1. Introduction
Radiotherapy (RT) for intracranial neoplasms, many of which are benign and/or have good long-term prognosis, is inherently associated with a risk of damaging normal brain parenchyma and causing late toxicities [
1,
2]. The latest effort to deliver highly conformal RT and potentially decrease chronic adverse effects of cerebral irradiation in appropriate patients is manifested by the rapid rise of proton radiotherapy (PRT).
As compared to photons, PRT offers a unique dose deposition known as the Bragg peak, before and beyond which there is only limited dose absorption [
3] in the normal tissue, and therefore only limited effects in non-target tissue. As a result, the major advantage of PRT over photon techniques such as three-dimensional conformal RT (3DCRT) and volumetric-modulated arc therapy (VMAT) is the step dose gradient (fall off) that provides a low dose profile in the entrance and exit path of the particles. Data from multiple tumor sites has demonstrated superior dosimetry with PRT over photon modalities [
4,
5,
6,
7,
8,
9], which is also valid for intracerebral neoplasms [
10,
11].
However, a central question facing radiation oncology is the assessment of which patients will benefit most from PRT. It has been posited by Zietman et al. that PRT may be most advantageous based on the location and anatomic considerations of the tumor with surrounding tissue [
12]. When applied to intracranial malignancies, it is important to consider the location of primary tumors to be irradiated with PRT. Here, dosimetric differences as compared to photon-based techniques vary greatly based on location. For instance, tumors abutting the optic apparatus or the brainstem, especially if dose-escalation is warranted, may show the most striking dosimetric differences between PRT and photons. Conversely, it is likely that tumors that are relatively away from dose-limiting structures may have negligible dosimetric differences.
