Treatment of Depression with Botulinum Toxin


Abstract
:1. Emotional Proprioception Is a Novel Therapeutic Approach in the Treatment of Depression
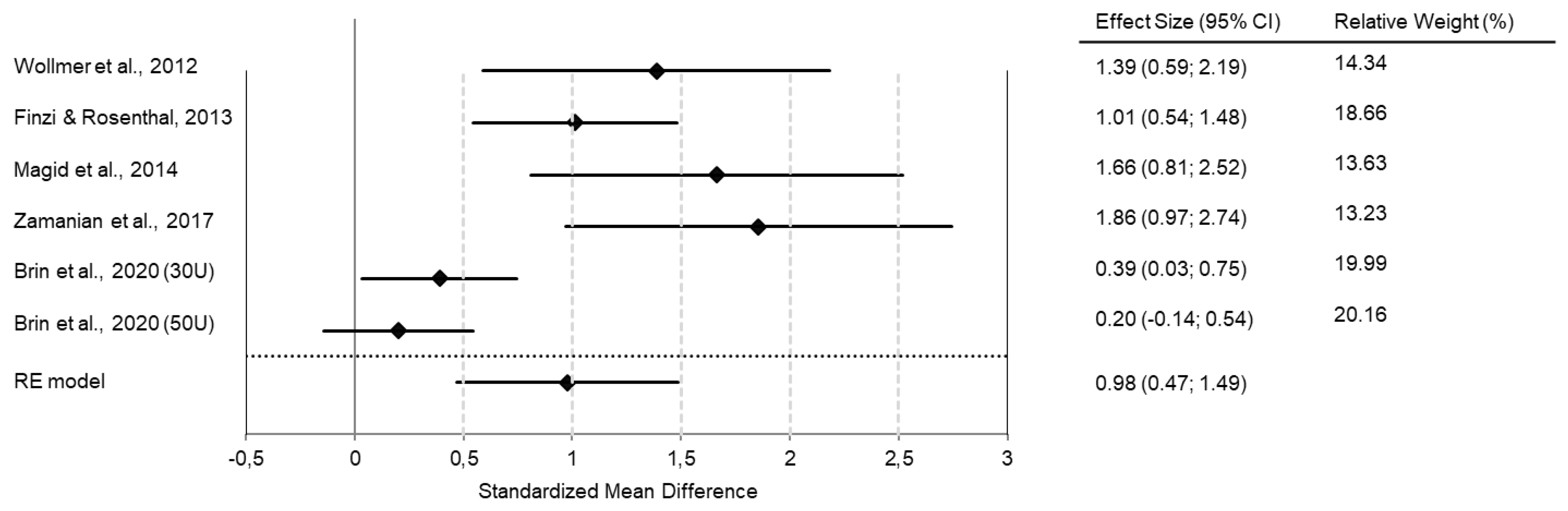
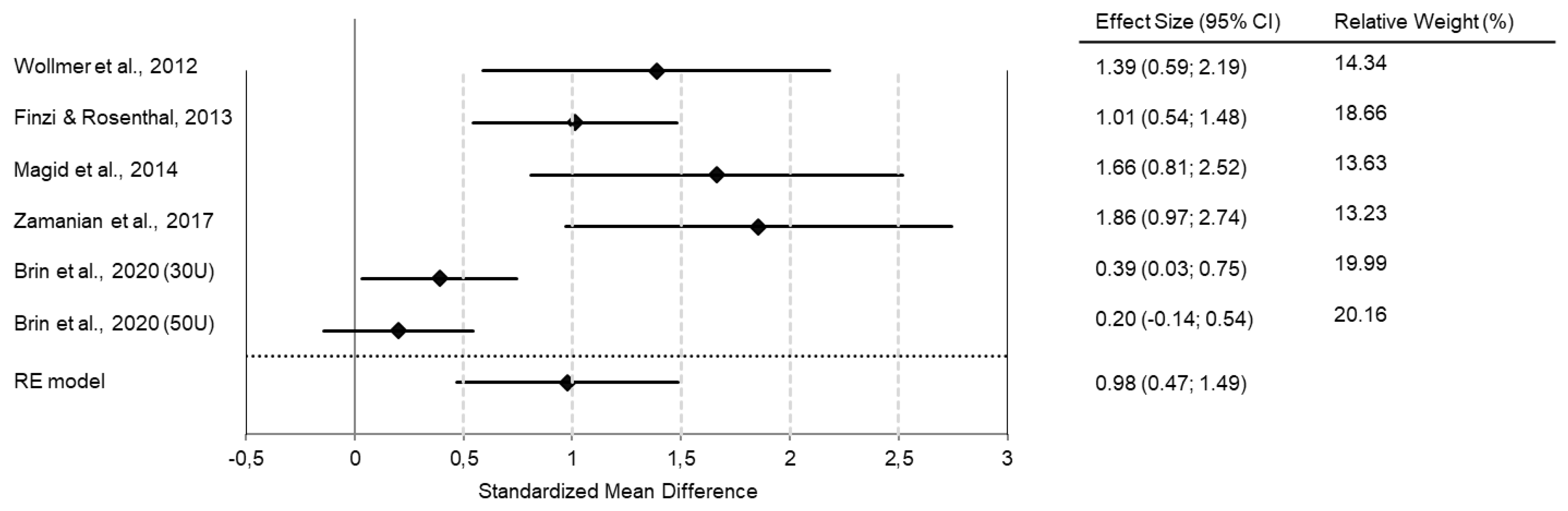
2. Clinical Trials Show the Efficacy of BoNT as a Treatment for Depression
3. Further Studies Confirm the Antidepressant Effect of BoNT
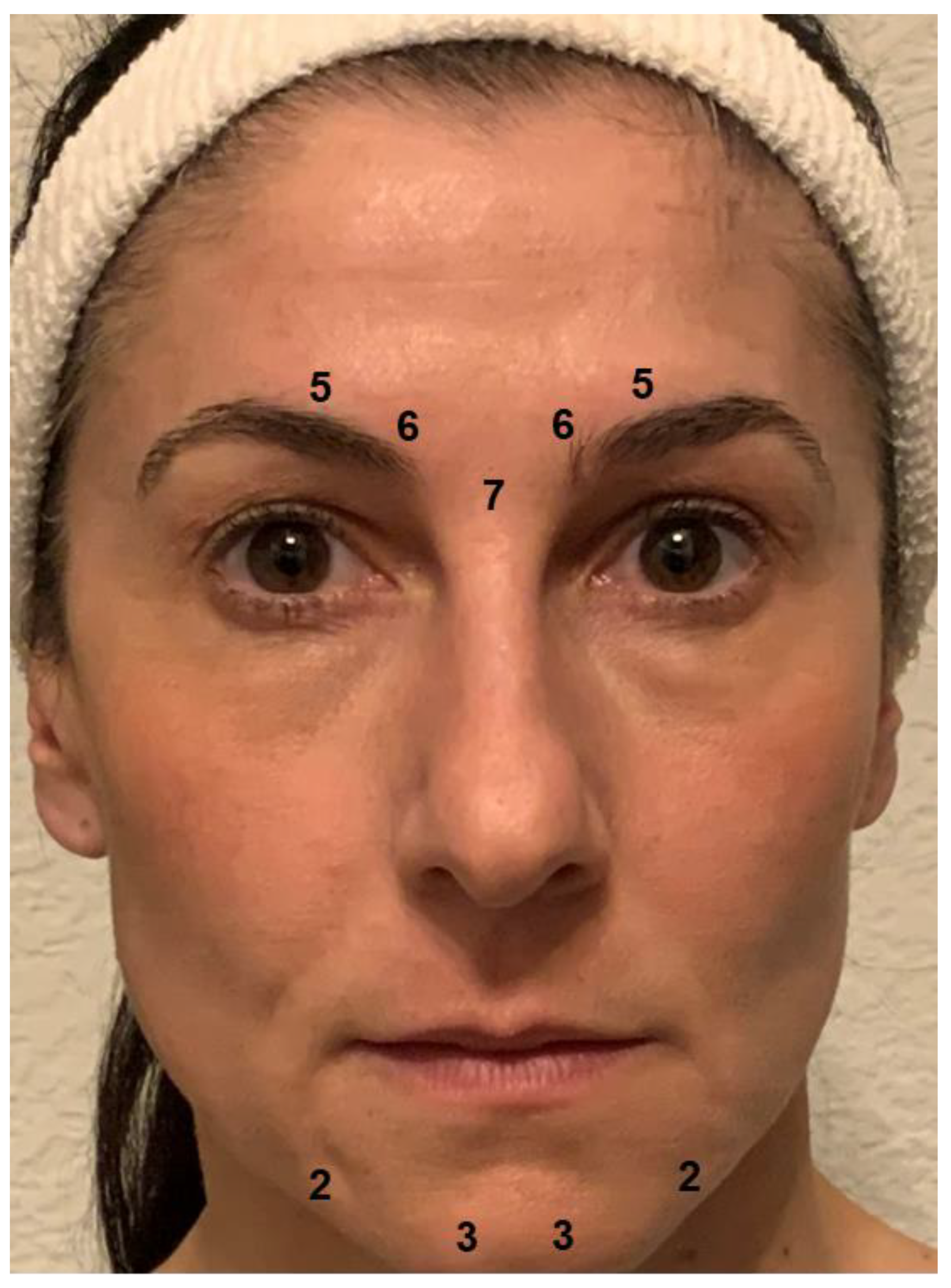
4. BoNT Is a Ready-to-Use Tool in the Clinical Management of Depression
5. Several Mechanisms of Action May Account for the Antidepressant Effect of BoNT
6. BoNT May Play an Integrative and Transdiagnostic Role in the Treatment of Mental Disorders
7. The Clinical Development of BoNT Therapy for Depression Is Currently Stuck in Phase II
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D.; Niederehe, G.; Thase, M.E.; Lavori, P.W.; Lebowitz, B.D.; et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: A STAR*D report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef] [PubMed]
- Shorter, E. Darwin’s contribution to psychiatry. Br. J. Psychiatry 2018, 195, 473–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, G.E.; Fair, P.L.; Salt, P.; Mandel, M.R.; Klerman, G.L. Facial muscle patterning to affective imagery in depressed and nondepressed subjects. Science 1976, 192, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Al Abdulmohsen, T.; Kruger, T.H. The contribution of muscular and auditory pathologies to the symptomatology of autism. Med. Hypotheses 2011, 77, 1038–1047. [Google Scholar] [CrossRef]
- Heckmann, M.; Teichmann, B.; Schröder, U.; Sprengelmeyer, R.; Ceballos-Baumann, A.O. Pharmacologic denervation of frown muscles enhances baseline expression of happiness and decreases baseline expression of anger, sadness, and fear. J. Am. Acad. Dermatol. 2003, 49, 213–216. [Google Scholar] [CrossRef]
- Sommer, B.; Zschocke, I.; Bergfeld, D.; Sattler, G.; Augustin, M. Satisfaction of patients after treatment with botulinum toxin for dynamic facial lines. Dermatol. Surg. 2003, 29, 456–460. [Google Scholar]
- Lewis, M.B.; Bowler, P.J. Botulinum toxin cosmetic therapy correlates with a more positive mood. J. Cosmet. Dermatol. 2009, 8, 24–26. [Google Scholar] [CrossRef]
- Sykianakis, D.; Stratigos, A.; Chatziioannou, A.; Christodoulou, C. Botulinum toxin type A treatment is associated with improved social and psychological behavior: A retrospective study. J. Cosmet. Dermatol. 2022, 21, 142–148. [Google Scholar] [CrossRef]
