Aflatoxin M1 Analysis in Urine of Mill Workers in Bangladesh: A Pilot Study


Abstract
1. Introduction
2. Results
2.1. Characteristics of the Study Groups
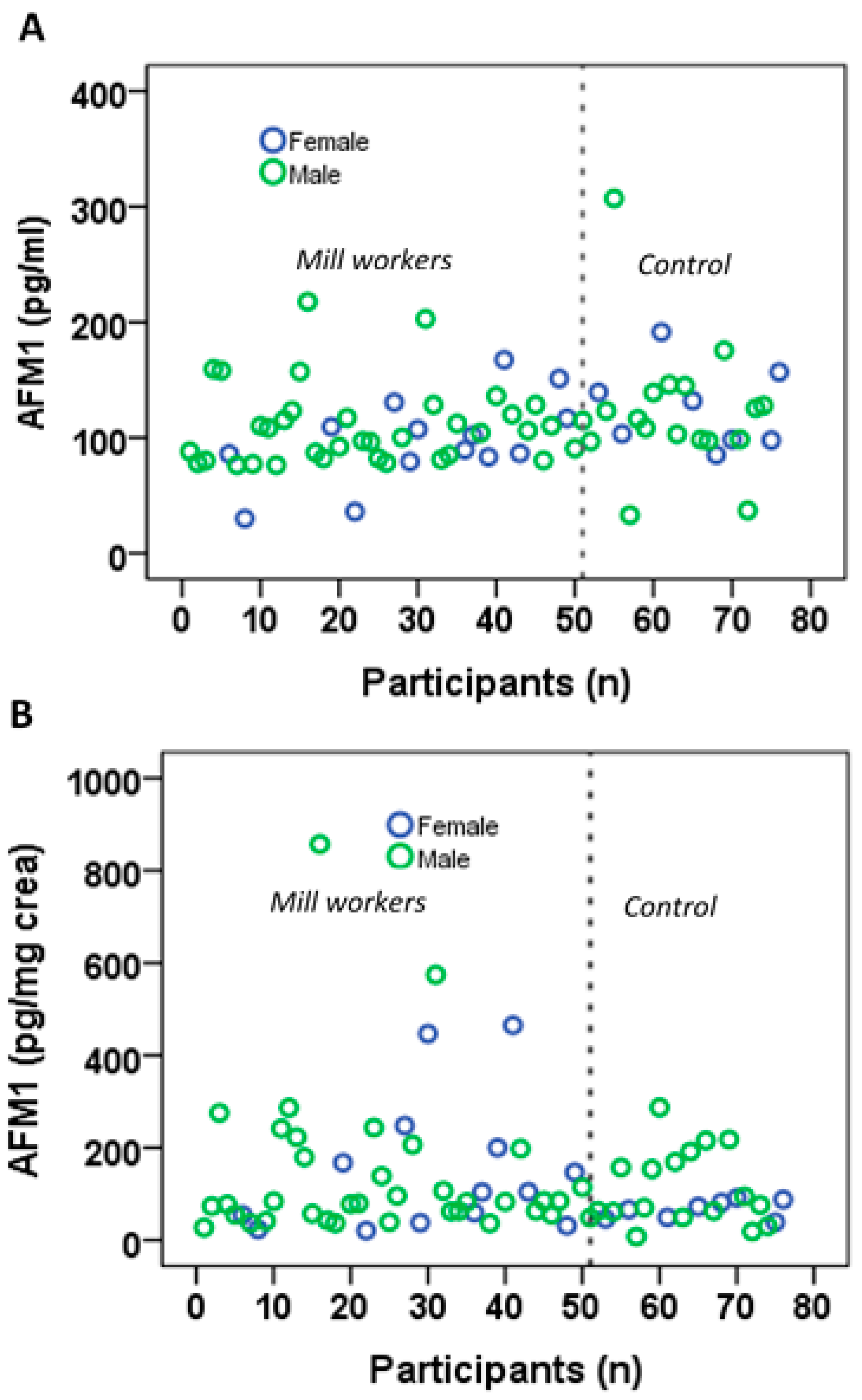
2.2. Levels of AFM1 in Urine of Mill Workers and Control Group
2.3. Relationship between AFM1 Biomarker Levels and Food Consumption
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Study Subjects and Sampling
5.2. Food Consumption Data
5.3. Sample Preparation and AFM1 Analysis
5.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, Y.; Sang, S. Phytochemicals in Whole Grain Wheat and Their Health-promoting Effects. Mol. Nutr. Food Res. 2017, 61, 1600852. [Google Scholar] [CrossRef] [PubMed]
- Tieri, M.; Ghelfi, F.; Vitale, M.; Vetrani, C.; Marventano, S.; Lafranconi, A.; Godos, J.; Titta, L.; Gambera, A.; Alonzo, E.; et al. Whole Grain Consumption and Human Health: An Umbrella Review of Observational Studies. Int. J. Food Sci. Nutr. 2020, 71, 668–677. [Google Scholar] [CrossRef] [PubMed]
- Paterson, R.R.M.; Lima, N. How Will Climate Change Affect Mycotoxins in Food? Food Res. Int. 2010, 43, 1902–1914. [Google Scholar] [CrossRef]
- Pitt, J.I.; Taniwaki, M.H.; Cole, M.B. Mycotoxin Production in Major Crops as Influenced by Growing, Harvesting, Storage and Processing, with Emphasis on the Achievement of Food Safety Objectives. Food Control 2013, 32, 205–215. [Google Scholar] [CrossRef]
- Van Der Fels-Klerx, H.J.; Klemsdal, S.; Hietaniemi, V.; Lindblad, M.; Ioannou-Kakouri, E.; Van Asselt, E.D. Mycotoxin Contamination of Cereal Grain Commodities in Relation to Climate in North West Europe. Food Addit. Contam. Part A 2012, 29, 1581–1592. [Google Scholar] [CrossRef]
- Eskola, M.; Kos, G.; Elliott, C.T.; Hajšlová, J.; Mayar, S.; Krska, R. Worldwide Contamination of Food-Crops with Mycotoxins: Validity of the Widely Cited ‘FAO Estimate’ of 25%. Crit. Rev. Food Sci. Nutr. 2020, 60, 2773–2789. [Google Scholar] [CrossRef]
- Loi, M.; Logrieco, A.F.; Pusztahelyi, T.; Leiter, É.; Hornok, L.; Pócsi, I. Advanced Mycotoxin Control and Decontamination Techniques in View of an Increased Aflatoxin Risk in Europe Due to Climate Change. Front. Microbiol. 2023, 13, 1085891. [Google Scholar] [CrossRef]
- Ali, N.; Blaszkewicz, M.; Hossain, K.; Degen, G.H. Determination of Aflatoxin M1 in Urine Samples Indicates Frequent Dietary Exposure to Aflatoxin B1 in the Bangladeshi Population. Int. J. Hyg. Environ. Health 2017, 220, 271–281. [Google Scholar] [CrossRef]
