Detection and Prognostic Relevance of Circulating and Disseminated Tumour Cell in Dogs with Metastatic Mammary Carcinoma: A Pilot Study

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Results
2.1. Clinical Characteristics
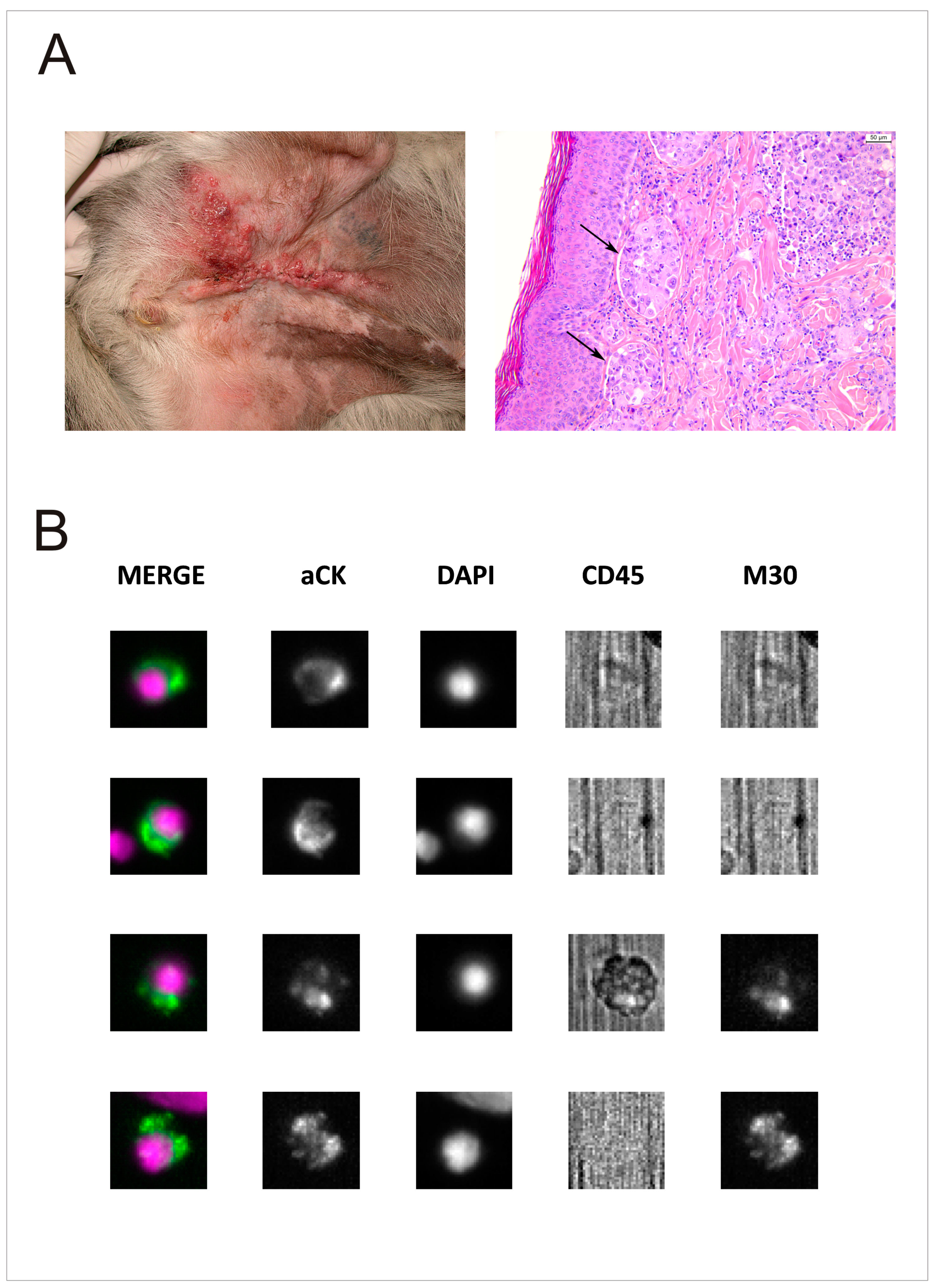
