Effects of a Single Session of OnabotulinumtoxinA Therapy on Sleep Quality and Psychological Measures: Preliminary Findings in a Population of Chronic Migraineurs

 ,
, 
 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Results
2.1. Population
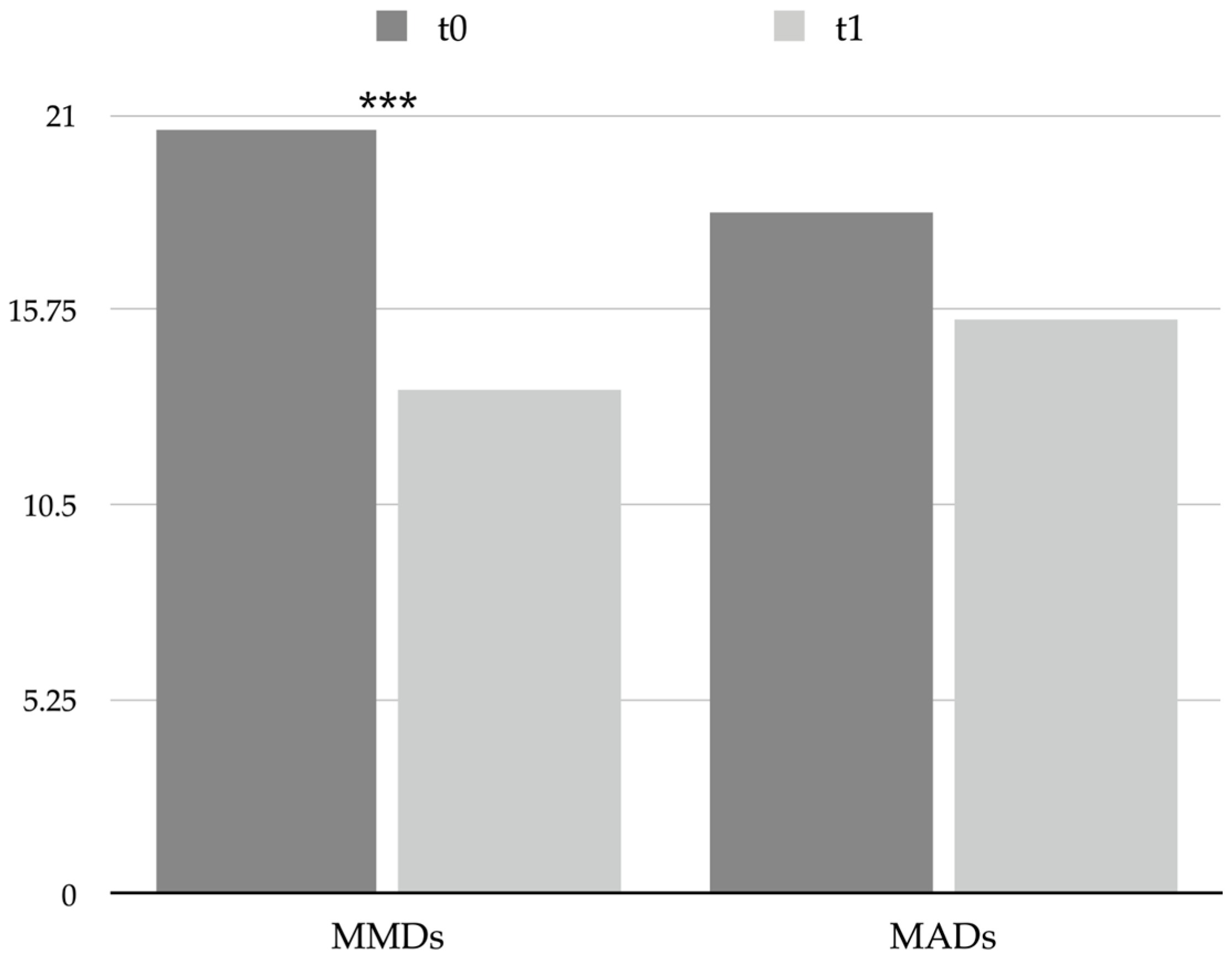
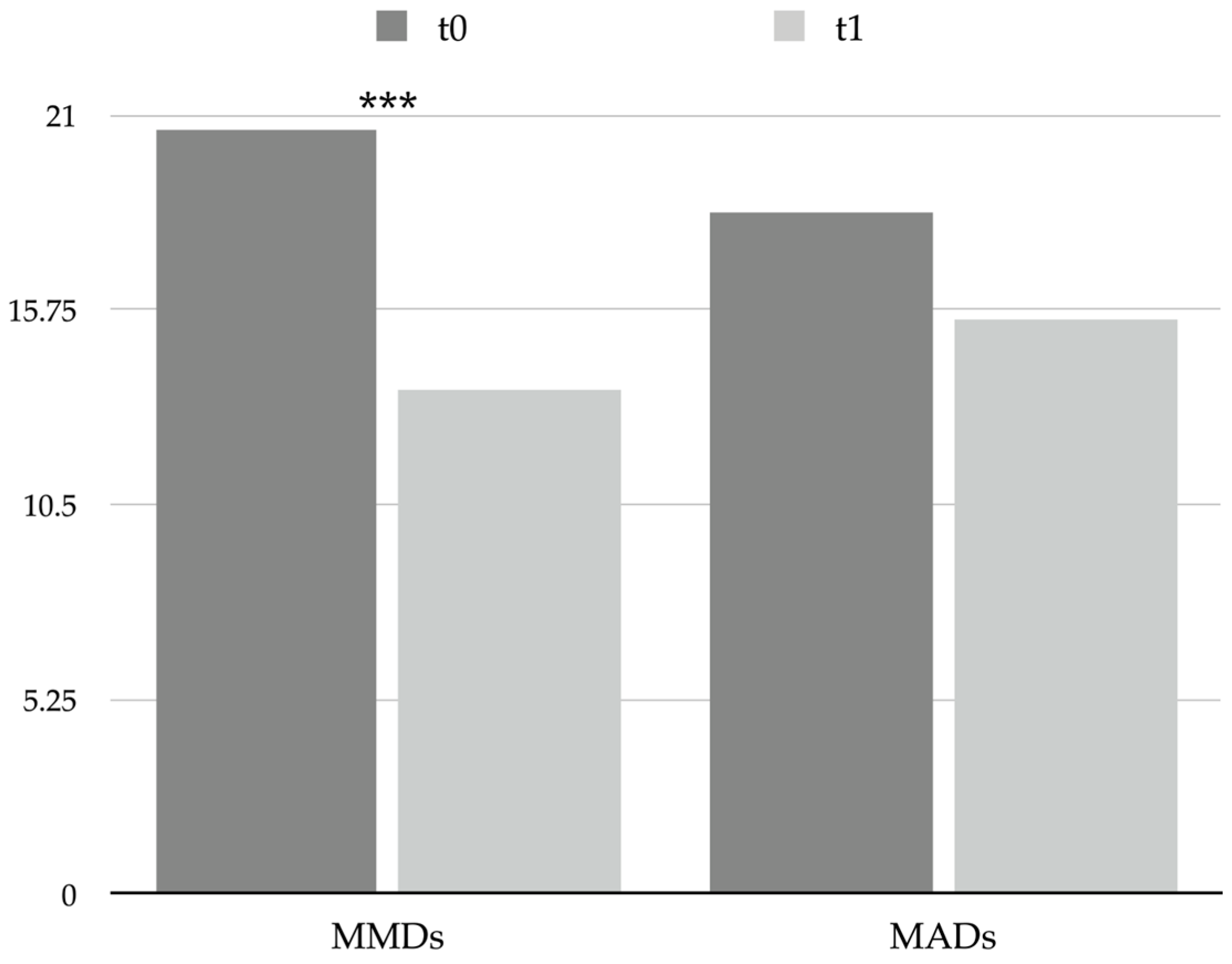
2.2. Headache Features
2.3. Sleep Quality
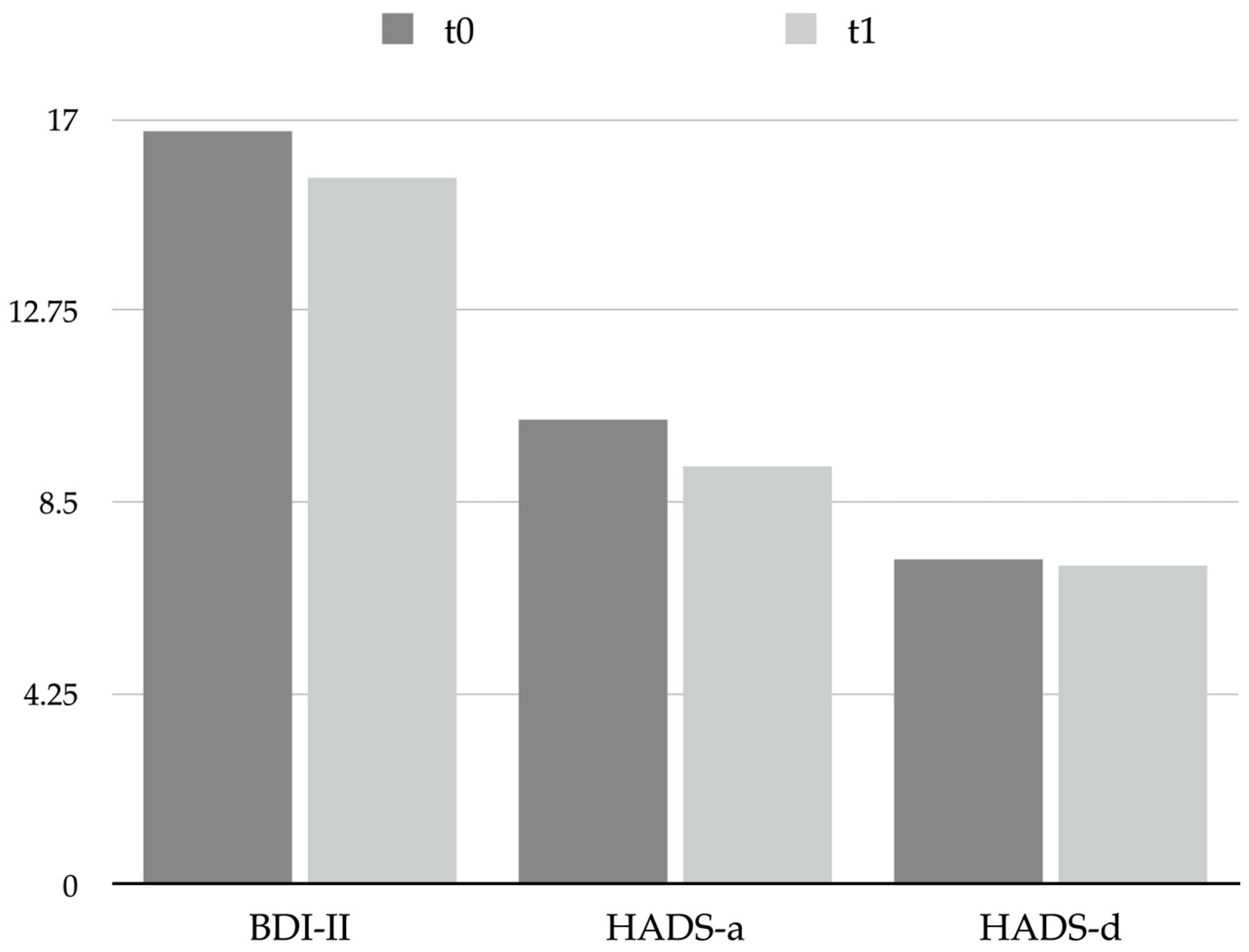
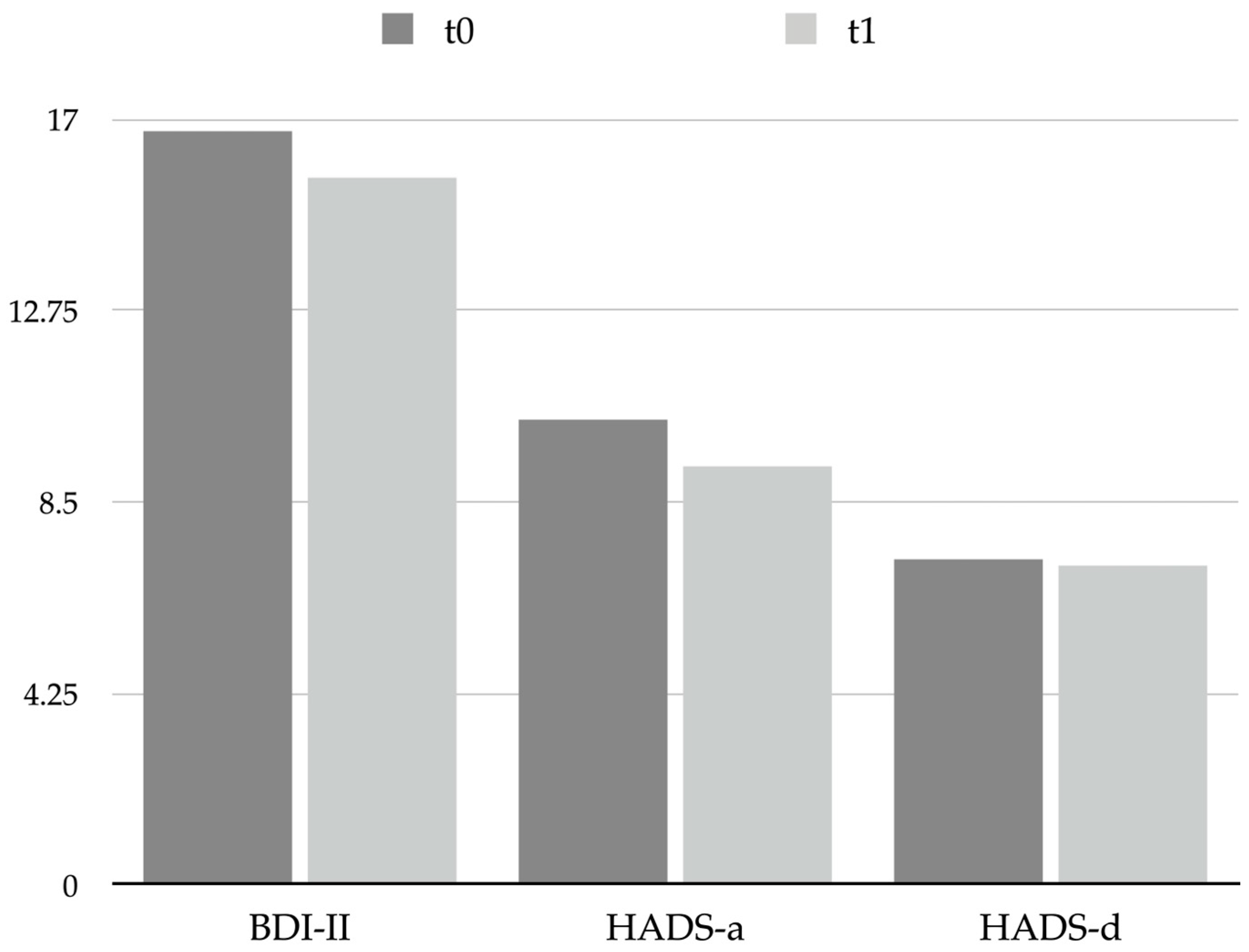
2.4. Psychological Correlates
2.5. Impact and Disability
2.6. Correlation Analysis
3. Discussion
4. Materials and Methods
4.1. Study Procedures
4.2. Participants
4.3. Study Design
4.4. Preventive Treatment Protocol
4.5. Clinical Assessment
4.5.1. Headache Features
4.5.2. Pittsburgh Sleep Quality Index (PSQI)
4.5.3. Psychological Symptoms Investigation
HADS
BDI-II
4.5.4. Headache Impact and Related Disability
HIT-6
MIDAS
4.6. Statistical Analysis and Data Presentation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cosentino, G.; Fierro, B.; Vigneri, S.; Talamanca, S.; Paladino, P.; Baschi, R.; Indovino, S.; Maccora, S.; Valentino, F.; Fileccia, E.; et al. Cyclical changes of cortical excitability and metaplasticity in migraine: Evidence from a repetitive transcranial magnetic stimulation study. Pain 2014, 155, 1070–1078. [Google Scholar] [CrossRef] [PubMed]
- Brighina, F.; Bolognini, N.; Cosentino, G.; MacCora, S.; Paladino, P.; Baschi, R.; Vallar, G.; Fierro, B. Visual cortex hyperexcitability in migraine in response to sound-induced flash illusions. Neurology 2015, 84, 2057–2061. [Google Scholar] [CrossRef]
- Braganza, D.L.; Fitzpatrick, L.E.; Nguyen, M.L.; Crowe, S.F. Interictal Cognitive Deficits in Migraine Sufferers: A Meta-Analysis. Neuropsychol. Rev. 2022, 32, 736–757. [Google Scholar] [CrossRef] [PubMed]
