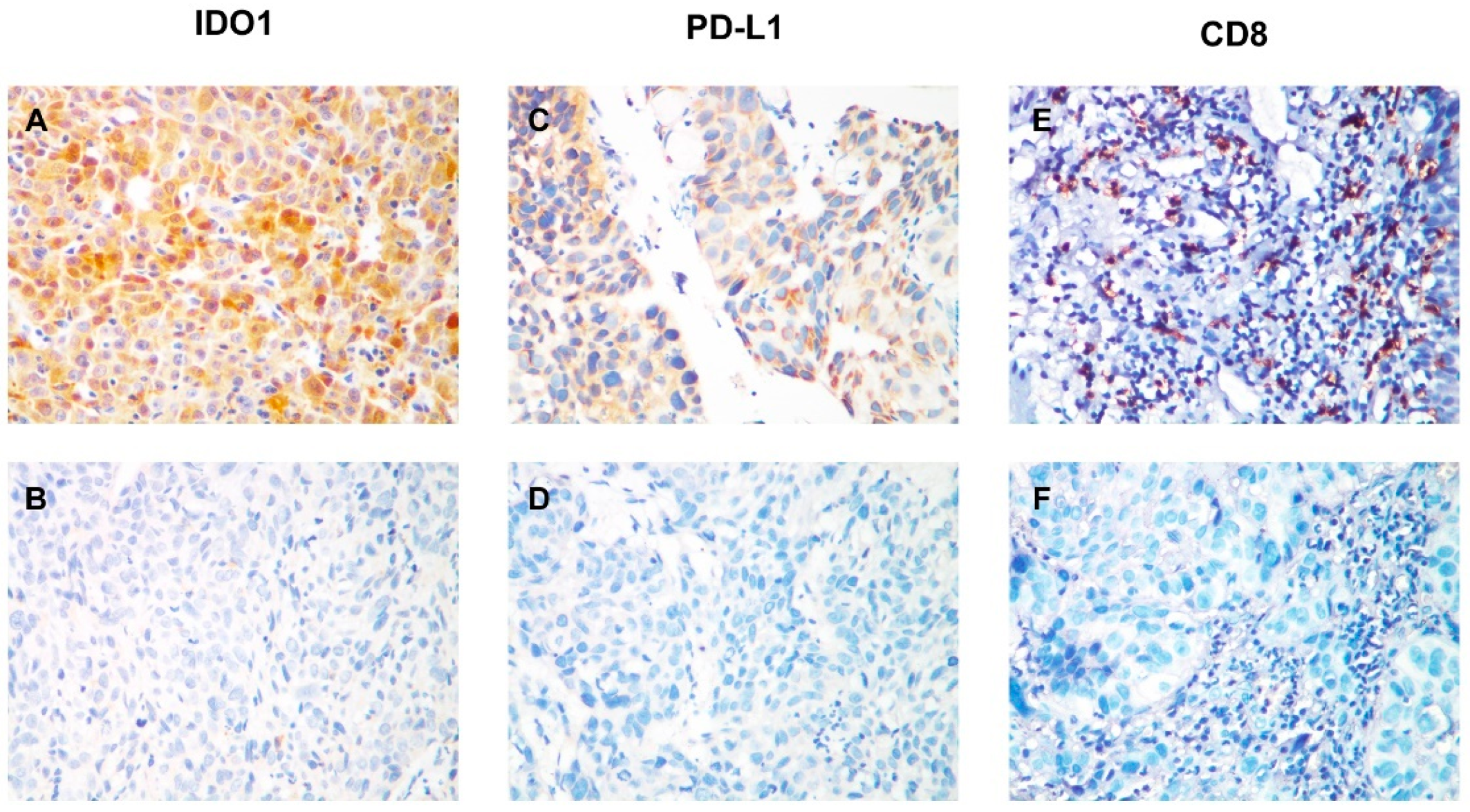
4.3. Immunohistochemistry
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Sjoquist, K.M.; Burmeister, B.H.; Smithers, B.M.; Zalcberg, J.R.; Simes, R.J.; Barbour, A.; Gebski, V. Australasian Gastro-Intestinal Trials Group. Survival after neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal carcinoma: An updated meta-analysis. Lancet Oncol. 2011, 12, 681–692. [Google Scholar] [CrossRef]
- Van Hagen, P.; Hulshof, M.C.; van Lanschot, J.J.; Steyerberg, E.W.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.; Richel, D.J.; Nieuwenhuijzen, G.A.; Hospers, G.A.; Bonenkamp, J.J.; et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N. Engl. J. Med. 2012, 366, 2074–2084. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Liu, H.; Chen, Y.; Zhu, C.; Fang, W.; Yu, Z.; Mao, W.; Xiang, J.; Han, Y.; Chen, Z.; et al. Neoadjuvant chemoradiotherapy followed by surgery versus surgery alone for locally advanced squamous cell carcinoma of the esophagus (NEOCRTEC5010): A phase III multicenter, randomized, open-label clinical trial. J. Clin. Oncol. 2018, 36, 2796–2803. [Google Scholar] [CrossRef] [PubMed]
- Scheer, R.V.; Fakiris, A.J.; Johnstone, P.A. Quantifying the benefit of a pathologic complete response after neoadjuvant chemoradiotherapy in the treatment of esophageal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 996–1001. [Google Scholar] [CrossRef] [PubMed]
- Xi, M.; Yang, Y.; Zhang, L.; Yang, H.; Merrell, K.W.; Hallemeier, C.L.; Shen, R.K.; Haddock, M.G.; Hofstetter, W.L.; Maru, D.M.; et al. Multi-institutional analysis of recurrence and survival after neoadjuvant chemoradiotherapy of esophageal cancer: Impact of histology on recurrence patterns and outcomes. Ann. Surg. 2018, in press. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Shalabi, A.; Hubbard-Lucey, V.M. Comprehensive analysis of the clinical immuno-oncology landscape. Ann. Oncol. 2018, 29, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Tumeh, P.C.; Harview, C.L.; Yearley, J.H.; Shintaku, I.P.; Taylor, E.J.; Robert, L.; Chmielowski, B.; Spasic, M.; Henry, G.; Ciobanu, V.; et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014, 515, 568–571. [Google Scholar] [CrossRef]
- Kang, Y.K.; Boku, N.; Satoh, T.; Ryu, M.H.; Chao, Y.; Kato, K.; Chung, H.C.; Chen, J.S.; Muro, K.; Kang, W.K.; et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 390, 2461–2471. [Google Scholar] [CrossRef]