2.2. Histopathology
2.3. Treatment and Response
2.4. CTC and DTC Prevalence in MMC
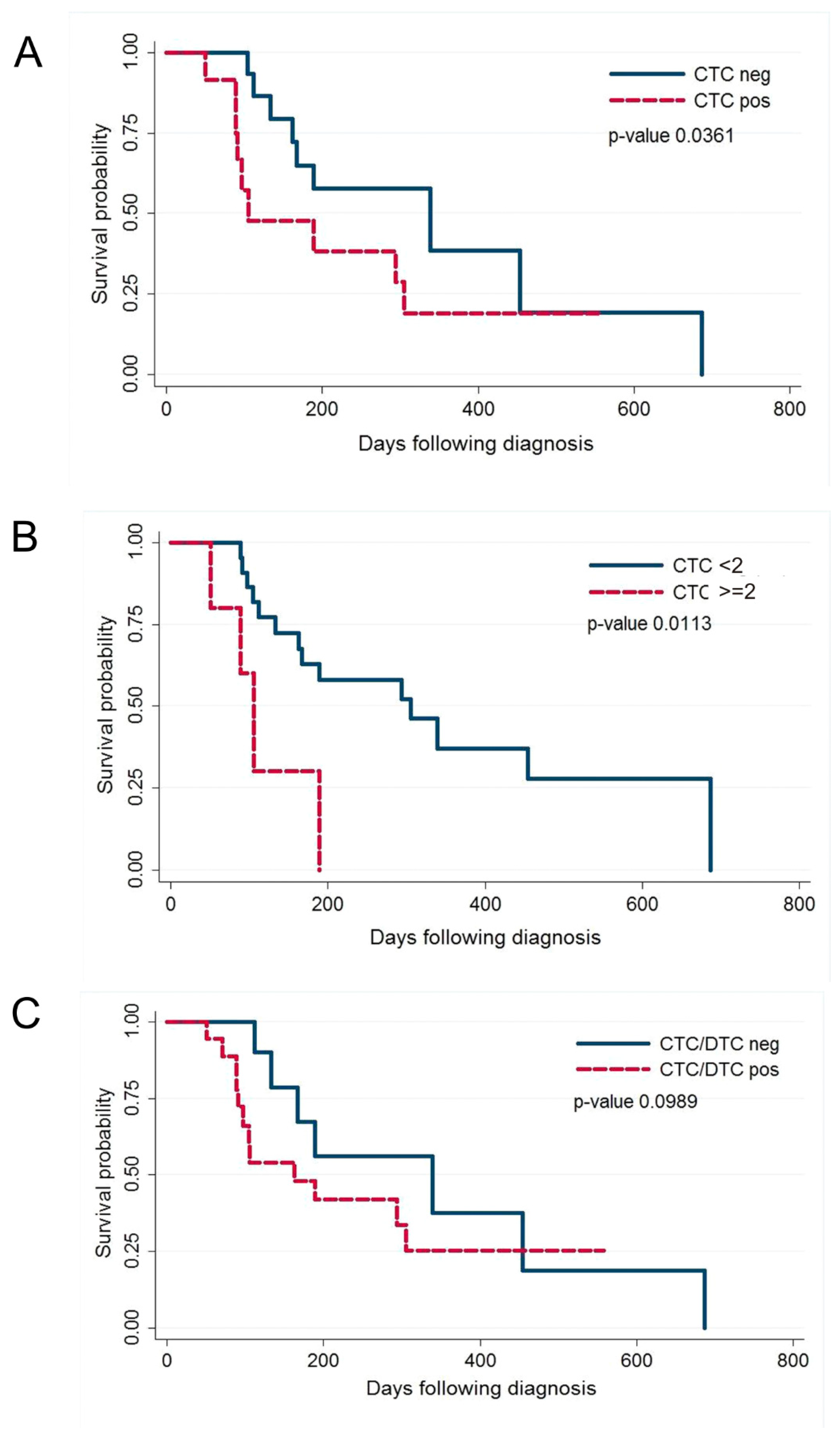
2.5. Prognostic Significance of CTC/DTC Enumeration
3. Discussion
4. Methods
4.1. Animals and Samples
- 1.
