Macrovascular Networks on Contrast-Enhanced Magnetic Resonance Imaging Improves Survival Prediction in Newly Diagnosed Glioblastoma


 , , ,
, , ,
Abstract
1. Introduction
2. Results
2.1. Determination of the Cutoff for Number of Vessel-Like Structures in Glioblastoma
2.2. Patient Characteristics
2.3. Survival Analysis According the Treatment Received and Macrovascular Network
3. Discussion
4. Material and Methods
4.1. Study Data
4.2. MRI Protocol
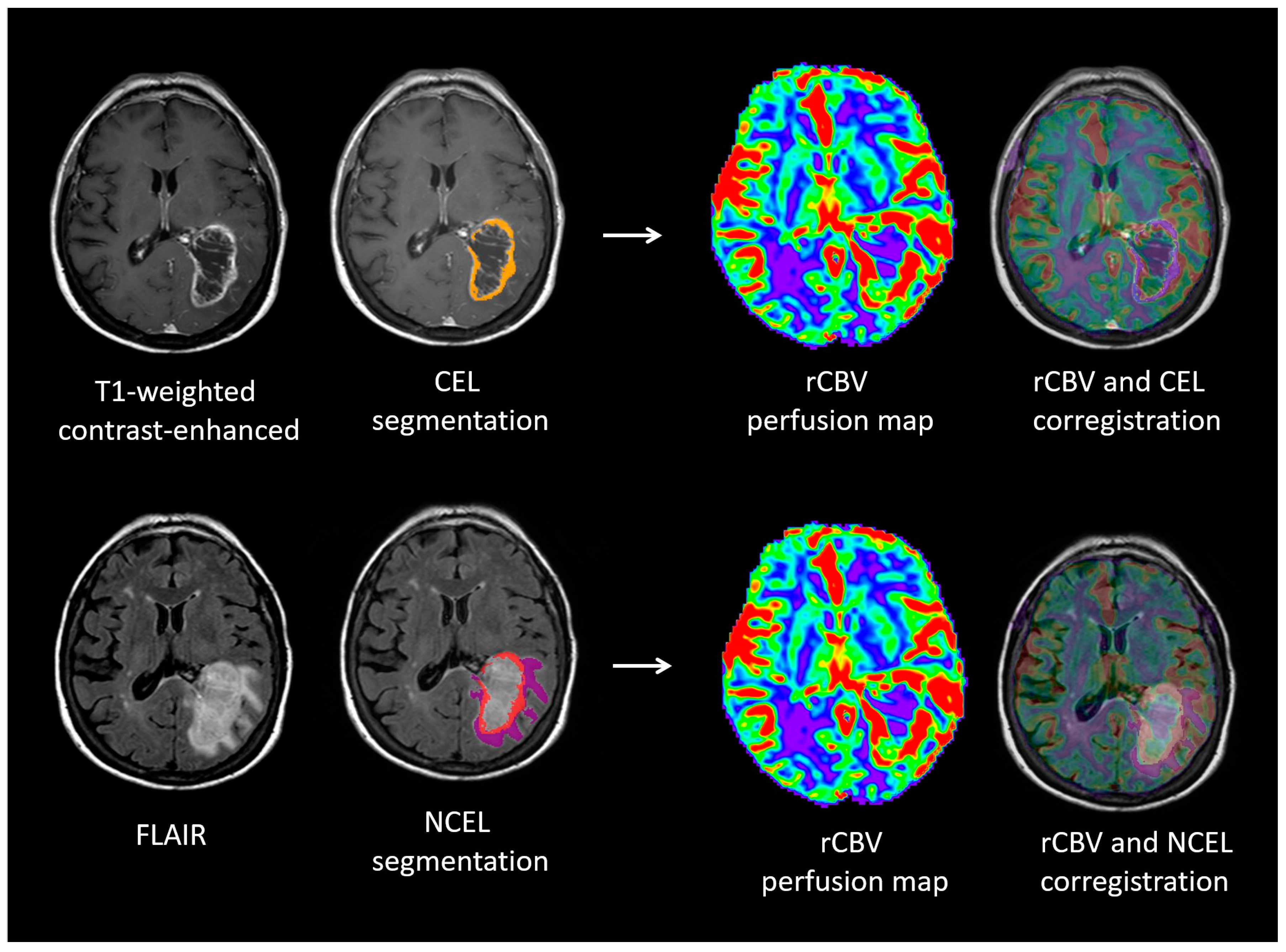
4.3. Quantitative Image Analysis
4.4. Qualitative Image Analysis
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Leon, S.P.; Folkerth, R.D.; Black, P.M. Microvessel density is a prognostic indicator for patients with astroglial brain tumors. Cancer 1996, 77, 362–372. [Google Scholar] [CrossRef]
- Birner, P.; Piribauer, M.; Fischer, I.; Gatterbauer, B.; Marosi, C.; Ambros, P.F.; Ambros, I.M.; Bredel, M.; Oberhuber, G.; Rössler, K.; et al. Vascular patterns in glioblastoma influence clinical outcome and associate with variable expression of angiogenic proteins: Evidence for distinct angiogenic subtypes. Brain Pathol. 2003, 13, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Folkerth, R.D. Descriptive analysis and quantification of angiogenesis in human brain tumors. J. Neurooncol. 2000, 50, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Wesseling, P.; van der Laak, J.A.; Link, M.; Teepen, H.L.; Ruiter, D.J. Quantitative analysis of microvascular changes in diffuse astrocytic neoplasms with increasing grade of malignancy. Hum. Pathol. 1998, 29, 352–358. [Google Scholar] [CrossRef]
- Lund, E.L.; Spang-Thomsen, M.; Skovgaard-Poulsen, H.; Kristjansen, P.E. Tumor angiogenesis—A new therapeutic target in gliomas. Acta Neurol. Scand. 1998, 97, 52–56. [Google Scholar] [CrossRef]
- Zhong, H.; De Marzo, A.M.; Laughner, E.; Lim, M.; Hilton, D.; Zagzag, D.; Buechler, P.; Isaacs, W.B.; Semenza, G.L.; Simons, J.W. Overexpression of hypoxia-inducable factor 1a in common human cancers and their metastases. Cancer Res. 1999, 59, 5830–5835. [Google Scholar] [PubMed]
- Argyriou, A.A.; Giannopoulou, E.; Kalofonos, H.P. Angiogenesis and anti-angiogenic molecularly targeted therapies in malignant gliomas. Oncology 2009, 77, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Griffith, B.; Alotaibi, F.; Zagzag, D.; Fine, H.; Golfinos, J.; Schultz, L. Glioma angiogenesis and perfusion imaging: Understanding relationship between tumor blood volume and leakiness with increasing glioma grade. AJNR Am. J. Neuroradiol. 2015, 36, 2030–2035. [Google Scholar] [CrossRef]
- Sharma, S.; Sharma, M.C.; Sarkar, C. Morphology of angiogenesis in human cancer: A conceptual overview, histoprognostic perspective and significance of neoangiogenesis. Histopathology 2005, 46, 481–489. [Google Scholar] [CrossRef]
- Di Ieva, A. Angioarchitectural morphometrics of brain tumors: Are there any potential histopathological biomarkers? Microvasc. Res. 2010, 80, 522–533. [Google Scholar] [CrossRef] [PubMed]