- Peres, M.F.P.; Mercante, J.P.P.; Tobo, P.R.; Kamei, H.; Bigal, M.E. Anxiety and depression symptoms and migraine: A symptom-based approach research. J. Headache Pain. 2017, 18, 37. [Google Scholar] [CrossRef]
- Zhang, Q.; Shao, A.; Jiang, Z.; Tsai, H.; Liu, W. The exploration of mechanisms of comorbidity between migraine and depression. J. Cell. Mol. Med. 2019, 23, 4505–4513. [Google Scholar] [CrossRef] [PubMed]
- Marmura, M.J. Triggers, Protectors, and Predictors in Episodic Migraine. Curr. Pain Headache Rep. 2018, 22, 81. [Google Scholar] [CrossRef]
- Vgontzas, A.; Pavlović, J.M. Sleep Disorders and Migraine: Review of Literature and Potential Pathophysiology Mechanisms. Headache 2018, 58, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- Drescher, J.; Wogenstein, F.; Gaul, C.; Kropp, P.; Reinel, D.; Siebenhaar, Y.; Scheidt, J. Distribution of migraine attacks over the days of the week: Preliminary results from a web-based questionnaire. Acta Neurol. Scand. 2019, 139, 340–345. [Google Scholar] [CrossRef]
- Stanyer, E.C.; Creeney, H.; Nesbitt, A.D.; Holland, P.R.; Hoffmann, J. Subjective Sleep Quality and Sleep Architecture in Patients with Migraine: A Meta-analysis. Neurology 2021, 97, E1620–E1631. [Google Scholar] [CrossRef]
- Viticchi, G.; Falsetti, L.; Paolucci, M.; Altamura, C.; Buratti, L.; Salvemini, S.; Brunelli, N.; Bartolini, M.; Vernieri, F.; Silvestrini, M. Influence of chronotype on migraine characteristics. Neurol. Sci. 2019, 40, 1841–1848. [Google Scholar] [CrossRef]
- Nelson, K.L.; Davis, J.E.; Corbett, C.F. Sleep quality: An evolutionary concept analysis. Nurs. Forum 2022, 57, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.; Cui, L.; Merikangas, K.R. Are sleep difficulties associated with migraine attributable to anxiety and depression? Headache 2008, 48, 1451–1459. [Google Scholar] [CrossRef] [PubMed]
