A Pan-Cancer Approach to Predict Responsiveness to Immune Checkpoint Inhibitors by Machine Learning

 , , ,
, , , 
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Datasets
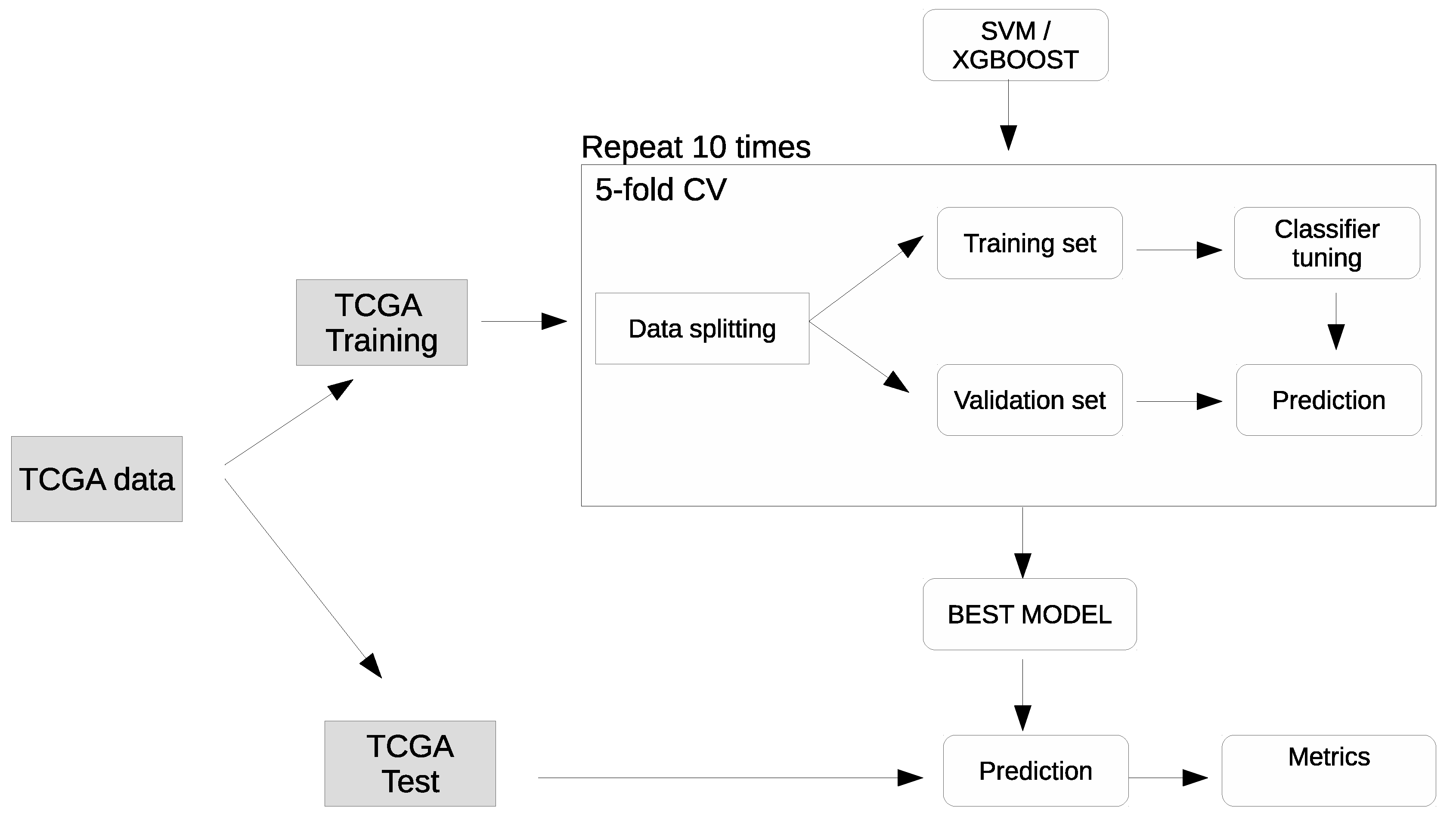
4.2. Machine learning methods
4.3. Computational Details
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ICI | immune checkpoint inhibitors |
| TCGA | The Cancer Genome Atlas |
| XGboost | Extreme distributed gradient boosting library |
| SVM | Support Vector Machine |
| TMB | Tumor Mutational Burden |
| CI | confidence intervals |
| HR | Hazard ratio |
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cancer Types | Label | Number of Samples | HR | 95% CI for HR | p Value |
|---|---|---|---|---|---|
| UVM | TMB/TGF- score positive | n = 80 | 0.3 | 0.04–2.2 | 0.24 |
| SKCM | TMB/TGF- score positive | n = 103 | 0.45 | 0.11–2 | 0.29 |
| GBM | TMB/TGF- score positive | n = 146 | 0.69 | 0.28–1.7 | 0.42 |
| LIHC | TMB/TGF- score positive | n = 349 | 1 | 0.59–1.8 | 0.91 |
| SARC | TMB/TGF- score positive | n = 201 | 0.85 | 0.41–1.8 | 0.66 |
| PCPG | TMB/TGF- score positive | n = 177 | 4.9 | 0.8–30 | 0.085 |
| TCGT | TMB/TGF- score positive | n = 127 | 1.5 | 0.89–2.6 | 0.12 |
| THCA | TMB/TGF- score positive | n = 481 | 0.87 | 0.11–6.7 | 0.89 |
| PAAD | TMB/TGF- score positive | n = 146 | 1 | 0.53–1.9 | 0.96 |
| PRAD | TMB/TGF- score positive | n = 410 | 3 | 0.74–12 | 0.12 |
| UCEC | TMB/TGF- score positive | n = 542 | 0.25 | 0.092–0.69 | 0.007 |
| CHOL | TMB/TGF- score positive | n = 35 | 2.2 | 0.69–7 | 0.18 |
| KICH | TMB/TGF- score positive | n = 64 | 6.4 | 1.6–26 | 0.0091 |
| BLCA | TMB/TGF- score positive | n = 412 | 0.67 | 0.42–1.1 | 0.096 |
| KIRP | TMB/TGF- score positive | n = 266 | 0.27 | 0.064–1.1 | 0.071 |
| HNSC | TMB/TGF- score positive | n = 488 | 1.1 | 0.8–1.6 | 0.48 |
| CESC | TMB/TGF- score positive | n = 282 | 0.48 | 0.19–1.2 | 0.11 |
| BRCA | TMB/TGF- score positive | n = 1009 | 0.94 | 0.57–1.6 | 0.81 |
| OV | TMB/TGF- score positive | n = 164 | 0.67 | 0.31–1.4 | 0.31 |
| LGG | TMB/TGF- score positive | n = 499 | 0.87 | 0.38–2 | 0.74 |
| LUAD | TMB/TGF- score positive | n = 492 | 0.58 | 0.33–1 | 0.05 |
| ESCA | TMB/TGF- score positive | n = 151 | 1.3 | 0.65–2.7 | 0.45 |
| READ | TMB/TGF- score positive | n = 125 | 0.86 | 0.19–3.9 | 0.85 |
| LUSC | TMB/TGF- score positive | n = 484 | 0.79 | 0.52–1.2 | 0.28 |
| COAD | TMB/TGF- score positive | n = 462 | 0.73 | 0.39–1.4 | 0.33 |
| UCS | TMB/TGF- score positive | n = 56 | 1.1 | 0.4–3.3 | 0.8 |
| MESO | TMB/TGF- score positive | n = 76 | 0.5 | 0.21–1.2 | 0.11 |