- Preusser, M.; Heinzl, H.; Gelpi, E.; Schonegger, K.; Haberler, C.; Birner, P.; Marosi, C.; Hegi, M.; Gorlia, T.; Hainfellner, J.A.; European Organization for Research and Treatment of Cancer Brain Tumor Group. Histopathologic assessment of hot-spot microvessel density and vascular patterns in glioblastoma: Poor observer agreement limits clinical utility as prognostic factors: A translational research project of the European Organization for Research and Treatment of Cancer Brain Tumor Group. Cancer 2006, 107, 162–170. [Google Scholar] [PubMed]
- Russell, S.M.; Elliott, R.; Forshaw, D.; Golfinos, J.G.; Nelson, P.K.; Kelly, P.J. Glioma vascularity correlates with reduced patient survival and increased malignancy. Surg. Neurol. 2009, 72, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Kadota, T.; Nakagawa, H.; Kuroda, C. Malignant glioma. Evaluation with 3D time-of-flight MR angiography. Acta Radiol. 1998, 39, 227–232. [Google Scholar] [PubMed]
- Sugahara, T.; Korogi, Y.; Kochi, M.; Ikushima, I.; Hirai, T.; Okuda, T.; Shigematsu, Y.; Liang, L.; Ge, Y.; Ushio, Y.; et al. Correlation of MR imaging determined cerebral blood volume maps with histologic and angiographic determination of vascularity of gliomas. AJR Am. J. Roentgenol. 1998, 171, 1479–1486. [Google Scholar] [CrossRef] [PubMed]
- Wetzel, S.G.; Cha, S.; Law, M.; Johnson, G.; Golfinos, J.; Lee, P.; Nelson, P.K. Preoperative assessment of intracranial tumors with perfusion MR and a volumetric interpolated examination: A comparative study with DSA. AJNR Am. J. Neuroradiol. 2002, 23, 1767–1774. [Google Scholar]
- Puig, J.; Blasco, G.; Daunis-i-Estadella, J.; Alberich-Bayarri, A.; Essig, M.; Jain, R.; Remollo, S.; Hernández, D.; Puigdemont, M.; Sánchez-González, J.; et al. High-resolution blood-pool-contrast-enhanced MR angiography in glioblastoma: Tumor-associated neovascularization as a biomarker for patient survival. A. preliminary study. Neuroradiology 2016, 58, 17–26. [Google Scholar] [CrossRef]
- Aronen, H.; Gazit, I.; Louis, D.; Buchbinder, B.R.; Pardo, F.S.; Weisskoff, R.M.; Harsh, G.R.; Cosgrove, G.R.; Halpern, E.F.; Hochberg, F.H.; et al. Cerebral blood volume maps of gliomas: Comparison with tumor grade and histologic findings. Radiology 1994, 191, 41–51. [Google Scholar] [CrossRef]
- Le Bas, J.F.; Kremer, S.; Grand, S.; Rémy, C.; Le Duc, G.; Tropres, I.; Fonchy, E.; Peoc’h, M.; Szabo de Edelenyi, F.; Estève, F.; et al. NMR perfusion imaging: Applications to the study of brain tumor angiogenesis. Bull. Acad. Natl. Med. 2000, 184, 557–567. [Google Scholar]
- Hirai, T.; Murakami, R.; Nakamura, H.; Kitajima, M.; Fukuoka, H.; Sasao, A.; Akter, M.; Hayashida, Y.; Toya, R.; Oya, N.; et al. Prognostic value of perfusion MR imaging of high-grade astrocytomas: Long-term follow-up study. AJNR Am. J. Neuroradiol. 2008, 29, 1505–1510. [Google Scholar] [CrossRef]