- Olesen, J. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar]
- Torres-Ferrús, M.; Ursitti, F.; Alpuente-Ruiz, A.; Brunello, F.; Chiappino, D.; De Vries, T.; Di Marco, S.; Ferlisi, S.; Guerritore, L.; Gonzalez-Garcia, N.; et al. From transformation to chronification of migraine: Pathophysiological and clinical aspects. J. Headache Pain. 2020, 21, 42. [Google Scholar] [CrossRef] [PubMed]
- May, A.; Schulte, L.H. Chronic migraine: Risk factors, mechanisms and treatment. Nat. Rev. Neurol. 2016, 12, 455–464. [Google Scholar] [CrossRef]
- Maccora, S.; Bolognini, N.; Cosentino, G.; Baschi, R.; Vallar, G.; Fierro, B.; Brighina, F. Multisensorial Perception in Chronic Migraine and the Role of Medication Overuse. J. Pain 2020, 21, 919–929. [Google Scholar] [CrossRef]
- Seng, E.K.; Buse, D.C.; Klepper, J.E.; Mayson, S.J.; Grinberg, A.S.; Grosberg, B.M.; Pavlovic, J.M.; Robbins, M.S.; Vollbracht, S.E.; Lipton, R.B. Psychological Factors Associated with Chronic Migraine and Severe Migraine-Related Disability: An Observational Study in a Tertiary Headache Center. Headache 2017, 57, 593–604. [Google Scholar] [CrossRef]
- Schwedt, T.J. Chronic migraine. BMJ 2014, 348, g1416. [Google Scholar] [CrossRef]
- Burstein, R.; Blumenfeld, A.M.; Silberstein, S.D.; Manack Adams, A.; Brin, M.F. Mechanism of Action of OnabotulinumtoxinA in Chronic Migraine: A Narrative Review. Headache 2020, 60, 1259–1272. [Google Scholar] [CrossRef]
- Diener, H.C.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; Degryse, R.E.; Lipton, R.B.; Silberstein, S.D.; Brin, M.F. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia 2010, 30, 804–814. [Google Scholar] [CrossRef]
- Matharu, M.; Halker, R.; Pozo-Rosich, P.; DeGryse, R.; Manack Adams, A.; Aurora, S.K. The impact of onabotulinumtoxinA on severe headache days: PREEMPT 56-week pooled analysis. J. Headache Pain 2017, 18, 78. [Google Scholar] [CrossRef] [PubMed]
