Botulinum Toxin—A Current Place in the Treatment of Chronic Migraine and Other Primary Headaches


Abstract
:1. Introduction
2. Clinical History of Botulinum Toxin
3. Tension-Type Headache
4. The Use of Botulinum Toxin for the Treatment of Cluster Headache
5. Botulinum Toxin in the Management of Chronic Migraine
6. Mode of Action of ONA-BoNTA
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Headache Classification Commitee of the International Headache Society, International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [CrossRef] [PubMed]
- Bahra, A.; Evans, R.W. The secondary Headaches. Cephalalgia 2021, 41, 427–430. [Google Scholar] [CrossRef] [PubMed]
- Steiner, T.J.; Stovner, L.J.; Vos, T. GBD 2015: Migraine is the third cause of disability in under 50s. J. Headache Pain 2016, 17, 104. [Google Scholar] [CrossRef] [PubMed]
- Bigal, M.E.; Lipton, R.B. Modifiable risk factors for migraine progression. Headache 2006, 46, 1334–1343. [Google Scholar] [CrossRef] [PubMed]
- Burch, R.C.; Buse, D.C.; Lipton, R.B. Migraine: Epidemiology, Burden and Comorbidity. Neurol. Clin. 2019, 37, 631–649. [Google Scholar] [CrossRef]
- Aurora, S.K.; Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F.; PREEMPT 1 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PRREMPT 1 trial. Cephalalgia 2010, 30, 793–803. [Google Scholar] [CrossRef]
- Diener, H.C.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; DeGryse, R.E.; Lipton, R.B.; Silberstein, S.D.; Brin, M.F.; PREEMPT 2 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PRREMPT 2 trial. Cephalalgia 2010, 30, 804–814. [Google Scholar] [CrossRef]