- Jain, R.; Narang, J.; Griffith, B.; Bagher-Ebadian, H.; Scarpace, L.; Mikkelsen, T.; Littenberg, B.; Schultz, L.R. Prognostic vascular imaging biomarkers in high-grade gliomas: Tumor permeability as an adjunct to blood volume estimates. Acad. Radiol. 2013, 20, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Gutierrez, J.; Narang, J.; Scarpace, L.; Schultz, L.; Lemke, N.; Patel, S.C.; Mikkelsen, T.; Rock, J. In vivo correlation of tumor blood volume and permeability with histological and molecular angiogenic markers in gliomas. Am. J. Neuroradiol. 2011, 32, 388–394. [Google Scholar] [CrossRef]
- Mills, S.J.; Patankar, T.A.; Haroon, H.A.; Balériaux, D.; Swindell, R.; Jackson, A. Do cerebral blood volume and contrast transfer coefficient predict prognosis in human glioma? AJNR Am. J. Neuroradiol. 2006, 27, 853–858. [Google Scholar] [PubMed]
- Catalaa, I.; Henry, R.; Dillon, W.P.; Graves, E.E.; McKnight, T.R.; Lu, Y.; Vigneron, D.B.; Nelson, S.J. Perfusion, diffusion and spectroscopy values in newly diagnosed cerebral gliomas. NMR Biomed. 2006, 19, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Jafari-Khouzani, K.; Emblem, K.E.; Kalpathy-Cramer, J.; Bjørnerud, A.; Vangel, M.G.; Gerstner, E.R.; Schmainda, K.M.; Paynabar, K.; Wu, O.; Wen, P.Y.; et al. Repeatability of Cerebral Perfusion Using Dynamic Susceptibility Contrast MRI in Glioblastoma Patients. Transl. Oncol. 2015, 8, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Jia, Z.Z.; Shi, W.; Shi, J.L.; Shen, D.D.; Gu, H.M.; Zhou, X.J. Comparison between perfusion computed tomography and dynamic contrast-enhanced magnetic resonance imaging in assessing glioblastoma microvasculature. Eur. J. Radiol. 2017, 87, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Hammoud, M.A.; Sawaya, R.; Shi, W.; Thall, P.F.; Leeds, N.E. Prognostic significance of preoperative MRI scans in glioblastoma multiforme. J. Neurooncol. 1996, 27, 65–73. [Google Scholar] [CrossRef]
- Zinn, P.O.; Sathyan, P.; Mahajan, B.; Bruyere, J.; Hegi, M.; Majumder, S.; Colen, R.R. A novel volume-age-KPS (VAK) glioblastoma classification identifies a prognostic cognate microRNAgene signature. PLoS ONE 2012, 7, e41522. [Google Scholar] [CrossRef]
- Gutman, D.A.; Cooper, L.A.; Hwang, S.N.; Holder, C.A.; Gao, J.; Aurora, T.D.; Dunn, W.D., Jr.; Scarpace, L.; Mikkelsen, T.; Jain, R.; et al. MR imaging predictors of molecular profile and survival: Multi-institutional study of the TCGA glioblastoma data set. Radiology 2013, 267, 560–569. [Google Scholar] [CrossRef]
- Park, J.K.; Hodges, T.; Arko, L.; Shen, M.; Dello Iacono, D.; McNabb, A.; Olsen Bailey, N.; Kreisl, T.N.; Iwamoto, F.M.; Sul, J.; et al. Scale to predict survival after surgery for recurrent glioblastoma multiforme. J. Clin. Oncol. 2010, 28, 3838–3843. [Google Scholar] [CrossRef]
- Lacroix, M.; Abi-Said, D.; Fourney, D.R.; Gokaslan, Z.L.; Shi, W.; DeMonte, F.; Lang, F.F.; McCutcheon, I.E.; Hassenbusch, S.J.; Holland, E.; et al. A multivariate analysis of 416 patients with glioblastoma multiforme: Prognosis, extent of resection, and survival. J. Neurosurg. 2001, 95, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Pope, W.B.; Sayre, J.; Perlina, A.; Villablanca, J.P.; Mischel, P.S.; Cloughesy, T.F. MR imaging correlates of survival in patients with high-grade gliomas. AJNR Am. J. Neuroradiol. 2005, 26, 2466–2474. [Google Scholar] [PubMed]