- Kudo, T.; Hamamoto, Y.; Kato, K.; Ura, T.; Kojima, T.; Tsushima, T.; Hironaka, S.; Hara, H.; Satoh, T.; Iwasa, S.; et al. Nivolumab treatment for oesophageal squamous-cell carcinoma: An open-label, multicentre, phase 2 trial. Lancet Oncol. 2017, 18, 631–639. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Bendell, J.; Calvo, E.; Kim, J.W.; Ascierto, P.A.; Sharma, P.; Ott, P.A.; Peltola, K.; Jaeger, D.; Evans, J.; et al. CheckMate-032 study: Efficacy and safety of nivolumab and nivolumab plus ipilimumab in patients with metastatic esophagogastric cancer. J. Clin. Oncol. 2018, 36, 2836–2844. [Google Scholar] [CrossRef] [PubMed]
- Doi, T.; Piha-Paul, S.A.; Jalal, S.I.; Saraf, S.; Lunceford, J.; Koshiji, M.; Bennouna, J. Safety and antitumor activity of the anti-programmed death-1 antibody pembrolizumab in patients with advanced esophageal carcinoma. J. Clin. Oncol. 2018, 36, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Komiya, T.; Huang, C.H. Updates in the Clinical Development of Epacadostat and Other Indoleamine 2,3-Dioxygenase 1 Inhibitors (IDO1) for Human Cancers. Front. Oncol. 2018, 8, 423. [Google Scholar] [CrossRef] [PubMed]
- Zhai, L.; Spranger, S.; Binder, D.C.; Gritsina, G.; Lauing, K.L.; Giles, F.J.; Wainwright, D.A. Molecular pathways: Targeting IDO1 and other tryptophan dioxygenases for cancer immunotherapy. Clin. Cancer Res. 2015, 21, 5427–5433. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, A.; Cerbelli, B.; Lionetto, L.; Zizzari, I.; Salati, M.; Pisano, A.; Federica, M.; Simmaco, M.; Nuti, M.; Marchetti, P. Can IDO activity predict primary resistance to anti-PD-1 treatment in NSCLC? J. Transl. Med. 2018, 16, 219. [Google Scholar] [CrossRef] [PubMed]
- Beatty, G.L.; O’Dwyer, P.J.; Clark, J.; Shi, J.G.; Bowman, K.J.; Scherle, P.A.; Newton, R.C.; Schaub, R.; Maleski, J.; Leopold, L.; et al. First-in-Human Phase I study of the oral inhibitor of indoleamine 2,3-dioxygenase-1 epacadostat (INCB024360) in patients with advanced solid malignancies. Clin. Cancer Res. 2017, 23, 3269–3276. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, T.C.; Hamid, O.; Smith, D.C.; Bauer, T.M.; Wasser, J.S.; Olszanski, A.J.; Luke, J.J.; Balmanoukian, A.S.; Schmidt, E.V.; Zhao, Y.; et al. Epacadostat plus pembrolizumab in patients with advanced solid tumors: Phase I results from a multicenter, open-label phase I/II trial (ECHO-202/KEYNOTE-037). J. Clin. Oncol. 2018, 36, 3223. [Google Scholar] [CrossRef]
- Yagi, T.; Baba, Y.; Ishimoto, T.; Iwatsuki, M.; Miyamoto, Y.; Yoshida, N.; Watanabe, M.; Baba, H. PD-L1 expression, tumor-infiltrating lymphocytes, and clinical outcome in patients with surgically resected esophageal cancer. Ann. Surg. 2017, in press. [Google Scholar] [CrossRef]
- Kiyozumi, Y.; Baba, Y.; Okadome, K.; Yagi, T.; Ishimoto, T.; Iwatsuki, M.; Miyamoto, Y.; Yoshida, N.; Watanabe, M.; Komohara, Y.; et al. IDO1 expression is associated with immune tolerance and poor prognosis in patients with surgically resected esophageal cancer. Ann. Surg. 2018, in press. [Google Scholar] [CrossRef]