- Becker, W.J. Botulinum Toxin in the Treatment of Headache. Toxins 2020, 12, 803. [Google Scholar] [CrossRef]
- Ramachandran, R.; Yaksh, T.L. Therapeutic use of botulinum toxin in migraine: Mechanisms of action. Br. J. Pharmacol. 2014, 171, 4177–4192. [Google Scholar] [CrossRef]
- Robertson, C.E.; Garza, I. Critical analysis of the use of onatobotulinumtoxinA (botulinum toxin type A) in migraine. Neuropsychiatr. Dis. Treat. 2012, 8, 35–48. [Google Scholar] [CrossRef] [Green Version]
- Kahriman, A.; Zhu, S. Migraine and Tension-Type Headache. Semin. Neurol. 2018, 38, 608–618. [Google Scholar] [CrossRef]
- Pihut, M.; Ferendiuk, E.; Szewczyk, M.; Kasprzyk, K.; Wieckiewicz, M. The efficiency of botulinum toxin type A for the treatment of masseter muscle pain in patients with temporomandibular joint dysfunction and tension-type headache. J. Headache Pain 2016, 17, 29. [Google Scholar] [CrossRef]
- Ashkenazi, A.; Blumenfeld, A. OnabotulinumtoxinA for the treatment of headache. Headache 2013, 53, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Roland, S.B.; Pripp, A.H.; Msomphora, M.R.; Kvarstein, G. The efficacy of botulinum toxin A treatment for tension-type or cervivogenic headache: A systematic review and meta-analysis of randomized, placebo-controlled trials. Scand. J. Pain 2021, 21, 635–652. [Google Scholar] [CrossRef] [PubMed]
- Gaul, C.; Holle-Lee, D.; Straube, A. Botulinum toxin type A in headache treatment: Established and experimental indications. Nervenarzt 2016, 87, 853–859. [Google Scholar] [CrossRef]
- Lipton, R.B.; Cady, R.K.; Stewart, W.F.; Wilks, K.; Hall, C. Diagnostic lessons from the spectrum study. Neurology 2002, 14, 27–31. [Google Scholar] [CrossRef] [PubMed]