- Mazurowski, M.A.; Desjardins, A.; Malof, J.M. Imaging descriptors improve the predictive power of survival models for glioblastoma patients. Neuro Oncol. 2013, 15, 1389–1394. [Google Scholar] [CrossRef] [PubMed]
- Wiki for the VASARI Feature Set the National Cancer Institute Web Site. Available online: https://wiki.cancerimagingarchive.net/display/Public/VASARI+Research+Project (accessed on 2 September 2018).
- Scott, J.G.; Bauchet, L.; Fraum, T.J.; Nayak, L.; Cooper, A.R.; Chao, S.T.; Suh, J.H.; Vogelbaum, M.A.; Peereboom, D.M.; Zouaoui, S.; et al. Recursive partitioning analysis of prognostic factors for glioblastoma patients aged 70 years or older. Cancer 2012, 118, 5595–5600. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.W.; Jee, T.K.; Kong, D.S.; Nam, D.H.; Lee, J.I.; Seol, H.J. Outcome of conventional treatment and prognostic factor in elderly glioblastoma patients. Acta Neurochir. 2014, 156, 641–651. [Google Scholar] [CrossRef] [PubMed]
- Denekamp, J. Angiogenesis, neovascular proliferation and vascular pathophysiology as targets for cancer therapy. Br. J. Radiol. 1993, 66, 181–196. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Liu, H.; Tong, H.; Wang, S.; Yang, Y.; Liu, G.; Zhang, W. Clinical Applications of Contrast-Enhanced Perfusion MRI Techniques in Gliomas: Recent Advances and Current Challenges. Contrast Media Mol. Imaging 2017, 2017, 7064120. [Google Scholar] [CrossRef]
- Jain, R.; Poisson, L.; Narang, J.; Gutman, D.; Scarpace, L.; Hwang, S.N.; Holder, C.; Wintermark, M.; Colen, R.R.; Kirby, J.; et al. Genomic mapping and survival prediction in glioblastoma: Molecular subclassification strengthened by hemodynamic imaging biomarkers. Radiology 2013, 267, 212–220. [Google Scholar] [CrossRef]
- Jain, R.; Poisson, L.M.; Gutman, D.; Scarpace, L.; Hwang, S.N.; Holder, C.A.; Wintermark, M.; Rao, A.; Colen, R.R.; Kirby, J.; et al. Outcome prediction in patients with glioblastoma by using imaging, clinical, and genomic biomarkers: Focus on the nonenhancing component of the tumor. Radiology 2014, 272, 484–493. [Google Scholar] [CrossRef]
- Margiewicz, S.; Cordova, C.; Chi, A.S.; Jain, R. State of the Art Treatment and Surveillance Imaging of Glioblastomas. Semin. Roentgenol. 2018, 53, 23–36. [Google Scholar] [CrossRef]
- Griffith, B.; Jain, R. Perfusion Imaging in Neuro-Oncology: Basic Techniques and Clinical Applications. Magn Reson. Imaging Clin. N. Am. 2016, 24, 765–779. [Google Scholar] [CrossRef] [PubMed]
- Weidner, N. The importance of tumour angiogenesis. The evidence continues to grow. Am. J. Clin. Pathol. 2004, 122, 675–677. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Folkerth, R.D. Histologic measures of angiogenesis in human primary brain tumors. Cancer Treat Res. 2004, 117, 79–95. [Google Scholar] [PubMed]