- Davis, J.I.; Senghas, A.; Brandt, F.; Ochsner, K.N. The effects of BOTOX injections on emotional experience. Emotion 2010, 10, 433–440. [Google Scholar] [CrossRef] [Green Version]
- Havas, D.A.; Glenberg, A.M.; Gutowski, K.A.; Lucarelli, M.J.; Davidson, R.J. Cosmetic use of botulinum toxin-a affects processing of emotional language. Psychol. Sci. 2010, 21, 895–900. [Google Scholar] [CrossRef]
- Baumeister, J.C.; Papa, G.; Foroni, F. Deeper than skin deep—The effect of botulinum toxin-A on emotion processing. Toxicon 2016, 118, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Hennenlotter, A.; Dresel, C.; Castrop, F.; Ceballos-Baumann, A.O.; Wohlschläger, A.M.; Haslinger, B. The link between facial feedback and neural activity within central circuitries of emotion-new insights from botulinum toxin-induced denervation of frown muscles. Cereb. Cortex 2009, 19, 537–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.J.; Neta, M.; Davis, F.C.; Ruberry, E.J.; Dinescu, D.; Heatherton, T.F.; Stotland, M.A.; Whalen, P.J. Botulinum toxin-induced facial muscle paralysis affects amygdala responses to the perception of emotional expressions: Preliminary findings from an A-B-A design. Biol. Mood Anxiety Disord. 2014, 4, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulnes, L.C.; Mariën, P.; Vandekerckhove, M.; Cleeremans, A. The effects of Botulinum toxin on the detection of gradual changes in facial emotion. Sci. Rep. 2019, 9, 11734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finzi, E.; Rosenthal, N.E. Emotional proprioception: Treatment of depression with afferent facial feedback. J. Psychiatr. Res. 2016, 80, 93–96. [Google Scholar] [CrossRef]
- Finzi, E.; Wasserman, E. Treatment of depression with botulinum toxin A: A case series. Dermatol. Surg. 2006, 32, 645–649. [Google Scholar] [CrossRef]
- Wollmer, M.A.; de Boer, C.; Kalak, N.; Beck, J.; Götz, T.; Schmidt, T.; Hodzic, M.; Bayer, U.; Kollmann, T.; Kollewe, K.; et al. Facing depression with botulinum toxin: A randomized controlled trial. J. Psychiatr. Res. 2012, 46, 574–581. [Google Scholar] [CrossRef] [Green Version]
- Finzi, E.; Rosenthal, N.E. Treatment of depression with onabotulinumtoxinA: A randomized, double-blind, placebo controlled trial. J. Psychiatr. Res. 2014, 52, 1–6. [Google Scholar] [CrossRef]