- At least one unidimensional lesion measurable by ultrasound or computed tomography (CT), according to the canine Response Evaluation Criteria In Solid Tumours version 1.0 (cRECIST v1.0) [41];
- 2.
- Clinically detectable metastatic disease or the presence of lymphatic emboli, confirmed by histopathology;
- 3.
- Prior surgery without systemic chemotherapy permitted.
- 4.
- Availability of tumour tissue for histopathological evaluation and immune-histochemical staining.
4.2. Histopathological Analysis
4.3. CTCs/DTCs Enumeration
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Frese, K.K.; Tuveson, D.A. Maximizing mouse cancer models. Nat. Rev. Cancer 2007, 7, 645–658. [Google Scholar] [CrossRef] [PubMed]
- Decker, W.K.; da Silva, R.F.; Sanabria, M.H.; Angelo, L.S.; Guimaraes, F.; Burt, B.M.; Kheradmand, F.; Paust, S. Cancer Immunotherapy: Historical Perspective of a Clinical Revolution and Emerging Preclinical Animal Models. Front. Immunol. 2017, 8, 829. [Google Scholar] [CrossRef] [PubMed]
- Abdelmegeed, S.M.; Mohammed, S. Canine mammary tumours as a model for human disease. Oncol. Lett. 2018, 15, 8195–8205. [Google Scholar] [PubMed]
- Schneider, R. Comparison of age, sex and incidence rates in human and canine breast cancer. Cancer 1970, 26, 419–426. [Google Scholar] [CrossRef]
- Dobson, J.M.; Samuel, S.; Milstein, H.; Rogers, K.; Wood, J.L. Canine neoplasia in the UK: Estimates of incidence rates from a population of insured dogs. J. Small Anim. Pract. 2002, 43, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Merlo, D.F.; Rossi, L.; Pellegrino, C.; Ceppi, M.; Cardellino, U.; Capurro, C.; Ratto, A.; Sambucco, P.L.; Sestito, V.; Tanara, G.; et al. Cancer incidence in pet dogs: Findings of the Animal Tumor Registry of Genoa, Italy. J. Vet. Intern. Med. 2008, 22, 976–984. [Google Scholar] [CrossRef] [PubMed]
- Vascellari, M.; Capello, K.; Carminato, A.; Zanardello, C.; Baioni, E.; Mutinelli, F. Incidence of mammary tumours in the canine population living in the Veneto region (Northeastern Italy): Risk factors and similarities to human breast cancer. Prev. Vet. Med. 2016, 126, 183–189. [Google Scholar] [CrossRef]
- Dorn, C.R.; Taylor, D.O.; Schneider, R.; Hibbard, H.H.; Klauber, M.R. Survey of animal neoplasms in Alameda and Contra Costa Counties, California. II. Cancer morbidity in dogs and cats from Alameda County. J. Natl. Cancer Inst. 1968, 40, 307–318. [Google Scholar]
- Vascellari, M.; Baioni, E.; Ru, G.; Carminato, A.; Mutinelli, F. Animal tumour registry of two provinces in northern Italy: Incidence of spontaneous tumours in dogs and cats. BMC Vet. Res. 2009, 5, 39. [Google Scholar] [CrossRef]
- Sorenmo, K.U.; Shofer, F.S.; Goldschmidt, M.H. Effect of spaying and timing of spaying on survival of dogs with mammary carcinoma. J. Vet. Intern. Med. 2000, 14, 266–270. [Google Scholar] [CrossRef]
- Schneider, R.; Dorn, C.R.; Taylor, D.O. Factors influencing canine mammary cancer development and postsurgical survival. J. Natl. Cancer Inst. 1969, 43, 1249–1261. [Google Scholar] [PubMed]
- Beauvais, W.; Cardwell, J.M.; Brodbelt, D.C. The effect of neutering on the risk of mammary tumours in dogs—A systematic review. J. Small Anim. Pract. 2012, 53, 314–322. [Google Scholar] [CrossRef]