- Abdulrauf, S.I.; Evardsen, K.; Ho, K.L.; Yang, X.Y.; Rock, J.P.; Rosenblum, M.L. Vascular endothelial growth factor expression and vascular density as prognostic markers of survival in patients with low-grade astrocytoma. J. Neurosurg. 1998, 88, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Jafri, N.F.; Clarke, J.L.; Weinberg, V.; Barani, I.J.; Cha, S. Relationship of glioblastoma multiforme to the subventricular zone is associated with survival. Neuro Oncol. 2013, 15, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Chaichana, K.; Parker, S.; Olivi, A.; Quinones-Hinojosa, A. A proposed classification system that projects outcomes based on preoperative variables for adult patients with glioblastoma multiforme. J. Neurosurg. 2010, 112, 997–1004. [Google Scholar] [CrossRef]
- Adeberg, S.; Bostel, T.; Konig, L.; Welzel, T.; Debus, J.; Combs, S.E. A comparison of long-term survivors and short-term survivors with glioblastoma, subventricular zone involvement: A predictive factor for survival? Radiat Oncol. 2014, 9, 95. [Google Scholar] [CrossRef]
- Takano, S. Glioblastoma angiogenesis: VEGF resistance solutions and new strategies based on molecular mechanisms of tumor vessel formation. Brain Tumor Pathol. 2012, 29, 73–86. [Google Scholar] [CrossRef]
- Friedman, H.S.; Prados, M.D.; Wen, P.Y.; Mikkelsen, T.; Schiff, D.; Abrey, L.E.; Yung, W.K.; Paleologos, N.; Nicholas, M.K.; Jensen, R.; et al. Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J. Clin. Oncol. 2009, 27, 4733–4740. [Google Scholar] [CrossRef]
- Gilbert, M.R.; Dignam, J.J.; Armstrong, T.S.; Wefel, J.S.; Blumenthal, D.T.; Vogelbaum, M.A.; Colman, H.; Chakravarti, A.; Pugh, S.; Won, M.; et al. A randomized trial of bevacizumab for newly diagnosed glioblastoma. N. Engl. J. Med. 2014, 370, 699–708. [Google Scholar] [CrossRef]
- Chinot, O.L.; Wick, W.; Mason, W.; Henriksson, R.; Saran, F.; Nishikawa, R.; Carpentier, A.F.; Hoang-Xuan, K.; Kavan, P.; Cernea, D.; et al. Bevacizumab plus radiotherapy-temozolomide for newly diagnosed glioblastoma. N. Engl. J. Med. 2014, 370, 709–722. [Google Scholar] [CrossRef] [PubMed]
- Wick, W.; Gorlia, T.; Bendszus, M.; Taphoorn, M.; Sahm, F.; Harting, I.; Brandes, A.A.; Taal, W.; Domont, J.; Idbaih, A.; et al. Lomustine and Bevacizumab in Progressive Glioblastoma. N. Engl. J. Med. 2017, 377, 1954–1963. [Google Scholar] [CrossRef] [PubMed]
- Sawlani, R.N.; Raizer, J.; Horowitz, S.W.; Shin, W.; Grimm, S.A.; Chandler, J.P.; Levy, R.; Getch, C.; Carroll, T.J. Glioblastoma: A method for predicting response to antiangiogenic chemotherapy by using MR perfusion imaging—Pilot study. Radiology 2010, 255, 622–628. [Google Scholar] [CrossRef]
- Kickingereder, P.; Wiestler, B.; Burth, S.; Wick, A.; Nowosielski, M.; Heiland, S.; Schlemmer, H.P.; Wick, W.; Bendszus, M.; Radbruch, A. Relative cerebral blood volume is a potential predictive imaging biomarker of bevacizumab efficacy in recurrent glioblastoma. Neuro Oncol. 2015, 17, 1139–1147. [Google Scholar] [CrossRef] [PubMed]
- Puig, J.; Blasco, G.; Essig, M.; Daunis-i-Estadella, J.; Laguillo, G.; Quiles, A.M.; Remollo, S.; Bergmann, K.; Joly, C.; Bernado, L.; et al. Albumin-binding MR blood pool contrast agent improves diagnostic performance in human brain tumour: Comparison of two contrast agents for glioblastoma. Eur. Radiol. 2013, 23, 1093–1101. [Google Scholar] [CrossRef]