- Food and Agriculture Organization of the United Nations (FAO); World Health Organization (WHO). Aflatoxins. Safety Evaluation of Certain Contaminants in Food: Prepared by the 83rd Meeting of the Joint FAO/WHO Expert Committee on Food Additives (JECFA). WHO Addit. Ser. 2018, 2, 280. [Google Scholar]
- Rushing, B.R.; Selim, M.I. Aflatoxin B1: A Review on Metabolism, Toxicity, Occurrence in Food, Occupational Exposure, and Detoxification Methods. Food Chem. Toxicol. 2019, 124, 81–100. [Google Scholar] [CrossRef]
- IARC. Working Group Report No. 9, Mycotoxin Control in Lowand Middle Income Countries; Wild, C.P., Miller, J.D., Groopman, J.D., Eds.; IARC Publicationlyon: Lyon, France, 2015. [Google Scholar]
- Wild, C.P.; Turner, P.C. The Toxicology of Aflatoxins as a Basis for Public Health Decisions. Mutagenesis 2002, 17, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Kensler, T.W.; Roebuck, B.D.; Wogan, G.N.; Groopman, J.D. Aflatoxin: A 50-Year Odyssey of Mechanistic and Translational Toxicology. Toxicol. Sci. 2011, 120, S28–S48. [Google Scholar] [CrossRef]
- Saha Turna, N.; Comstock, S.S.; Gangur, V.; Wu, F. Effects of Aflatoxin on the Immune System: Evidence from Human and Mammalian Animal Research. Crit. Rev. Food Sci. Nutr. 2023, 1–19. [Google Scholar] [CrossRef] [PubMed]
- IARC International Agency for Research on Cancer. Aflatoxins. In Chemical Agents and Related Occupations; IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 100F; IARC Press: Lyon, France, 2012; pp. 225–248. [Google Scholar]
- Liu, Y.; Wu, F. Global Burden of Aflatoxin-Induced Hepatocellular Carcinoma: A Risk Assessment. Environ. Health Perspect. 2010, 118, 818–824. [Google Scholar] [CrossRef]
- Giovati, L.; Magliani, W.; Ciociola, T.; Santinoli, C.; Conti, S.; Polonelli, L. AFM1 in Milk: Physical, Biological, and Prophylactic Methods to Mitigate Contamination. Toxins 2015, 7, 4330–4349. [Google Scholar] [CrossRef] [PubMed]
- BFSA Bangladesh Food Safety Authority. Food Safety Regulations. 2017. Available online: https://apps.fas.usda.gov/newgainapi/api/Report/DownloadReportByFileName?fileName=Bangladesh%20issues%20Regulation%20on%20Food%20Safety%202017%20_Dhaka_Bangladesh_03-06-2021 (accessed on 10 December 2023).