- Misdorp, W.; Hart, A.A. Prognostic factors in canine mammary cancer. J. Natl. Cancer Inst. 1976, 56, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, S.A.; Lee, A.C.; Saunders, W.J. Classification and behavior of canine mammary epithelial neoplasms based on life-span observations in beagles. Vet. Pathol. 1999, 36, 423–436. [Google Scholar] [CrossRef] [PubMed]
- Gilbertson, S.R.; Kurzman, I.D.; Zachrau, R.E.; Hurvitz, A.I.; Black, M.M. Canine mammary epithelial neoplasms: Biologic implications of morphologic characteristics assessed in 232 dogs. Vet. Pathol. 1983, 20, 127–142. [Google Scholar] [CrossRef] [PubMed]
- Tran, C.M.; Moore, A.S.; Frimberger, A.E. Surgical treatment of mammary carcinomas in dogs with or without postoperative chemotherapy. Vet. Comp. Oncol. 2016, 14, 252–262. [Google Scholar] [CrossRef] [PubMed]
- Goldschmidt, M.; Pena, L.; Rasotto, R.; Zappulli, V. Classification and grading of canine mammary tumours. Vet. Pathol. 2011, 48, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Pena, L.; De Andres, P.J.; Clemente, M.; Cuesta, P.; Perez-Alenza, M.D. Prognostic value of histological grading in noninflammatory canine mammary carcinomas in a prospective study with two-year follow-up: Relationship with clinical and histological characteristics. Vet. Pathol. 2013, 50, 94–105. [Google Scholar] [CrossRef]
- Yamagami, T.; Kobayashi, T.; Takahashi, K.; Sugiyama, M. Prognosis for canine malignant mammary tumours based on TNM and histologic classification. J. Vet. Med. Sci. 1996, 58, 1079–1083. [Google Scholar] [CrossRef]
- Klopfleisch, R.; von Euler, H.; Sarli, G.; Pinho, S.S.; Gartner, F.; Gruber, A.D. Molecular carcinogenesis of canine mammary tumours: News from an old disease. Vet. Pathol. 2011, 48, 98–116. [Google Scholar] [CrossRef]
- Paget, S. The distribution of secondary growths in cancer of the breast. 1889. Cancer Metastasis Rev. 1989, 8, 98–101. [Google Scholar] [PubMed]
- Lambert, A.W.; Pattabiraman, D.R.; Weinberg, R.A. Emerging Biological Principles of Metastasis. Cell 2017, 168, 670–691. [Google Scholar] [CrossRef] [PubMed]
- Braun, S.; Vogl, F.D.; Naume, B.; Janni, W.; Osborne, M.P.; Coombes, R.C.; Schlimok, G.; Diel, I.J.; Gerber, B.; Gebauer, G.; et al. A pooled analysis of bone marrow micrometastasis in breast cancer. N. Engl. J. Med. 2005, 353, 793–802. [Google Scholar] [CrossRef] [PubMed]
- Husemann, Y.; Geigl, J.B.; Schubert, F.; Musiani, P.; Meyer, M.; Burghart, E.; Forni, G.; Eils, R.; Fehm, T.; Riethmuller, G.; et al. Systemic spread is an early step in breast cancer. Cancer Cell 2008, 13, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Pantel, K.; Brakenhoff, R.H.; Brandt, B. Detection, clinical relevance and specific biological properties of disseminating tumour cells. Nat. Rev. Cancer 2008, 8, 329–340. [Google Scholar] [CrossRef] [PubMed]
- Fidler, I.J. Metastasis: Quantitative analysis of distribution and fate of tumour emboli labeled with 125 I-5-iodo-2’-deoxyuridine. J. Natl. Cancer Inst. 1970, 45, 773–782. [Google Scholar] [PubMed]
- Fidler, I.J.; Talmadge, J.E. Evidence that intravenously derived murine pulmonary melanoma metastases can originate from the expansion of a single tumour cell. Cancer Res. 1986, 46, 5167–5171. [Google Scholar] [PubMed]
