The Value of Monitoring the Behavior of Circulating Tumor Cells at the End of Endocrine Therapy in Breast Cancer Patients


Abstract
1. Introduction
2. Results
3. Discussion
4. Methods and Patients
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Anampa, J.; Makower, D.; Sparano, J.A. Progress in adjuvant chemotherapy for breast cancer: An overview. BMC Med. 2015, 13. [Google Scholar] [CrossRef] [PubMed]
- Gnant, M.; Steger, G.G. Fighting overtreatment in adjuvant breast cancer therapy. Lancet 2009, 374, 2029–2030. [Google Scholar] [CrossRef]
- Cardoso, F.; van’t Veer, L.J.; Bogaerts, J.; Slaets, L.; Viale, G.; Delaloge, S.; Pierga, J.-Y.; Brain, E.; Causeret, S.; DeLorenzi, M.; et al. 70-Gene Signature as an Aid to Treatment Decisions in Early-Stage Breast Cancer. N. Engl. J. Med. 2016, 375, 717–729. [Google Scholar] [CrossRef] [PubMed]
- Shak, S.; Petkov, V.; Miller, D.P.; Howlader, N.; Gliner, N.; Howe, W.; Schussler, N.C.; Cronin, K.; Baehner, F.L.; Penberthy, L. Breast cancer specific mortality in patients with early-stage hormone receptor–positive invasive breast cancer and oncotype DX recurrence score results in the SEER database. J. Clin. Oncol. 2016, 34, 176. [Google Scholar] [CrossRef]
