Safety Profile and Lack of Immunogenicity of IncobotulinumtoxinA in Pediatric Spasticity and Sialorrhea: A Pooled Analysis

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Results
2.1. Demographics
2.2. Safety: Pediatric Spasticity and Sialorrhea
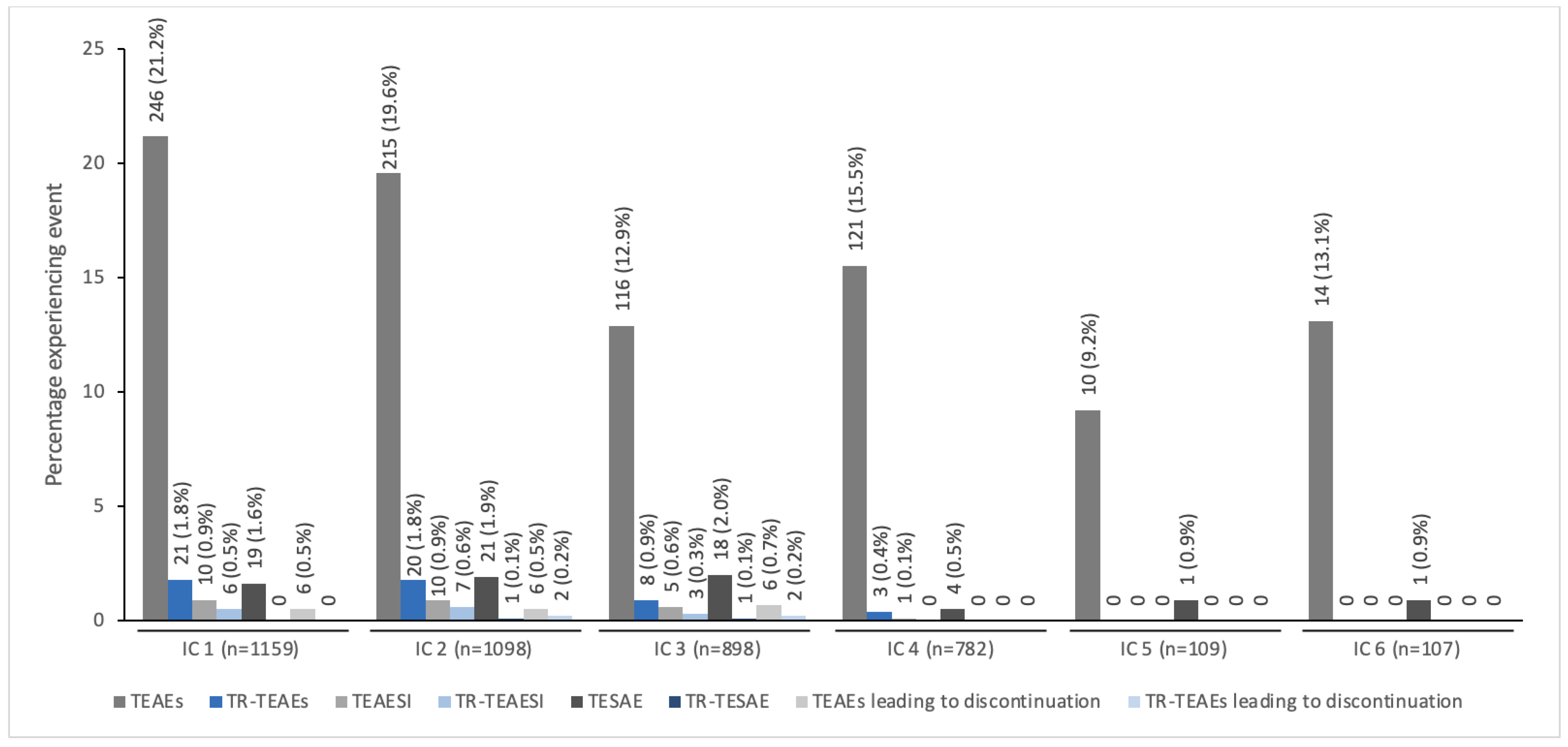
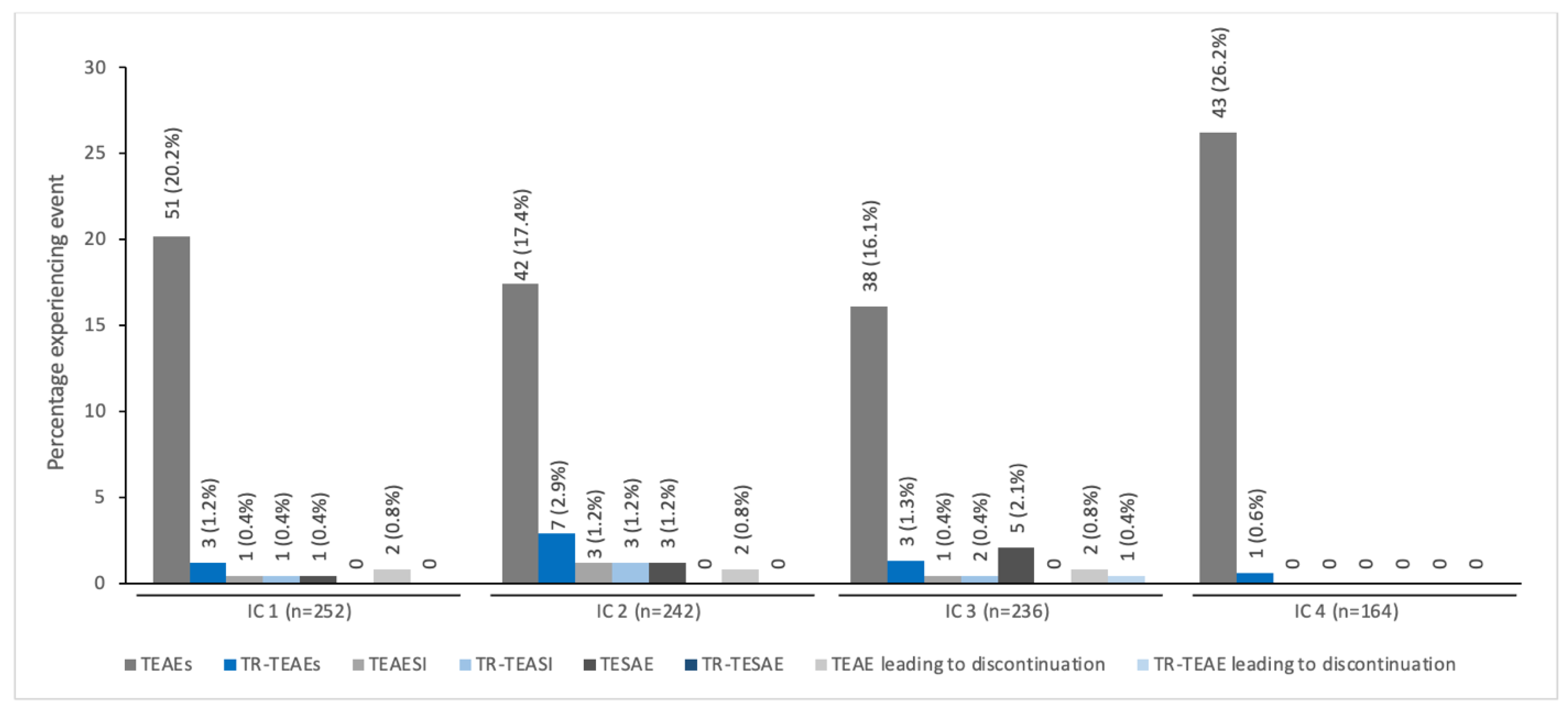
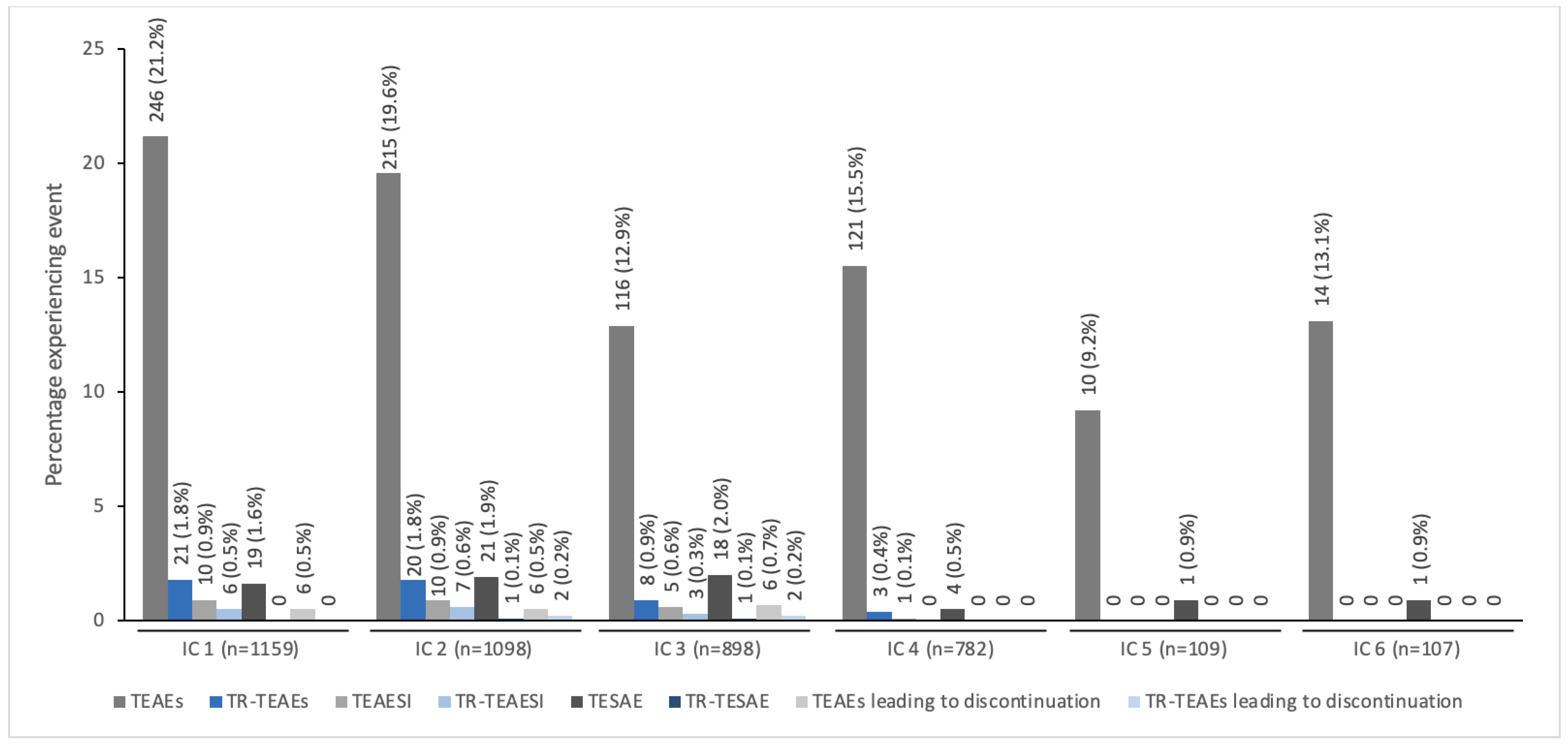
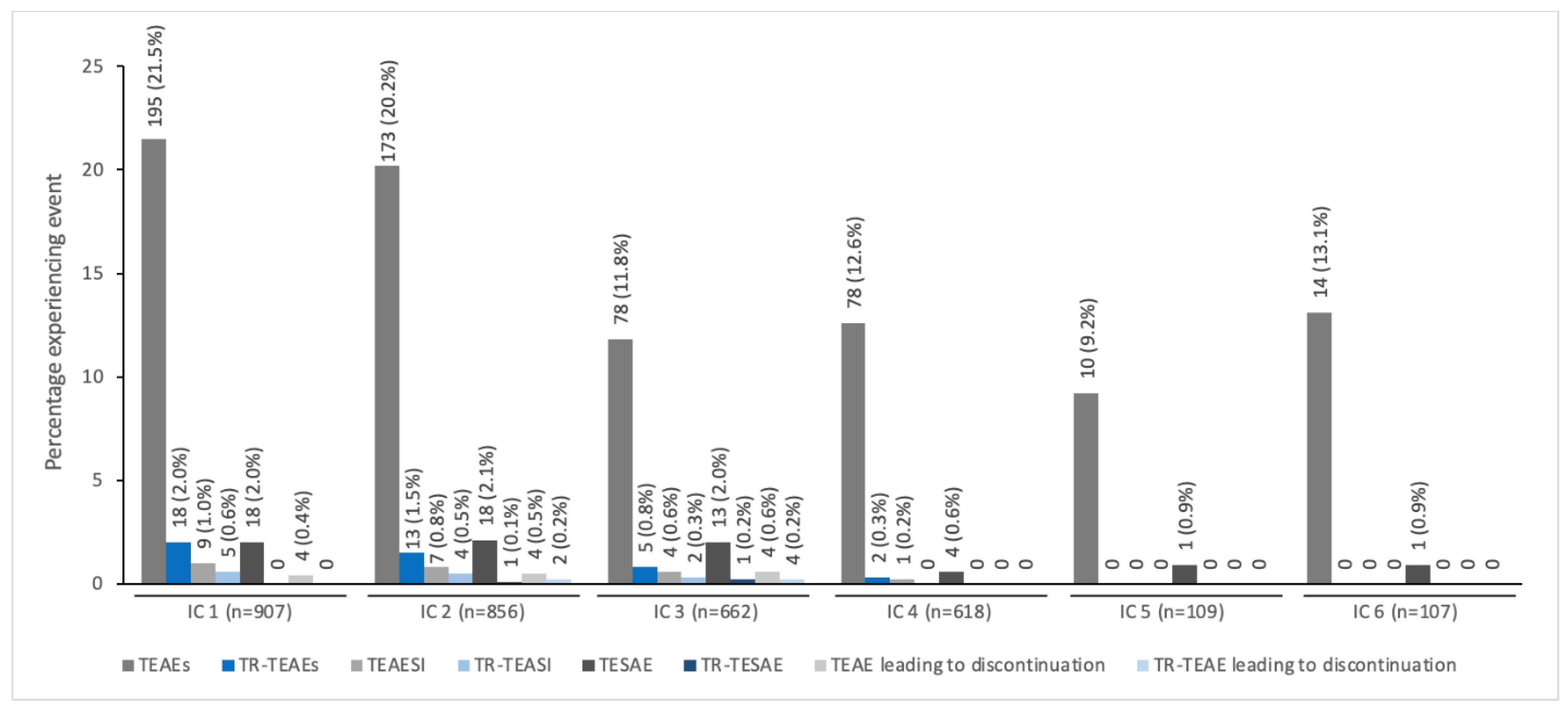
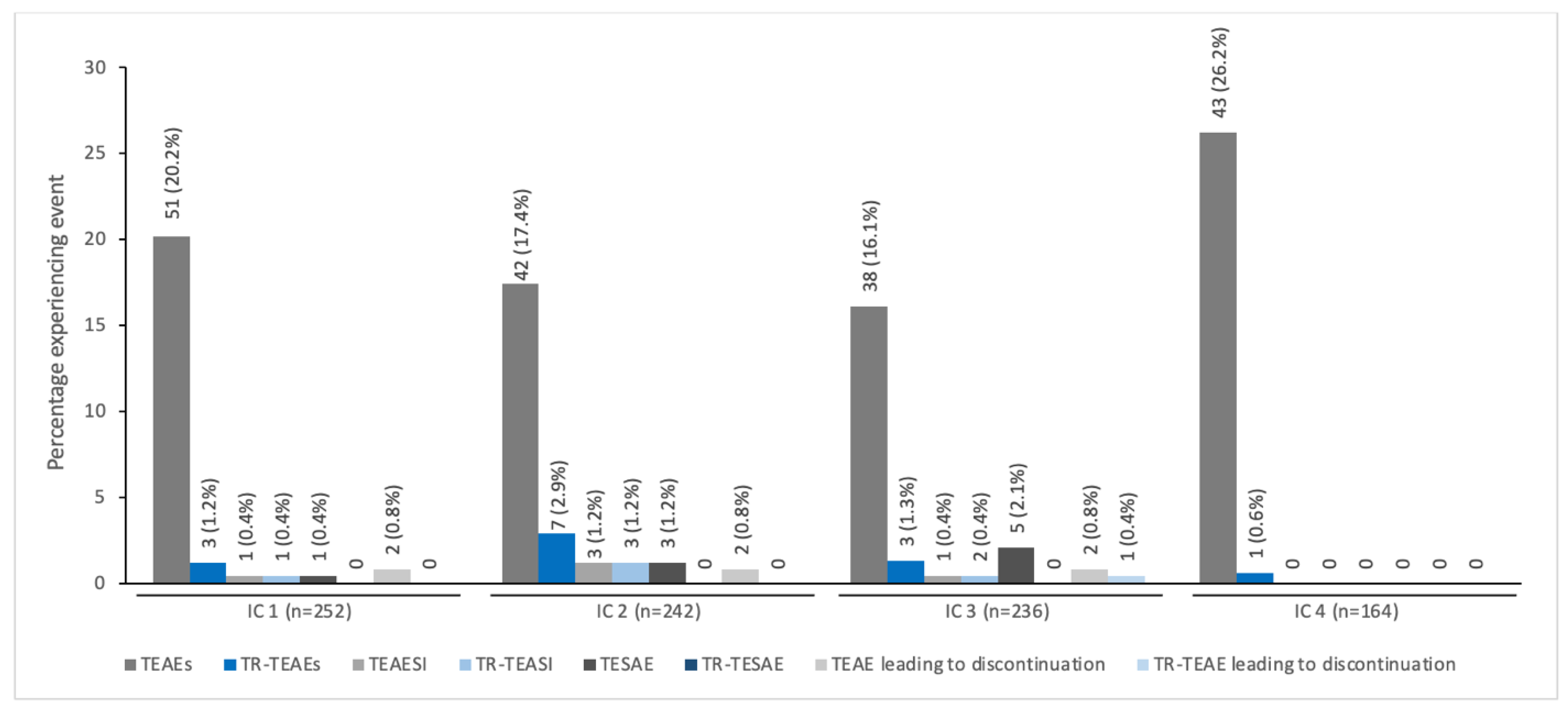
2.3. TEAEs by IC
2.4. Most Common TEAEs by Indication
2.4.1. Spasticity
2.4.2. Sialorrhea
2.5. Immunogenicity
3. Discussion
Strengths and Weaknesses
4. Conclusions
5. Materials and Methods
5.1. Participants
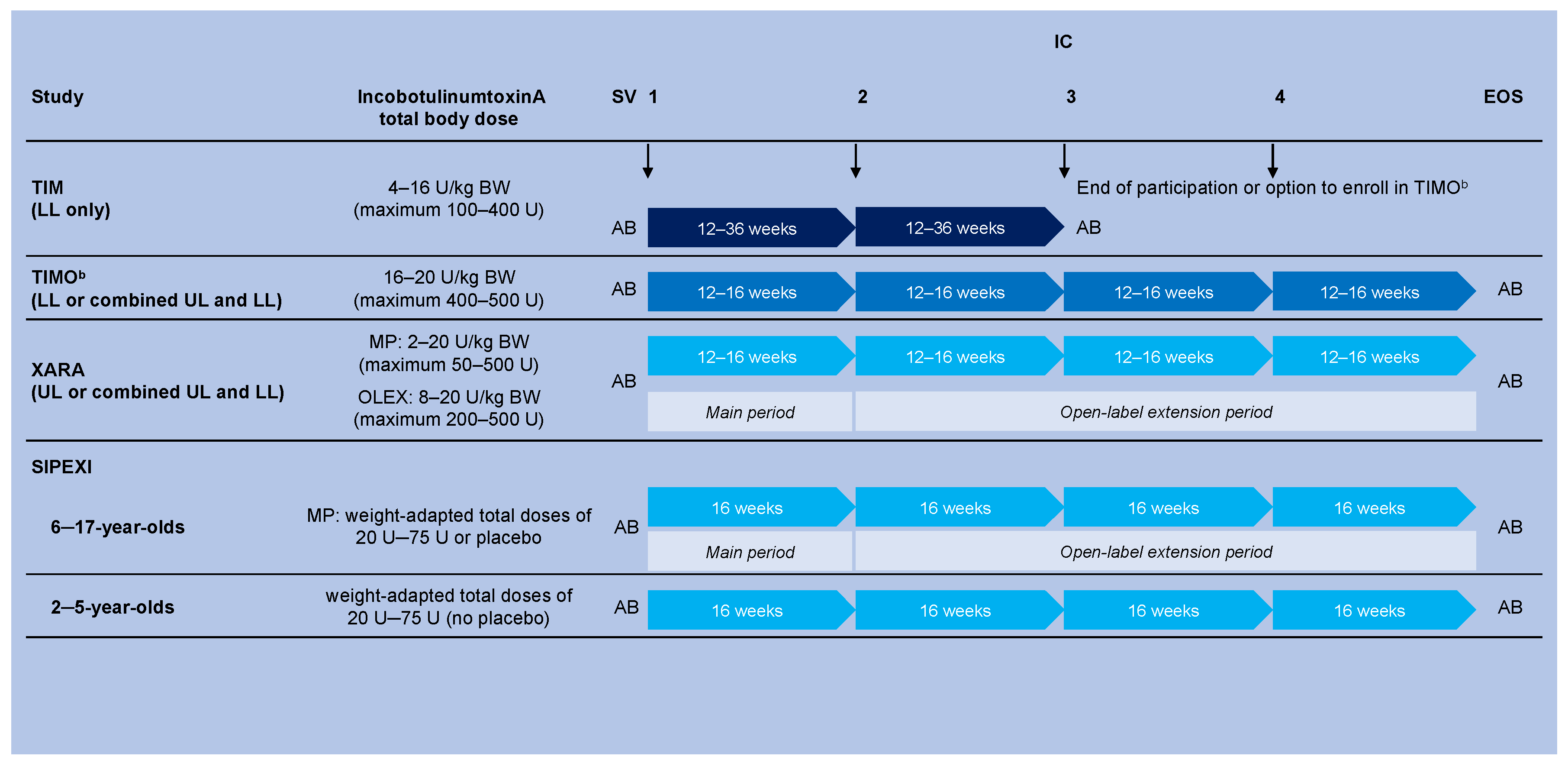
5.2. Trial Designs and Treatment
5.2.1. Spasticity
5.2.2. Sialorrhea
5.3. Standard Protocol Approvals, Registrations, and Patient Consent
5.4. Assessments
5.4.1. Safety
5.4.2. Antibody Measurements
5.4.3. Statistics