| ACC | TMB/TGF- score positive | n = 78 | 6.4 | 2.3–18 | 4 |
| STAD | TMB/TGF- score positive | n = 345 | 0.62 | 0.35–1.1 | 0.088 |
| Cluster Subtype | TMB/TGF- Score Negative | TMB/TGF- Score Positive | Total |
|---|---|---|---|
| 1 | 1957 | 266 | 2223 |
| 2 | 1994 | 379 | 2373 |
| 3 | 1704 | 166 | 1870 |
| 4 | 913 | 150 | 1063 |
| 5 | 334 | 36 | 370 |
| 6 | 149 | 7 | 156 |




References
- Friedrich, M.; Jasinski-Bergner, S.; Lazaridou, M.F.; Subbarayan, K.; Massa, C.; Tretbar, S.; Mueller, A.; Handke, D.; Biehl, K.; Bukur, J.; et al. Tumor-induced escape mechanisms and their association with resistance to checkpoint inhibitor therapy. Cancer Immunol. Immunother. 2019, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Costantini, A.; Takam Kamga, P.; Dumenil, C.; Chinet, T.; Emile, J.F.; Giroux Leprieur, E. Plasma Biomarkers and Immune Checkpoint Inhibitors in Non-Small Cell Lung Cancer: New Tools for Better Patient Selection? Cancers 2019, 11, 1269. [Google Scholar] [CrossRef] [PubMed]
- Havel, J.J.; Chowell, D.; Chan, T.A. The evolving landscape of biomarkers for checkpoint inhibitor immunotherapy. Nat. Rev. Cancer 2019, 19, 133. [Google Scholar] [CrossRef] [PubMed]
- Darvin, P.; Toor, S.M.; Sasidharan Nair, V.; Elkord, E. Immune checkpoint inhibitors: Recent progress and potential biomarkers. Exp. Mol. Med. 2018, 50, 165. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, M. Correlate tumor mutation burden with immune signatures in human cancers. BMC Immunol. 2019, 20, 4. [Google Scholar] [CrossRef]
- Prat, A.; Navarro, A.; Paré, L.; Reguart, N.; Galván, P.; Pascual, T.; Martínez, A.; Nuciforo, P.; Comerma, L.; Alos, L.; et al. Immune-Related Gene Expression Profiling After PD-1 Blockade in Non-Small Cell Lung Carcinoma, Head and Neck Squamous Cell Carcinoma, and Melanoma. Cancer Res. 2017, 77, 3540–3550. [Google Scholar] [CrossRef]
- Zhang, L.; Jones-O’Connor, M.; Awadalla, M.; Zlotoff, D.A.; Thavendiranathan, P.; Groarke, J.D.; Villani, A.C.; Lyon, A.R.; Neilan, T.G. Cardiotoxicity of Immune Checkpoint Inhibitors. Curr. Treat. Options Cardiovasc. Med. 2019, 21, 32. [Google Scholar] [CrossRef]
- Maleki Vareki, S. High and low mutational burden tumors versus immunologically hot and cold tumors and response to immune checkpoint inhibitors. J. Immunother. Cancer 2018, 6, 157. [Google Scholar] [CrossRef]
- Buchbinder, E.I.; Desai, A. CTLA-4 and PD-1 Pathways: Similarities, Differences, and Implications of Their Inhibition. Am. J. Clin. Oncol. 2016, 39, 98–106. [Google Scholar] [CrossRef]
