Postprandial Glycemic and Insulinemic Responses to Common Breakfast Beverages Consumed with a Standard Meal in Adults Who Are Overweight and Obese

Abstract
:1. Introduction
2. Subjects and Methods
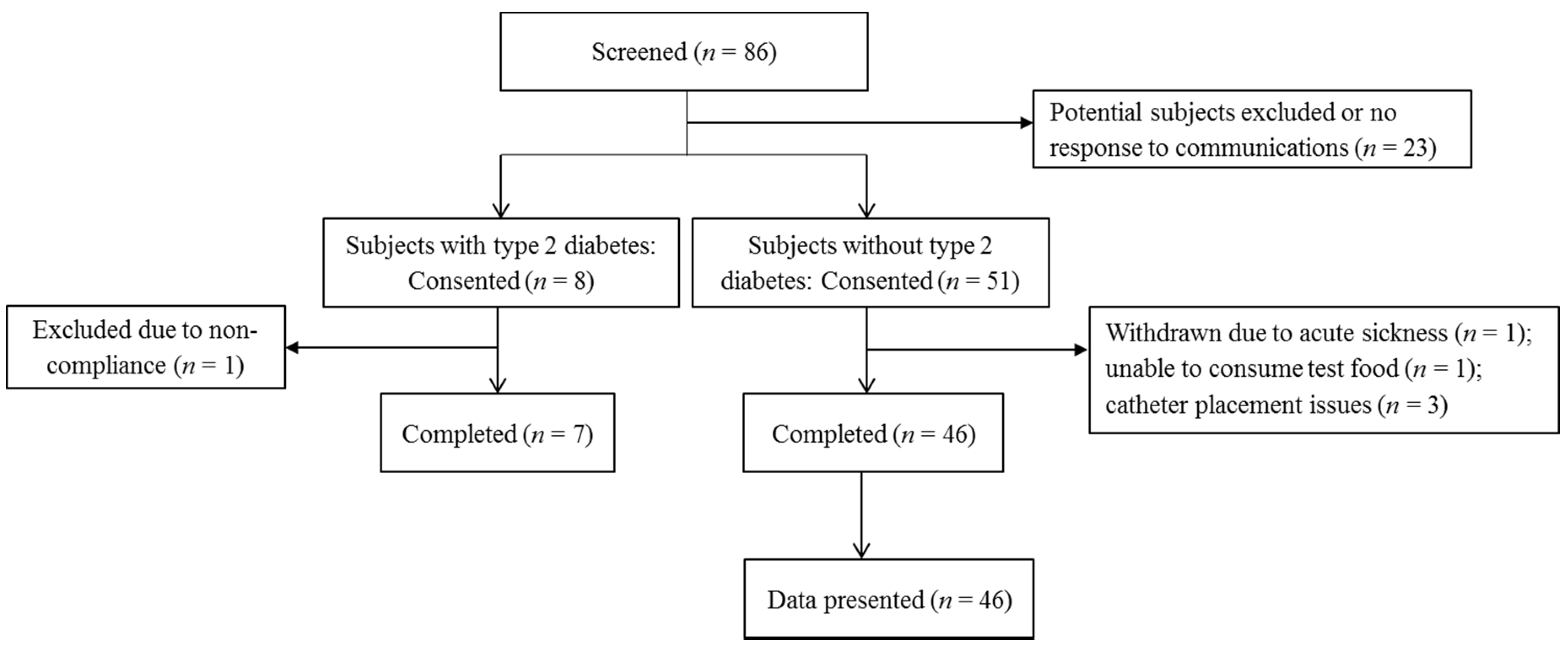
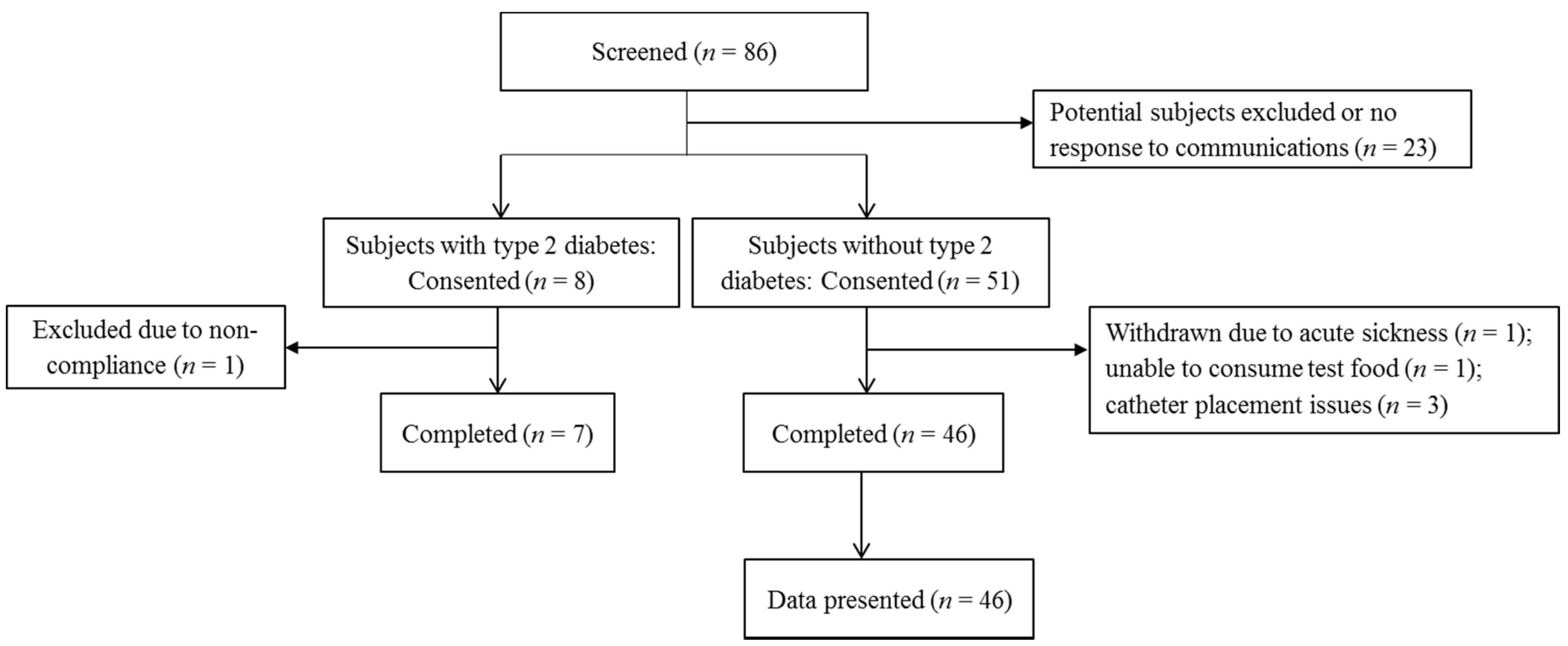
2.1. Subject Recruitment
2.2. Subject Screening
2.3. Experimental Design
2.4. Multi-Pass Dietary Recall