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hareb, F.; Bertoncelli, C.M.; Rosello, O.; Rampal, V.; Solla, F. Botulinum toxin in children with cerebral palsy: An update. Neuropediatrics 2020, 51, 1–5. [Google Scholar] [CrossRef]
- Sätilä, H. Over 25 years of pediatric botulinum toxin treatments: What have we learned from injection techniques, doses, dilutions, and recovery of repeated injections? Toxins 2020, 12, 440. [Google Scholar] [CrossRef]
- Hung, S.A.; Liao, C.L.; Lin, W.P.; Hsu, J.C.; Guo, Y.H.; Lin, Y.C. Botulinum toxin injections for treatment of drooling in children with cerebral palsy: A systematic review and meta-analysis. Children 2021, 8, 1089. [Google Scholar] [CrossRef]
- Peeraully, R.; Lam, C.; Mediratta, N.; Patel, R.; Williams, A.; Shenoy, M.; Fraser, N. Intradetrusor injection of botulinum toxin A in children: A 10-year single centre experience. Int. Urol. Nephrol. 2019, 51, 1321–1327. [Google Scholar] [CrossRef]
- Mahan, M.; Engel, J.M. The resurgence of botulinum toxin injection for strabismus in children. Curr. Opin. Ophthalmol. 2017, 28, 460–464. [Google Scholar] [CrossRef]
- Carr, W.W.; Jain, N.; Sublett, J.W. Immunogenicity of botulinum toxin formulations: Potential therapeutic implications. Adv. Ther. 2021, 38, 5046–5064. [Google Scholar] [CrossRef]
- Riva, A.; Amadori, E.; Vari, M.S.; Spalice, A.; Belcastro, V.; Viri, M.; Capodiferro, D.; Romeo, A.; Verrotti, A.; Delphi panel experts’ group; et al. Impact and management of drooling in children with neurological disorders: An Italian Delphi consensus. Ital. J. Pediatr. 2022, 48, 118. [Google Scholar] [CrossRef]
- Heinen, F.; Desloovere, K.; Schroeder, A.S.; Berweck, S.; Borggraefe, I.; van Campenhout, A.; Andersen, G.L.; Aydin, R.; Becher, J.G.; Bernert, G.; et al. The updated European Consensus 2009 on the use of Botulinum toxin for children with cerebral palsy. Eur. J. Paediatr. Neurol. 2010, 14, 45–66. [Google Scholar] [CrossRef]