To this extent, we performed a planning study of patients with intracranial malignancies based on five different locations in order to assess the magnitude of dosimetric differences between PRT and photon-based modalities in each location. Implications of these results include more refined selection of patients receiving PRT, cost-effectiveness, and future clinical toxicity assessment.
2. Results
Each cohort comprised 10 patients for comparison, minus one patient (frontal lobe) for whom a clinically reasonable 3DCRT plan could not be generated. Patient characteristics are depicted in
Table 1. Target coverage was similar for all locations between all three modalities.
Table 2 and
Figure 1 display mean doses to targets and organs-at-risk (OARs) for frontal lobe cases. Most notably, PRT afforded the greatest relative dose reductions in D
mean to the contralateral hippocampus, optic nerve, brainstem, and infratentorial normal brain. This was at the expense of structures with D
mean increases with PRT such as the ipsilateral optic nerve. Most maximum doses were comparable (within ± 10% dose difference of photon techniques) for various OARs.
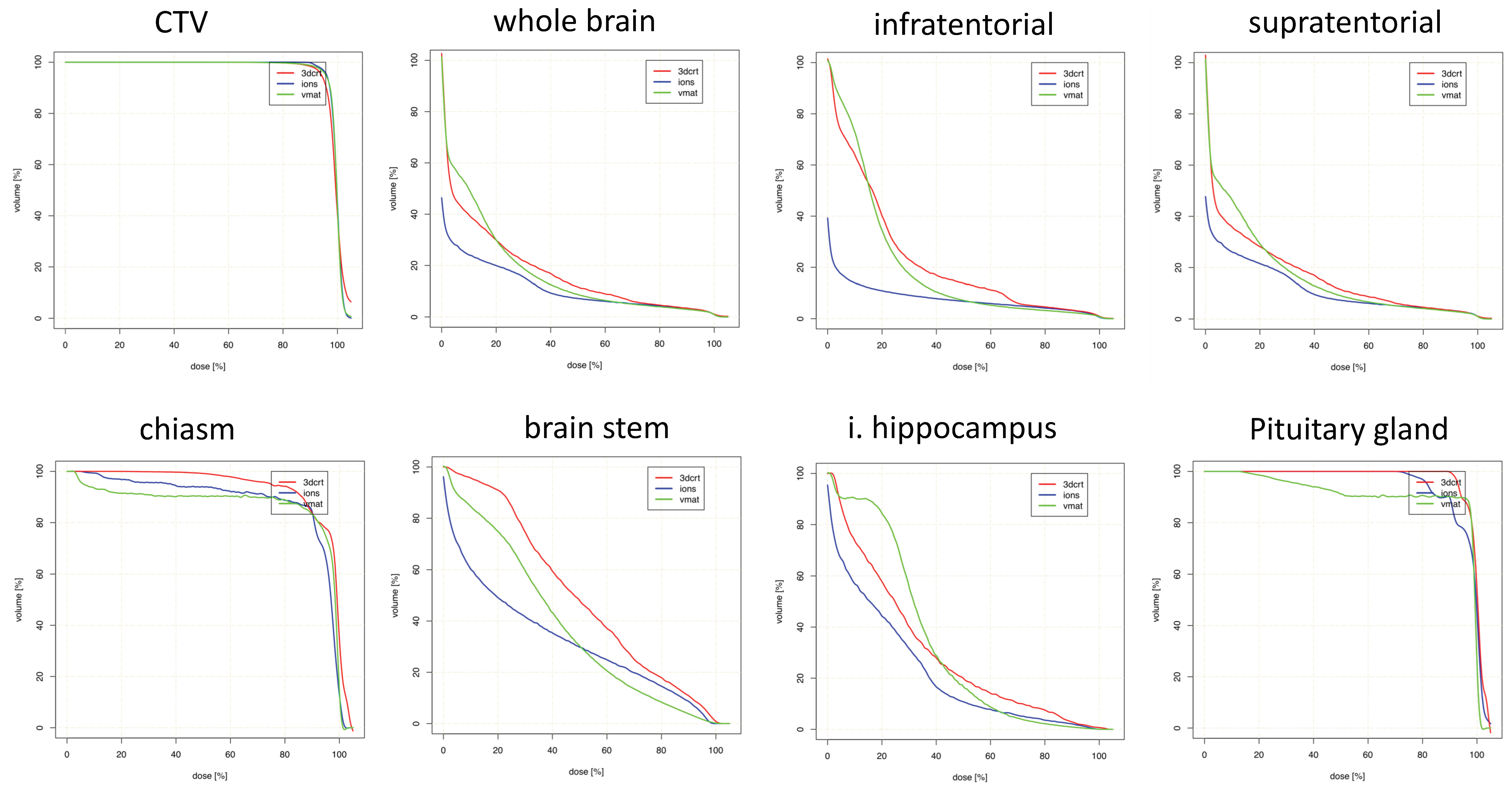
Figures for suprasellar lesions are illustrated in
Table 3 and
Figure 2. Maximum doses were again comparable for most OARs. The greatest D
mean reductions with PRT were observed for whole brain, supratentorial brain and infratentorial brain, with no large dose increases by utilizing PRT.
