Health Status in Long-Term Survivors of Hepatoblastoma

 ,
,
Abstract
1. Introduction
2. Results
2.1. Health Status and Performance Evaluation
2.1.1. Physical Performance
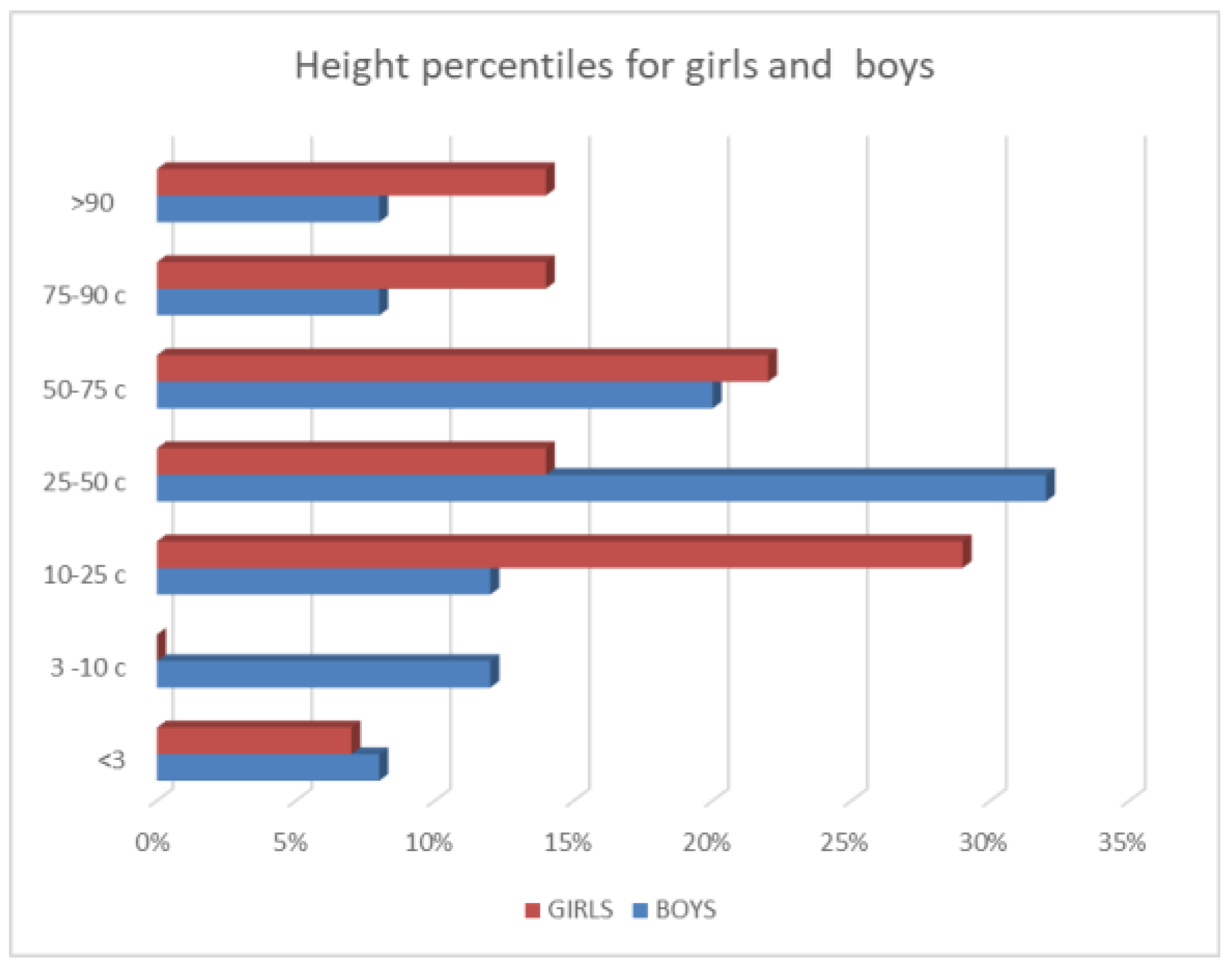
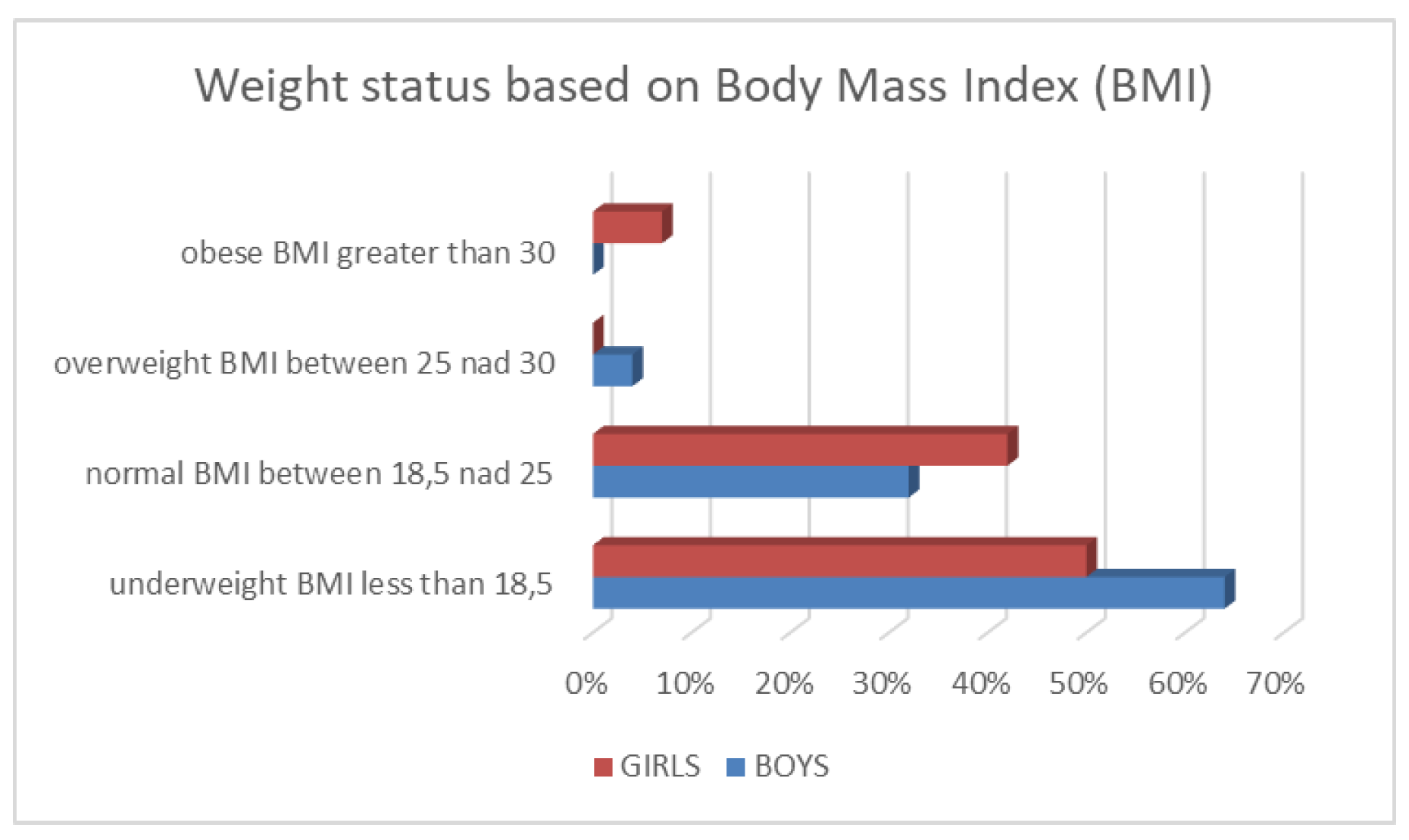
2.1.2. Physical Development
2.1.3. Puberty
2.1.4. Hearing
2.1.5. Cardiovascular Status
2.1.6. Skeletal System
2.1.7. Nephrotoxicity
2.1.8. Genito-Urinary
2.1.9. Gastrointestinal
2.1.10. Neurological Disorders
2.1.11. Hematological Disorders
2.1.12. Late complications of surgical tumor resection
2.1.13. Late Complications after Liver Transplantation
2.1.14. School performance
2.1.15. Second malignant neoplasms
2.1.16. Deaths
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Perilongo, G.; Maibach, R.; Shafford, E.; Brugieres, L.; Brock, P.; Morland, B.; de Camargo, B.; Zsiros, J.; Roebuck, D.; Zimmermann, A.; et al. Cisplatin versus Cisplatin plus Doxorubicin for Standard-Risk Hepatoblastoma. N. Engl. J. Med. 2009, 361, 1662–1670. [Google Scholar] [CrossRef] [PubMed]
- Zsíros, J.; Maibach, R.; Shafford, E.; Brugieres, L.; Brock, P.; Czauderna, P.; Roebuck, D.; Childs, M.; Zimmermann, A.; Laithier, V.; et al. Successful treatment of childhood High-Risk Hepatoblastoma with dose-intensive multiagent chemotherapy and surgery: Final results of the SIOPEL-3HR study. J. Clin. Oncol. 2010, 28, 2584–2590. [Google Scholar]