- Bellows, S.; Jankovic, J. Immunogenicity associated with botulinum toxin treatment. Toxins 2019, 11, 491. [Google Scholar] [CrossRef]
- Frevert, J. Pharmaceutical, biological, and clinical properties of botulinum neurotoxin type A products. Drugs R D 2015, 15, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Hefter, H.; Brauns, R.; Ürer, B.; Rosenthal, D.; Albrecht, P. Effective long-term treatment with incobotulinumtoxin (Xeomin®) without neutralizing antibody induction: A monocentric, cross-sectional study. J. Neurol. 2020, 267, 1340–1347. [Google Scholar] [CrossRef]
- Samadzadeh, S.; Ürer, B.; Brauns, R.; Rosenthal, D.; Lee, J.I.; Albrecht, P.; Hefter, H. Clinical implications of difference in antigenicity of different botulinum neurotoxin type A preparations: Clinical take-home messages from our research pool and literature. Toxins 2020, 12, 499. [Google Scholar] [CrossRef]
- Car, H.; Bogucki, A.; Bonikowski, M.; Dec-Ćwiek, M.; Drużdż, A.; Koziorowski, D.; Rudzińska-Bar, M.; Sarzyńska-Długosz, I.; Sławek, J. Botulinum toxin type-A preparations are not the same medications—Basic science (Part 1). Neurol. Neurochir. Pol. 2021, 55, 133–140. [Google Scholar] [CrossRef]
- Albrecht, P.; Jansen, A.; Lee, J.I.; Moll, M.; Ringelstein, M.; Rosenthal, D.; Bigalke, H.; Aktas, O.; Hartung, H.P.; Hefter, H. High prevalence of neutralizing antibodies after long-term botulinum neurotoxin therapy. Neurology 2019, 92, e48–e54. [Google Scholar] [CrossRef]
- Lacroix-Desmazes, S.; Mouly, S.M.; Popoff, M.-R.; Colosimo, C. Systematic analysis of botulinum neurotoxin type A immunogenicity in clinical studies. Basal Ganglia. 2017, 9, 12–17. [Google Scholar] [CrossRef]
- Merz Pharmaceuticals, L.L.C. Xeomin-Incobotulinumtoxina Injection. Package Insert. April 2021. Available online: https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=ccdc3aae-6e2d-4cd0-a51c-8375bfee9458&type=display (accessed on 10 March 2022).