- Scott, L.J. Gadobutrol: A review of its use for contrast-enhanced magnetic resonance imaging in adults and children. Clin. Drug Investig. 2013, 33, 303–314. [Google Scholar] [CrossRef]
- Bennett, I.E.; Guo, H.; Kountouri, N.; D’abaco, G.M.; Hovens, C.M.; Moffat, B.A.; Desmond, P.; Drummond, K.; Kaye, A.H.; Morokoff, A.P. Preoperative biomarkers of tumour vascularity are elevated in patients with glioblastoma multiforme. J. Clin. Neurosci. 2015, 22, 1802–1808. [Google Scholar] [CrossRef]
- Korkolopoulou, P.; Patsouris, E.; Kavantzas, N.; Konstantinidou, A.E.; Christodoulou, P.; Thomas-Tsagli, E.; Pananikolaou, A.; Eftychiadis, C.; Pavlopoulos, P.M.; Angelidakis, D.; et al. Prognostic implications of microvessel morphometry in diffuse astrocytic neoplasms. Neuropathol. Appl. Neurobiol. 2002, 28, 57–66. [Google Scholar] [CrossRef]
- Bullitt, E.; Gerig, G.; Pizer, S.M.; Lin, W.; Aylward, S.R. Measuring tortuosity of the intracerebral vasculature from MRA images. IEEE Trans. Med. Imaging 2003, 22, 1163–1171. [Google Scholar] [CrossRef]
- Jain, R.K. Normalizing tumor vasculature with antiangiogenic therapy: A new paradigm for combination therapy. Nat. Med. 2001, 7, 987–989. [Google Scholar] [CrossRef]
- Wardlaw, G.; Wong, R.; Noseworthy, M.D. Identification of intratumour low frequency microvascular components via BOLD signal fractal dimension mapping. Phys. Med. 2008, 24, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Bullitt, E.; Reardon, D.A.; Smith, J.K. A review of micro- and macrovascular analysis in the assessment of tumor-associated vasculature as visualized by MR. Neuroimage 2007, 37, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Di Ieva, A. Fractal analysis of microvascular networks in malignant brain tumors. Clin. Neuropathol. 2012, 31, 342–351. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall (n = 97) | Less Developed Macrovascular Network (n = 44) | Highly Developed Macrovascular Network (n = 53) | p-Value |
|---|---|---|---|---|
| Male (%) | 62 (63.9%) | 66 (68.2%) | 58 (60.4%) | 0.426 |
| Age at diagnosis (years) | 58 (15) | 54 (15) | 61 (12) | 0.026 |
| Karnofsky score | 87.45 (18.23) | 90.20 (7.65) | 85.76 (14.02) | 0.063 |
| VolumeCEL (cm3) | 20.4 (19.12) | 13.55 (10.52) | 26.28 (22.71) | 0.001 |
| VolumeNCEL (cm3) | 50.67 (32.64) | 44.91 (27.6) | 55.62 (36.02) | 0.260 |
| Volume of necrosis (cm3) | 20.37 (21.84) | 21.52 (28.2) | 19.41 (14.86) | 0.310 |
| rCBFCEL | 16.08 (4.92) | 14.31 (4.06) | 18.52 (5.04) | 0.001 |
| rCBFNCEL | 16.45 (4.34) | 15.5 (4.05) | 17.75 (4.49) | 0.118 |
| rCBVCEL | 1.76 (0.93) | 1.66 (1.09) | 1.83 (0.81) | 0.181 |
| rCBVNCEL | 2.08 (1.18) | 1.88 (0.86) | 2.22 (1.37) | 0.361 |
| MTTCEL (s) | 5.74 (1.93) | 5.71 (1.68) | 5.77 (2.12) | 0.938 |
| MTTNCEL (s) | 6.06 (2.23) | 6.14 (2.57) | 6 (2) | 0.898 |
| TTPCEL (s) | 25.99 (8.67) | 25.86 (9.26) | 26.09 (8.38) | 0.667 |
| TTPNCEL (s) | 25.85 (7.12) | 24.67 (5.67) | 26.64 (7.96) | 0.296 |
| DMTCEL (s) | −0.26 (1.21) | −0.38 (1.35) | −0.18 (1.11) | 0.573 |
| DMTNCEL (s) | −0.12 (0.57) | −0.16 (0.51) | −0.1 (0.62) | 0.725 |
