Whole Grains Contribute Only a Small Proportion of Dietary Fiber to the U.S. Diet


Abstract
:1. Introduction
1.1. Dietary Fiber
1.2. Whole Grains
1.3. Significance
2. Materials and Methods
2.1. Data Set
2.2. Study Variables
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th ed.2015. Available online: https://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 13 December 2016).
- NHS. How to Get More Fibre into Your Diet. Available online: http://www.nhs.uk/Livewell/Goodfood/Pages/how-to-get-more-fibre-into-your-diet.aspx/ (accessed on 13 January 2017).
- Institute of Medicine of the National Academy of Sciences. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients); National Academy Press: Washington, DC, USA, 2002. [Google Scholar]
- McGill, C.; Fulgoni, V.L., III; Devareddy, L. Ten-year trends in fiber and whole grain intakes and food sources for the United States population: National Health and Nutrition Examination Survey 2001–2010. Nutrients 2015, 7, 1119. [Google Scholar] [CrossRef] [PubMed]
- Keast, D.R.; Fulgoni, V.L.; Nicklas, T.A.; O’Neil, C.E. Food sources of energy and nutrients among children in the United States: National Health and Nutrition Examination Survey 2003–2006. Nutrients 2013, 5, 283–301. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, C.E.; Keast, D.R.; Fulgoni, V.L.; Nicklas, T.A. Food sources of energy and nutrients among adults in the US: NHANES 2003–2006. Nutrients 2012, 4, 2097–2120. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.H.; Yen, S.T. The U.S. Grain Consumption Landscape: Who Eats Grain, in What Form, Where, and How Much? Economic Research Report Number 50. United States Department of Agriculture, Department of Economic Research Service, 2007–2011. Available online: http://purl.umn.edu/55967 (accessed on 13 December 2016).
- Gropper, S.S.; Acosta, P.B. The therapeutic effect of fiber in treating obesity. J. Am. Coll. Nutr. 1987, 6, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; Mander, A.P.; Jones, L.R.; Emmett, P.M.; Jebb, S.A. Energy-dense, low-fiber, high-fat dietary pattern is associated with increased fatness in childhood. Am. J. Clin. Nutr. 2008, 87, 846–854. [Google Scholar] [PubMed]
- Slavin, J.L. Dietary fiber and body weight. Nutrition 2005, 21, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Howarth, N.C.; Huang, T.T.; Roberts, S.B.; McCrory, M.A. Dietary fiber and fat are associated with excess weight in young and middle-aged US adults. J. Am. Diet. Assoc. 2005, 105, 1365–1372. [Google Scholar] [CrossRef] [PubMed]
- Du, H.; van der, A.D.; Boshuizen, H.C.; Forouhi, N.G.; Wareham, N.J.; Halkjaer, J.; Tjonneland, A.; Overvad, K.; Jakobsen, M.U.; Boeing, H.; et al. Dietary fiber and subsequent changes in body weight and waist circumference in European men and women. Am. J. Clin. Nutr. 2010, 91, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Overby, N.C.; Sonestedt, E.; Laaksonen, D.E.; Birgisdottir, B.E. Dietary fiber and the glycemic index: A background paper for the Nordic nutrition recommendations 2012. Food. Nutr. Res. 2013, 57. [Google Scholar] [CrossRef] [PubMed]
- Johansson-Persson, A.; Ulmius, M.; Cloetens, L.; Karhu, T.; Herzig, K.H.; Onning, G. A high intake of dietary fiber influences C-reactive protein and fibrinogen, but not glucose and lipid metabolism, in mildly hypercholesterolemic subjects. Eur. J. Nutr. 2014, 53, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J. Fiber and prebiotics: Mechanisms and health benefits. Nutrients 2013, 5, 1417–1435. [Google Scholar] [CrossRef] [PubMed]