- Rosenberg, A.J.; Wainwright, D.A.; Rademaker, A.; Galvez, C.; Genet, M.; Zhai, L.; Lauing, K.L.; Mulcahy, M.F.; Hayes, J.P.; Odell, D.D.; et al. Indoleamine 2,3-dioxygenase 1 and overall survival of patients diagnosed with esophageal cancer. Oncotarget 2018, 9, 23482–23493. [Google Scholar] [CrossRef]
- Pelekanou, V.; Barlow, W.E.; Nahleh, Z.A.; Wasserman, B.; Lo, Y.C.; von Wahlde, M.K.; Hayes, D.; Hortobagyi, G.N.; Gralow, J.; Tripathy, D.; et al. Tumor-infiltrating lymphocytes and PD-L1 expression in pre- and posttreatment breast cancers in the SWOG S0800 phase II neoadjuvant chemotherapy trial. Mol. Cancer Ther. 2018, 17, 1324–1331. [Google Scholar] [CrossRef] [PubMed]
- Denkert, C.; von Minckwitz, G.; Brase, J.C.; Sinn, B.V.; Gade, S.; Kronenwett, R.; Pfitzner, B.M.; Salat, C.; Loi, S.; Schmitt, W.D.; et al. Tumor-infiltrating lymphocytes and response to neoadjuvant chemotherapy with or without carboplatin in human epidermal growth factor receptor 2-positive and triple-negative primary breast cancers. J. Clin. Oncol. 2015, 33, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Teng, F.; Meng, X.; Kong, L.; Mu, D.; Zhu, H.; Liu, S.; Zhang, J.; Yu, J. Tumor-infiltrating lymphocytes, forkhead box P3, programmed death ligand-1, and cytotoxic T lymphocyte-associated antigen-4 expressions before and after neoadjuvant chemoradiation in rectal cancer. Transl. Res. 2015, 166, 721–732. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.J.; Zaidi, A.H.; Smith, M.A.; Omstead, A.N.; Kosovec, J.E.; Matsui, D.; Martin, S.A.; DiCarlo, C.; Werts, E.D.; Silverman, J.F.; et al. The dynamic and transient immune microenvironment in locally advanced esophageal adenocarcinoma post chemoradiation. Ann. Surg. 2018, 268, 992–999. [Google Scholar] [CrossRef] [PubMed]
- Troiano, G.; Caponio, V.C.A.; Zhurakivska, K.; Arena, C.; Pannone, G.; Mascitti, M.; Santarelli, A.; Lo Muzio, L. High PD-L1 expression in the tumour cells did not correlate with poor prognosis of patients suffering for oral squamous cells carcinoma: A meta-analysis of the literature. Cell Prolif. 2018, e12537. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.F.; Wong, M.C.M.; Thomson, P.J.; Li, K.Y.; Su, Y.X. The prognostic role of PD-L1 expression for survival in head and neck squamous cell carcinoma: A systematic review and meta-analysis. Oral Oncol. 2018, 86, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Hatogai, K.; Kitano, S.; Fujii, S.; Kojima, T.; Daiko, H.; Nomura, S.; Yoshino, T.; Ohtsu, A.; Takiguchi, Y.; Doi, T.; et al. Comprehensive immunohistochemical analysis of tumor microenvironment immune status in esophageal squamous cell carcinoma. Oncotarget 2016, 7, 47252–47264. [Google Scholar] [CrossRef]