- Magid, M.; Reichenberg, J.S.; Poth, P.E.; Robertson, H.T.; LaViolette, A.K.; Kruger, T.H.; Wollmer, M.A. Treatment of major depressive disorder using botulinum toxin A: A 24-week randomized, double-blind, placebo-controlled study. J. Clin. Psychiatry 2014, 75, 837–844. [Google Scholar] [CrossRef]
- Zamanian, A.; Ghanbari Jolfaei, A.; Mehran, G.; Azizian, Z. Efficacy of Botox versus Placebo for Treatment of Patients with Major Depression. Iran. J. Public Health 2017, 46, 982–984. [Google Scholar]
- Brin, M.F.; Durgam, S.; Lum, A.; James, L.; Liu, J.; Thase, M.E.; Szegedi, A. OnabotulinumtoxinA for the treatment of major depressive disorder: A phase 2 randomized, double-blind, placebo-controlled trial in adult females. Int. Clin. Psychopharmacol. 2020, 35, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Magid, M.; Finzi, E.; Kruger, T.H.; Robertson, H.T.; Keeling, B.H.; Jung, S.; Reichenberg, J.S.; Rosenthal, N.E.; Wollmer, M.A. Treating depression with botulinum toxin: A pooled analysis of randomized controlled trials. Pharmacopsychiatry 2015, 48, 205–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parsaik, A.K.; Mascarenhas, S.S.; Hashmi, A.; Prokop, L.J.; John, V.; Okusaga, O.; Singh, B. Role of Botulinum Toxin in Depression. J. Psychiatr. Pract. 2016, 22, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Coles, N.A.; Larsen, J.T.; Kuribayashi, J.; Kuelz, A. Does Blocking Facial Feedback Via Botulinum Toxin Injections Decrease Depression? A Critical Review and Meta-Analysis. Emot. Rev. 2019, 11, 294–309. [Google Scholar] [CrossRef]
- Qian, H.; Shao, F.; Lenahan, C.; Shao, A.; Li, Y. Efficacy and Safety of Botulinum Toxin vs. Placebo in Depression: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Psychiatry 2020, 11, 603087. [Google Scholar] [CrossRef]
- Arnone, D.; Galadari, H.; Rodgers, C.J.; Östlundh, L.; Aziz, K.A.; Stip, E.; Young, A.H. Efficacy of onabotulinumtoxinA in the treatment of unipolar major depression: Systematic review, meta-analysis and meta-regression analyses of double-blind randomised controlled trials. J. Psychopharmacol. 2021, 35, 910–918. [Google Scholar] [CrossRef]
- Schulze, J.; Neumann, I.; Magid, M.; Finzi, E.; Sinke, C.; Wollmer, M.A.; Krüger, T.H.C. Botulinum toxin for the management of depression: An updated review of the evidence and meta-analysis. J. Psychiatr. Res. 2021, 135, 332–340. [Google Scholar] [CrossRef]
- Chugh, S.; Chhabria, A.; Jung, S.; Kruger, T.H.C.; Wollmer, M.A. Botulinum Toxin as a Treatment for Depression in a Real-world Setting. J. Psychiatr. Pract. 2018, 24, 15–20. [Google Scholar] [CrossRef]