- Marchese, S.; Polo, A.; Ariano, A.; Velotto, S.; Costantini, S.; Severino, L. Aflatoxin B1 and M1: Biological Properties and Their Involvement in Cancer Development. Toxins 2018, 10, 214. [Google Scholar] [CrossRef]
- Panel, E.C. Scientific Opinion—Risk Assessment of Aflatoxins in Food. EFSA J. 2020, 18, e06040. [Google Scholar] [CrossRef]
- Turner, P.C.; Flannery, B.; Isitt, C.; Ali, M.; Pestka, J. The Role of Biomarkers in Evaluating Human Health Concerns from Fungal Contaminants in Food. Nutr. Res. Rev. 2012, 25, 162–179. [Google Scholar] [CrossRef]
- Vidal, A.; Mengelers, M.; Yang, S.; De Saeger, S.; De Boevre, M. Mycotoxin Biomarkers of Exposure: A Comprehensive Review. Comp. Rev. Food Sci. Food Safe 2018, 17, 1127–1155. [Google Scholar] [CrossRef]
- Gerding, J.; Ali, N.; Schwartzbord, J.; Cramer, B.; Brown, D.L.; Degen, G.H.; Humpf, H.-U. A Comparative Study of the Human Urinary Mycotoxin Excretion Patterns in Bangladesh, Germany, and Haiti Using a Rapid and Sensitive LC-MS/MS Approach. Mycotoxin Res. 2015, 31, 127–136. [Google Scholar] [CrossRef]
- Solfrizzo, M.; Gambacorta, L.; Visconti, A. Assessment of Multi-Mycotoxin Exposure in Southern Italy by Urinary Multi-Biomarker Determination. Toxins 2014, 6, 523–538. [Google Scholar] [CrossRef] [PubMed]
- Heyndrickx, E.; Sioen, I.; Huybrechts, B.; Callebaut, A.; De Henauw, S.; De Saeger, S. Human Biomonitoring of Multiple Mycotoxins in the Belgian Population: Results of the BIOMYCO Study. Environ. Int. 2015, 84, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Ali, N.; Manirujjaman, M.; Rana, S.; Degen, G.H. Determination of Aflatoxin M1 and Deoxynivalenol Biomarkers in Infants and Children Urines from Bangladesh. Arch. Toxicol. 2020, 94, 3775–3786. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, M.F.; Gado, M.; Abdelsadek, D.; Zahran, F.; El-Salhey, N.N.; Mehrez, O.; Abdel-Hay, S.; Mohamed, S.M.; De Ruyck, K.; Yang, S.; et al. Mycotoxin Contamination in the Arab World: Highlighting the Main Knowledge Gaps and the Current Legislation. Mycotoxin Res. 2023. [Google Scholar] [CrossRef] [PubMed]
- Degen, G. Tools for Investigating Workplace-Related Risks from Mycotoxin Exposure. WMJ 2011, 4, 315–327. [Google Scholar] [CrossRef]
- Fromme, H.; Gareis, M.; Völkel, W.; Gottschalk, C. Overall Internal Exposure to Mycotoxins and Their Occurrence in Occupational and Residential Settings—An Overview. Int. J. Hyg. Environ. Health 2016, 219, 143–165. [Google Scholar] [CrossRef]
- Straumfors, A.; Uhlig, S.; Eriksen, G.S.; Heldal, K.K.; Eduard, W.; Krska, R.; Sulyok, M. Mycotoxins and Other Fungal Metabolites in Grain Dust from Norwegian Grain Elevators and Compound Feed Mills. WMJ 2015, 8, 361–373. [Google Scholar] [CrossRef]