- Lawrence, M.S.; Stojanov, P.; Polak, P.; Kryukov, G.V.; Cibulskis, K.; Sivachenko, A.; Carter, S.L.; Stewart, C.; Mermel, C.H.; Roberts, S.A.; et al. Mutational heterogeneity in cancer and the search for new cancer-associated genes. Nature 2013, 499, 214–218. [Google Scholar] [CrossRef]
- Li, B.; Li, T.; Pignon, J.C.; Wang, B.; Wang, J.; Shukla, S.A.; Dou, R.; Chen, Q.; Hodi, F.S.; Choueiri, T.K.; et al. Landscape of tumor-infiltrating T cell repertoire of human cancers. Nat. Genet. 2016, 48, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Schulz, M.; Salamero-Boix, A.; Niesel, K.; Alekseeva, T.; Sevenich, L. Microenvironmental Regulation of Tumor Progression and Therapeutic Response in Brain Metastasis. Front. Immunol. 2019, 10, 1713. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.S.; Mellman, I. Elements of cancer immunity and the cancer-immune set point. Nature 2017, 541, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Hu-Lieskovan, S.; Wargo, J.A.; Ribas, A. Primary, Adaptive, and Acquired Resistance to Cancer Immunotherapy. Cell 2017, 168, 707–723. [Google Scholar] [CrossRef] [PubMed]
- Khong, H.T.; Restifo, N.P. Natural selection of tumor variants in the generation of “tumor escape” phenotypes. Nat. Immunol. 2002, 3, 999–1005. [Google Scholar] [CrossRef]
- Kather, J.N.; Suarez-Carmona, M.; Charoentong, P.; Weis, C.A.; Hirsch, D.; Bankhead, P.; Horning, M.; Ferber, D.; Kel, I.; Herpel, E.; et al. Topography of cancer-associated immune cells in human solid tumors. eLife 2018, 7, e36967. [Google Scholar] [CrossRef]
- Thorsson, V.; Gibbs, D.L.; Brown, S.D.; Wolf, D.; Bortone, D.S.; Yang, T.H.O.; Porta-Pardo, E.; Gao, G.; Plaisier, C.L.; Eddy, J.A.; et al. The Immune Landscape of Cancer. Immunity 2018, 48, 812–830.e14. [Google Scholar] [CrossRef]
- Şenbabaoğlu, Y.; Gejman, R.S.; Winer, A.G.; Liu, M.; Van Allen, E.M.; de Velasco, G.; Miao, D.; Ostrovnaya, I.; Drill, E.; Luna, A.; et al. Tumor immune microenvironment characterization in clear cell renal cell carcinoma identifies prognostic and immunotherapeutically relevant messenger RNA signatures. Genome Biol. 2016, 17, 231. [Google Scholar] [CrossRef]
- Danaher, P.; Warren, S.; Lu, R.; Samayoa, J.; Sullivan, A.; Pekker, I.; Wallden, B.; Marincola, F.M.; Cesano, A. Pan-cancer adaptive immune resistance as defined by the Tumor Inflammation Signature (TIS): Results from The Cancer Genome Atlas (TCGA). J. Immunother. Cancer 2018, 6, 63. [Google Scholar] [CrossRef]
- Mariathasan, S.; Turley, S.J.; Nickles, D.; Castiglioni, A.; Yuen, K.; Wang, Y.; Kadel, E.E., III; Koeppen, H.; Astarita, J.L.; Cubas, R.; et al. TGFB attenuates tumour response to PD-L1 blockade by contributing to exclusion of T cells. Nature 2018, 554, 544–548. [Google Scholar] [CrossRef]