- Finzi, E.; Kels, L.; Axelowitz, J.; Shaver, B.; Eberlein, C.; Krueger, T.H.; Wollmer, M.A. Botulinum toxin therapy of bipolar depression: A case series. J. Psychiatr. Res. 2018, 104, 55–57. [Google Scholar] [CrossRef]
- Zhang, Q.; Wu, W.; Fan, Y.; Li, Y.; Liu, J.; Xu, Y.; Jiang, C.; Tang, Z.; Cao, C.; Liu, T.; et al. The safety and efficacy of botulinum toxin A on the treatment of depression. Brain Behav. 2021, 11, e2333. [Google Scholar] [CrossRef]
- Zhu, C.; Wang, K.; Yu, T.; Liu, H. Effects of botulinum toxin type a on mood and cognitive function in patients with parkinson’s disease and depression. Am. J. Transl. Res. 2021, 13, 2717–2723. [Google Scholar] [PubMed]
- Affatato, O.; Moulin, T.C.; Pisanu, C.; Babasieva, V.S.; Russo, M.; Aydinlar, E.I.; Torelli, P.; Chubarev, V.N.; Tarasov, V.V.; Schiöth, H.B.; et al. High efficacy of onabotulinumtoxinA treatment in patients with comorbid migraine and depression: A meta-analysis. J. Transl. Med. 2021, 19, 133. [Google Scholar] [CrossRef] [PubMed]
- Hall, T.A.; McGwin, G., Jr.; Searcey, K.; Xie, A.; Hupp, S.L.; Owsley, C.; Kline, L.B. Health-related quality of life and psychosocial characteristics of patients with benign essential blepharospasm. Arch. Ophthalmol. 2006, 124, 116–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gündel, H.; Busch, R.; Ceballos-Baumann, A.; Seifert, E. High psychiatric comorbidity in spasmodic torticollis: A controlled study. J. Nerv. Ment. Dis. 2003, 191, 465–473. [Google Scholar] [CrossRef] [Green Version]
- Ceylan, D.; Erer, S.; Zarifoğlu, M.; Türkeş, N.; Özkaya, G. Evaluation of anxiety and depression scales and quality of LIFE in cervical dystonia patients on botulinum toxin therapy and their relatives. Neurol. Sci. 2019, 40, 725–731. [Google Scholar] [CrossRef]
- Kristensen, J.K.; Vestergaard, D.G.; Swartling, C.; Bygum, A. Association of primary hyperhidrosis with depression and anxiety: A systematic review. Acta Derm. Venereol. 2020, 100, adv00240. [Google Scholar] [CrossRef]
- Green, K.E.; Rastall, D.; Eggenberger, E. Treatment of blepharospasm/hemifacial spasm. Curr. Treat Options Neurol. 2017, 19, 41. [Google Scholar] [CrossRef]
- Bedarf, J.R.; Kebir, S.; Michelis, J.P.; Wabbels, B.; Paus, S. Depression in blepharospasm: A question of facial feedback? Neuropsychiatr. Dis. Treat. 2017, 13, 1861–1865. [Google Scholar] [CrossRef] [Green Version]