- Allard, W.J.; Matera, J.; Miller, M.C.; Repollet, M.; Connelly, M.C.; Rao, C.; Tibbe, A.G.; Uhr, J.W.; Terstappen, L.W. Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with nonmalignant diseases. Clin. Cancer Res. 2004, 10, 6897–6904. [Google Scholar] [CrossRef] [PubMed]
- Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, M.C.; Reuben, J.M.; Doyle, G.V.; Allard, W.J.; Terstappen, L.W.; et al. Circulating tumour cells, disease progression and survival in metastatic breast cancer. N. Engl. J. Med. 2004, 351, 781–791. [Google Scholar] [CrossRef] [PubMed]
- Hayes, D.F.; Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Miller, M.C.; Matera, J.; Allard, W.J.; Doyle, G.V.; Terstappen, L.W. Circulating tumour cells at each follow-up time point during therapy of metastatic breast cancer patients predict progression-free and overall survival. Clin. Cancer Res. 2006, 12, 4218–4224. [Google Scholar] [CrossRef] [PubMed]
- Bidard, F.C.; Peeters, D.J.; Fehm, T.; Nole, F.; Gisbert-Criado, R.; Mavroudis, D.; Grisanti, S.; Generali, D.; Garcia-Saenz, J.A.; Stebbing, J.; et al. Clinical validity of circulating tumour cells in patients with metastatic breast cancer: A pooled analysis of individual patient data. Lancet Oncol. 2014, 15, 406–414. [Google Scholar] [CrossRef]
- Chmielewska, M.; Losiewicz, K.; Socha, P.; Mecik-Kronenberg, T.; Wasowicz, K. The application of circulating tumour cells detecting methods in veterinary oncology. Pol. J. Vet. Sci. 2013, 16, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Da Costa, A.; Lenze, D.; Hummel, M.; Kohn, B.; Gruber, A.D.; Klopfleisch, R. Identification of six potential markers for the detection of circulating canine mammary tumour cells in the peripheral blood identified by microarray analysis. J. Comp. Pathol. 2012, 146, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Da Costa, A.; Kohn, B.; Gruber, A.D.; Klopfleisch, R. Multiple RT-PCR markers for the detection of circulating tumour cells of metastatic canine mammary tumours. Vet. J. 2013, 196, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Mego, M.; Gao, H.; Cohen, E.N.; Anfossi, S.; Giordano, A.; Tin, S.; Fouad, T.M.; De Giorgi, U.; Giuliano, M.; Woodward, W.A.; et al. Circulating tumour cells (CTCs) are associated with abnormalities in peripheral blood dendritic cells in patients with inflammatory breast cancer. Oncotarget 2017, 8, 35656–35668. [Google Scholar] [CrossRef] [PubMed]
- Rossi, E.; Basso, U.; Celadin, R.; Zilio, F.; Pucciarelli, S.; Aieta, M.; Barile, C.; Sava, T.; Bonciarelli, G.; Tumolo, S.; et al. M30 Neoepitope Expression in Epithelial Cancer: Quantification of Apoptosis in Circulating Tumor Cells by CellSearch Analysis. Clin. Cancer Res. 2010, 16, 5233–5243. [Google Scholar] [CrossRef] [PubMed]
- Rupa, J.D.; de Bruine, A.P.; Gerbers, A.J.; Leers, M.P.; Nap, M.; Kessels, A.G.; Schutte, B.; Arends, J.W. Simultaneous detection of apoptosis and proliferation in colorectal carcinoma by multiparameter flow cytometry allows separation of high and low-turnover tumours with distinct clinical outcome. Cancer 2003, 97, 2404–2411. [Google Scholar] [CrossRef] [PubMed]
- Hayes, D.F. Biomarker validation and testing. Mol. Oncol. 2015, 9, 960–966. [Google Scholar] [CrossRef] [PubMed]