- Charoentong, P.; Finotello, F.; Angelova, M.; Mayer, C.; Efremova, M.; Rieder, D.; Hackl, H.; Trajanoski, Z. Pan-cancer Immunogenomic Analyses Reveal Genotype-Immunophenotype Relationships and Predictors of Response to Checkpoint Blockade. Cell Rep. 2017, 18, 248–262. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Lichtenberg, T.; Hoadley, K.A.; Poisson, L.M.; Lazar, A.J.; Cherniack, A.D.; Kovatich, A.J.; Benz, C.C.; Levine, D.A.; Lee, A.V.; et al. An Integrated TCGA Pan-Cancer Clinical Data Resource to Drive High-Quality Survival Outcome Analytics. Cell 2018, 173, 400–416.e11. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, D.L. An R package for classification of immune subtypes, in cancer, using gene expression data. 2019; original-date: 2019-05-21T16:04:14Z. [Google Scholar]
- Hastie, T.; Tibshirani, R.; Friedman, J. The Elements of Statistical Learning: Data Mining, Inference, and Prediction; Springer: New York, NY, USA, 2001. [Google Scholar]
- Matthews, B.W. Comparison of the predicted and observed secondary structure of T4 phage lysozyme. Biochim. Biophys. Acta 1975, 405, 442–451. [Google Scholar] [CrossRef]
- Jurman, G.; Riccadonna, S.; Furlanello, C. A comparison of MCC and CEN error measures in multi-class prediction. PLoS ONE 2012, 7, e41882. [Google Scholar] [CrossRef] [PubMed]
- Bonotto, M.; Garattini, S.K.; Basile, D.; Ongaro, E.; Fanotto, V.; Cattaneo, M.; Cortiula, F.; Iacono, D.; Cardellino, G.G.; Pella, N.; et al. Immunotherapy for gastric cancers: Emerging role and future perspectives. Expert Rev. Clin. Pharmacol. 2017, 10, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Visconti, R.; Morra, F.; Guggino, G.; Celetti, A. The between Now and Then of Lung Cancer Chemotherapy and Immunotherapy. Int. J. Mol. Sci. 2017, 18, 1374. [Google Scholar] [CrossRef] [PubMed]
- Emens, L.A. Breast Cancer Immunotherapy: Facts and Hopes. Clin. Cancer Res. 2018, 24, 511–520. [Google Scholar] [CrossRef]
- Basile, D.; Garattini, S.K.; Bonotto, M.; Ongaro, E.; Casagrande, M.; Cattaneo, M.; Fanotto, V.; De Carlo, E.; Loupakis, F.; Urbano, F.; et al. Immunotherapy for colorectal cancer: Where are we heading? Expert Opin. Biol. Ther. 2017, 17, 709–721. [Google Scholar] [CrossRef]
- Cattrini, C.; Dellepiane, C.; Cavo, A.; Buzzatti, G.; Tolomeo, F.; Messina, C.; Boccardo, F. Immunotherapy for genitourinary cancer: State of the art and new perspectives. Anticancer Drugs 2016, 27, 585–599. [Google Scholar] [CrossRef]