- Dabrowski, E.; Chambers, H.G.; Gaebler-Spira, D.; Banach, M.; Kaňovský, P.; Dersch, H.; Althaus, M.; Geister, T.L.; Heinen, F. IncobotulinumtoxinA efficacy/safety in upper-limb spasticity in pediatric cerebral palsy: Randomized controlled trial. Pediatr. Neurol. 2021, 123, 10–20. [Google Scholar] [CrossRef]
- Heinen, F.; Kaňovský, P.; Schroeder, A.S.; Chambers, H.G.; Dabrowski, E.; Geister, T.L.; Hanschmann, A.; Martinez-Torres, F.J.; Pulte, I.; Banach, M.; et al. IncobotulinumtoxinA for the treatment of lower-limb spasticity in children and adolescents with cerebral palsy: A Phase 3 study. J. Pediatr. Rehabil. Med. 2021, 14, 183–197. [Google Scholar] [CrossRef]
- Kaňovský, P.; Heinen, F.; Schroeder, A.S.; Chambers, H.G.; Dabrowski, E.; Geister, T.L.; Hanschmann, A.; Martinez-Torres, F.J.; Pulte, I.; Banach, M.; et al. Safety and efficacy of repeat long-term incobotulinumtoxinA treatment for lower limb or combined upper/lower limb spasticity in children with cerebral palsy. J. Pediatr. Rehabil. Med. 2022, 15, 113–127. [Google Scholar] [CrossRef]
- Berweck, S.; Bonikowski, M.; Kim, H.; Althaus, M.; Flatau-Baqué, B.; Mueller, D.; Banach, M.D. Placebo-controlled clinical trial of incobotulinumtoxinA for sialorrhea in children: SIPEXI. Neurology 2021, 97, e1425–e1436, PMCID:PMC8520391. [Google Scholar] [CrossRef]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef]
- Dimitrova, R.; Kim, H.; Meilahn, J.; Chambers, H.G.; Racette, B.A.; Bonikowski, M.; Park, E.S.; McCusker, E.; Liu, C.; Brin, M.F. Efficacy and safety of onabotulinumtoxinA with standardized physiotherapy for the treatment of pediatric lower limb spasticity: A randomized, placebo-controlled, phase III clinical trial. NeuroRehabilitation 2022, 50, 33–46. [Google Scholar] [CrossRef]
- Szpindel, A.; Myers, K.A.; Ng, P.; Dorais, M.; Koclas, L.; Pigeon, N.; Shevell, M.; Oskoui, M. Epilepsy in children with cerebral palsy: A data linkage study. Dev. Med. Child Neurol. 2022, 64, 259–265. [Google Scholar] [CrossRef]
- León-Valenzuela, A.; Palacios, J.S.; Del Pino Algarrada, R. IncobotulinumtoxinA for the treatment of spasticity in children with cerebral palsy—A retrospective case series focusing on dosing and tolerability. BMC Neurol. 2020, 20, 126. [Google Scholar] [CrossRef]
- Dressler, D.; Paus, S.; Seitzinger, A.; Gebhardt, B.; Kupsch, A. Long-term efficacy and safety of incobotulinumtoxinA injections in patients with cervical dystonia. J. Neurol. Neurosurg. Psychiatry 2013, 84, 1014–1019. [Google Scholar] [CrossRef]
- Wissel, J.; Bensmail, D.; Ferreira, J.J.; Molteni, F.; Satkunam, L.; Moraleda, S.; Rekand, T.; McGuire, J.; Scheschonka, A.; Flatau-Baqué, B.; et al. Safety and efficacy of incobotulinumtoxinA doses up to 800 U in limb spasticity: The TOWER study. Neurology 2017, 88, 1321–1328, PMCID:PMC5379931. [Google Scholar] [CrossRef]
- Jost, W.H.; Friedman, A.; Michel, O.; Oehlwein, C.; Sławek, J.; Bogucki, A.; Ochudlo, S.; Banach, M.; Pagan, F.; Flatau-Baqué, B.; et al. SIAXI: Placebo-controlled, randomized, double-blind study of incobotulinumtoxinA for sialorrhea. Neurology 2019, 92, e1982–e1991, PMCID:PMC6511076. [Google Scholar] [CrossRef]
- Coleman, W.P., 3rd; Sattler, G.; Weissenberger, P.; Hast, M.A.; Hanschmann, A. Safety of incobotulinumtoxinA in the treatment of facial lines: Results from a pooled analysis of randomized, prospective, controlled clinical studies. Dermatol. Surg. 2017, 43 (Suppl. 3), S293–S303. [Google Scholar] [CrossRef]
- Koman, L.A.; Brashear, A.; Rosenfeld, S.; Chambers, H.; Russman, B.; Rang, M.; Root, L.; Ferrari, E.; Garcia de Yebenes Prous, J.; Smith, B.P.; et al. Botulinum toxin type a neuromuscular blockade in the treatment of equinus foot deformity in cerebral palsy: A multicenter, open-label clinical trial. Pediatrics 2001, 108, 1062–1071. [Google Scholar] [CrossRef]
- Oshima, M.; Deitiker, P.; Hastings-Ison, T.; Aoki, K.R.; Graham, H.K.; Atassi, M.Z. Antibody responses to botulinum neurotoxin type A of toxin-treated spastic equinus children with cerebral palsy: A randomized clinical trial comparing two injection schedules. J. Neuroimmunol. 2017, 306, 31–39. [Google Scholar] [CrossRef]