- Fehm, T.; Braun, S.; Muller, V.; Janni, W.; Gebauer, G.; Marth, C.; Schindlbeck, C.; Wallwiener, D.; Borgen, E.; Naume, B.; et al. A concept for the standardized detection of disseminated tumour cells in bone marrow from patients with primary breast cancer and its clinical implementation. Cancer 2006, 107, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Muller, V.; Pantel, K. Bone marrow micrometastases and circulating tumour cells: Current aspects and future perspectives. Breast Cancer Res. 2004, 6, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, S.M.; Thamm, D.H.; Vail, D.M.; London, C.A. Response evaluation criteria for solid tumours in dogs (v1.0): A Veterinary Cooperative Oncology Group (VCOG) consensus document. Vet. Comp. Oncol. 2015, 13, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Misdorp, W.; Else, R.W.; Hellme’n, E.; Lipscomb, T.P. Histological Classification of Mammary Tumours of the Dog and the Cat; Armed Forces Institute of Pathology and the American Registry of Pathology and The World Health Organization: Washington, DC, USA, 1999; Volume 7. [Google Scholar]
- Jaillardon, L.; Abadie, J.; Godard, T.; Campone, M.; Loussouarn, D.; Siliart, B.; Nguyen, F. The dog as a naturally-occurring model for insulin-like growth factor type 1 receptor-overexpressing breast cancer: An observational cohort study. BMC Cancer 2015, 15, 664. [Google Scholar] [CrossRef] [PubMed]
- Thamm, D.H.; Hayes, D.F.; Meuten, T.; Laver, T.; Thomas, D.G. Epithelial Cell Adhesion Molecule Expression in Canine Tumours. J. Comp. Pathol. 2016, 155, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Sozmen, M.; Brown, P.J.; Eveson, J.W. Cytokeratin immunostaining in normal dog major and minor salivary glands. Vet. Res. 1998, 29, 457–465. [Google Scholar] [PubMed]
- Rossi, E.; Rugge, M.; Facchinetti, A.; Pizzi, M.; Nardo, G.; Barbieri, V.; Manicone, M.; De Faveri, S.; Chiara Scaini, M.; Basso, U.; et al. Retaining the long-survive capacity of Circulating Tumor Cells (CTCs) followed by xeno-transplantation: Not only from metastatic cancer of the breast but also of prostate cancer patients. Oncoscience 2014, 1, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Kleinbaum, D.G.; Klein, M. Survival Analysis A Self-Learning Text; Springer: New York, NY, USA, 2005. [Google Scholar]
- Morrow, C.J.; Trapani, F.; Metcalf, R.L.; Bertolini, G.; Hodgkinson, C.L.; Khandelwal, G.; Kelly, P.; Galvin, M.; Carter, L.; Simpson, K.L.; et al. Tumourigenic non-small-cell lung cancer mesenchymal circulating tumour cells: A clinical case study. Ann. Oncol. 2016, 27, 1155–1160. [Google Scholar] [CrossRef] [PubMed]
- Hodgkinson, C.L.; Morrow, C.J.; Li, Y.; Metcalf, R.L.; Rothwell, D.G.; Trapani, F.; Polanski, R.; Burt, D.J.; Simpson, K.L.; Morris, K.; et al. Tumorigenicity and genetic profiling of circulating tumour cells in small-cell lung cancer. Nat. Med. 2014, 20, 897–903. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.F.; Xu, Y.; Yan g, X.R.; Guo, W.; Zhang, X.; Qiu, S.J.; Shi, R.Y.; Hu, B.; Zhou, J.; Fan, J. Circulating stem cell-like epithelial cell adhesion molecule-positive tumour cells indicate poor prognosis of hepatocellular carcinoma after curative resection. Hepatology 2013, 57, 1458–1468. [Google Scholar] [CrossRef] [PubMed]