- Czauderna, P. Hepatoblastoma throughout SIOPEL trials-clinical lessons learnt. Front. Biosci. (Elite Ed) 2012, 4, 470–479. [Google Scholar] [CrossRef] [PubMed]
- Hiyama, E.; Kurihara, S.; Ueda, Y.; Hishiki, T.; Ida, K.; Iehara, T.; Watanabe, K.; Hoshino, K.; Ko, K.; Tanaka, Y. Late toxicities, especially second malignancies, with GWAS analysis in hepatoblastoma cases treated in the Japanese study group for pediatric liver tumor protocol-2. J. Clin. Oncol. 2019, 37, 10043. [Google Scholar] [CrossRef]
- Armenian, S.H.; Bhatia, S. Chronic Health Conditions in Childhood Cancer Survivors: Is it All Treatment-Related—Or Do Genetics Play a Role? J. Gen. Intern. Med. 2009, 24, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Clemens, E.; van der Kooi, A.L.F.; Broer, L.; van Dulmen-den Broeder, E.; Visscher, H.; Kremer, L.; Tissing, W.; Loonen, J.; Ronckers, C.M.; Pluijm, S.M.F.; et al. The influence of genetic variation on late toxicities in childhood cancer survivors: A review. Crit. Rev. Hematol. Oncol. 2018, 126, 154–167. [Google Scholar] [CrossRef] [PubMed]
- Bertolini, P.; Lassalle, M.; Mercier, G.; Raquin, M.A.; Izzi, G.; Corradini, N.; Hartmann, O. Platinum compound-related ototoxicity in children: Long-term follow-up reveals continuous worsening of hearing loss. J. Pediatr. Hematol. Oncol. 