- May, A.; Scwedt, T.J.; Magis, D.; Pozo-Rosich, P.; Evers, S.; Wang, S.J. Cluster headache. Nat. Rev. Dis. Primers 2018, 1, 18006. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.; May, A. Diagnosis, pathophysiology, and management of cluster headache. Lancet Neurol. 2018, 17, 75–83. [Google Scholar] [CrossRef]
- Freund, B.; Kotchetkov, I.S.; Rao, A. The Efficacy of Botulinum Toxin in Cluster Headache: A Systematic Review. J. Oral Facial Pain Headache 2020, 34, 129–134. [Google Scholar] [CrossRef]
- Bratbak, D.F.; Nordgard, S.; Stovner, L.J. Pilot study of sphenopalatine injection of onabotulinumtoxinA for the treatment of itractable chronic cluster headache. Cephalalgia 2016, 36, 503–509. [Google Scholar] [CrossRef] [Green Version]
- Crespi, J.; Bratbak, D.; Dodick, D.W. Open-Label, Multi-Dose, Pilot Safety Study of Injection of OnabotulinumtoxinA toward the Otic Ganglion for the Treatment of Intractable Chroni Cluster Headache. Headache 2020, 60, 1632–1634. [Google Scholar] [CrossRef] [PubMed]
- Adams, A.M.; Serrano, D.; Buse, D.C.; Reed, M.L.; Marske, V.; Fanning, K.M.; Lipton, R.B. The impact of chronic migraine: The Chronic Migraine Epidemiology and Outcomes (CaMEO) Study methods and baseline results. Cephalalgia 2015, 35, 563–578. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.F. OnabotulinumtoxinA injection in the treatment of chronic migraine. Prog. Brain Res. 2020, 255, 171–206. [Google Scholar] [PubMed]
- Jackson, J.; Kuriyama, A.; Hayashino, Y. Botulinum toxin A for prophylactic treatment of migraine and tension headaches in adults: A meta-analysis. J. Am. Med. Assoc. 2012, 307, 1736–1745. [Google Scholar]