- Affatato, O.; Moulin, T.C.; Pisanu, C.; Babasieva, V.S.; Russo, M.; Aydinlar, E.I.; Torelli, P.; Chubarev, V.N.; Tarasov, V.V.; Schiöth, H.B.; et al. High efficacy of onabotulinumtoxinA treatment in patients with comorbid migraine and depression: A meta-analysis. J. Transl. Med. 2021, 19, 133. [Google Scholar] [CrossRef] [PubMed]
- Scott, A.J.; Webb, T.L.; Martyn-St James, M.; Rowse, G.; Weich, S. Improving sleep quality leads to better mental health: A meta-analysis of randomised controlled trials. Sleep Med. Rev. 2021, 60, 101556. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, S.H.; Jang, S.-I.; Park, E.-C. Association Between Sleep Quality and Anxiety in Korean Adolescents. J. Prev. Med. Public Health 2022, 55, 173–181. [Google Scholar] [CrossRef]
- Yu, J.; Rawtaer, I.; Fam, J.; Jiang, M.-J.; Feng, L.; Kua, E.H.; Mahendran, R. Sleep correlates of depression and anxiety in an elderly Asian population. Psychogeriatrics 2016, 16, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, V.; Ornello, R.; Gagliardo, A.; Torrente, A.; Illuminato, E.; Caponnetto, V.; Frattale, I.; Golini, R.; Di Felice, C.; Graziano, F.; et al. Social distancing in chronic migraine during the COVID-19 outbreak: Results from a multicenter observational study. Nutrients 2021, 13, 1361. [Google Scholar] [CrossRef]
- Currò, C.T.; Ciacciarelli, A.; Vitale, C.; La Spina, P.; Toscano, A.; Vita, G.; Trimarchi, G.; Silvestri, R.; Autunno, M. Sleep and sleep-modifying factors in chronic migraine patients during the COVID-19 lockdown. Neurol. Sci. 2022, 43, 6639–6655. [Google Scholar] [CrossRef]
- Pilati, L.; Torrente, A.; Alonge, P.; Vassallo, L.; Maccora, S.; Gagliardo, A.; Pignolo, A.; Iacono, S.; Ferlisi, S.; Di Stefano, V. Sleep and Chronobiology as a Key to Understand Cluster Headache. Neurol. Int. 2023, 15, 497–507. [Google Scholar] [CrossRef]