Table 4 and
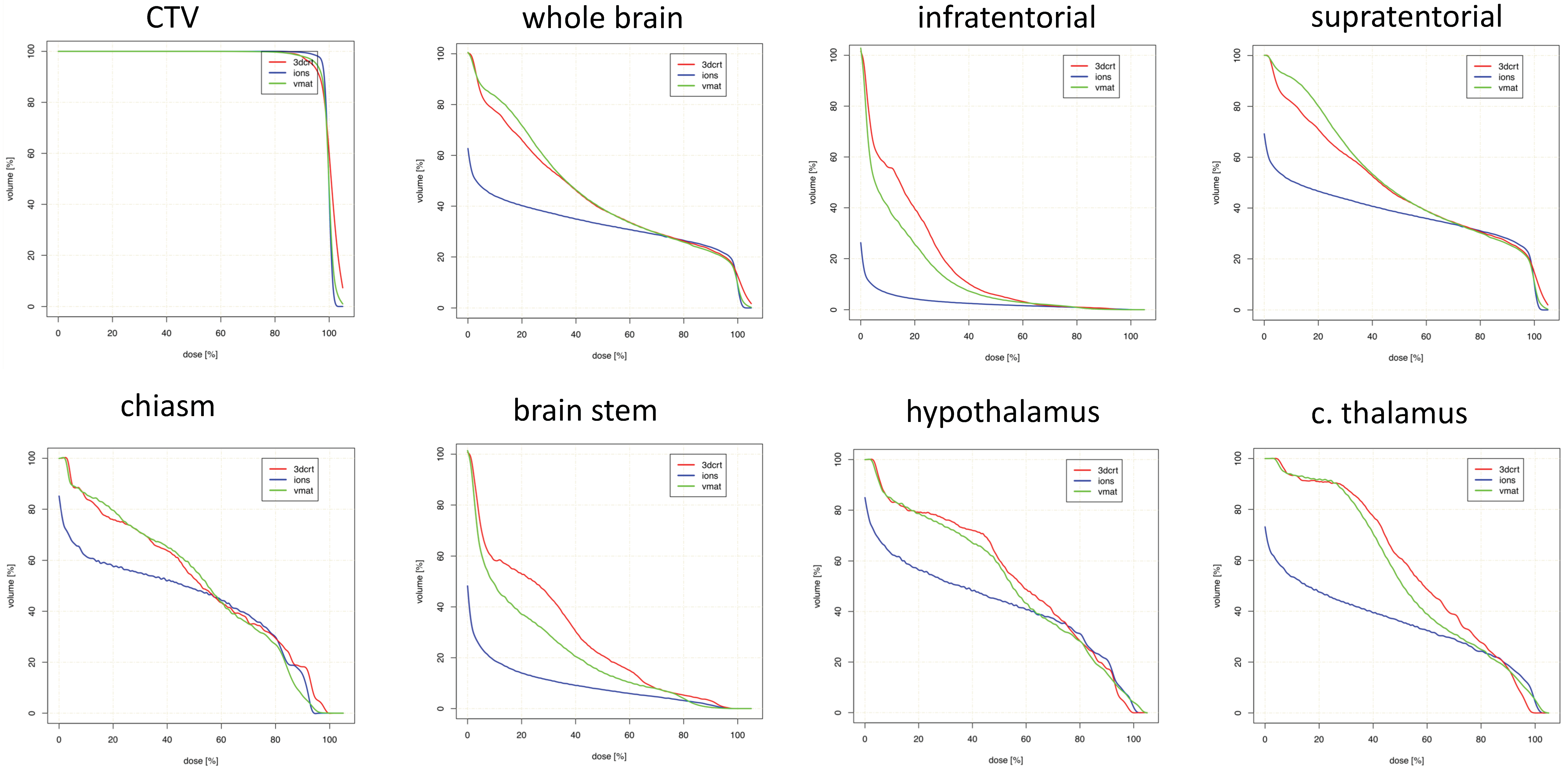
Figure 3 show data regarding temporal tumors. Maximum doses were also similar for most OARs. OARs for which PRT led to the greatest mean dose reductions were the contralateral hippocampus and thalamus.