- IQWiG-Berichte Nr. 457, Biomarkerbasierte Tests zur Entscheidung für Oder Gegen Eine Adjuvante Systemische Chemotherapie Beim Primären Mammakarzinom Abschlussbericht. Stand: 27.10.2016 Auftrag: D14-01 Version: 1.0. Available online: https://www.iqwig.de/de/projekte-ergebnisse/projekte/nichtmedikamentoese-verfahren/d14-01-biomarkerbasierte-tests-zur-entscheidung-fur-oder-gegen-eine-adjuvante-systemische-chemotherapie-beim-primaren-mamma-karzinom.6097.html (accessed on 19 July 2018).
- Carter, H.; Chen, S.; Isik, L.; Tyekucheva, S.; Velculescu, V.E.; Kinzler, K.W.; Vogelstein, B.; Karchin, R. Cancer-Specific High-Throughput Annotation of Somatic Mutations: Computational Prediction of Driver Missense Mutations. Cancer Res. 2009, 69, 6660–6667. [Google Scholar] [CrossRef] [PubMed]
- Jordan, V.C. Tamoxifen Resistance Trumped and Oral Selective Estrogen Receptor Degraders Arrive. Clin. Cancer Res. 2018, 24, 3480–3482. [Google Scholar] [CrossRef] [PubMed]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: Patient-level meta-analysis of randomised trials. Lancet 2011, 378, 771–784. [Google Scholar] [CrossRef]
- Davies, C.; Pan, H.; Godwin, J.; Gray, R.; Arriagada, R.; Raina, V.; Abraham, M.; Alencar, V.H.M.; Badran, A.; Bonfill, X.; et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet 2013, 381, 805–816. [Google Scholar] [CrossRef]
- Gray, R.G.; Rea, D.; Handley, K.; Bowden, S.J.; Perry, P.; Earl, H.M.; Poole, C.J.; Bates, T.; Chetiyawardana, S.; Dewar, J.A.; et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years in 6953 women with early breast cancer. J. Clin. Oncol. 2013, 31, 5. [Google Scholar] [CrossRef]