- Cho, S.J.; Song, T.J.; Chu, M.K. Sleep and Tension-Type Headache. Curr. Neurol. Neurosci. Rep. 2019, 19, 44. [Google Scholar] [CrossRef]
- Cho, S.; Lee, M.J.; Park, H.R.; Kim, S.; Joo, E.Y.; Chung, C.S. Effect of sleep quality on headache-related impact in primary headache disorders. J. Clin. Neurol. 2020, 16, 237–244. [Google Scholar] [CrossRef]
- Lin, Y.-K.; Lin, G.-Y.; Lee, J.-T.; Lee, M.-S.; Tsai, C.-K.; Hsu, Y.-W.; Lin, Y.Z.; Tsai, Y.C.; Yang, F.C. Associations Between Sleep Quality and Migraine Frequency: A Cross-Sectional Case-Control Study. Medicine 2016, 95, e3554. [Google Scholar] [CrossRef] [PubMed]
- Duan, S.; Ren, Z.; Xia, H.; Wang, Z.; Zheng, T.; Liu, Z. Association between sleep quality, migraine and migraine burden. Front. Neurol. 2022, 13, 955298. [Google Scholar] [CrossRef] [PubMed]
- Saçmacı, H.; Tanik, N.; İnan, L.E. Current Perspectives on the Impact of Chronic Migraine on Sleep Quality: A Literature Review. Nat. Sci. Sleep 2022, 14, 1783–1800. [Google Scholar] [CrossRef] [PubMed]
- Buse, D.C.; Rains, J.C.; Pavlovic, J.M.; Fanning, K.M.; Reed, M.L.; Manack Adams, A.; Lipton, R.B. Sleep Disorders Among People with Migraine: Results from the Chronic Migraine Epidemiology and Outcomes (CaMEO) Study. Headache 2019, 59, 32–45. [Google Scholar] [CrossRef]
- Pilati, L.; Torrente, A.; Di Marco, S.; Ferlisi, S.; Notaro, G.; Romano, M.; Alonge, P.; Vassallo, L.; Ferraù, L.; Autunno, M.; et al. Erenumab and Possible CGRP Effect on Chronotype in Chronic Migraine: A Real-Life Study of 12 Months Treatment. J. Clin. Med. 2023, 12, 3585. [Google Scholar] [CrossRef]