- Kozuma, Y.; Takada, K.; Toyokawa, G.; Kohashi, K.; Shimokawa, M.; Hirai, F.; Tagawa, T.; Okamoto, T.; Oda, Y.; Maehara, Y. Indoleamine 2,3-dioxygenase 1 and programmed cell death-ligand 1 co-expression correlates with aggressive features in lung adenocarcinoma. Eur. J. Cancer 2018, 101, 20–29. [Google Scholar] [CrossRef]
- Rosenbaum, M.W.; Gigliotti, B.J.; Pai, S.I.; Parangi, S.; Wachtel, H.; Mino-Kenudson, M.; Gunda, V.; Faquin, W.C. PD-L1 and IDO1 are expressed in poorly differentiated thyroid carcinoma. Endocr. Pathol. 2018, 29, 59–67. [Google Scholar] [CrossRef]
- Formenti, S.C.; Demaria, S. Combining radiotherapy and cancer immunotherapy: A paradigm shift. J. Natl. Cancer Inst. 2013, 105, 256–265. [Google Scholar] [CrossRef]
- Tanaka, Y.; Aoyagi, K.; Minashi, K.; Komatsuzaki, R.; Komatsu, M.; Chiwaki, F.; Tamaoki, M.; Nishimura, T.; Takahashi, N.; Oda, I.; et al. Discovery of a good responder subtype of esophageal squamous cell carcinoma with cytotoxic T-lymphocyte signatures activated by chemoradiotherapy. PLoS ONE 2015, 10, e0143804. [Google Scholar] [CrossRef] [PubMed]
- Deng, L.; Liang, H.; Burnette, B.; Beckett, M.; Darga, T.; Weichselbaum, R.R.; Fu, Y.X. Irradiation and anti-PD-L1 treatment synergistically promote antitumor immunity in mice. J. Clin. Investig. 2014, 124, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Dovedi, S.J.; Adlard, A.L.; Lipowska-Bhalla, G.; McKenna, C.; Jones, S.; Cheadle, E.J.; Stratford, I.J.; Poon, E.; Morrow, M.; Stewart, R.; et al. Acquired resistance to fractionated radiotherapy can be overcome by concurrent PD-L1 blockade. Cancer Res. 2014, 74, 5458–5468. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Bolduc, A.R.; Hoda, M.N.; Gamble, D.N.; Dolisca, S.B.; Bolduc, A.K.; Hoang, K.; Ashley, C.; McCall, D.; Rojiani, A.M.; et al. The indoleamine 2,3-dioxygenase pathway controls complement-dependent enhancement of chemo-radiation therapy against murine glioblastoma. J. Immunother. Cancer 2014, 2, 21. [Google Scholar] [CrossRef] [PubMed]
- Maleki Vareki, S.; Rytelewski, M.; Figueredo, R.; Chen, D.; Ferguson, P.J.; Vincent, M.; Min, W.; Zheng, X.; Koropatnick, J. Indoleamine 2,3-dioxygenase mediates immune-independent human tumor cell resistance to olaparib, gamma radiation, and cisplatin. Oncotarget 2014, 5, 2778–2791. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Hong, M.; Ahn, S.; Choi, Y.L.; Kim, K.M.; Oh, D.; Ahn, Y.C.; Jung, S.H.; Ahn, M.J.; Park, K.; et al. Changes in tumour expression of programmed death-ligand 1 after neoadjuvant concurrent chemoradiotherapy in patients with squamous oesophageal cancer. Eur. J. Cancer 2016, 52, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ladomersky, E.; Zhai, L.; Lenzen, A.; Lauing, K.L.; Qian, J.; Scholtens, D.M.; Gritsina, G.; Sun, X.; Liu, Y.; Yu, F.; et al. IDO1 inhibition synergizes with radiation and PD-1 blockade to durably increase survival against advanced glioblastoma. Clin. Cancer Res. 2018, 24, 2559–2573. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total (n = 158), % |
|---|---|
| Age (years) | |
| <56 | 72 (45.6) |
| ≥56 | 86 (54.4) |
| Sex | |
| Male | 131 (82.9) |
| Female | 27 (17.1) |
| Smoking history | |
| Yes | 104 (65.8) |
| No | 54 (34.2) |
| Alcohol history | |
| Yes | 57 (36.1) |
| No | 101 (63.9) |
| Performance status | |
| 0 | 90 (57.0) |
| 1–2 | 68 (43.0) |
| Weight loss | |
| <10% | 140 (88.6) |
| ≥10% | 18 (11.4) |
| Histologic grade | |
| Gx/1/2 | 118 (74.7) |
| G3 | 40 (25.3) |
| Tumor location | |
| Upper/middle | 120 (75.9) |
| Distal | 38 (24.1) |
| Primary tumor length | |
| ≤5 cm | 72 (45.6) |
| >5 cm | 86 (54.4) |
| Clinical T stage | |
| T1-2 | 30 (19.0) |
| T3-4 | 128 (81.0) |
| Clinical N stage | |
| N0 | 11 (7.0) |
| N1-3 | 147 (93.0) |
| Clinical TNM stage | |
| II | 34 (215) |
| III | 124 (78.5) |
| Chemotherapy regimen | |
| Cisplatin/vinorelbine | 92 (58.2) |
| Cisplatin/fluorouracil | 16 (10.1) |
| Cisplatin/taxane | 50 (31.6) |
| Radiation dose (Gy) | |
| Median (range) | 40.0 (36.0–50.4) |
| Radiotherapy modality | |
| 3DCRT | 105 (66.5) |
| IMRT | 53 (33.5) |
| Characteristic | IDO1 Expression | P-Value | PD-L1 Expression | P-Value | ||
|---|---|---|---|---|---|---|
| Negative | Positive | Negative | Positive | |||
| Age (years) | 0.135 | 0.098 | ||||
| <56 | 42 (41.2%) | 30 (53.6%) | 42 (40.8%) | 30 (54.5%) | ||
| ≥56 | 60 (58.8%) | 26 (46.4%) | 61 (59.2%) | 25 (45.5%) | ||
| Sex | 0.115 | 0.132 | ||||
| Male | 81 (79.4%) | 50 (89.3%) | 82 (79.6%) | 49 (89.1%) | ||
| Female | 21 (20.6%) | 6 (10.7%) | 21 (20.4%) | 6 (10.9%) | ||
| Smoking history | 0.690 | 0.041 | ||||
| Yes | 66 (64.7%) | 38 (67.9%) | 62 (60.2%) | 42 (76.4%) | ||
| No | 36 (35.3%) | 18 (32.1%) | 41 (39.8%) | 13 (23.6%) | ||
| Alcohol history | 0.045 | 0.687 | ||||
| Yes | 31 (30.4%) | 26 (46.4%) | 36 (35.0%) | 21 (38.2%) | ||
| No | 71 (69.6%) | 30 (53.6%) | 67 (65.0%) | 34 (61.8%) | ||
| Performance status | 0.480 | 0.573 | ||||
| 0 | 56 (54.9%) | 34 (60.7%) | 57 (55.3%) | 33 (60.0) | ||
| 1–2 | 46 (45.1%) | 22 (39.3%) | 46 (44.7%) | 22 (40.0%) | ||
| Weight loss | 0.213 | 0.700 | ||||
| <10% | 88 (86.3%) | 52 (92.9%) | 92 (89.3%) | 48 (87.3%) | ||