- Pan, H.; Gray, R.; Braybrooke, J.; Davies, C.; Taylor, C.; McGale, P.; Peto, R.; Pritchard, K.I.; Bergh, J.; Dowsett, M.; et al. 20-Year Risks of Breast-Cancer Recurrence after Stopping Endocrine Therapy at 5 Years. N. Engl. J. Med. 2017, 377, 1836–1846. [Google Scholar] [CrossRef] [PubMed]
- Hahn, E.E.; Tang, T.; Lee, J.S.; Munoz-Plaza, C.E.; Shen, E.; Rowley, B.; Maeda, J.L.; Mosen, D.M.; Ruckdeschel, J.C.; Gould, M.K. Use of posttreatment imaging and biomarkers in survivors of early-stage breast cancer: Inappropriate surveillance or necessary care? Cancer 2016, 122, 908–916. [Google Scholar] [CrossRef] [PubMed]
- Fidler, I.J. The pathogenesis of cancer metastasis: The “seed and soil” hypothesis revisited. Nat. Rev. Cancer 2003, 3, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Pachmann, K.; Camara, O.; Kavallaris, A.; Krauspe, S.; Malarski, N.; Gajda, M.; Kroll, T.; Jörke, C.; Hammer, U.; Altendorf-Hofmann, A.; et al. Monitoring the response of circulating epithelial tumor cells to adjuvant chemotherapy in breast cancer allows detection of patients at risk of early relapse. J. Clin. Oncol. 2008, 26, 1208–1215. [Google Scholar] [CrossRef] [PubMed]