- Ochudlo, S.; Bryniarski, P.; Opala, G. Botulinum toxin improves the quality of life and reduces the intensification of depressive symptoms in patients with blepharospasm. Parkinson. Relat. Disord. 2007, 13, 505–508. [Google Scholar] [CrossRef]
- Jahanshahi, M.; Marsden, C.D. Psychological functioning before and after treatment of torticollis with botulinum toxin. J. Neurol. Neurosurg. Psychiatry 1992, 55, 229–231. [Google Scholar] [CrossRef] [Green Version]
- Weber, A.; Heger, S.; Sinkgraven, R.; Heckmann, M.; Elsner, P.; Rzany, B. Psychosocial aspects of patients with focal hyperhidrosis: Marked reduction of social phobia, anxiety and depression and increased quality of life after treatment with botulinum toxin A. Br. J. Dermatol. 2005, 152, 342–345. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Fan, S.; Luo, Y.; Peng, B. Botulinum toxin relieves anxiety and depression in patients with hemifacial spasm and blepharospasm. Neuropsychiatr. Dis. Treat 2019, 15, 33–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumenfeld, A.M.; Tepper, S.J.; Robbins, L.D.; Manack Adams, A.; Buse, D.C.; Orejudos, A.; D Silberstein, S. Effects of onabotulinumtoxinA treatment for chronic migraine on common comorbidities including depression and anxiety. J. Neurol. Neurosurg Psychiatry 2019, 90, 353–360. [Google Scholar] [CrossRef] [Green Version]
- Maasumi, K.; Thompson, N.R.; Kriegler, J.S.; Tepper, S.J. Effect of OnabotulinumtoxinA injection on depression in chronic migraine. Headache 2015, 55, 1218–1224. [Google Scholar] [CrossRef]
- Hexsel, D.; Brum, C.; Siega, C.; Schilling-Souza, J.; Dal’Forno, T.; Heckmann, M.; Rodrigues, T.C. Evaluation of self-esteem and depression symptoms in depressed and nondepressed subjects treated with onabotulinumtoxinA for glabellar lines. Dermatol. Surg. 2013, 39, 1088–1096. [Google Scholar] [CrossRef] [PubMed]
- Khademi, M.; Roohaninasab, M.; Goodarzi, A.; Seirafianpour, F.; Dodangeh, M.; Khademi, A. The healing effects of facial BOTOX injection on symptoms of depression alongside its effects on beauty preservation. J. Cosmet. Dermatol. 2021, 20, 1411–1415. [Google Scholar] [CrossRef]
- Makunts, T.; Wollmer, M.A.; Abagyan, R. Postmarketing safety surveillance data reveals antidepressant effects of botulinum toxin across various indications and injection sites. Sci. Rep. 2020, 10, 12851. [Google Scholar] [CrossRef]