- Torrente, A.; Pilati, L.; Di Marco, S.; Maccora, S.; Alonge, P.; Vassallo, L.; Lupica, A.; Coppola, S.; Camarda, C.; Bolognini, N.; et al. OnabotulinumtoxinA Modulates Visual Cortical Excitability in Chronic Migraine: Effects of 12-Week Treatment. Toxins 2023, 15, 23. [Google Scholar] [CrossRef]
- Blumenfeld, A.M.; Tepper, S.J.; Robbins, L.D.; Adams, A.M.; Buse, D.C.; Orejudos, A.; Silberstein, S.D. Effects of onabotulinumtoxinA treatment for chronic migraine on common comorbidities including depression and anxiety. J. Neurol. Neurosurg. Psychiatry 2019, 90, 353–360. [Google Scholar] [CrossRef]
- Aydinlar, E.I.; Dikmen, P.Y.; Kosak, S.; Kocaman, A.S. OnabotulinumtoxinA effectiveness on chronic migraine, negative emotional states and sleep quality: A single-center prospective cohort study. J. Headache Pain 2017, 18, 14–16. [Google Scholar] [CrossRef]
- Demiryurek, B.E.; Ertem, D.H.; Tekin, A.; Ceylan, M.; Aras, Y.G.; Gungen, B.D. Effects of onabotulinumtoxinA treatment on efficacy, depression, anxiety, and disability in Turkish patients with chronic migraine. Neurol. Sci. 2016, 37, 1779–1784. [Google Scholar] [CrossRef]
- Burch, R.C.; Buse, D.C.; Lipton, R.B. Migraine: Epidemiology, Burden, and Comorbidity. Neurol. Clin. 2019, 37, 631–649. [Google Scholar] [CrossRef]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Bendtsen, L.; Sacco, S.; Ashina, M.; Mitsikostas, D.; Ahmed, F.; Pozo-Rosich, P.; Martelletti, P. Guideline on the use of onabotulinumtoxinA in chronic migraine: A consensus statement from the European Headache Federation. J.Headache Pain. 2018, 19, 91. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds CF 3rd Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Kim, S.; Bae, D.W.; Park, S.G.; Park, J.W. The impact of Pain-related emotions on migraine. Sci. Rep. 2021, 11, 577. [Google Scholar] [CrossRef] [PubMed]