- Angelova, M.; Charoentong, P.; Hackl, H.; Fischer, M.L.; Snajder, R.; Krogsdam, A.M.; Waldner, M.J.; Bindea, G.; Mlecnik, B.; Galon, J.; et al. Characterization of the immunophenotypes and antigenomes of colorectal cancers reveals distinct tumor escape mechanisms and novel targets for immunotherapy. Genome Biol. 2015, 16, 64. [Google Scholar] [CrossRef]
- Tamborero, D.; Rubio-Perez, C.; Muiños, F.; Sabarinathan, R.; Piulats, J.M.; Muntasell, A.; Dienstmann, R.; Lopez-Bigas, N.; Gonzalez-Perez, A. A Pan-cancer Landscape of Interactions between Solid Tumors and Infiltrating Immune Cell Populations. Clin. Cancer Res. 2018, 24, 3717–3728. [Google Scholar] [CrossRef]
- McGranahan, N.; Furness, A.J.S.; Rosenthal, R.; Ramskov, S.; Lyngaa, R.; Saini, S.K.; Jamal-Hanjani, M.; Wilson, G.A.; Birkbak, N.J.; Hiley, C.T.; et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science 2016, 351, 1463–1469. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Gilligan, B.M.; Yuan, J.; Li, T. Current status and perspectives in translational biomarker research for PD-1/PD-L1 immune checkpoint blockade therapy. J. Hematol. Oncol. 2016, 9, 47. [Google Scholar] [CrossRef] [PubMed]
- Meléndez, B.; Van Campenhout, C.; Rorive, S.; Remmelink, M.; Salmon, I.; D’Haene, N. Methods of measurement for tumor mutational burden in tumor tissue. Transl. Lung Cancer Res. 2018, 7, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, Z.R.; Connelly, C.F.; Fabrizio, D.; Gay, L.; Ali, S.M.; Ennis, R.; Schrock, A.; Campbell, B.; Shlien, A.; Chmielecki, J.; et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med. 2017, 9, 34. [Google Scholar] [CrossRef] [PubMed]
- Martin, T.M.; Davis, S.R. GenomicDataCommons R-Package | NCI Genomic Data Commons Access 2019. Available online: https://bioconductor.org/packages/GenomicDataCommons,http://github.com/Bioconductor/GenomicDataCommons (accessed on 31 May 2018).
- Ellrott, K.; Bailey, M.H.; Saksena, G.; Covington, K.R.; Kandoth, C.; Stewart, C.; Hess, J.; Ma, S.; Chiotti, K.E.; McLellan, M.; et al. Scalable Open Science Approach for Mutation Calling of Tumor Exomes Using Multiple Genomic Pipelines. Cell Syst. 2018, 6, 271–281.e7. [Google Scholar] [CrossRef]
- Alexandrov, L.B.; Nik-Zainal, S.; Wedge, D.C.; Aparicio, S.A.J.R.; Behjati, S.; Biankin, A.V.; Bignell, G.R.; Bolli, N.; Borg, A.; Børresen-Dale, A.L.; et al. Signatures of mutational processes in human cancer. Nature 2013, 500, 415–421. [Google Scholar] [CrossRef]
- Gibbs, D.L. This Repo Contains the Code Necessary to Reproduce the Clusters Found in “The Immune Landscape of Cancer”. Available online: https://github.com/Gibbsdavidl/Immune-Subtype-Clustering (accessed on 31 May 2018).