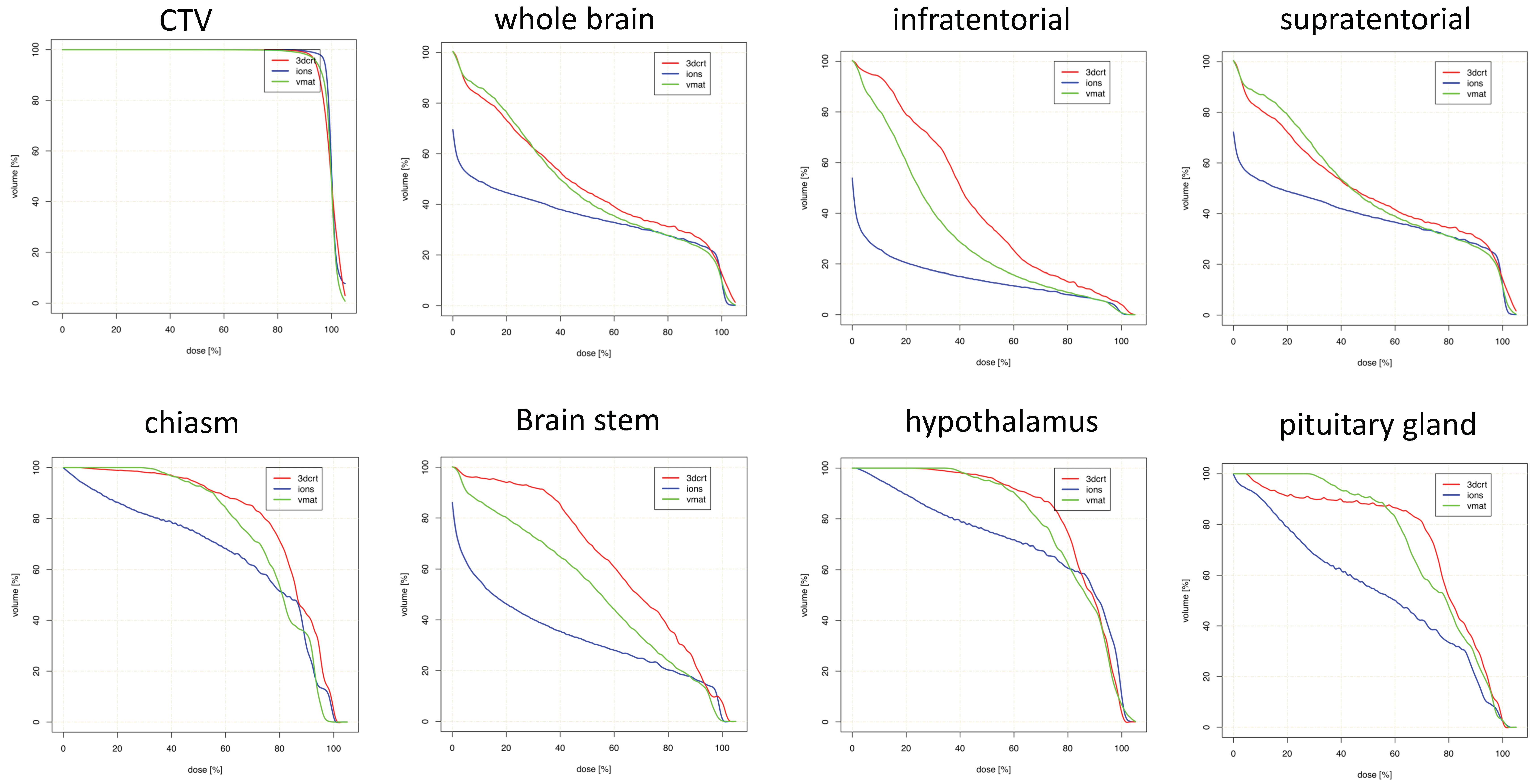
Parietal targets displayed the most notable dose reductions with PRT (
Table 5 and
Figure 4). This included multiple maximum dose (D
max) values for several OARs, including bilateral optic nerves, brainstem, and chiasm. Decreased mean doses to nearly every OAR was observed with PRT, most notably bilateral optic nerves and several contralateral structures (subventricular zone (SVZ), thalamus, hippocampus).