| Microvascular permeability, K2CEL | −56.48 (57.21) | −51.75 (67.45) | −59.9 (49.48) | 0.274 |
| Microvascular permeability, K2NCEL | −53.82 (61.23) | −46.25 (83.83) | −59.31 (38.29) | 0.099 |
| ADCCEL (mm2 s−1 × 10−3) | 0.30 (0.07) | 0.30 (0.07) | 0.31 (0.08) | 0.952 |
| ADCNCEL (mm2 s−1 × 10−3) | 0.44 (0.03) | 0.44 (0.03) | 0.44 (0.03) | 0.944 |
| Vessel-like structures (n) | 9.56 (8.11) | 2.75 (1.94) | 15.21 (6.83) | <0.001 |
| Treatment | 0.280 | |||
| Surgery + RT + TMZ (%) | 64 (65.98%) | 33 (34.01%) | 31 (31.96%) | |
| Surgery + RT (%) | 11 (11.34%) | 5 (5.14%) | 6 (6.19%) | |
| RT + TMZ (%) | 14 (14.42%) | 3 (3.08%) | 11 (11.34%) | |
| TMZ (%) | 7 (7.22%) | 3 (3.08%) | 4 (4.11%) | |
| Palliative (%) | 1 (1.03%) | 0 (0%) | 1 (1.03%) |
| Variable | Overall (n = 97) | Less than 1 Year (n = 56) | More than 1 Year (n = 29) | p-Value |
|---|---|---|---|---|
| Male (%) | 62 (63.9%) | 23 (79.3%) | 33 (58.9%) | 0.060 |
| Age at diagnosis (years) | 57.75 (14.43) | 62.07 (12.66) | 50 (15.11) | <0.001 |
| Karnofsky score | 87.45 (18.23) | 82.52 (13.15) | 91.03 (12.66) | 0.084 |
| Highly/less developed macrovascular network | 44/53 | 16/40 | 18/11 | 0.002 |
| CEL (cm3) | 20.4 (19.12) | 22.41 (21.16) | 19.36 (17.04) | 0.421 |
| Non-CEL (cm3) | 50.67 (32.64) | 48.33 (27.55) | 50.73 (40.82) | 1.000 |
| Necrosis (cm3) | 20.37 (21.84) | 17.99 (15.45) | 23.1 (22.48) | 0.647 |
| rCBFCEL | 16.08 (4.92) | 15.95 (4.74) | 15.59 (5.39) | 0.512 |
| rCBFNCEL | 16.45 (4.34) | 16.69 (3.46) | 15.33 (5.94) | 0.463 |
| rCBVCEL | 1.27 (0.73) | 1.42 (0.88) | 1.05 (0.36) | 0.342 |
| rCBVNCEL | 1.54 (0.95) | 1.64 (1.09) | 1.42 (0.73) | 0.763 |
| MTTCEL (s) | 5.74 (1.93) | 5.86 (1.79) | 5.59 (2.29) | 0.424 |
| MTTNCEL (s) | 6.06 (2.23) | 5.79 (1.91) | 6.31 (2.79) | 0.485 |
| TTPCEL (s) | 25.99 (8.67) | 24.55 (5.91) | 28.78 (13.08) | 0.590 |
| TTPNCEL (s) | 25.85 (7.12) | 25.15 (6.13) | 27.02 (9.75) | 0.808 |
| DMTCEL (s) | −0.26 (1.21) | −0.58 (1.2) | 0.46 (1.09) | 0.006 |
| DMTNCEL (s) | −0.12 (0.57) | −0.26 (0.58) | 0.18 (0.47) | 0.010 |
| Microvascular permeability, K2 CEL | −56.48 (57.21) | −64.46 (68.17) | −52.38 (26.57) | 0.730 |
| Microvascular permeability, K2 NCEL | −53.82 (61.23) | −58.03 (68.31) | −48.27 (55.32) | 0.730 |
| ADCCEL (mm2 s−1 × 10−3) | 0.3 (0.07) | 0.3 (0.06) | 0.31 (0.08) | 0.831 |
| ADCNCEL (mm2 s−1 × 10−3) | 0.44 (0.03) | 0.43 (0.03) | 0.45 (0.02) | 0.041 |
| Vessel-like structures (n) | 9.56 (8.11) | 12.46 (8.62) | 6.59 (5.48) | 0.002 |
| Treatment | 0.003 | |||
| Standard treatment (%) | 64 (65.98%) | 28 (28.87%) | 27 (27.84%) | |
| Surgery + RT (%) | 11 (11.34%) | 8 (8.25%) | 1 (1.03%) | |
| RT + TMZ (%) | 14 (14.43%) | 12 (12.36%) | 1 (1.03%) | |
| TMZ (%) | 7 (7.22%) | 7 (7.22%) | 0 (0%) | |
| Palliative (%) | 1 (1.03%) | 1 (1.03%) | 0 (0%) |
| Variable | Area under Curve | Cutoff | Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value | Hazard Ratio (95% CI) | p-Value | Likelihood p (Multivariate) |
|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | |||||||||