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]


| Cohort | Cancer Type Full Name | Number of Cases | Percentage of TMB/TGF- Score Positive Cases |
|---|---|---|---|
| HNSC | head and neck squamous cell carcinoma | 488 | 15.57 |
| LUSC | lung squamous cell carcinoma | 476 | 14.71 |
| LIHC | liver hepatocellular carcinoma | 350 | 14.29 |
| UCEC | uterine corpus endometrial carcinoma | 511 | 14.29 |
| CESC | cervical squamous cell carcinoma and endocervical adenocarcinoma | 282 | 14.18 |
| BLCA | bladder urothelial carcinoma | 397 | 14.11 |
| STAD | stomach adenocarcinoma | 349 | 13.75 |
| PRAD | prostate adenocarcinoma | 401 | 13.72 |
| KIRP | kidney renal papillary cell carcinoma | 267 | 13.48 |
| BRCA | breast invasive carcinoma | 970 | 13.30 |
| ESCA | esophageal carcinoma | 151 | 13.25 |
| MESO | mesothelioma | 77 | 12.99 |
| SKCM | skin cutaneous melanoma | 103 | 12.62 |
| UCS | uterine carcinosarcoma | 56 | 12.50 |
| UVM | uveal melanoma | 80 | 12.50 |
| READ | rectum adenocarcinoma | 126 | 11.90 |
| THCA | thyroid carcinoma | 481 | 11.85 |
| COAD | colon adenocarcinoma | 383 | 11.75 |
| PAAD | pancreatic adenocarcinoma | 146 | 11.64 |
| CHOL | cholangiocarcinoma | 35 | 11.43 |
| TGCT | testicular germ cell tumors | 143 | 11.19 |
| PCPG | pheochromocytoma and paraganglioma | 177 | 10.73 |
| LUAD | lung adenocarcinoma | 450 | 10.22 |
| SARC | sarcoma | 201 | 9.95 |
| KICH | kidney chromophobe | 64 | 9.38 |
| LGG | brain lower grade glioma | 501 | 7.98 |
| OV | ovarian serous cystadenocarcinoma | 165 | 7.88 |
| ACC | adrenocortical carcinoma | 78 | 7.69 |
| GBM | glioblastoma multiforme | 147 | 4.08 |
| Endpoint | Status | Number of Samples | HR | 95% CI for HR | p Value |
|---|---|---|---|---|---|
| OS | TMB/TGF- score positive | n = 8007 | 0.86 | 0.75–0.98 | 0.01 |
| DSS | TMB/TGF- score positive | n = 7741 | 0.79 | 0.67–0.93 | 0.0056 |
| PFI | TMB/TGF- score positive | n = 8007 | 0.89 | 0.79–0.99 | 0.059 |
| Cluster | Status | Number of Samples | HR | 95% CI for HR | p Value |
|---|---|---|---|---|---|
| Cluster 1 | TMB/TGF- score positive | n = 2200 | 0.82 | 0.64–1 | 0.11 |
| Cluster 2 | TMB/TGF- score positive | n = 2357 | 0.76 | 0.61–0.93 | 0.0095 |
| Cluster 3 | TMB/TGF- score positive | n = 1867 | 0.84 | 0.53–1.3 | 0.48 |
| Cluster 4 | TMB/TGF- score positive | n = 1061 | 0.72 | 0.52–0.99 | 0.044 |
| Cluster 5 | TMB/TGF- score positive | n = 368 | 1.7 | 0.71–3.9 | 0.24 |
| Cluster 6 | TMB/TGF- score positive | n = 154 | 2.7 | 1.1–6.8 | 0.037 |
| Model | ACC (CI) | ACC Test | MCC (CI) | MCC Test |
|---|---|---|---|---|
| SVM | 0.879 (0.878–0.881) | 0.877 | 0.296 (0.287–0306) | 0.271 |
| XGBoost | 0.878 (0.877–0.880) | 0.879 | 0.260 (0.250–0.269) | 0.260 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polano, M.; Chierici, M.; Dal Bo, M.; Gentilini, D.; Di Cintio, F.; Baboci, L.; Gibbs, D.L.; Furlanello, C.; Toffoli, G. A Pan-Cancer Approach to Predict Responsiveness to Immune Checkpoint Inhibitors by Machine Learning. Cancers 2019, 11, 1562. https://doi.org/10.3390/cancers11101562
Polano M, Chierici M, Dal Bo M, Gentilini D, Di Cintio F, Baboci L, Gibbs DL, Furlanello C, Toffoli G. A Pan-Cancer Approach to Predict Responsiveness to Immune Checkpoint Inhibitors by Machine Learning. Cancers. 2019; 11(10):1562. https://doi.org/10.3390/cancers11101562
Chicago/Turabian StylePolano, Maurizio, Marco Chierici, Michele Dal Bo, Davide Gentilini, Federica Di Cintio, Lorena Baboci, David L. Gibbs, Cesare Furlanello, and Giuseppe Toffoli. 2019. "A Pan-Cancer Approach to Predict Responsiveness to Immune Checkpoint Inhibitors by Machine Learning" Cancers 11, no. 10: 1562. https://doi.org/10.3390/cancers11101562
APA StylePolano, M., Chierici, M., Dal Bo, M., Gentilini, D., Di Cintio, F., Baboci, L., Gibbs, D. L., Furlanello, C., & Toffoli, G. (2019). A Pan-Cancer Approach to Predict Responsiveness to Immune Checkpoint Inhibitors by Machine Learning. Cancers, 11(10), 1562. https://doi.org/10.3390/cancers11101562