2004, 26, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Brock, P.R.; Yeomans, E.C.; Bellman, S.C.; Pritchard, J. Cisplatin therapy in infants: Short and long-term morbidity. Br. J. Cancer 1992, 18, S36–S40. [Google Scholar]
- Brock, P.R.; Knight, K.R.; Freyer, D.R.; Campbell, K.C.; Steyger, P.S.; Blakley, B.W.; Rassekh, S.R.; Chang, K.W.; Fligor, B.J.; Rajput, K.; et al. Platinum-induced ototoxicity in children: A consensus review on mechanisms, predisposition, and protection, including a new International Society of Pediatric Oncology Boston ototoxicity scale. J. Clin. Oncol 2012, 30, 2408–2417. [Google Scholar] [CrossRef] [PubMed]
- Sivaprakasam, P.; Gupta, A.A.; Greenberg, M.L.; Capra, M.; Nathan, P.C. Survival and long-term outcomes in children with Hepatoblastoma treated with continuous infusion of Cisplatin and Doxorubicin. J. Ped. Hematol. Oncol. 2011, 33, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Brock, P.R.; Maibach, R.; Childs, M.; Rajput, K.; Roebuck, D.; Sullivan, M.J.; Laithier, V.; Ronghe, M.; Dall’Igna, P.; Hiyama, E.; et al. Sodium thiosulfate for protection from Cisplatin-Induced hearing loss. N. Engl. J. Med. 2018, 378, 2376–2385. [Google Scholar] [CrossRef] [PubMed]
- PHITT - University of Birmingham. Available online: https://www.birmingham.ac.uk (accessed on 18 June 2019).