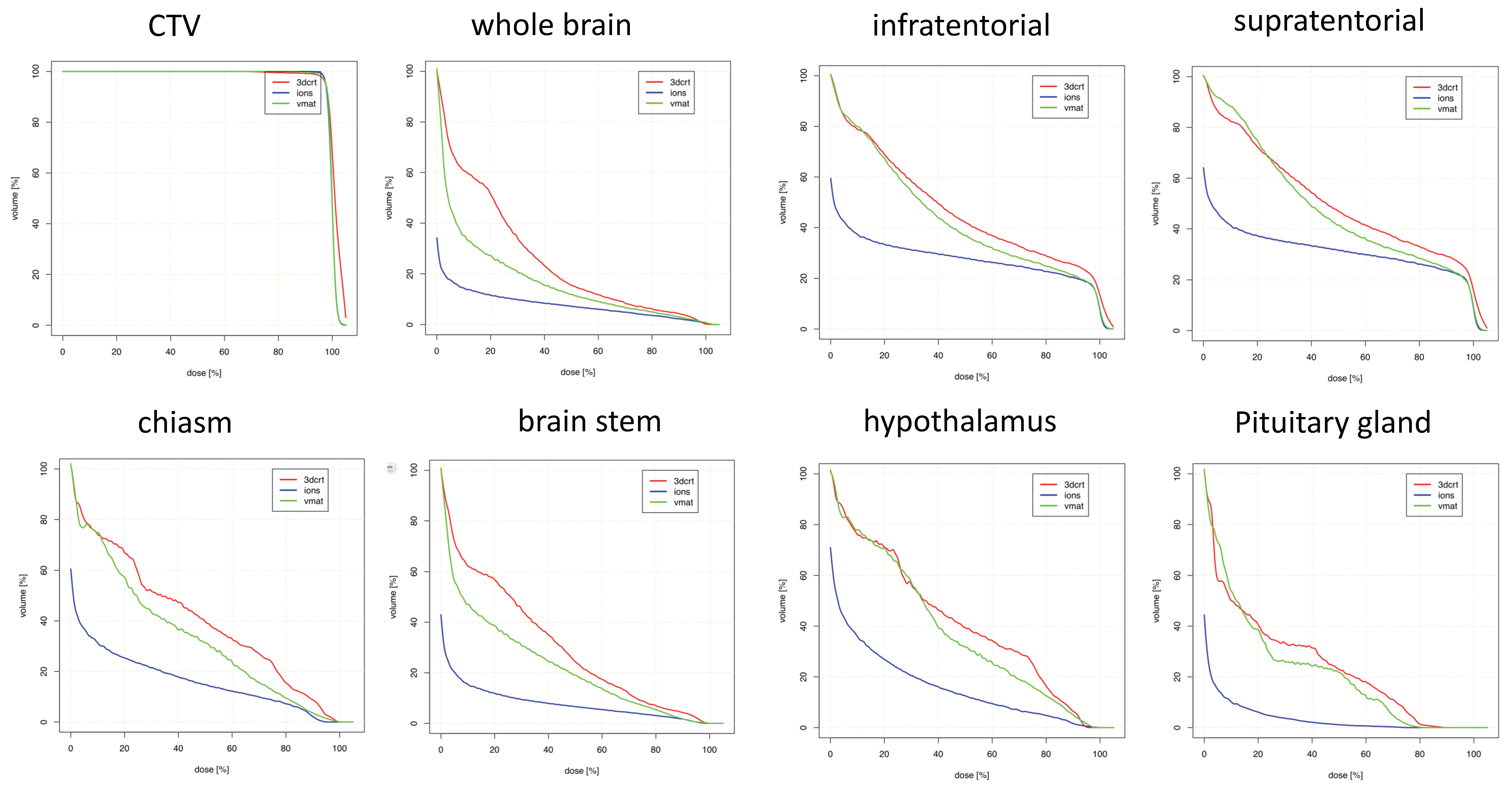
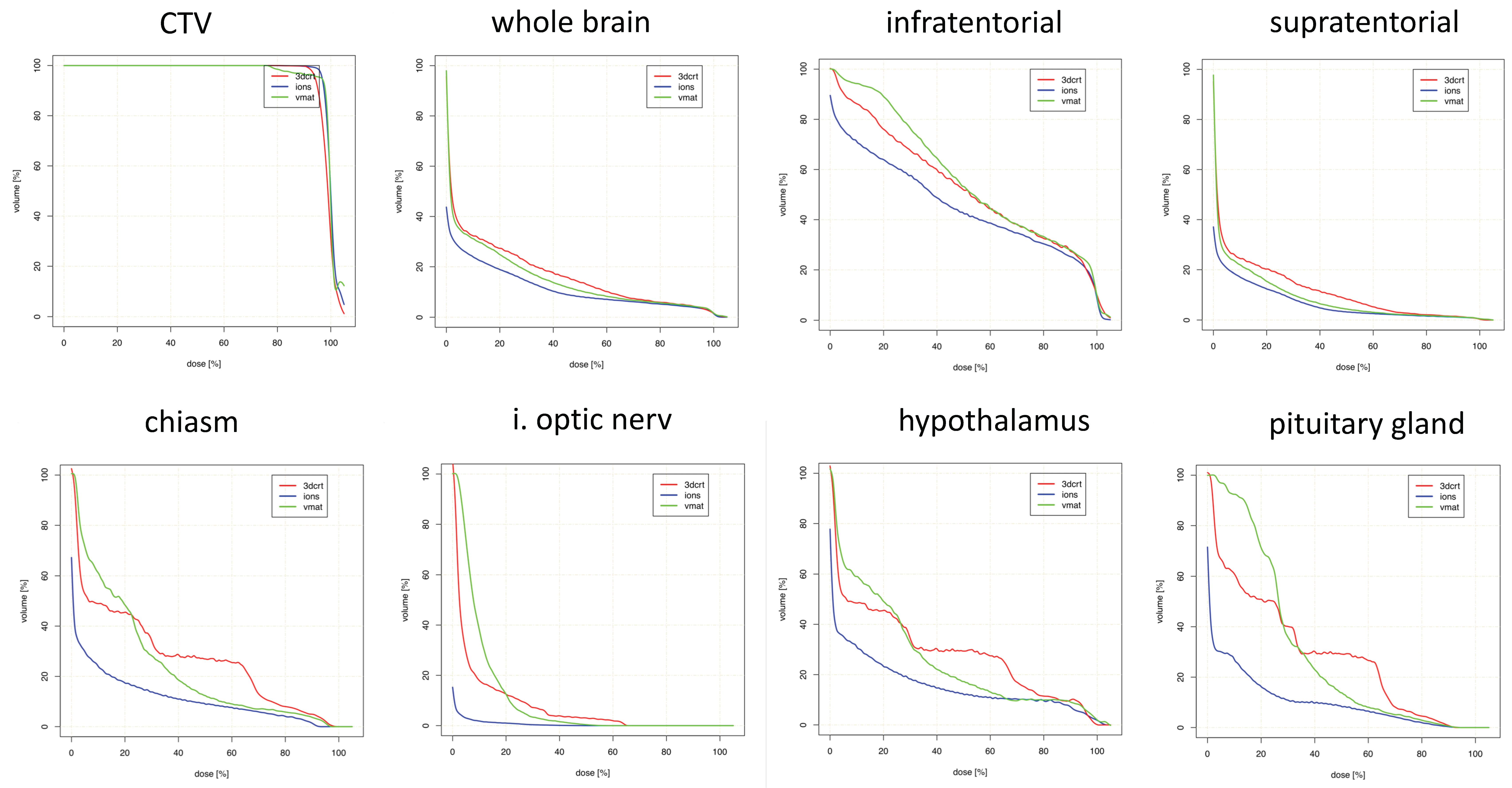
Lastly,
Table 6 and
Figure 5 display values for posterior cranial fossa disease. D
max values were comparable or slightly decreased with PRT for all OARs except the brainstem. D
mean reductions were highest in bilateral optic nerves, and the anatomical area corresponding to the hypothalamus/pituitary/chiasm. There were non-significant relative increases in D
mean for bilateral thalami and SVZ, however, along with the ipsilateral hippocampus.