- Kranz, S.; Brauchla, M.; Slavin, J.L.; Miller, K.B. What do we know about dietary fiber intake in children and health? The effects of fiber intake on constipation, obesity, and diabetes in children. Adv. Nutr. 2012, 3, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarczyk, M.M.; Miller, M.J.; Freund, G.G. The health benefits of dietary fiber: Beyond the usual suspects of type 2 diabetes mellitus, cardiovascular disease and colon cancer. Metabolism 2012, 61, 1058–1066. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.W.; Baird, P.; Davis, R.H., Jr.; Ferreri, S.; Knudtson, M.; Koraym, A.; Waters, V.; Williams, C.L. Health benefits of dietary fiber. Nutr. Rev. 2009, 67, 188–205. [Google Scholar] [CrossRef] [PubMed]
- Jonnalagadda, S.S.; Harnack, L.; Hai Liu, R.; McKeown, N.; Seal, C.; Liu, S.; Fahey, G.C. Putting the whole grain puzzle together: Health benefits associated with whole grains—Summary of American society for nutrition 2010 satellite symposium. J. Nutr. 2011, 141, 1011S–1022S. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.S.; Qi, L.; Fahey, G.C.; Klurfeld, D.M. Consumption of cereal fiber, mixtures of whole grain and bran, and whole grains and risk reduction in type 2 diabetes, obesity, and cardiovascular disease. Am. J. Clin. Nutr. 2013, 98, 594–619. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Healthy Diet Fact Sheet n°394. Available online: http://www.who.int/mediacentre/factsheets/fs394/en/ (accessed on 13 January 2017).
- Oldways Trust. Whole Grain Guidelines Worldwide. Available online: http://wholegrainscouncil.org/whole-grains-101/how-much-enough/whole-grain-guidelines-worldwide (accessed on 13 January 2017).
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. Dietary Guidelines for Americans 2005. Available online: https://www.cnpp.usda.gov/dietary-guidelines-2005 (accessed on 13 December 2016).
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans 2010. Available online: https://www.cnpp.usda.gov/dietary-guidelines-2010 (accessed on 13 December 2016).
- Krebs-Smith, S.M.; Guenther, P.M.; Subar, A.F.; Kirkpatrick, S.I.; Dodd, K.W. Americans do not meet federal dietary recommendations. J. Nutr. 2010, 140, 1832–1838. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, C.E.; Nicklas, T.A.; Zanovec, M.; Cho, S. Whole-grain consumption is associated with diet quality and nutrient intake in adults: The National Health and Nutrition Examination Survey, 1999–2004. J. Am. Diet. Assoc. 2010, 110, 1461–1468. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Draft Guideline: Whole Grains Label Statements, Guidance for Industry and FDA Staff; Food and Drug Administration: College Park, MD, USA, 2006. [Google Scholar]
- Clemens, R.; Kranz, S.; Mobley, A.R.; Nicklas, T.A.; Raimondi, M.P.; Rodriguez, J.C.; Slavin, J.L.; Warshaw, H. Filling America’s fiber intake gap: Summary of a roundtable to probe realistic solutions with a focus on grain-based foods. J. Nutr. 2012, 142, 1390s–1401s. [Google Scholar] [CrossRef] [PubMed]
- Nicklas, T.A.; O’Neil, C.E.; Liska, D.J.; Almeida, N.G.; Fulgoni, V.L., III. Modeling dietary fiber intakes in US adults: Implications for public policy. Food Nutr. Sci. 2011, 2, 925–931. [Google Scholar] [CrossRef]
- Reicks, M.; Jonnalagadda, S.; Albertson, A.M.; Joshi, N. Total dietary fiber intakes in the US population are related to whole grain consumption: Results from the national health and nutrition examination survey 2009 to 2010. Nutr. Res. 2014, 34, 226–234. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture. ChooseMyPlate.gov. Available online: https://www.choosemyplate.gov/ (accessed on 13 December 2016).