- Gurney, J.G.; Tersak, J.M.; Ness, K.K.; Landier, W.; Matthay, K.K.; Schmidt, M.L. Hearing loss, quality of life, and academic problems in long-term neuroblastoma survivors: A report from the Children’s oncology group. Pediatrics 2007, 120, e1229–e1236. [Google Scholar] [CrossRef] [PubMed]
- Bess, F.H.; Dodd-Murphy, J.; Parker, R.A. Children with minimal sensorineural hearing loss: Prevalence, educational performance and functional status. Ear Hear. 1998, 19, 339–354. [Google Scholar] [CrossRef] [PubMed]
- Mertens, A.C.; Liu, Q.; Neglia, J.P.; Wasilewski, K.; Leisenring, W.; Armstrong, G.T.; Robison, L.l.; Yasui, Y. Cause-specific late mortality among 5-year survivors of childhood cancer: The childhood cancer survivor study. J. Natl. Cancer Inst. 2008, 100, 1368–1379. [Google Scholar] [CrossRef] [PubMed]
- Tukenova, M.; Guibout, C.; Oberlin, O.; Doyon, F.; Mousannif, A.; Haddy, N.; Guerin, S.; Packquement, H.; Aouba, A.; Hawkins, M.; et al. Role of cancer treatment in long-term overall and cardiovascular mortality after childhood cancer. J. Clin. Oncol. 2010, 28, 1308–1315. [Google Scholar] [CrossRef] [PubMed]
- Bagnasco, F.; Caruso, S.; Andreanob, A.; Valsecchi, G.M.; Jankovic, M.; Biondi, A.; Miligi, L.; Casella, C.; Terenziani, M.; Massimino, M.; et al. Late mortality and causes of death among 5-year survivors of childhood cancer diagnosed in the period 1960–1999 and registered in the Italian Off-Therapy registry. Eur. J. Cancer 2019, 110, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Lipshultz, S.E.; Diamond, M.B.; Franco, V.I.; Aggarwal, S.; Leger, K.; Santos, M.V.; Sallan, S.E.; Chow, E.J. Managing Chemotherapy-Related cardiotoxicity in survivors of childhood cancers. Paediatr. Drugs 2014, 16, 373–389. [Google Scholar] [CrossRef] [PubMed]
- Oeffinger, K.C.; Mertens, A.C.; Sklar, C.A.; Kawashima, T.; Hudson, M.M.; Meadows, A.T.; Fridman, D.L.; Marina, N.; Hobbie, W.; Kadan-Lottick, N.S.; et al. Chronic health conditions in adult survivors of childhood cancer. N. Engl. J. Med. 2006, 355, 1572–1582. [Google Scholar] [CrossRef] [PubMed]
- Kremer, L.C.; van Dalen, E.C.; Offringa, M.; Otenkamp, J.; Voute, P.A. Anthracycline-induced clinical heart failure in a cohort of 607 children: Long-term follow-up study. J. Clin. Oncol. 2001, 19, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Armenian, S.; Smita, B. Predicting and preventing Anthracycline-Related cardiotoxicity. Am. Soc. Clin. Oncol. Educ. B 2018, 38, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Neglia, J.P.; Friedman, D.L.; Yasui, Y.; Mertens, A.C.; Hammond, S.; Stovall, M.; Donaldson, S.S.; Meadows, A.T.; Robison, L.L. Second malignant neoplasms in five-year survivors of childhood cancer: Childhood cancer survivor study. JNCI J. Natl. Cancer Inst. 2001, 93, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Ju, H.Y.; Moon, E.K.; Lim, J.; Park, B.K.; Shin, H.Y.; Won, Y.J.; Park, H.J. Second malignant neoplasms after childhood cancer: A nationwide population-based study in Korea. PLoS ONE 2018, 13, e0207243. [Google Scholar] [CrossRef] [PubMed]
- Hepatoblastoma and Medulloblastoma: Justin’s Story. Available online: https://www.chop.edu/stories/hepatoblastoma-and-medulloblastoma-justin-s-story (accessed on 19 June 2019).