Comparable CTV coverage could be achieved in all three treatment modalities. In one patient, no reasonable 3DCRT plan could be generated due to proximity to critical OARs. This plan was excluded from the analysis. The inhomogeneity coefficient (IC) and homogeneity index (HI) were mostly equivalent or superior in the proton plans as compared to 3DCRT and VMAT, without reaching statistical significance, as depicted in
Table 7.
3. Discussion
Our results offer overarching summaries that the PRT dose-sparing effect on various OARs is fundamentally dependent on tumor location. In other words, acknowledging the reliance on treatment planning techniques, PRT is more adept at sparing certain OARs depending on the location of primary disease. These data help to improve refined selection of patients receiving PRT, cost-effectiveness, and future clinical toxicity assessment.
When creating a treatment plan for any patient, regardless of technique or modality, it is impossible to spare every OAR to the lowest level possible. Rather, depending on which OARs are prioritized for a particular patient with a lesion in a given location (e.g., in terms of pre-existing comorbidities, life expectancy, and cost of managing late toxicities), this study may assist in evaluating whether PRT is indeed the most effective option. We acknowledge the limited applicability to other cases undergoing different treatment planning techniques, protocols, beam arrangements, and/or optimizations; nevertheless, these results can improve patient selection. For instance, if hippocampal sparing to the fullest degree is desired in a high-functioning young patient with parietal low-grade glioma, PRT may indeed be an appropriate option. The same may not be true if the tumor is in the posterior cranial fossa, and such cases may be equivalently served with state-of-the art IMRT techniques. The addition of these results to patient selection for PRT have large implications on cost-effectiveness, as detailed below.
Based on our results, broad generalizations based on location include that PRT provides the most optimal dose-sparing to OARs located at intermediate and farther distances from the target. In individual cases, PRT can lower OAR D
mean and D
max in proximity to the target; however, this cannot be displayed in a heterogenous cohort or even enable sufficient dose coverage of the target volume in proximity to critical OARs. In this context, in temporal tumors, excellent D
mean reductions are observed for the contralateral, but not ipsilateral, hippocampus. Nevertheless, although it is acknowledged that clinical and economic ramifications of dosimetric sparing of most intracerebral organs is currently unclear, it is likely that organs in the “intermediate distance” range could experience the most “clinically meaningful” toxicity reductions from improved dosimetry in terms of decreased D
mean with PRT. This is because dose reductions offered by PRT to distant organs is largely of overall low magnitude, on account of the already lower doses reaching farther anatomic locations. Another major theme herein is that PRT can effectively reduce integral brain doses (e.g., to normal whole brain tissue, or that supra/infratentorially), which some studies have postulated to relate to secondary malignancies [
13]. However, it must be cautioned that the notion of “clinically meaningful” toxicity reductions are currently theoretical and not supported by prospective randomized evidence thus far [
14].
Importantly, though the main goal of this study was to separate disease based on anatomical location, it is essential to recognize that achievable OAR doses are heavily dependent on particular locations within one of the five subsites delineated herein. For instance, a midline frontal lobe lesion and a well-lateralized one may have starkly different (contralateral) OAR doses (and dose-sparing), although both are still categorized in the same location group for this investigation. Hence, to that extent, our results do admittedly generalize within a group, but the overall conclusion should be that OAR sparing potential should still be taken on an individualized basis. The authors focused mainly on the comparisons of PRT versus other techniques. However, comparisons of 3DCRT versus VMAT were also performed (
Table 7). Here, no striking differences could be proven, which could be due to the high standard of variation of all five cohorts. This could lead to a demarcation of finer differences in dose reduction of −1% to −50% that did not reach statistical significance in the majority of calculations (
Table 2,
Table 3,
Table 4,
Table 5 and
Table 6).