| ≥10% | 14 (13.7%) | 4 (7.1%) | 11 (10.7%) | 7 (12.7%) | ||
| Histologic grade | 0.405 | 0.679 | ||||
| Gx/1/2 | 74 (72.5%) | 44 (78.6%) | 78 (75.7%) | 40 (72.7%) | ||
| G3 | 28 (27.5%) | 12 (21.4%) | 25 (24.3%) | 15 (27.3%) | ||
| Tumor location | 0.078 | 0.763 | ||||
| Upper/middle | 82 (80.4%) | 38 (67.9%) | 79 (76.7%) | 41 (74.5%) | ||
| Distal | 20 (19.6%) | 18 (32.1%) | 24 (23.3%) | 14 (25.5%) | ||
| Primary tumor length | 0.012 | 0.090 | ||||
| ≤5 cm | 54 (52.9%) | 18 (32.1%) | 52 (50.5%) | 20 (36.4%) | ||
| >5 cm | 48 (47.1%) | 38 (67.9%) | 51 (49.5%) | 35 (63.6%) | ||
| Clinical T stage | 0.123 | 0.850 | ||||
| T1-2 | 23 (22.5%) | 7 (12.5%) | 20 (19.4%) | 10 (18.2%) | ||
| T3-4 | 79 (77.5%) | 49 (87.5%) | 83 (80.6%) | 45 (81.8%) | ||
| Clinical N stage | 0.330 | 0.332 | ||||
| N0 | 9 (8.8%) | 2 (3.6%) | 9 (8.7%) | 2 (3.6%) | ||
| N1-3 | 93 (91.2%) | 54 (96.4%) | 94 (91.3%) | 53 (96.4%) | ||
| Clinical TNM stage | 0.041 | 0.734 | ||||
| II | 27 (26.5%) | 7 (12.5%) | 23 (22.3%) | 11 (20.0) | ||
| III | 75 (73.5%) | 49 (87.5%) | 80 (77.7%) | 44 (80.0) | ||
| CD8+ TIL density | 0.264 | 0.777 | ||||
| Low | 47 (46.1%) | 31 (55.4%) | 50 (48.5%) | 28 (50.9%) | ||
| High | 55 (53.9%) | 25 (44.6%) | 53 (51.5%) | 27 (49.1%) | ||
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | P-Value | Odds Ratio (95% CI) | P-Value | |
| Age (<56 vs. ≥56) | 1.001 (0.532–1.884) | 0.997 | ||
| Sex (female vs. male) | 1.840 (0.798–4.242) | 0.153 | ||
| Smoking history (yes vs. no) | 0.580 (0.299–1.127) | 0.108 | ||
| Alcohol history (yes vs. no) | 0.597 (0.306–1.166) | 0.131 | ||
| Performance status (0 vs. 1–2) | 0.750 (0.397–1.417) | 0.375 | ||
| Weight loss (<10% vs. ≥10%) | 0.728 (0.273–1.947) | 0.527 | ||
| Histologic grade (Gx/1/2 vs. G3) | 1.182 (0.570–2.451) | 0.654 | ||
| Tumor location (upper/middle vs. distal) | 1.051 (0.503–2.200) | 0.894 | ||
| Primary tumor length (≤5 vs. >5 cm) | 1.233 (0.655–2.321) | 0.516 | ||
| Clinical TNM stage (II vs. III) | 1.231 (0.574–2.637) | 0.593 | ||
| Chemotherapy regimena (1 vs. 2/3) | 1.790 (0.934–3.431) | 0.079 | ||
| Radiation dose (≤40 vs. >40 Gy) | 0.849 (0.429–1.681) | 0.639 | ||
| Radiotherapy modality (3DCRT vs. IMRT) | 1.235 (0.631–2.417) | 0.538 | ||
| IDO1 (negative vs. positive) | 2.600 (1.294–5.224) | 0.007 | 2.194 (1.068–4.507) | 0.032 |
| PD-L1 (negative vs. positive) | 2.827 (1.392–5.739) | 0.004 | 2.425 (1.172–5.021) | 0.017 |
| CD8+ TIL density (low vs. high) | 0.560 (0.296–1.059) | 0.075 | ||
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | P-Value | Hazard Ratio (95% CI) | P-Value | |
| Age (<56 vs. ≥56) | 3.585 (1.894–6.788) | <0.001 | 3.332 (1.744–6.369) | <0.001 |