| Age at diagnosis | 0.737 | 59.73 | 0.679 | 0.724 | 0.826 | 0.538 | 1.042 (1.022,1.063) | <0.001 | |
| DMTNCEL | 0.697 | −0.50 | 0.267 | 1.000 | 1.000 | 0.405 | 0.444 (0.232,0.852) | 0.015 | |
| Vessel-like structures | 0.709 | 6.94 | 0.696 | 0.621 | 0.780 | 0.514 | 1.029 (0.998,1.061) | 0.033 | |
| Highly developed macrovascular network | 0.667 | Present | 0.714 | 0.621 | 0.784 | 0.529 | 1.254 (0.788,1.998) | 0.029 | |
| Standard treatment | 0.778 | Present | 0.625 | 0.931 | 0.946 | 0.562 | 0.163 (0.092,0.288) | <0.001 | |
| Bivariate Analysis | |||||||||
| Age at diagnosis DMTNCEL | 0.859 | 58 −0.48 | 0.867 | 0.733 | 0.867 | 0.733 | 1.042 (1.014–1.071) 0.560 (0.284–1.105) | 0.002 0.095 | <0.001 |
| Age at diagnosis Standard treatment | 0.850 | 54.8 2.0 | 0.714 | 0.897 | 0.930 | 0.619 | 1.026 (1.005–1.048) 0.213 (0.117–0.388) | <0.001 0.015 | <0.001 |
| Vessel-like structures Standard treatment | 0.864 | 5 Present | 0.768 | 0.897 | 0.935 | 0.667 | 1.017 (0.987–1.048) 0.170 (0.096–0.301) | 0.044 <0.001 | <0.001 |
| Highly developed macrovascular network Standard treatment | 0.850 | - | 0.625 | 0.931 | 0.946 | 0.562 | 1.265 (0.792–2.019) 0.163 (0.092–0.288) | 0.032 <0.001 | <0.001 |
| Trivariate Analysis * | |||||||||
| Age at diagnosis Standard treatment Highly developed macrovascular network | 0.901 | - | 0.833 | 0.933 | 0.962 | 0.737 | 0.604 (0.459–0.796) 0.163 (0.090–0.297) 1.481 (0.909–2.414) | <0.001 <0.001 0.045 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puig, J.; Biarnés, C.; Daunis-i-Estadella, P.; Blasco, G.; Gimeno, A.; Essig, M.; Balaña, C.; Alberich-Bayarri, A.; Jimenez-Pastor, A.; Camacho, E.; et al. Macrovascular Networks on Contrast-Enhanced Magnetic Resonance Imaging Improves Survival Prediction in Newly Diagnosed Glioblastoma. Cancers 2019, 11, 84. https://doi.org/10.3390/cancers11010084
Puig J, Biarnés C, Daunis-i-Estadella P, Blasco G, Gimeno A, Essig M, Balaña C, Alberich-Bayarri A, Jimenez-Pastor A, Camacho E, et al. Macrovascular Networks on Contrast-Enhanced Magnetic Resonance Imaging Improves Survival Prediction in Newly Diagnosed Glioblastoma. Cancers. 2019; 11(1):84. https://doi.org/10.3390/cancers11010084
Chicago/Turabian StylePuig, Josep, Carles Biarnés, Pepus Daunis-i-Estadella, Gerard Blasco, Alfredo Gimeno, Marco Essig, Carme Balaña, Angel Alberich-Bayarri, Ana Jimenez-Pastor, Eduardo Camacho, and et al. 2019. "Macrovascular Networks on Contrast-Enhanced Magnetic Resonance Imaging Improves Survival Prediction in Newly Diagnosed Glioblastoma" Cancers 11, no. 1: 84. https://doi.org/10.3390/cancers11010084
APA StylePuig, J., Biarnés, C., Daunis-i-Estadella, P., Blasco, G., Gimeno, A., Essig, M., Balaña, C., Alberich-Bayarri, A., Jimenez-Pastor, A., Camacho, E., Thio-Henestrosa, S., Capellades, J., Sanchez-Gonzalez, J., Navas-Martí, M., Domenech-Ximenos, B., Del Barco, S., Puigdemont, M., Leiva-Salinas, C., Wintermark, M., ... Pedraza, S. (2019). Macrovascular Networks on Contrast-Enhanced Magnetic Resonance Imaging Improves Survival Prediction in Newly Diagnosed Glioblastoma. Cancers, 11(1), 84. https://doi.org/10.3390/cancers11010084