- Viegas, S.; Viegas, C.; Oppliger, A. Occupational Exposure to Mycotoxins: Current Knowledge and Prospects. Ann. Work Expo. Health 2018, 62, 923–941. [Google Scholar] [CrossRef]
- Franco, L.T.; Ismail, A.; Amjad, A.; de Oliveira, C.A.F. Occurrence of Toxigenic Fungi and Mycotoxins in Workplaces and Human Biomonitoring of Mycotoxins in Exposed Workers: A Systematic Review. Toxin Rev. 2021, 40, 576–591. [Google Scholar] [CrossRef]
- Föllmann, W.; Ali, N.; Blaszkewicz, M.; Degen, G.H. Biomonitoring of Mycotoxins in Urine: Pilot Study in Mill Workers. J. Toxicol. Environ. Health Part A 2016, 79, 1015–1025. [Google Scholar] [CrossRef]
- Viegas, S.; Assunção, R.; Martins, C.; Nunes, C.; Osteresch, B.; Twarużek, M.; Kosicki, R.; Grajewski, J.; Ribeiro, E.; Viegas, C. Occupational Exposure to Mycotoxins in Swine Production: Environmental and Biological Monitoring Approaches. Toxins 2019, 11, 78. [Google Scholar] [CrossRef]
- Dawlatana, M.; Coker, R.D.; Nagler, M.J.; Wild, C.P.; Hassan, M.S.; Blunden, G. The Occurrence of Mycotoxins in Key Commodities in Bangladesh: Surveillance Results from 1993 to 1995. J. Nat. Toxins 2002, 11, 379–386. [Google Scholar] [PubMed]
- Bhuiyan, M.N.H.; Hassan, M.T.; Begum, M.; Ahan, M.; Rahim, M. Occurrence and Seasonal Trends of Aflatoxin in Rice, Maize and Wheat in Bangladesh. Int. J. Sustain. Agril. Tech. 2013, 9, 8–14. [Google Scholar]
- Roy, M.; Harris, J.; Afreen, S.; Deak, E.; Gade, L.; Balajee, S.A.; Park, B.; Chiller, T.; Luby, S. Aflatoxin Contamination in Food Commodities in Bangladesh. Food Addit. Contam. Part B 2013, 6, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Ali, N.; Hossain, K.; Blaszkewicz, M.; Rahman, M.; Mohanto, N.C.; Alim, A.; Degen, G.H. Occurrence of Aflatoxin M1 in Urines from Rural and Urban Adult Cohorts in Bangladesh. Arch. Toxicol 2016, 90, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- Islam, F.; Das Trisha, A.; Hafsa, J.M.; Hasan, A.; Degen, G.H.; Ali, N. Occurrence of Aflatoxin M1 in Human Breast Milk in Bangladesh. Mycotoxin Res. 2021, 37, 241–248. [Google Scholar] [CrossRef]
- Mayer, S.; Engelhart, S.; Kolk, A.; Blome, H. The Significance of Mycotoxins in the Framework of Assessing Workplace Related Risks. Mycotox. Res. 2008, 24, 151–164. [Google Scholar] [CrossRef]
- Ferri, F.; Brera, C.; De Santis, B.; Fedrizzi, G.; Bacci, T.; Bedogni, L.; Capanni, S.; Collini, G.; Crespi, E.; Debegnach, F.; et al. Survey on Urinary Levels of Aflatoxins in Professionally Exposed Workers. Toxins 2017, 9, 117. [Google Scholar] [CrossRef]
- Debegnach, F.; Brera, C.; Mazzilli, G.; Sonego, E.; Buiarelli, F.; Ferri, F.; Rossi, P.G.; Collini, G.; De Santis, B. Optimization and Validation of a LC-HRMS Method for Aflatoxins Determination in Urine Samples. Mycotoxin Res. 2020, 36, 257–266. [Google Scholar] [CrossRef]