The implications of these results include cost-effectiveness of PRT [
15]. Though a complete discussion is beyond the scope of this article, it should be mentioned that in longer-term survivors, there may be cost-savings associated with a decrease in dose to several OARs, although a link between dosimetry and clinical toxicity reductions remains to be proven. For instance, preservation of memory and quality of life from decreased hippocampal doses (a focus of the Radiation Therapy Oncology Group 0933 trial [
16]) are both associated with economic cost reductions. Similarly, it may be extrapolated from our findings that proton irradiation of tumors in any location may have the highest likelihood of having cost-effective PRT delivery, depending on the particular location within an anatomical subsite as discussed above. Further data are needed in order to corroborate this notion, however.
Our results complement other series that performed treatment planning comparisons in different entities. Fuss and colleagues performed a dosimetric comparison for optic pathway glioma, wherein PRT could reduce the D
max to the contralateral optic nerve by almost 50%; chiasm and pituitary gland doses were also reduced significantly using PRT [
17]. Pituitary dysfunction and secondary hypopituitarism are well known late effects of cranial irradiation [
18,
19], which becomes more relevant and prevalent in long-term survivors. The prevention of second malignancies is of minor importance in high-grade gliomas due to the still limited life expectancy, but is of interest in other intracranial tumors [
20,
21]. In centrally localized craniopharyngioma, PRT was superior to IMRT when comparing radiation dose exposure to the contralateral SVZ and hippocampus [
22]. When discussing the preservation of neuronal function after radiation therapy, the dosimetric advantages of PRT for the whole brain, hippocampus, temporal lobes, and sensory organs are easily apparent. Karunamuni and colleagues were able to discern a dose-dependent thinning of the cerebral cortex of 0.0033 mm/Gy with a pronounced effect in the temporal lobes and limbic cortex [
23]. It seems obvious that the degree of radiation-related neurocognitive dysfunction is a function of the exposed treatment volume and dose to the critical organs.
Though difficult to extrapolate these results to children, the advantages become even more relevant in this population. Declines in intelligence quotient (IQ), processing speed, and fine motor skills have been reported after conformal radiation therapy [
24,
25,
26]. To gain a better view on this topic, we performed a more detailed analysis of organs responsible for neurocognitive performance like the hypothalamus, the hippocampus, and the SVZ. The hippocampus and the bilateral SVZ are known to harbor neural progenitor cells [
27,
28], that are assumed to contribute to neurogenesis and injury repair with their self-renewing capacities [
29,
30], which could play a major role in the origin of neurocognitive impairment. However, the role of radiotherapeutic dose to the stem-cell niches is discussed controversial in the community [
31]. In glioblastoma, increased doses to the SVZ correlated with improved outcomes [
32,
33], suggesting tumor propagation and regeneration by cancer stem cells (CSCs) localized in the stem-cell niches.
The limitations of this analysis, in addition to the retrospective nature and relatively small sample size, include institutional-related nuances of treatment planning, beam arrangement, treatment technique, and optimization. It is also acknowledged that mean doses were most focused upon herein, but other parameters are undoubtedly important as well, depending on the level of correlative data available, as well as the type of OAR. A major limitation is that OAR doses are enormously dependent on priorities and weights of optimization and treatment planning, thus limiting the applicability of this and any other dosimetric study. The inclusion of different tumor types is of less consequence in a planning study similar to this, although outliers in size cannot be ignored. Retrospective contouring of several OARs that were not initially used for dose calculations is also acknowledged. Moreover, although location is not a discrete variable and tumors were lumped into specific categories, it is also not excluded that disease in different locations within each of the five groups may result in different results than those observed here. As such, further experiences are needed to validate these conclusions.

 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}