- Delgado, M.R.; Bonikowski, M.; Carranza-Del Río, J.; Dursun, N.; Bonikowski, M.; Aydin, R.; Maciag-Tymecka, I.; Oleszek, J.; Dabrowski, E.; Grandoulier, A.S.; et al. Safety and efficacy of repeat open-label abobotulinumtoxinA treatment in pediatric cerebral palsy. J. Child Neurol. 2017, 32, 1058–1064. [Google Scholar] [CrossRef] [Green Version]
- Delgado, M.R.; Tilton, A.; Carranza-Del Río, J.; Dursun, N.; Bonikowski, M.; Aydin, R.; Maciag-Tymecka, I.; Oleszek, J.; Dabrowski, E.; Grandoulier, A.S.; et al. Efficacy and safety of abobotulinumtoxinA for upper limb spasticity in children with cerebral palsy: A randomized repeat-treatment study. Dev. Med. Child Neurol. 2021, 63, 592–600, PMCID:PMC8048784. [Google Scholar] [CrossRef]
- Frevert, J.; Dressler, D. Clinical Relevance of Immunoresistance to Botulinum Therapy. In Botulinum Toxin Therapy Manual for Dystonia and Spasticity; Rosales, R.L., Dressler, D., Eds.; IntechOpen: London, UK, 2016. [Google Scholar] [CrossRef]
- Benecke, R. Clinical relevance of botulinum toxin immunogenicity. BioDrugs 2012, 26, e1–e9. [Google Scholar] [CrossRef]
- Frevert, J. Content of botulinum neurotoxin in Botox®/Vistabel®, Dysport®/Azzalure®, and Xeomin®/Bocouture®. Drugs R D 2010, 10, 67–73. [Google Scholar] [CrossRef]
- Kerscher, M.; Wanitphakdeedecha, R.; Trindade de Almeida, A.; Maas, C.; Frevert, J. IncobotulinumtoxinA: A highly purified and precisely manufactured botulinum neurotoxin type A. J. Drugs Dermatol. 2019, 18, 52–57. [Google Scholar]
- Rahman, E.; Alhitmi, H.K.; Mosahebi, A. Immunogenicity to botulinum toxin type A: A systematic review with meta-analysis across therapeutic indications. Aesthet. Surg. J. 2022, 42, 106–120. [Google Scholar] [CrossRef]
- Bonikowski, M.; Sławek, J. Safety and efficacy of Botulinum toxin type A preparations in cerebral palsy—An evidence-based review. Neurol. Neurochir. Pol. 2021, 55, 158–164. [Google Scholar] [CrossRef]
- FDA. Center for Drug Evaluation and Research Administration, U.S. Food and Drug Administration. Guidance for Industry: Immunogenicity Assessment for Therapeutic Protein Products. In FDA.; 2014. Available online: https://www.fda.gov/media/85017/download (accessed on 17 March 2022).
- EMA. European Medicines Agency. Guideline on Immunogenicity Assessment of Therapeutic Proteins. EMA. 2017. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-immunogenicity-assessment-therapeutic-proteins-revision-1_en.pdf (accessed on 17 March 2022).
- Park, J.Y.; Sunga, O.; Wanitphakdeedecha, R.; Frevert, J. Neurotoxin impurities: A review of threats to efficacy. Plast. Reconstr. Surg. Glob. Open 2020, 8, e2627. [Google Scholar] [CrossRef]
- Ashworth, B. Preliminary trial of carisoprodol in multiple sclerosis. Practitioner 1964, 192, 540–542. [Google Scholar]
- Mier, R.J.; Bachrach, S.J.; Lakin, R.C.; Barker, T.; Childs, J.; Moran, M. Treatment of sialorrhea with glycopyrrolate: A double-blind, dose-ranging study. Arch. Pediatr. Adolesc. Med. 2000, 154, 1214–1218. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indication | Spasticity a | Sialorrhea b | Overall |
|---|---|---|---|
| n | 907 | 252 | 1159 |
| Male sex, n (%) | 541 (59.6) | 159 (63.1) | 700 (60.4) |
| Age, years, mean (SD) | 6.7 (4.2) | 9.4 (3.7) | 7.3 (4.3) |
| Weight, kg, mean (SD) | 23.3 (13.9) | 27.6 (11.8) | 24.2 (13.6) |
| GMFCS-E&R levels c | |||
| I–II | 452 (49.8) | 61 (24.2) | 513 (44.3) |
| III | 206 (22.7) | 25 (9.9) | 231 (19.9) |
| IV–V | 249 (27.5) | 79 (31.3) | 328 (28.3) |
| missing | 0 (0.0) | 87 (34.5) | 87 (7.5) |
| Number of ICs (Mean, SD) | 3.59 (1.31) | 3.55 (0.73) | 3.58 (1.21) |
| Pre-treatment with BoNT d (Yes), n (%) | 462 (50.9) | Missing e | 462 (39.9) |
| Location of spasticity: | |||
| LL | 849 (93.6%) | n/a | n/a |
| UL | 454 (50.1%) | n/a | n/a |
| Affected body side | |||
| Left | 138 (15.2) | n/a | n/a |
| Right | 168 (18.5) | n/a | n/a |