- Centers for Disease Control and Prevention; National Center for Health Statistics. National Health and Nutrition Examination Survey (NHANES). Available online: https://www.cdc.gov/nchs/nhanes/ (accessed on 13 December 2016).
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [PubMed]
- Bowman, S.A.; Friday, J.E.; Moshfegh, A. MyPyramid Equivalents Database, 2.0 for USDA Survey Foods 2003–2004. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/mped-databases-for-downloading/ (accessed on 26 February 2017).
- Center for Nutrition Policy and Promotion. CNPP 03-04 Fruit Database. Available online: https://www.cnpp.usda.gov/healthy-eating-index-support-files-03-04 (accessed on 16 February 2017).
- Food and Nutrient Database for Dietary Studies. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/fndds/ (accessed on 16 February 2017).
- International Food Information Council. 2016 Food and Health Survey. Available online: http://www.foodinsight.org/sites/default/files/2016-Food-and-Health-Survey-Report_%20FINAL_0.pdf (accessed on 13 December 2016).
- Mobley, A.R.; Slavin, J.L.; Hornick, B.A. The future of grain foods recommendations in dietary guidance. J. Nutr. 2013, 143, 1527S–1532S. [Google Scholar] [CrossRef] [PubMed]
- Brauchla, M.; Juan, W.; Story, J.; Kranz, S. Sources of dietary fiber and the association of fiber intake with childhood obesity risk (in 2–18 years old) and diabetes risk of adolescents 12–18 years old: NHANES 2003–2006. J. Nutr. Metab. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Hur, I.Y.; Reicks, M. Relationship between whole-grain intake, chronic disease risk indicators, and weight status among adolescents in the National Health and Nutrition Examination Survey, 1999–2004. J. Am. Diet. Assoc. 2012, 112, 46–55. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Participant Characteristic | Children 2–18 | Adults 19 & Older | ||
|---|---|---|---|---|
| Males | Females | Males | Females | |
| Unweighted sample size (N) | 6775 | 6646 | 10,181 | 10,789 |
| Gender (%) | 50.7 | 49.3 | 47.9 | 52.1 |
| Race-ethnicity (%) | ||||
| Non-Hispanic white | 30.9 | 29.3 | 34.0 | 36.8 |
| Non-Hispanic black | 7.0 | 7.4 | 5.1 | 6.3 |
| Mexican American | 9.5 | 9.1 | 6.1 | 6.1 |
| Other | 3.3 | 3.4 | 2.6 | 2.8 |
| Poverty Income Ratio (PIR) (%) | ||||
| <1.3 | 15.5 | 16.4 | 9.0 | 12.0 |
| 1.3–1.84 | 5.8 | 5.4 | 4.6 | 5.8 |
| 1.85–3.4 | 12.8 | 11.4 | 11.5 | 12.5 |
| >3.4 | 17.1 | 15.7 | 22.8 | 21.8 |
| Education (%) | ||||
| No high school diploma | N/A | N/A | 8.9 | 9.8 |
| High school graduate | N/A | N/A | 12.3 | 13.0 |
| More than high school | N/A | N/A | 26.6 | 29.2 |
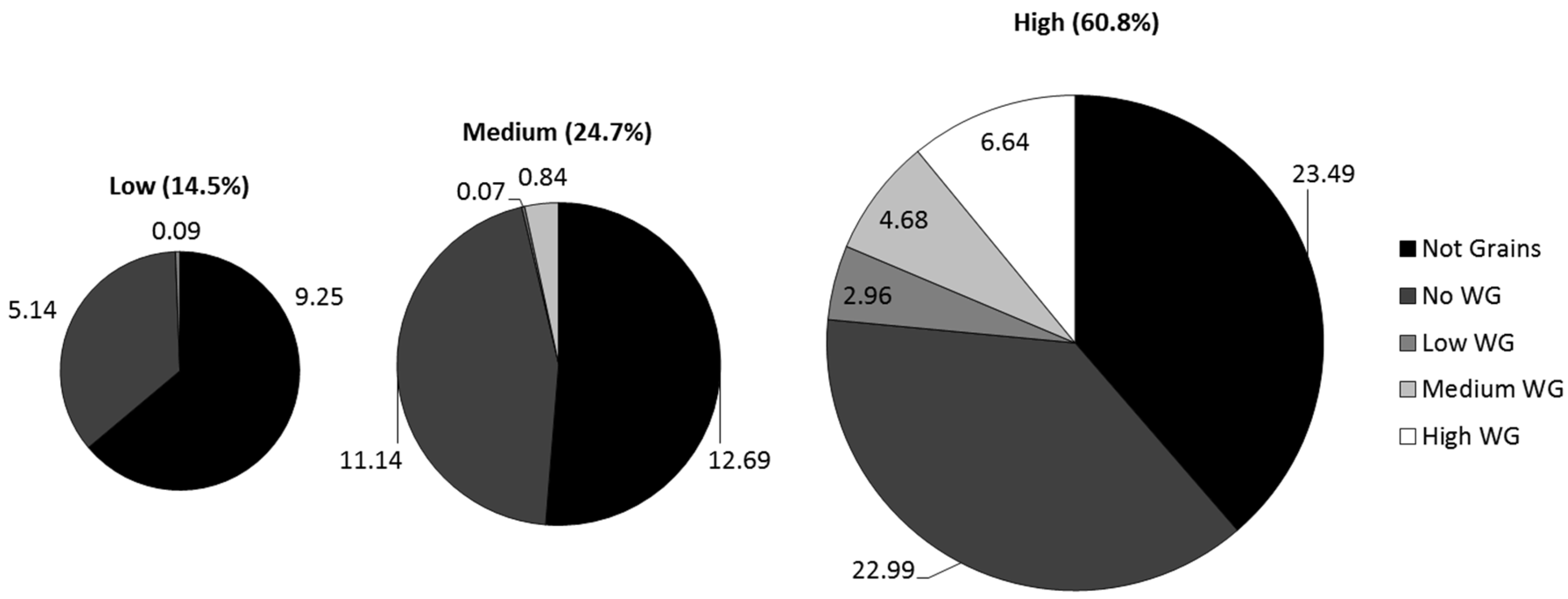
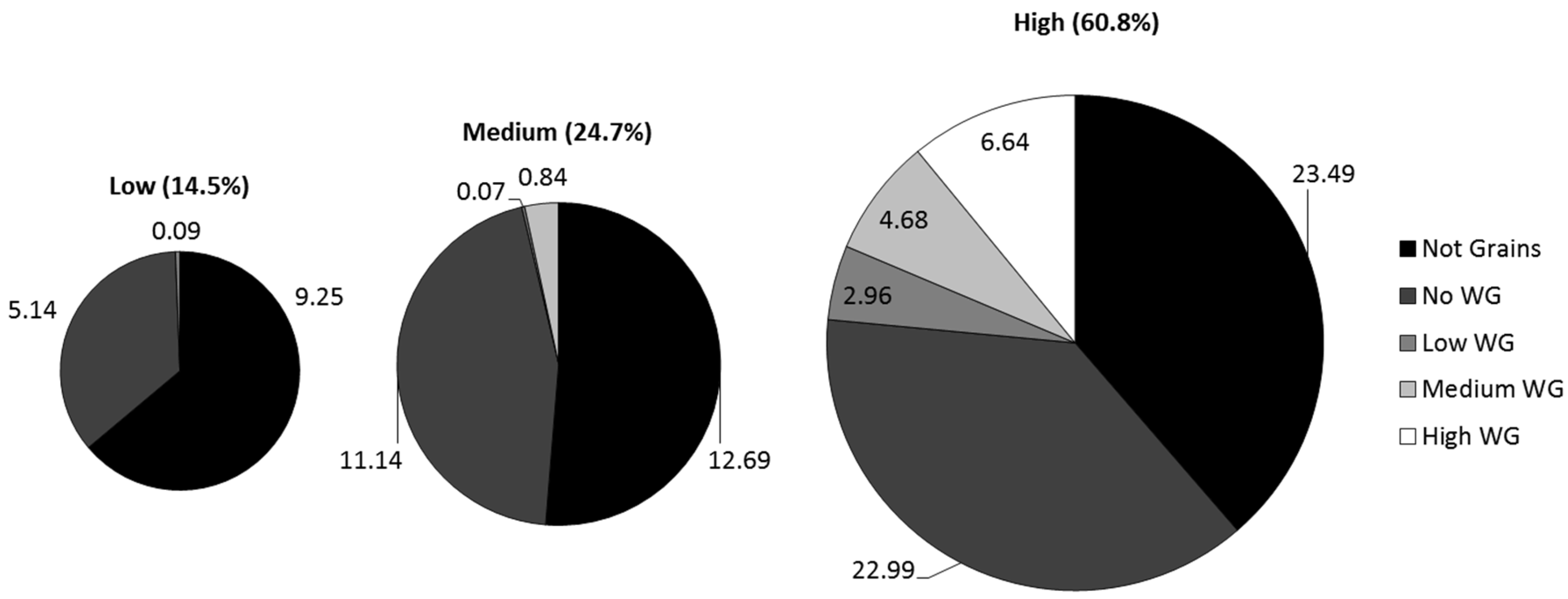
| Whole Grain (Tertiles) | Fiber (Tertiles) | WG % | Fiber % | % Reporting |
|---|---|---|---|---|