| Sex (female vs. male) | 0.280 (0.087–0.902) | 0.033 | ||
| Smoking history (yes vs. no) | 0.812 (0.435–1.516) | 0.514 | ||
| Alcohol history (yes vs. no) | 0.689 (0.389–1.221) | 0.202 | ||
| Performance status (0 vs. 1–2) | 1.061 (0.600–1.876) | 0.838 | ||
| Weight loss (<10% vs. ≥10%) | 0.993 (0.391–2.519) | 0.988 | ||
| Histologic grade (Gx/1/2 vs. G3) | 1.241 (0.615–2.501) | 0.547 | ||
| Tumor location (upper/middle vs. distal) | 1.226 (0.611–2.460) | 0.567 | ||
| Primary tumor length (≤5 vs. >5 cm) | 0.606 (0.336–1.090) | 0.095 | ||
| Clinical TNM stage (II vs. III) | 0.588 (0.263–1.314) | 0.196 | ||
| Chemotherapy regimen a (1 vs. 2/3) | 0.464 (0.258–0.837) | 0.011 | 0.420 (0.228–0.775) | 0.005 |
| Radiation dose (≤40 vs. >40 Gy) | 1.121 (0.524–2.396) | 0.769 | ||
| Radiotherapy modality (3DCRT vs. IMRT) | 1.255 (0.586–2.687) | 0.559 | ||
| IDO1 (negative vs. positive) | 0.236 (0.131–0.427) | <0.001 | 0.282 (0.153–0.519) | <0.001 |
| PD-L1 (negative vs. positive) | 0.509 (0.285–0.907) | 0.022 | ||
| CD8+ TIL density (low vs. high) | 1.748 (0.978–3.126) | 0.060 | ||
| Pathologic response (pCR vs. non-pCR) | 0.401 (0.211–0.764) | 0.005 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, S.; Zhao, L.; Liang, Z.; Liu, S.; Li, Y.; Liu, S.; Yang, H.; Liu, M.; Xi, M. Indoleamine 2,3-dioxygenase 1 and Programmed Cell Death-ligand 1 Co-expression Predicts Poor Pathologic Response and Recurrence in Esophageal Squamous Cell Carcinoma after Neoadjuvant Chemoradiotherapy. Cancers 2019, 11, 169. https://doi.org/10.3390/cancers11020169
Zhou S, Zhao L, Liang Z, Liu S, Li Y, Liu S, Yang H, Liu M, Xi M. Indoleamine 2,3-dioxygenase 1 and Programmed Cell Death-ligand 1 Co-expression Predicts Poor Pathologic Response and Recurrence in Esophageal Squamous Cell Carcinoma after Neoadjuvant Chemoradiotherapy. Cancers. 2019; 11(2):169. https://doi.org/10.3390/cancers11020169
Chicago/Turabian StyleZhou, Sha, Lei Zhao, Zhaohui Liang, Songran Liu, Yong Li, Shiliang Liu, Hong Yang, Mengzhong Liu, and Mian Xi. 2019. "Indoleamine 2,3-dioxygenase 1 and Programmed Cell Death-ligand 1 Co-expression Predicts Poor Pathologic Response and Recurrence in Esophageal Squamous Cell Carcinoma after Neoadjuvant Chemoradiotherapy" Cancers 11, no. 2: 169. https://doi.org/10.3390/cancers11020169
APA StyleZhou, S., Zhao, L., Liang, Z., Liu, S., Li, Y., Liu, S., Yang, H., Liu, M., & Xi, M. (2019). Indoleamine 2,3-dioxygenase 1 and Programmed Cell Death-ligand 1 Co-expression Predicts Poor Pathologic Response and Recurrence in Esophageal Squamous Cell Carcinoma after Neoadjuvant Chemoradiotherapy. Cancers, 11(2), 169. https://doi.org/10.3390/cancers11020169