- Ndaw, S.; Jargot, D.; Antoine, G.; Denis, F.; Melin, S.; Robert, A. Investigating Multi-Mycotoxin Exposure in Occupational Settings: A Biomonitoring and Airborne Measurement Approach. Toxins 2021, 13, 54. [Google Scholar] [CrossRef]
- Abrar, M.; Ahsan, S.; Nadeem, M.; Liaqat, A.; Chughtai, M.F.J.; Farooq, M.A.; Mehmood, T.; Khaliq, A.; Siddiqa, A. Detection and Quantification of Aflatoxins in Spices Stored in Different Food Packaging Materials. J. Stored Prod. Res. 2023, 101, 102081. [Google Scholar] [CrossRef]
- Zhao, X.; Schaffner, D.W.; Yue, T. Quantification of Aflatoxin Risk Associated with Chinese Spices: Point and Probability Risk Assessments for Aflatoxin B1. Food Control 2013, 33, 366–377. [Google Scholar] [CrossRef]
- Yogendrarajah, P.; Jacxsens, L.; De Saeger, S.; De Meulenaer, B. Co-Occurrence of Multiple Mycotoxins in Dry Chilli (Capsicum Annum L.) Samples from the Markets of Sri Lanka and Belgium. Food Control 2014, 46, 26–34. [Google Scholar] [CrossRef]
- Zareshahrabadi, Z.; Bahmyari, R.; Nouraei, H.; Khodadadi, H.; Mehryar, P.; Asadian, F.; Zomorodian, K. Detection of Aflatoxin and Ochratoxin A in Spices by High-Performance Liquid Chromatography. J. Food Qual. 2020, 2020, e8858889. [Google Scholar] [CrossRef]
- Ali, N. Aflatoxins in Rice: Worldwide Occurrence and Public Health Perspectives. Toxicol. Rep. 2019, 6, 1188–1197. [Google Scholar] [CrossRef]
- UBA (Umweltbundesamt). Normierung von Stoffgehalten im Urin—Kreatinin: Stellungnahme der Kommission “Human-Biomonitoring“ des Umweltbundesamtes. Bundesgesundheitsbl. Gesundheitsf. Gesundheitsschutz 2005, 48, 616–618. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Mill Workers | Control Group | p-Value |
|---|---|---|---|
| Subjects (n) | 51 | 25 | - |
| Mill-based workers (n) | |||
| Rice | 20 | - | - |
| Wheat | 9 | - | - |
| Maize | 11 | - | - |
| Spices | 11 | ||
| Gender (m/f) | 37/14 | 17/8 | 0.439 |
| Age (years) | 38.76 ± 10.92 | 38.64 ± 10.21 | 0.961 |
| BMI (kg/m2) | |||
| Mean ± SD | 21.74 ± 3.07 | 24.94 ± 3.45 | <0.001 |
| Range | 16.69–30.47 | 19.38–29.76 | - |
| Creatinine (mg/mL) | 1.34 ± 0.91 | 1.78 ± 1.07 | 0.086 |
| Socioeconomic status (n, %) | 0.170 | ||
| Low | 42 (82.4) | 22 (88.0) | |
| Medium | 8 (15.7) | 1 (4.0) | |
| Upper medium | 1 (2.0) | 2 (8.0) | |
| Education level (n, %) | 0.347 | ||
| Primary | 37 (72.5) | 18 (72.0) | |
| Secondary | 12 (23.5) | 4 (16.0) | |
| Above secondary | 2 (3.9) | 3 (12.0) |
| Group | n | Positive n (%) | Mean ± SD | Median | Maximum | ||||
|---|---|---|---|---|---|---|---|---|---|
| pg/mL | pg/mg Crea | pg/mL | pg/mg Crea | pg/mL | pg/mg Crea | ||||
| Mill workers | Male | 37 | 37 (100.0) | 109.7 ± 33.9 | 138.8 ± 131.3 | 104.1 | 82.5 | 217.7 | 857.1 |