- Jun, Z.; Xiaolong, Q.; Fangfang, L.; Xiaojing, G.; Feng, G.; Li, F. Silencing of syndecan-binding protein enhances the inhibitory effect of tamoxifen and increases cellular sensitivity to estrogen. Cancer Biol. Med. 2018, 15, 29. [Google Scholar] [CrossRef] [PubMed]
- Munz, M.; Baeuerle, P.A.; Gires, O. The Emerging Role of EpCAM in Cancer and Stem Cell Signaling. Cancer Res. 2009, 69, 5627–5629. [Google Scholar] [CrossRef] [PubMed]
- Rolle, A.; Günzel, R.; Pachmann, U.; Willen, B.; Pachmann, K. Increase in number of circulating disseminated epithelial cells after surgery for non-small cell lung cancer monitored by MAINTRAC® is a predictor for relapse: A preliminary report. World J. Surg. Oncol. 2005, 3. [Google Scholar] [CrossRef] [PubMed]
- Camara, O.; Kavallaris, A.; Nöschel, H.; Rengsberger, M.; Jörke, C.; Pachmann, K. Seeding of epithelial cells into circulation during surgery for breast cancer: The fate of malignant and benign mobilized cells. World J. Surg. Oncol. 2006, 4. [Google Scholar] [CrossRef] [PubMed]
- Chambers, A.F.; Naumov, G.N.; Vantyghem, S.A.; Tuck, A.B. Molecular biology of breast cancer metastasis Clinical implications of experimental studies on metastatic inefficiency. Breast Cancer Res. 2000, 2. [Google Scholar] [CrossRef]
- Meng, S.; Tripathy, D.; Frenkel, E.P.; Shete, S.; Naftalis, E.Z.; Huth, J.F.; Beitsch, P.D.; Leitch, M.; Hoover, S.; Euhus, D.; et al. Circulating tumor cells in patients with breast cancer dormancy. Clin. Cancer Res. 2004, 10, 8152–8162. [Google Scholar] [CrossRef] [PubMed]