- Silberstein, S.D.; Stark, S.R.; Lucas, S.M.; Christie, S.N.; Degryse, R.E.; Turkel, C.C. Botulinum toxin type A for the prophylactic treatment of chronic daily headache: A randomized, double-blind, placebo-controlled trial. Mayo Clin. Proc. 2005, 80, 1126–1137. [Google Scholar] [CrossRef]
- Vo, A.; Satori, R.; Jabbari, B.; Green, J.; Killgore, W.D.; Labutta, R.; Campbell, W.W. Botulinum toxin type-A in the prevention of migraine: A double-blind controlled trial. Aviat. Space Environ. Med. 2007, 78, 113–118. [Google Scholar]
- Blumenfeld, A.; Silberstein, S.D.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; Binder, W.J. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache 2010, 50, 1406–1418. [Google Scholar] [CrossRef]
- Dodick, D.W.; Mauskop, A.; Elkind, A.H.; DeGryse, R.E.; Brin, M.F.; Silberstein, S.D. Botulinum toxin type a for the prophylaxis of chronic daily headache: Subgroup analysis of patients not receiving other prophylactic medications: A randomized double-blind, placebo-cotrolled study. Headache 2005, 45, 315–324. [Google Scholar] [CrossRef]
- Rummel, A. The long journey of botulinum neurotoxins into the synapse. Toxicon 2015, 107, 9–24. [Google Scholar] [CrossRef]
- Burstein, R.; Blumenfeld, A.M.; Silberstein, S.D. Mechanism of Action of OnabotulinumtoxinA in Chronic Migraine: A Narrative Review. Headache 2020, 60, 1259–1272. [Google Scholar] [CrossRef]
- Matak, I.; Lacković, Z. Botulinum toxin A, brain and pain. Prog. Neurobiol. 2014, 119–120, 39–59. [Google Scholar] [CrossRef] [PubMed]