| Bilateral | 601 (66.3) | n/a | n/a |
| n (%) Subjects with: | Spasticity a (n = 907) | Sialorrhea b (n = 252) | Overall (n = 1159) |
|---|---|---|---|
| Any TEAE | 363 (40.0) | 118 (46.8) | 481 (41.5) |
| TR TEAE | 33 (3.6) | 12 (4.8) | 45 (3.9) |
| Any TEAESI | 18 (2.0) | 5 (2.0) | 23 (2.0) |
| TR TEAESI | 10 (1.1) | 5 (2.0) | 15 (1.3) |
| Any TESAE | 49 (5.4) | 9 (3.6) | 58 (5.0) |
| TR TESAE | 2 (0.2) | 0 (0.0) | 2 (0.2) |
| Any TEAE leading to discontinuation | 12 (1.3) | 6 (2.4) | 18 (1.6) |
| TR TEAE leading to discontinuation | 3 (0.3) | 1 (0.4) | 4 (0.3) |
| Any fatal TEAE | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Event | n (%) with Event |
|---|---|
| Muscular weakness | 6 (0.7) |
| Pain in extremity | 4 (0.4) |
| Myofascial pain syndrome | 2 (0.2) |
| Injection site pain | 5 (0.6) |
| Injection site erythema | 3 (0.3) |
| Influenza-like illness | 2 (0.2) |
| Pyrexia | 2 (0.2) |
| Study Screening | Last Study Visit b | |||||||
|---|---|---|---|---|---|---|---|---|
| Indication | N Eligible c | N Tested | Positive FIA Test, n (%) | Positive HDA Test, n (%) d | N Eligible c | N Tested | Positive FIA Test, n (%) | Positive HDA Test, n (%) e |
| Overall | 520 | 423 | 60 (14.2) | 10 (2.4) | 613 | 393 | 54 (13.7) | 10 (2.5) f |
| Sialorrhea | 163 | 80 | 10 (12.5) | 3 (3.8) | 197 | 75 | 8 (10.7) | 3 (4.0) f |
| Spasticity | 357 | 343 | 50 (14.6) | 7 (2.0) | 416 | 318 | 46 (14.5) | 7 (2.2) |
| Treatment-naïve | 141 | 139 | 13 (9.4) | 0 (0.0) | 164 | 125 | 14 (11.2) | 0 (0.0) |
| Pre-treated g | 216 | 204 | 37 (18.1) | 7 (3.4) | 252 | 193 | 32 (16.6) | 7 (3.6) |
| Patient | Indication | Pre-Treated/Naïve | HDA Result at Screening Visit b | HDA Result at Individual Final Visit b |
|---|---|---|---|---|
| 1 | Spasticity | Pre-treated | Positive | Positive |
| 2 | Spasticity | Pre-treated | Missing | Positive |
| 3 | Spasticity | Pre-treated | Positive | Positive |
| 4 | Spasticity | Pre-treated | Missing | Positive |
| 5 | Spasticity | Pre-treated | Missing | Positive |
| 6 | Spasticity | Pre-treated | Positive | Positive |
| 7 | Spasticity | Pre-treated | Missing | Positive |
| 8 | Spasticity | Pre-treated | Positive | Missing |
| 9 | Spasticity | Pre-treated | Positive | Negative |
| 10 | Spasticity | Pre-treated | Positive | Missing |
| 11 | Spasticity | Pre-treated | Positive | Missing |
| 12 | Sialorrhea | Undetermined | Positive | Positive |
| 13 | Sialorrhea | Undetermined | Positive | Positive |
| 14 | Sialorrhea | Undetermined | Positive | Positive |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berweck, S.; Banach, M.; Gaebler-Spira, D.; Chambers, H.G.; Schroeder, A.S.; Geister, T.L.; Althaus, M.; Hanschmann, A.; Vacchelli, M.; Bonfert, M.V.; et al. Safety Profile and Lack of Immunogenicity of IncobotulinumtoxinA in Pediatric Spasticity and Sialorrhea: A Pooled Analysis. Toxins 2022, 14, 585. https://doi.org/10.3390/toxins14090585
Berweck S, Banach M, Gaebler-Spira D, Chambers HG, Schroeder AS, Geister TL, Althaus M, Hanschmann A, Vacchelli M, Bonfert MV, et al. Safety Profile and Lack of Immunogenicity of IncobotulinumtoxinA in Pediatric Spasticity and Sialorrhea: A Pooled Analysis. Toxins. 2022; 14(9):585. https://doi.org/10.3390/toxins14090585
Chicago/Turabian StyleBerweck, Steffen, Marta Banach, Deborah Gaebler-Spira, Henry G. Chambers, A. S. Schroeder, Thorin L. Geister, Michael Althaus, Angelika Hanschmann, Matteo Vacchelli, Michaela V. Bonfert, and et al. 2022. "Safety Profile and Lack of Immunogenicity of IncobotulinumtoxinA in Pediatric Spasticity and Sialorrhea: A Pooled Analysis" Toxins 14, no. 9: 585. https://doi.org/10.3390/toxins14090585
APA StyleBerweck, S., Banach, M., Gaebler-Spira, D., Chambers, H. G., Schroeder, A. S., Geister, T. L., Althaus, M., Hanschmann, A., Vacchelli, M., Bonfert, M. V., Heinen, F., & Dabrowski, E. (2022). Safety Profile and Lack of Immunogenicity of IncobotulinumtoxinA in Pediatric Spasticity and Sialorrhea: A Pooled Analysis. Toxins, 14(9), 585. https://doi.org/10.3390/toxins14090585