- Cohen, I.V.; Makunts, T.; Atayee, R.; Abagyan, R. Population scale data reveals the antidepressant effects of ketamine and other therapeutics approved for non-psychiatric indications. Sci. Rep. 2017, 7, 1450. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Liu, J.; Liu, X.; Su, C.J.; Zhang, Q.L.; Wang, Z.H.; Cao, L.F.; Guo, X.Y.; Huang, Y.; Luo, W.; et al. Antidepressant-Like Action of Single Facial Injection of Botulinum Neurotoxin A is Associated with Augmented 5-HT Levels and BDNF/ERK/CREB Pathways in Mouse Brain. Neurosci. Bull. 2019, 35, 661–672. [Google Scholar] [CrossRef]
- Beer, K. Cost effectiveness of botulinum toxins for the treatment of depression: Preliminary observations. J. Drugs Dermatol. 2010, 9, 27–30. [Google Scholar]
- Brin, M.F.; Boodhoo, T.I.; Pogoda, J.M.; James, L.M.; Demos, G.; Terashima, Y.; Gu, J.; Eadie, N.; Bowen, B.L. Safety and tolerability of onabotulinumtoxinA in the treatment of facial lines: A meta-analysis of individual patient data from global clinical registration studies in 1678 participants. J. Am. Acad Dermatol. 2009, 61, 961–970. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, A.; Cohen, J.L.; Cox, S.E.; De Boulle, K.; Fagien, S.; Finn, C.J.; Flynn, T.; Lowe, N.J.; Raspaldo, H.; Sommer, B.; et al. Facial aesthetics: Achieving the natural, relaxed look. J. Cosmet. Laser Ther. 2007, 9 (Suppl. 1), 6–10. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.B. The interactions between botulinum-toxin-based facial treatments and embodied emotions. Sci. Rep. 2018, 8, 14720. [Google Scholar] [CrossRef] [PubMed]
- Ceolato, C.; Charles, E.; Clément, J.P.; Ranoux, D. Botulinum toxin in the treatment of resistant depressive disorder: Comparison of 2 facial injection sites. Toxicon 2018, 156 (Suppl. S1), 15. [Google Scholar] [CrossRef]
- Wollmer, M.A.; Kalak, N.; Jung, S.; de Boer, C.; Magid, M.; Reichenberg, J.S.; Brand, S.; Holsboer-Trachsler, E.; Kruger, T.H. Agitation predicts response of depression to botulinum toxin treatment in a randomized controlled trial. Front. Psychiatry 2014, 5, 36. [Google Scholar] [CrossRef] [Green Version]
- Reichenberg, J.S.; Hauptman, A.J.; Robertson, H.T.; Finzi, E.; Kruger, T.H.; Wollmer, M.A.; Magid, M. Botulinum toxin for depression: Does patient appearance matter? J. Am. Acad. Dermatol. 2016, 74, 171–173. [Google Scholar] [CrossRef] [Green Version]