- Pachmann, K. Longtime Recirculating Tumor Cells in Breast Cancer Patients. Clin. Cancer Res. 2005, 11, 5657–5658. [Google Scholar] [CrossRef] [PubMed]
- Pachmann, K.; Camara, O.; Kohlhase, A.; Rabenstein, C.; Kroll, T.; Runnebaum, I.B.; Hoeffken, K. Assessing the efficacy of targeted therapy using circulating epithelial tumor cells (CETC): The example of SERM therapy monitoring as a unique tool to individualize therapy. J. Cancer Res. Clin. Oncol. 2011, 137, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Pachmann, K.; Clement, J.H.; Schneider, C.-P.; Willen, B.; Camara, O.; Pachmann, U.; Höffken, K. Standardized quantification of circulating peripheral tumor cells from lung and breast cancer. Clin. Chem. Lab. Med. 2005, 43. [Google Scholar] [CrossRef] [PubMed]
- Lee, V.W.; Chiang, T.; Deodhar, S.D. Bioassay for quantitating circulating tumor cells in a syngeneic mouse tumor system. Cancer Res. 1976, 36, 2053–2058. [Google Scholar] [PubMed]
- Camara, O.; Rengsberger, M.; Egbe, A.; Koch, A.; Gajda, M.; Hammer, U.; Jorke, C.; Rabenstein, C.; Untch, M.; Pachmann, K. The relevance of circulating epithelial tumor cells (CETC) for therapy monitoring during neoadjuvant (primary systemic) chemotherapy in breast cancer. Ann. Oncol. 2007, 18, 1484–1492. [Google Scholar] [CrossRef] [PubMed]