- Teepen, J.C.; van Leeuwen, F.E.; Tissing, W.J.; van Dulmen-den Broeder, E.; van den Heuvel-Eibrink, M.M.; van der Pal, H.J.; Loonen, J.J.; Bresters, D.; Versluys, B.; Neggers, S.J.C.M.M.; et al. Long-Term Risk of Subsequent Malignant Neoplasms After Treatment of Childhood Cancer in the DCOG LATER Study Cohort: Role of Chemotherapy. J Clin Oncol. 2017, 35, 2288–2298. [Google Scholar] [CrossRef] [PubMed]
- Trobaugh-Lotrario, A.D.; López-Terrada, D.; Li, P.; Feusner, J.H. Hepatoblastoma in patients with molecularly proven familial adenomatous polyposis: Clinical characteristics and rationale for surveillance screening. Pediatr. Blood Cancer 2018, 65, e27103. [Google Scholar] [CrossRef] [PubMed]
- Eren, E.; Demirkaya, M.; Çakır, E.D.P.; Sevinir, B.; Sağlam, H.; Tarım, O. A rare cause of precocious puberty: Hepatoblastoma. J. Clin. Res. Pediatr. Endocrinol. 2009, 1, 281–283. [Google Scholar] [CrossRef] [PubMed]
- Marino, S.; Caruso, M.; Magro, G.; D’Amico, S.; La Spina, M.; Moscheo, C.; Russo, G.; Di Cataldo, A. Hepatoblastoma presenting as precocious puberty: A case report. J. Pediatr. Endocrinol. Metab. 2015, 28, 429–432. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, C.A.J.; Gietema, J.A.; Vonk, J.M.; Tissing, W.J.E.; Hendrika, M.; Boezen, H.M.; Zwart, N.; Postma, A. Body mass index and annual increase of body mass index in long-term childhood cancer survivors; relationship to treatment. Support. Care Cancer 2012, 20, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Wasilewski-Masker, K.; Kaste, S.C.; Hudson, M.M.; Esiashvili, N.; Mattano, L.A.; Meacham, L.R. Bone mineral density deficits in survivors of childhood cancer: Long-term follow-up guidelines and review of the literature. Pediatrics 2008, 121, e705–e713. [Google Scholar] [CrossRef] [PubMed]
- Den Hoed, M.; Klap, B.C.; Te Winkel, M.L.; Pieters, R.; van Waas, M.; Neggers, S.J.; Boot, A.M.; Blijdorp, K.; van Dorp, W.; Pluijm, S.M.; et al. Bone mineral density after childhood cancer in 346 long-term adult survivors of childhood cancer. Osteoporos. Int. 2014, 26, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Towbin, A.J.; Braojos Braga, F.D.C.; Zhang, B.; Geller, J.I.; Tiao, G.M.; Podberesky, D.J. Fractures in children with newly diagnosed hepatoblastoma. Pediatr. Radiol. 2018, 48, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Skinner, R. Late renal toxicity of treatment for childhood malignancy: Risk factors, long-term outcomes, and surveillance. Pediatr. Nephrol. 2018, 33, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Kaliciński, P.; Szymczak, M.; Smirska, E.; Pawłowska, J.; Teisseyre, J.; Kamiński, A.; Broniszczak, D.; Lembas, A.; Klimaszewski, J. Longitudinal study of renal function in pediatric liver transplant recipients. Ann. Transplant. 2005, 10, 53–58. [Google Scholar] [PubMed]
- Ismail, H.; Broniszczak, D.; Kaliciński, P.; Dembowska-Bagińska, B.; Perek, D.; Teisseyre, J.; Kluge, P.; Kościesza, A.; Lembas, A.; Markiewicz, M. Changing treatment and outcome of children with hepatoblastoma: Analysis of a single center experience over the last 20 years. J. Pediatr. Surg. 2012, 479, 1331–1339. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Buuren, S. Body-mass index cut-off values for underweight in Dutch children. Ned. Tijdschr. Geneeskd. 2004, 148, 1967–1972. [Google Scholar]
- Body Mass Index - BMI - WHO/Europe. Nutrition. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 6 July 2019).