- Cosio, T.; Campione, E. A new hypothesis in botulin therapy for depression: Insula cortex modification. Dermatol. Ther. 2019, 32, e13008. [Google Scholar] [CrossRef]
- Ibragić, S.; Matak, I.; Dračić, A.; Smajlović, A.; Muminović, M.; Proft, F.; Sofić, E.; Lacković, Z.; Riederer, P. Effects of botulinum toxin type A facial injection on monoamines and their metabolites in sensory, limbic and motor brain regions in rats. Neurosci. Lett. 2016, 617, 213–217. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Liu, T.; Luo, W. Botulinum Neurotoxin Therapy for Depression: Therapeutic Mechanisms and Future Perspective. Front. Psychiatry 2021, 12, 584416. [Google Scholar] [CrossRef]
- Molina, B.; Grangier, Y.; Mole, B.; Ribe, N.; Martín Diaz, L.; Prager, W.; Paliargues, F.; Kerrouche, N. Patient satisfaction after the treatment of glabellar lines with Botulinum toxin type A (Speywood Unit): A multi-centre European observational study. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1382–1388. [Google Scholar] [CrossRef]
- Caleo, M.; Schiavo, G. Central effects of tetanus and botulinum neurotoxins. Toxicon 2009, 54, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Weise, D.; Weise, C.M.; Naumann, M. Central Effects of Botulinum Neurotoxin-Evidence from Human Studies. Toxins 2019, 11, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruger, T.H.; Magid, M.; Wollmer, M.A. Can Botulinum Toxin Help Patients with Borderline Personality Disorder? Am. J. Psychiatry 2016, 173, 940–941. [Google Scholar] [CrossRef] [PubMed]
- Finzi, E.; Rosenthal, N.E. Botulinum toxin therapy of social anxiety disorder: A case series. J. Clin. Psychopharmacol. 2019, 39, 410–412. [Google Scholar] [CrossRef] [PubMed]
- Wollmer, M.A.; Neumann, I.; Jung, S.; Bechinie, A.; Herrmann, J.; Müller, A.; Wohlmuth, P.; Fournier-Kaiser, L.; Sperling, C.; Peters, L.; et al. Clinical effects of glabellar botulinum toxin injections on borderline personality disorder: A randomized controlled trial. J. Psychopharmacol. 2022, 36, 159–169. [Google Scholar] [CrossRef]
- Chen, W.J.; Niu, J.Q.; Chen, Y.T.; Deng, W.J.; Xu, Y.Y.; Liu, J.; Luo, W.F.; Liu, T. Unilateral facial injection of Botulinum neurotoxin A attenuates bilateral trigeminal neuropathic pain and anxiety-like behaviors through inhibition of TLR2-mediated neuroinflammation in mice. J. Headache Pain 2021, 22, 38. [Google Scholar] [CrossRef]