| Female | 14 | 12 (85.7) | 98.2 ± 37.9 | 150.8 ± 126.9 | 95.7 | 104.3 | 167.4 | 465.1 | |
| Total | 51 | 49 (96.1) | 106.5 ± 35.0 | 142.1 ± 126.1 | 102.0 | 83.1 | 217.7 | 857.1 | |
| Controls | Male | 17 | 15 (88.2) | 122.2 ± 59.5 | 113.3 ± 81.8 | 116.4 | 76.2 | 307.0 | 287.3 |
| Female | 8 | 8 (100.0) | 125.5 ± 36.2 | 66.8 ± 20.1 | 117.5 | 69.4 | 191.4 | 91.6 | |
| Total | 25 | 23 (92.0) | 123.3 ± 52.4 | 98.5 ± 71.2 | 116.4 | 72.6 | 307.0 | 287.3 | |
| Samples | n | Positive n (%) | Mean ± SD | Median | Max | |||
|---|---|---|---|---|---|---|---|---|
| pg/mL | pg/mg Crea | pg/mL | pg/mg Crea | pg/mL | pg/mg Crea | |||
| Rice mill workers | 20 | 19 (95.0) | 102.4 ± 32.7 | 146.5 ± 123.4 | 98.7 | 89.6 | 202.8 | 574.5 |
| Wheat mill workers | 9 | 8 (88.9) | 92.6 ± 41.2 | 73.9 ± 57.9 | 80.2 | 54.6 | 159.3 | 275.5 |
| Maize mill workers | 11 | 11 (100.0) | 115.7 ± 26.4 | 127.0 ± 111.8 | 114.7 | 84.9 | 167.4 | 465.1 |
| Spices mill workers | 11 | 11 (100.0) | 116.3 ± 40.4 | 205.0 ± 192.9 | 109.3 | 167.7 | 217.7 | 857.1 |
| N | AFM1 (pg/mL) | AFM1 (pg/mg Crea) | |||
|---|---|---|---|---|---|
| Mean ± SD | Max | Mean ± SD | Max | ||
| Regular rice consumption | |||||
| 1–2 times/day | 17 | 117.5 ± 26.0 | 159.3 | 103.0 ± 60.8 | 247.8 |
| 3 times/day | 59 | 110.5 ± 45.6 | 307.0 | 134.9 ± 129.7 | 857.1 |
| Last 2 days rice consumption | |||||
| 2–4 times/2 days | 17 | 114.7 ± 27.1 | 159.3 | 90.7 ± 49.7 | 198.0 |
| 5–6 times/2 days | 59 | 111.3 ± 45.5 | 307.0 | 138.5 ± 129.9 * | 857.1 |
| Food Items | Regular Food Consumption Habits | Last 2 Days Food Consumption | ||
|---|---|---|---|---|
| Correlation (r) | p-Value | Correlation (r) | p-Value | |
| Rice | 0.035 | 0.762 | 0.038 | 0.725 |
| Wheat/maize | 0.144 | 0.214 | 0.186 | 0.108 |
| Milks | 0.136 | 0.243 | 0.208 | 0.071 |
| Pulses | 0.083 | 0.474 | 0.015 | 0.898 |
| Ground nuts | 0.304 | 0.008 | 0.259 | 0.024 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, N.; Habib, A.; Mahmud, F.; Tuba, H.R.; Degen, G.H. Aflatoxin M1 Analysis in Urine of Mill Workers in Bangladesh: A Pilot Study. Toxins 2024, 16, 45. https://doi.org/10.3390/toxins16010045
Ali N, Habib A, Mahmud F, Tuba HR, Degen GH. Aflatoxin M1 Analysis in Urine of Mill Workers in Bangladesh: A Pilot Study. Toxins. 2024; 16(1):45. https://doi.org/10.3390/toxins16010045
Chicago/Turabian StyleAli, Nurshad, Ahsan Habib, Firoz Mahmud, Humaira Rashid Tuba, and Gisela H. Degen. 2024. "Aflatoxin M1 Analysis in Urine of Mill Workers in Bangladesh: A Pilot Study" Toxins 16, no. 1: 45. https://doi.org/10.3390/toxins16010045
APA StyleAli, N., Habib, A., Mahmud, F., Tuba, H. R., & Degen, G. H. (2024). Aflatoxin M1 Analysis in Urine of Mill Workers in Bangladesh: A Pilot Study. Toxins, 16(1), 45. https://doi.org/10.3390/toxins16010045