- Lobodasch, K.; Fröhlich, F.; Rengsberger, M.; Schubert, R.; Dengler, R.; Pachmann, U.; Pachmann, K. Quantification of circulating tumour cells for the monitoring of adjuvant therapy in breast cancer: An increase in cell number at completion of therapy is a predictor of early relapse. Breast 2007, 16, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Pachmann, K.; Camara, O.; Kroll, T.; Gajda, M.; Gellner, A.K.; Wotschadlo, J.; Runnebaum, I.B. Efficacy control of therapy using circulating epithelial tumor cells (CETC) as “Liquid Biopsy”: Trastuzumab in HER2/neu-positive breast carcinoma. J. Cancer Res. Clin. Oncol. 2011, 137, 1317–1327. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.; Bauer, M.; Wickerham, D.L.; Redmond, C.K.; Fisher, E.R.; Cruz, A.B.; Foster, R.; Gardner, B.; Lerner, H.; Margolese, R.; et al. Relation of number of positive axillary nodes to the prognosis of patients with primary breast cancer. An NSABP update. Cancer 1983, 52, 1551–1557. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Population | ||
| Number of patients Age | 36 31–80 | |
| Relapse | 10 | |
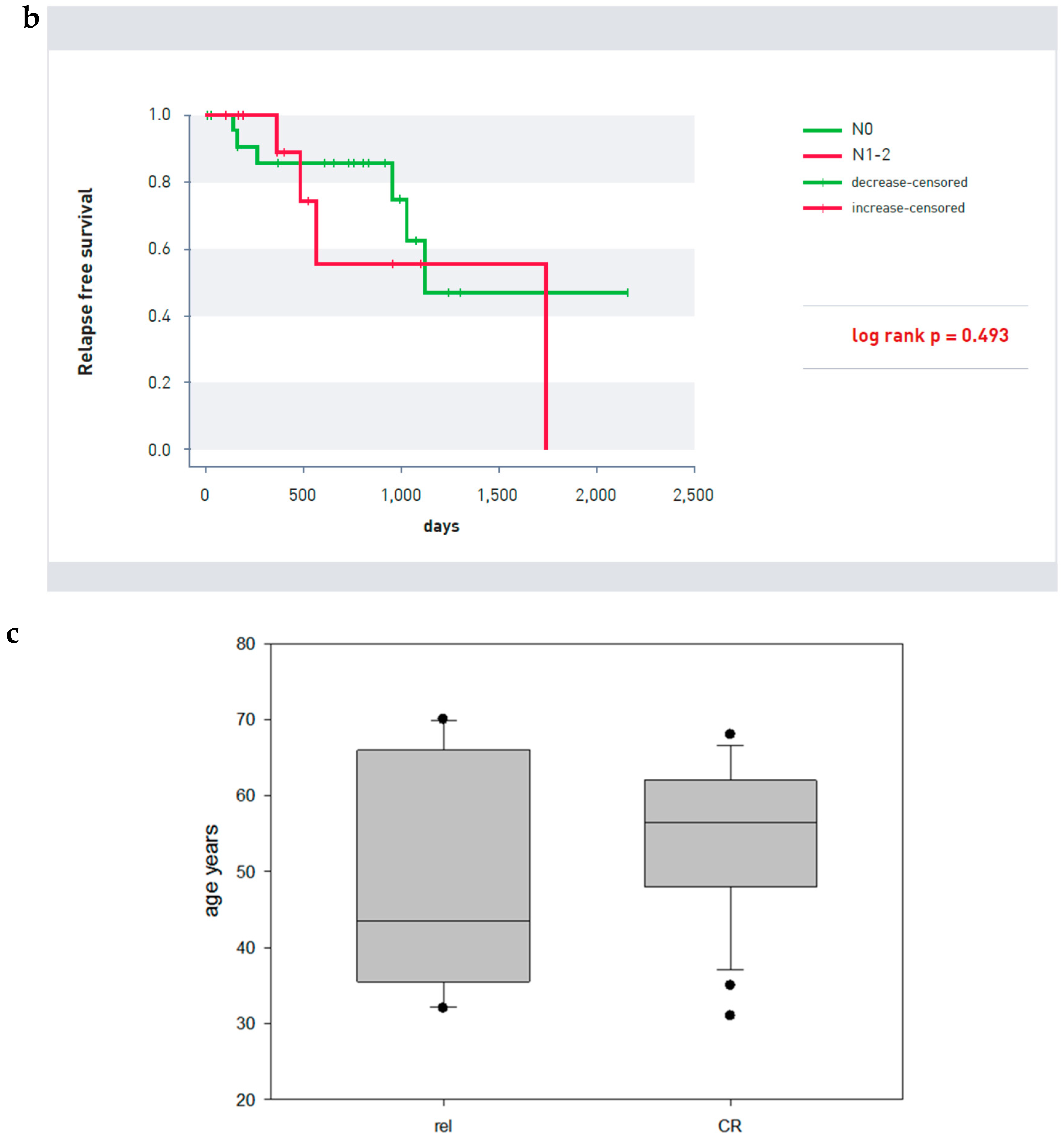
| Mean age patients relapsed | 43 | Ns |
| Mean age patients in complete remission | 56 | |
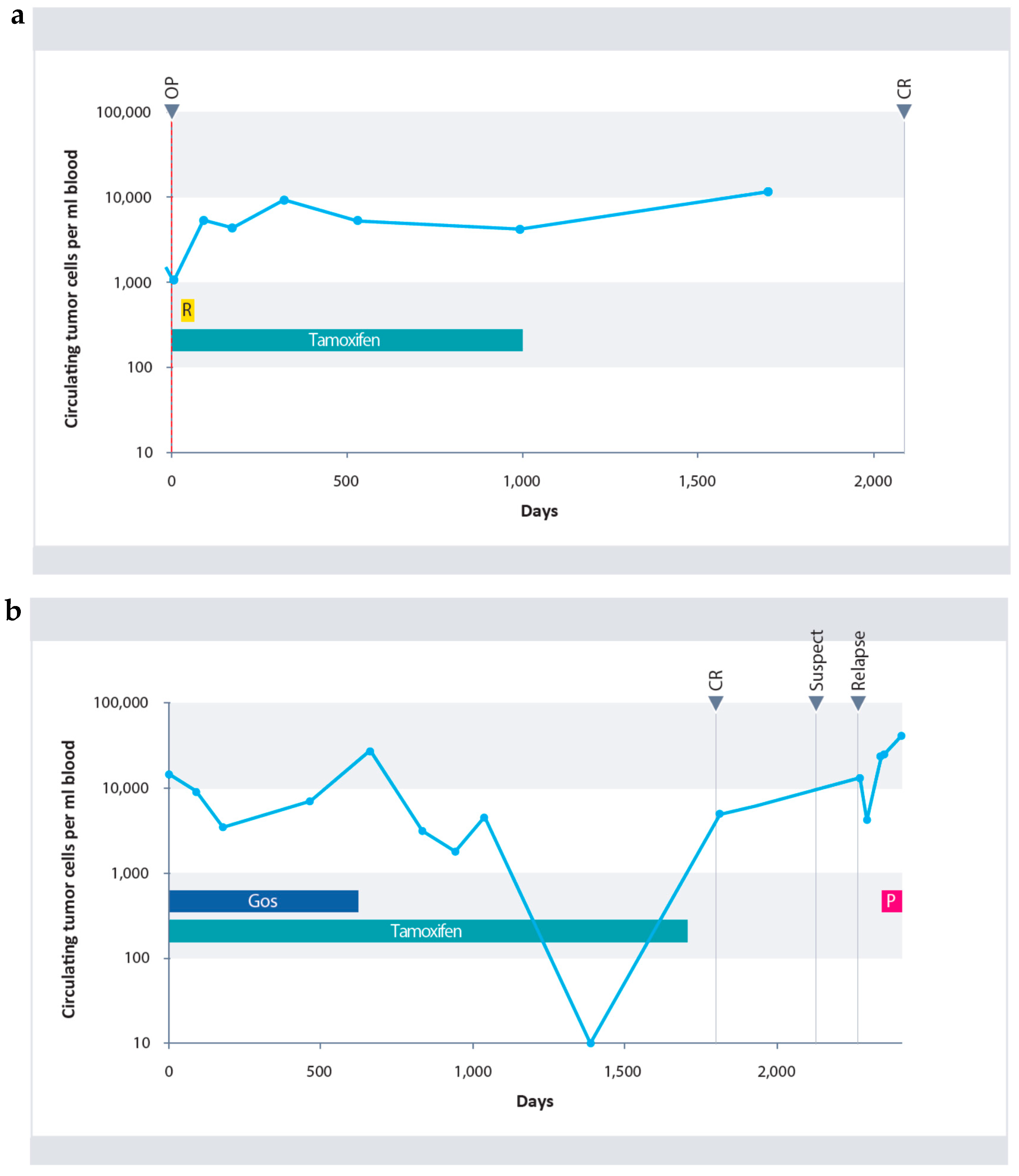