- Wollmer, M.A.; Makunts, T.; Krüger, T.H.C.; Abagyan, R. Postmarketing safety surveillance data reveals protective effects of botulinum toxin injections against incident anxiety. Sci. Rep. 2021, 11, 24173. [Google Scholar] [CrossRef]
- Yesudhas, A.; Radhakrishnan, R.K.; Sukesh, A.; Ravichandran, S.; Manickam, N.; Kandasamy, M. BOTOX® counteracts the innate anxiety-related behaviours in correlation with increased activities of key antioxidant enzymes in the hippocampus of ageing experimental mice. Biochem. Biophys. Res. Commun. 2021, 569, 54–60. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Study | Trial Number | Participants | Intervention * | PrimaryOutcome Scale | Primary Endpoint | Main Results |
|---|---|---|---|---|---|---|
| [17] | NCT00934687 | N = 30 (23 women/7 men) | 29/39 U onabotulinumtoxinA or saline placebo | HAM-D17 | 6 weeks after baseline | Significantly greater improvement and response rate in the BoNT group |
| [18] | NCT01556971 | N = 74 (69 women/5 men) | 29/40 U onabotulinumtoxinA or saline placebo | MADRS | 6 weeks after baseline | Significantly greater improvement, response and remission rate in the BoNT group |
| [19] | NCT01392963 | N = 30 (28 women/2 men) | 29/39 U onabotulinumtoxinA or saline placebo | HAM-D21 | 6 weeks after baseline | Significantly greater improvement and response rate in the BoNT group |
| [20] | TCTR20170409001 | N = 28 (14 women/14 men) | OnabotulinumtoxinA or unspecified placebo | BDI | 6 weeks after baseline | Significantly greater improvement in the BoNT group |
| [21] | NCT02116361 | N = 123 (women only) N = 132 (women only) | 30 U onabotulinumtoxinA or saline placebo 50 U onabotulinumtoxinA or saline placebo | MADRS | 6 weeks after baseline | Numerically greater improvement in the 30 U BoNT group |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wollmer, M.A.; Magid, M.; Kruger, T.H.C.; Finzi, E. Treatment of Depression with Botulinum Toxin. Toxins 2022, 14, 383. https://doi.org/10.3390/toxins14060383
Wollmer MA, Magid M, Kruger THC, Finzi E. Treatment of Depression with Botulinum Toxin. Toxins. 2022; 14(6):383. https://doi.org/10.3390/toxins14060383
Chicago/Turabian StyleWollmer, Marc Axel, Michelle Magid, Tillmann H. C. Kruger, and Eric Finzi. 2022. "Treatment of Depression with Botulinum Toxin" Toxins 14, no. 6: 383. https://doi.org/10.3390/toxins14060383
APA StyleWollmer, M. A., Magid, M., Kruger, T. H. C., & Finzi, E. (2022). Treatment of Depression with Botulinum Toxin. Toxins, 14(6), 383. https://doi.org/10.3390/toxins14060383