- Arnau, R.C.; Meagher, M.W.; Norris, M.P.; Bramson, R. Psychometric evaluation of the Beck Depression Inventory-II with primary care medical patients. Health Psychol. 2001, 20, 112–119. [Google Scholar] [CrossRef]
- Stovner, L.J.; Nichols, E.; Steiner, T.J.; Abd-Allah, F.; Abdelalim, A.; Al-Raddadi, R.M.; Ansha, M.G.; Barac, A.; Bensenor, I.M.; Doan, L.P.; et al. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 954–976. [Google Scholar] [CrossRef]
- Yang, M.; Rendas-Baum, R.; Varon, S.F.; Kosinski, M. Validation of the Headache Impact Test (HIT-6TM) across episodic and chronic migraine. Cephalalgia 2011, 31, 357–367. [Google Scholar] [CrossRef]
- D’Amico, D.; Mosconi, P.; Genco, S.; Usai, S.; Prudenzano, A.M.P.; Grazzi, L.; Leone, M.; Puca, F.M.; Bussone, G. The Migraine Disability Assessment (MIDAS) questionnaire: Translation and reliability of the Italian version. Cephalalgia 2001, 21, 947–952. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variable | N | % |
| Patients | 42 | 100.0 |
| Female | 32 | 76.2 |
| Male | 10 | 23.8 |
| Migraine without aura | 40 | 95.2 |
| Migraine with aura | 2 | 4.8 |
| Variable | Mean | SD |
| Age | 49.3 | 10.2 |
| Years from migraine onset | 24.2 | 12.9 |
| Type of acute medication | N1 | %1 |
| Triptans | 27 | 64.3 |
| NSAIDs | 15 | 35.7 |
| Association of indomethacin 25 mg, caffeine 75 mg, and prochlorperazine 2 mg | 7 | 16.7 |
| Betamethasone 4 mg 2 | 3 | 7.1 |
| Acetaminophen | 2 | 4.8 |
| Variable | t0 Mean (SD) | t1 Mean (SD) | p Value |
|---|---|---|---|
| MMDs | 20.6 (6.0) | 13.6 (6.2) | <0.001 |
| MADs | 18.4 (7.7) | 15.5 (10.1) | 0.053 |
| Variable | t0 Mean (SD) | t1 Mean (SD) | p Value |
|---|---|---|---|
| PSQI | 11.0 (5.0) | 9.8 (4.6) | 0.277 |
| Variable | t0 Mean (SD) | t1 Mean (SD) | p Value |
|---|---|---|---|
| BDI-II | 16.7 (10.2) | 15.7 (10.3) | 0.678 |
| HADS-a | 10.3 (4.8) | 9.3 (5.5) | 0.492 |