| Observation period after endocrine therapy | 608 days * | |
| Observation period after initial diagnosis | 2281 days * | |
| CETCs | ||
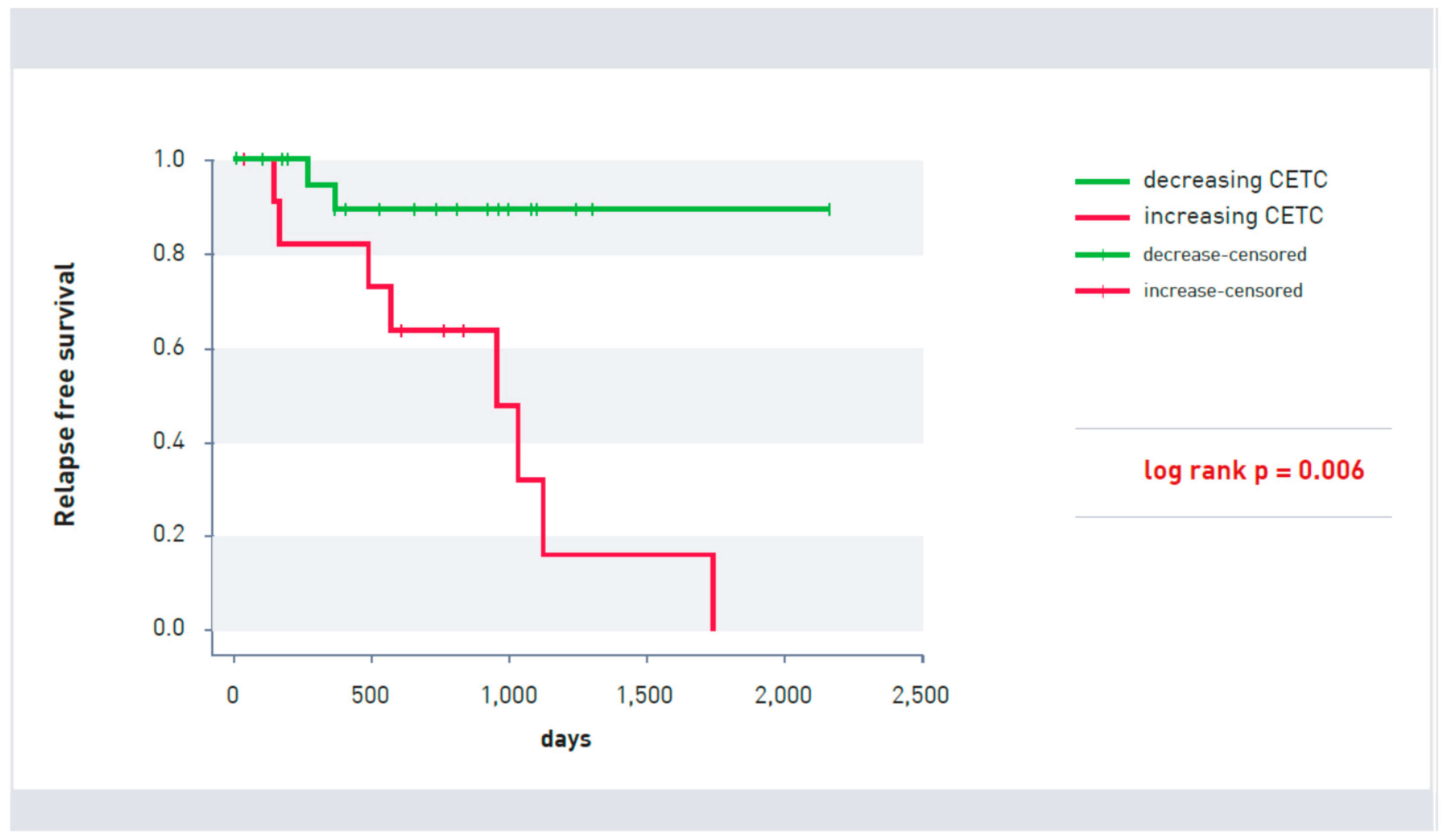
| Increasing | 12 | Rel 8 |
| Decreasing/Constant | 24 | Rel 2 |
| Tumor Size | ||
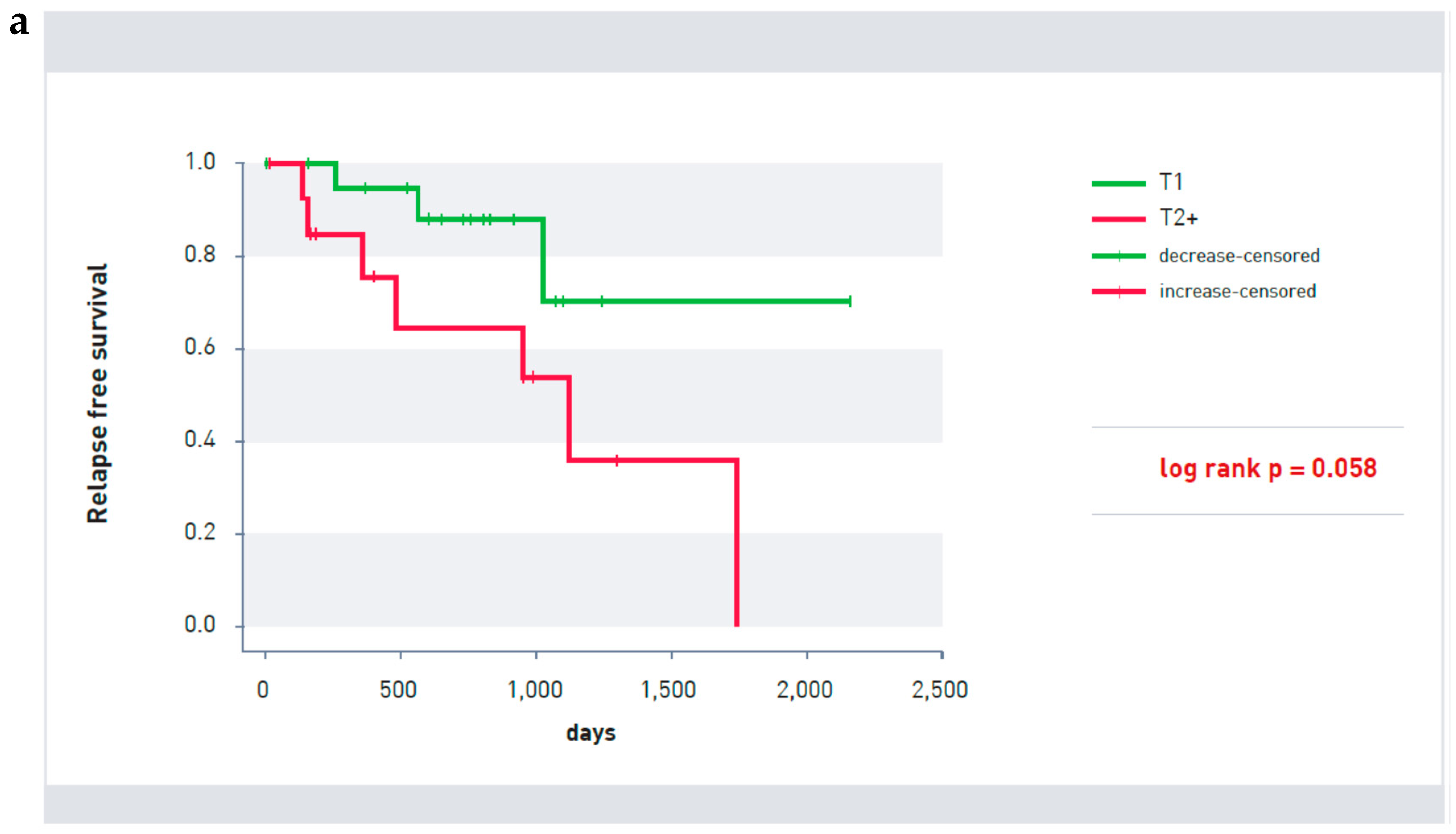
| T1 | 20 | Rel 3 |
| >T2 | 15 | Rel 7 |
| Unknown | 1 | |
| Nodal Status | ||
| N0 | 24 | Rel 6 |
| N1–2 | 12 | Rel 4 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pachmann, K.; Schuster, S. The Value of Monitoring the Behavior of Circulating Tumor Cells at the End of Endocrine Therapy in Breast Cancer Patients. Cancers 2018, 10, 407. https://doi.org/10.3390/cancers10110407
Pachmann K, Schuster S. The Value of Monitoring the Behavior of Circulating Tumor Cells at the End of Endocrine Therapy in Breast Cancer Patients. Cancers. 2018; 10(11):407. https://doi.org/10.3390/cancers10110407
Chicago/Turabian StylePachmann, Katharina, and Stefan Schuster. 2018. "The Value of Monitoring the Behavior of Circulating Tumor Cells at the End of Endocrine Therapy in Breast Cancer Patients" Cancers 10, no. 11: 407. https://doi.org/10.3390/cancers10110407
APA StylePachmann, K., & Schuster, S. (2018). The Value of Monitoring the Behavior of Circulating Tumor Cells at the End of Endocrine Therapy in Breast Cancer Patients. Cancers, 10(11), 407. https://doi.org/10.3390/cancers10110407