- Ferillo, M.; Migliaro, M.; Marotta, N.; Fortunato, F.; Bindi, M.; Pezzotti, F.; Ammendolia, A.; Giudice, A.; Foglio Bonda, P.L.; de Sira, A. Temporomandibular disorders and neck pain in primary headache patients: A retrospective machine learning study. Acta Odontol. Scand. 2022, 29, 1–7. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
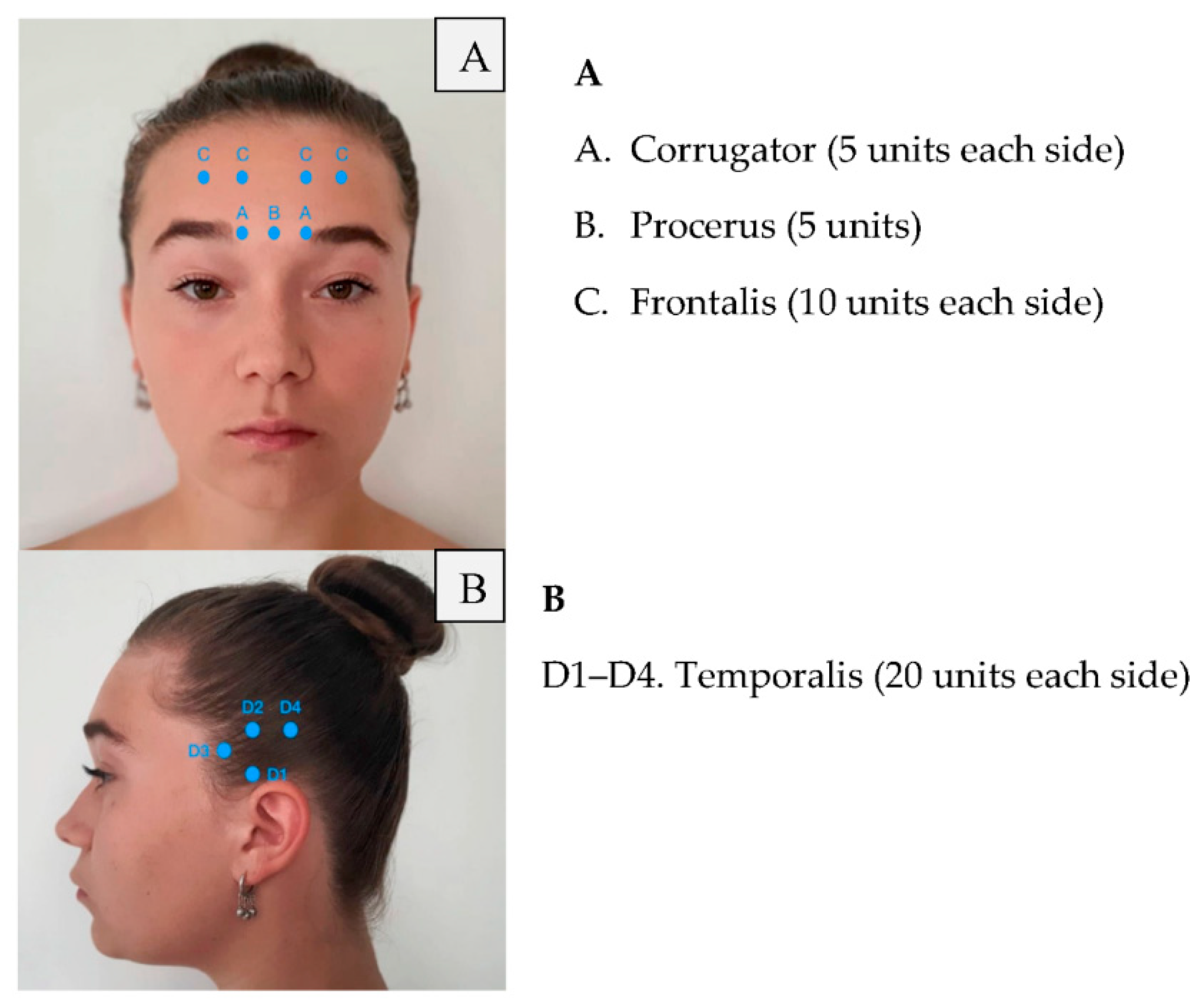
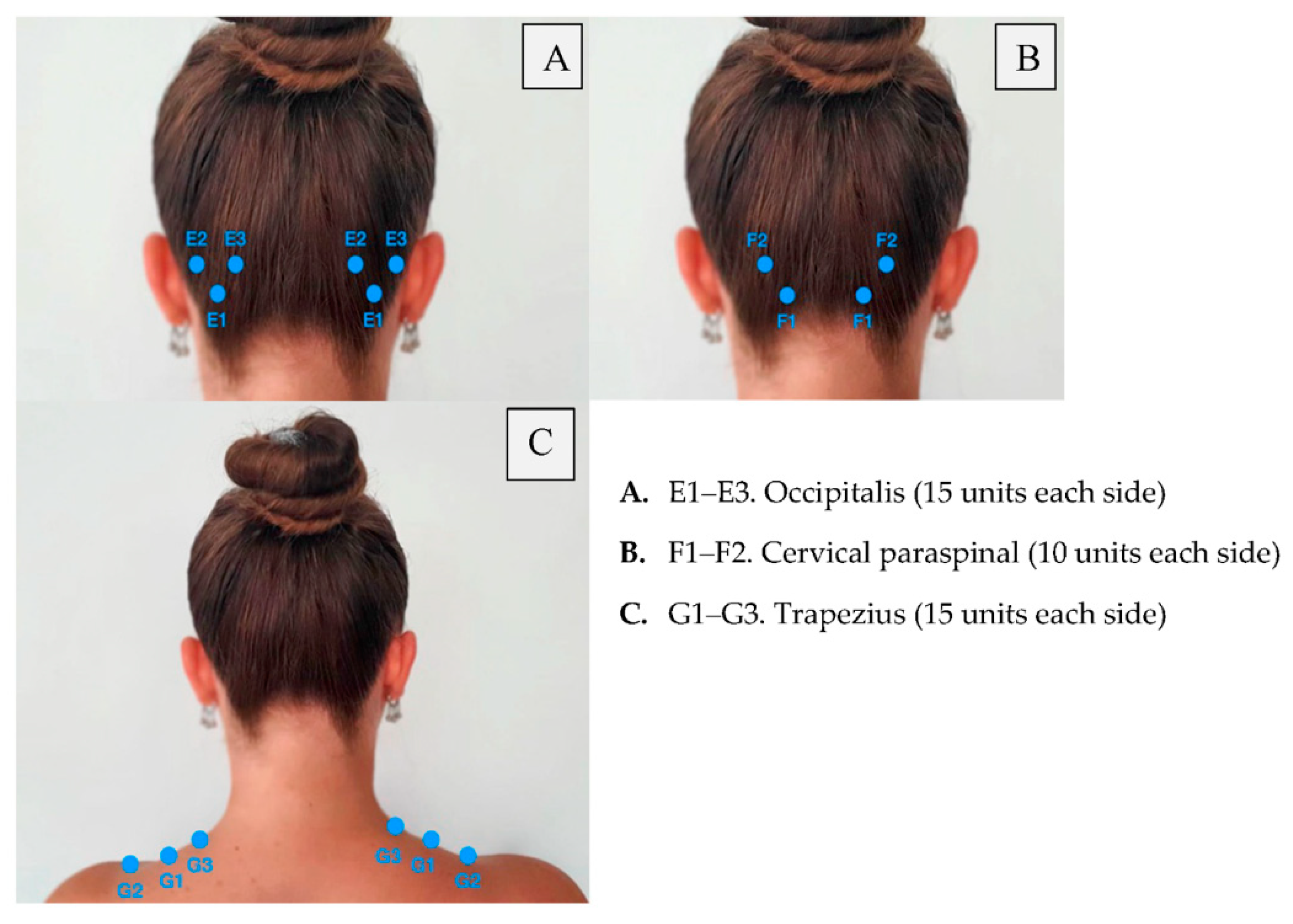
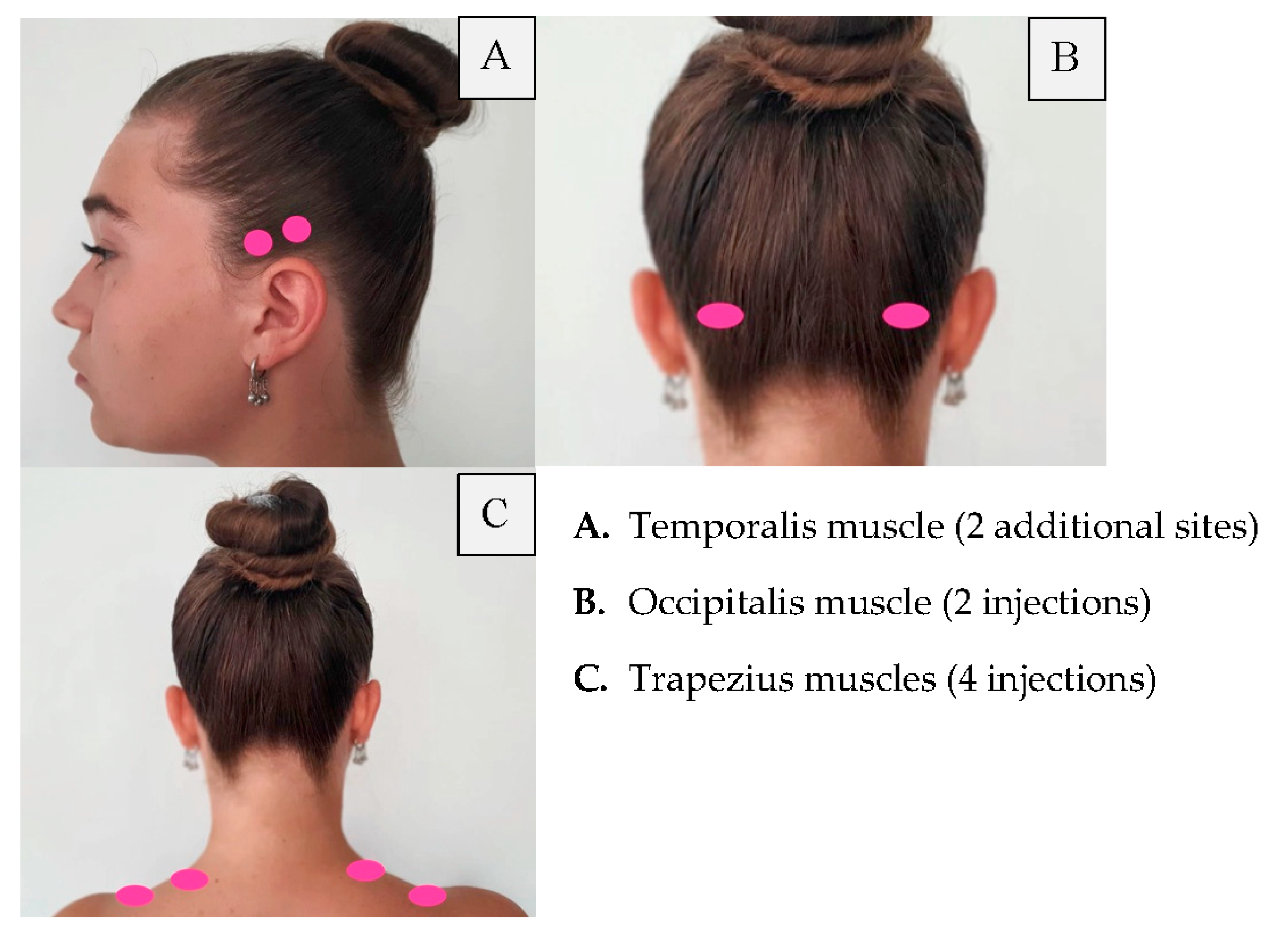
| Area of Injection | Recommended Dose |
|---|---|
| Frontalis Corrugator Procerus Occipitalis Temporalis Trapezius Cervical paraspinal muscle group | 20 units (4 sites) 10 units (2 sites) 5 units (1 site) 30 units (6 sites) + 10 units in 2 sites (follow the pain areas—optional injections) 40 units (8 sites) + 10 units in 2 sites (follow the pain areas—optional injections) 30 units (6 sites) + 20 units in 4 sites (follow the pain areas—optional injections) 20 units (4 sites) Summary: 155–195 units |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kępczyńska, K.; Domitrz, I. Botulinum Toxin—A Current Place in the Treatment of Chronic Migraine and Other Primary Headaches. Toxins 2022, 14, 619. https://doi.org/10.3390/toxins14090619
Kępczyńska K, Domitrz I. Botulinum Toxin—A Current Place in the Treatment of Chronic Migraine and Other Primary Headaches. Toxins. 2022; 14(9):619. https://doi.org/10.3390/toxins14090619
Chicago/Turabian StyleKępczyńska, Katarzyna, and Izabela Domitrz. 2022. "Botulinum Toxin—A Current Place in the Treatment of Chronic Migraine and Other Primary Headaches" Toxins 14, no. 9: 619. https://doi.org/10.3390/toxins14090619
APA StyleKępczyńska, K., & Domitrz, I. (2022). Botulinum Toxin—A Current Place in the Treatment of Chronic Migraine and Other Primary Headaches. Toxins, 14(9), 619. https://doi.org/10.3390/toxins14090619