- Marshall, W.A.; Tanner, J.M. Variations in pattern of pubertal changes in girls. Arch. Dis. Child. 1969, 44, 291–303. [Google Scholar] [CrossRef] [PubMed]
- Brock, P.R.; Bellman, S.C.; Yeomans, E.C.; Pinkerton, C.R.; Pritchard, J. Cisplatin ototoxicity in children: A practical grading system. Med. Pediatr. Oncol. 1991, 19, 295–300. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No/Male Female | Age at Diagnosis m-Months, y-Years | Age at Transplan-Tation | Indications for Transplantation | Age at Last Follow-up | Late Complications/Outcome | Other Late Effects |
|---|---|---|---|---|---|---|
| 1.M | 5 m | 10 m | POSTEXT* III | 10 y | Biliary complications—retransplantation two years later, 3rd transplantation within next 1 month due to primary poor function of the graft. During the next eight years several percutaneous transvascular balloon dilatations and stenting of the hepatic vein to inferior caval vein anastomosis were performed. Died of complications of idiopathic thrombocytopenia—10 years from diagnosis. | Brock 3 hearing impairment-hearing aids Acquired idiopathic thrombocytopenia |
| 2.M | 2 y | 2 y 4 m | POSTEXT IV | 16 y | None | None |
| 3.F | 7 m | 1 y | POSTEXT III | 13 y | None | Underweight BMI-16 |
| 4.F | 1 y 4 m | 1 y10 m | POSTEXT IV | 14 y | Eight years from transplantation-hypersplenism due to portal vein thrombosis, treated successfully with partial splenic embolization. | Hypertension |
| 5.M | 14 y | 14.5 y | POSTEXT IV | 20 y | None | Hypertension, proteinuria |
| 6.M | 1 y 7 m | 1 y 9 m | 7 y | None | Underweight BMI-16 | |
| 7.M | 11 m | 1 y 2 m | POSTEXT IV | 6 y | None | None |
| 8.M | 3 y 10 | 4 y | POSTEXT IV | 9 y | Late biliary anastomotic stenosis which was treated successfully with percutaneous transhepatic balloon dilatation | Underweight BMI 13, height <3 percentile Brock 3 hearing impairment-hearing aids |
| 9.M | 1 m | 4 y | biliary cirrhosis four years from the primary resection of large volume tumor | 6 y | 1.5 years after transplantation-thrombocytopenia treated successfully with steroid pulses and rituximab. Single percutaneous balloon dilatation of portal vein anastomosis. | BMI 16, height <3 percentile |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dembowska-Bagińska, B.; Więckowska, J.; Brożyna, A.; Święszkowska, E.; Ismail, H.; Broniszczak-Czyszek, D.; Stefanowicz, M.; Grajkowska, W.; Kaliciński, P. Health Status in Long-Term Survivors of Hepatoblastoma. Cancers 2019, 11, 1777. https://doi.org/10.3390/cancers11111777
Dembowska-Bagińska B, Więckowska J, Brożyna A, Święszkowska E, Ismail H, Broniszczak-Czyszek D, Stefanowicz M, Grajkowska W, Kaliciński P. Health Status in Long-Term Survivors of Hepatoblastoma. Cancers. 2019; 11(11):1777. https://doi.org/10.3390/cancers11111777
Chicago/Turabian StyleDembowska-Bagińska, Bożenna, Jolanta Więckowska, Agnieszka Brożyna, Ewa Święszkowska, Hor Ismail, Dorota Broniszczak-Czyszek, Marek Stefanowicz, Wiesława Grajkowska, and Piotr Kaliciński. 2019. "Health Status in Long-Term Survivors of Hepatoblastoma" Cancers 11, no. 11: 1777. https://doi.org/10.3390/cancers11111777
APA StyleDembowska-Bagińska, B., Więckowska, J., Brożyna, A., Święszkowska, E., Ismail, H., Broniszczak-Czyszek, D., Stefanowicz, M., Grajkowska, W., & Kaliciński, P. (2019). Health Status in Long-Term Survivors of Hepatoblastoma. Cancers, 11(11), 1777. https://doi.org/10.3390/cancers11111777