- Baccelli, I.; Schneeweiss, A.; Riethdorf, S.; Stenzinger, A.; Schillert, A.; Vogel, V.; Klein, C.; Saini, M.; Bauerle, T.; Wallwiener, M.; et al. Identification of a population of blood circulating tumour cells from breast cancer patients that initiates metastasis in a xenograft assay. Nat. Biotechnol. 2013, 31, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Lallo, A.; Schenk, M.W.; Frese, K.K.; Blackhall, F.; Dive, C. Circulating tumour cells and CDX models as a tool for preclinical drug development. Transl. Lung Cancer Res. 2017, 6, 397–408. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | N | CTC-Neg | CTC-Pos | p-Value |
|---|---|---|---|---|
| Breed | ||||
| Purebred | 18 | 11 (61.11%) | 7 (38.89%) | 0.448 |
| Crossbreed | 9 | 4 (44.44%) | 5 (55.56%) | |
| Age (years) | 27 | 10.53 (SD * 1.99) | 11.16 (SD * 2.72) | 0.492 |
| Weight (kg) | 27 | 20.83 (SD * 13.87) | 17.23 (SD * 11.33) | 0.475 |
| Previous surgery | ||||
| Non-surgical candidates | 6 | 3 (50.00%) | 3 (50.00%) | 1.000 |
| Prior surgery | 21 | 12 (57.14%) | 9 (42.86%) | |
| Neutering status | ||||
| Intact | 3 | 2 (66.67%) | 1 (33.33%) | 1.000 |
| Neutered | 24 | 13 (54.17%) | 11 (45.83%) | |
| Grading | ||||
| 1–2 | 8 | 3 (37.50%) | 5 (62.50%) | 0.204 |
| 3 | 16 | 11 (68.75%) | 5 (31.25%) | |
| Inflammatory carcinoma | ||||
| No | 14 | 11 (78.57%) | 3 (21.43%) | 0.035 |
| Yes | 10 | 3 (30.00%) | 7 (70.00%) | |
| Staging | ||||
| III + IV | 10 | 5 (50.00%) | 5 (50.00%) | 0.706 |
| V | 17 | 10 (58.82%) | 7 (41.18%) | |
| Metastatic sites | ||||
| Single | 12 | 6 (50.00%) | 6 (50.00%) | 1.000 |
| Multiple | 14 | 8 (57.14%) | 6 (42.86%) | |
| Oestrogen receptor | ||||
| Negative | 18 | 10 (55.56%) | 8 (44.44%) | 1.000 |
| Positive | 6 | 4 (66.67%) | 2 (33.33%) | |
| HER-2 | ||||
| Negative | 18 | 11 (61.11%) | 7 (38.89%) | 0.665 |
| Positive | 6 | 3 (50.00%) | 3 (50.00%) | |
| Progesterone receptor | ||||
| Negative | 23 | 13 (56.52%) | 10 (43.48%) | na ** |
| Positive | 1 | 1 (100.00%) | 0 (0.00%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marconato, L.; Facchinetti, A.; Zanardello, C.; Rossi, E.; Vidotto, R.; Capello, K.; Melchiotti, E.; Laganga, P.; Zamarchi, R.; Vascellari, M. Detection and Prognostic Relevance of Circulating and Disseminated Tumour Cell in Dogs with Metastatic Mammary Carcinoma: A Pilot Study. Cancers 2019, 11, 163. https://doi.org/10.3390/cancers11020163
Marconato L, Facchinetti A, Zanardello C, Rossi E, Vidotto R, Capello K, Melchiotti E, Laganga P, Zamarchi R, Vascellari M. Detection and Prognostic Relevance of Circulating and Disseminated Tumour Cell in Dogs with Metastatic Mammary Carcinoma: A Pilot Study. Cancers. 2019; 11(2):163. https://doi.org/10.3390/cancers11020163
Chicago/Turabian StyleMarconato, Laura, Antonella Facchinetti, Claudia Zanardello, Elisabetta Rossi, Riccardo Vidotto, Katia Capello, Erica Melchiotti, Paola Laganga, Rita Zamarchi, and Marta Vascellari. 2019. "Detection and Prognostic Relevance of Circulating and Disseminated Tumour Cell in Dogs with Metastatic Mammary Carcinoma: A Pilot Study" Cancers 11, no. 2: 163. https://doi.org/10.3390/cancers11020163
APA StyleMarconato, L., Facchinetti, A., Zanardello, C., Rossi, E., Vidotto, R., Capello, K., Melchiotti, E., Laganga, P., Zamarchi, R., & Vascellari, M. (2019). Detection and Prognostic Relevance of Circulating and Disseminated Tumour Cell in Dogs with Metastatic Mammary Carcinoma: A Pilot Study. Cancers, 11(2), 163. https://doi.org/10.3390/cancers11020163