| HADS-d | 7.2 (3.9) | 7.1 (5.0) | 0.901 |
| Variable | t0 Mean (SD) | t1 Mean (SD) | p Value |
|---|---|---|---|
| HIT-6 | 56.4 (12.5) | 53.7 (17.5) | 0.520 |
| MIDAS | 86.8 (64.4) | 59.3 (42.9) | 0.033 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torrente, A.; Alonge, P.; Pilati, L.; Gagliardo, A.; Vassallo, L.; Di Stefano, V.; Lupica, A.; Quartana, I.; Viticchi, G.; Silvestrini, M.; et al. Effects of a Single Session of OnabotulinumtoxinA Therapy on Sleep Quality and Psychological Measures: Preliminary Findings in a Population of Chronic Migraineurs. Toxins 2023, 15, 527. https://doi.org/10.3390/toxins15090527
Torrente A, Alonge P, Pilati L, Gagliardo A, Vassallo L, Di Stefano V, Lupica A, Quartana I, Viticchi G, Silvestrini M, et al. Effects of a Single Session of OnabotulinumtoxinA Therapy on Sleep Quality and Psychological Measures: Preliminary Findings in a Population of Chronic Migraineurs. Toxins. 2023; 15(9):527. https://doi.org/10.3390/toxins15090527
Chicago/Turabian StyleTorrente, Angelo, Paolo Alonge, Laura Pilati, Andrea Gagliardo, Lavinia Vassallo, Vincenzo Di Stefano, Antonino Lupica, Irene Quartana, Giovanna Viticchi, Mauro Silvestrini, and et al. 2023. "Effects of a Single Session of OnabotulinumtoxinA Therapy on Sleep Quality and Psychological Measures: Preliminary Findings in a Population of Chronic Migraineurs" Toxins 15, no. 9: 527. https://doi.org/10.3390/toxins15090527
APA StyleTorrente, A., Alonge, P., Pilati, L., Gagliardo, A., Vassallo, L., Di Stefano, V., Lupica, A., Quartana, I., Viticchi, G., Silvestrini, M., Bartolini, M., Camarda, C., & Brighina, F. (2023). Effects of a Single Session of OnabotulinumtoxinA Therapy on Sleep Quality and Psychological Measures: Preliminary Findings in a Population of Chronic Migraineurs. Toxins, 15(9), 527. https://doi.org/10.3390/toxins15090527