| High WG (WG ≥ 1.33) | High Fiber (DF ≥ 1.7) | 50.4 | 6.6 | 7.9 |
| Medium WG (0.71 < WG < 1.33) | High Fiber (DF ≥ 1.7) | 29.9 | 4.7 | 7.9 |
| Medium Fiber (0.9 < DF < 1.7) | 10.5 | 0.8 | 1.1 | |
| Low Fiber (0 < DF ≤ 0.9) | 0.2 | 0.01 | 0.02 | |
| Low WG (0 < WG ≤ 0.71) | High Fiber (DF ≥ 1.7) | 8.1 | 3.0 | 6.8 |
| Medium Fiber (0.9 < DF < 1.7) | 0.1 | 0.1 | 0.2 | |
| Low Fiber (0 < DF ≤ 0.9) | 0.9 | 0.1 | 0.6 | |
| No WG | Any Fiber (DF > 0) | 0.0 | 39.2 | 33.1 |
| Total | 100.0 | 54.5 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kranz, S.; Dodd, K.W.; Juan, W.Y.; Johnson, L.K.; Jahns, L. Whole Grains Contribute Only a Small Proportion of Dietary Fiber to the U.S. Diet. Nutrients 2017, 9, 153. https://doi.org/10.3390/nu9020153
Kranz S, Dodd KW, Juan WY, Johnson LK, Jahns L. Whole Grains Contribute Only a Small Proportion of Dietary Fiber to the U.S. Diet. Nutrients. 2017; 9(2):153. https://doi.org/10.3390/nu9020153
Chicago/Turabian StyleKranz, Sibylle, Kevin W. Dodd, Wen Yen Juan, LuAnn K. Johnson, and Lisa Jahns. 2017. "Whole Grains Contribute Only a Small Proportion of Dietary Fiber to the U.S. Diet" Nutrients 9, no. 2: 153. https://doi.org/10.3390/nu9020153
APA StyleKranz, S., Dodd, K. W., Juan, W. Y., Johnson, L. K., & Jahns, L. (2017). Whole Grains Contribute Only a Small Proportion of Dietary Fiber to the U.S. Diet. Nutrients, 9(2), 153. https://doi.org/10.3390/nu9020153