2.5. Body Mass and Body Composition
2.6. Diet
2.7. Acute Meal Glucose Tolerance Test (MGTT)
2.8. Plasma Glucose and Insulin Analyses and Calculations
2.9. Sample Size Estimation
2.10. Data Analysis
3. Results
3.1. Baseline Subject Characteristics
3.2. Dietary Intake and Body Composition before and at the End of the Study
3.3. Fasting State Glucose Homeostasis on Testing Days
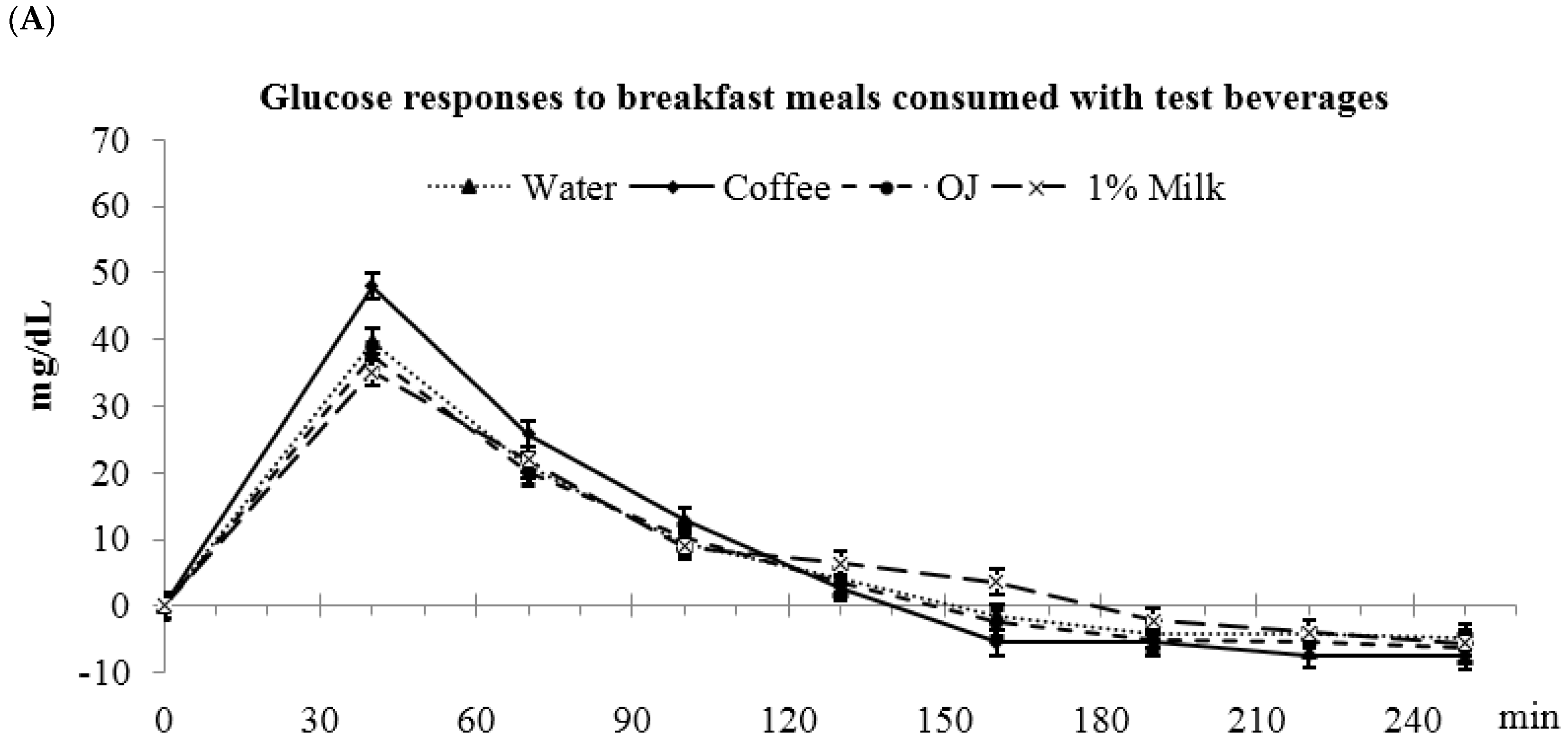
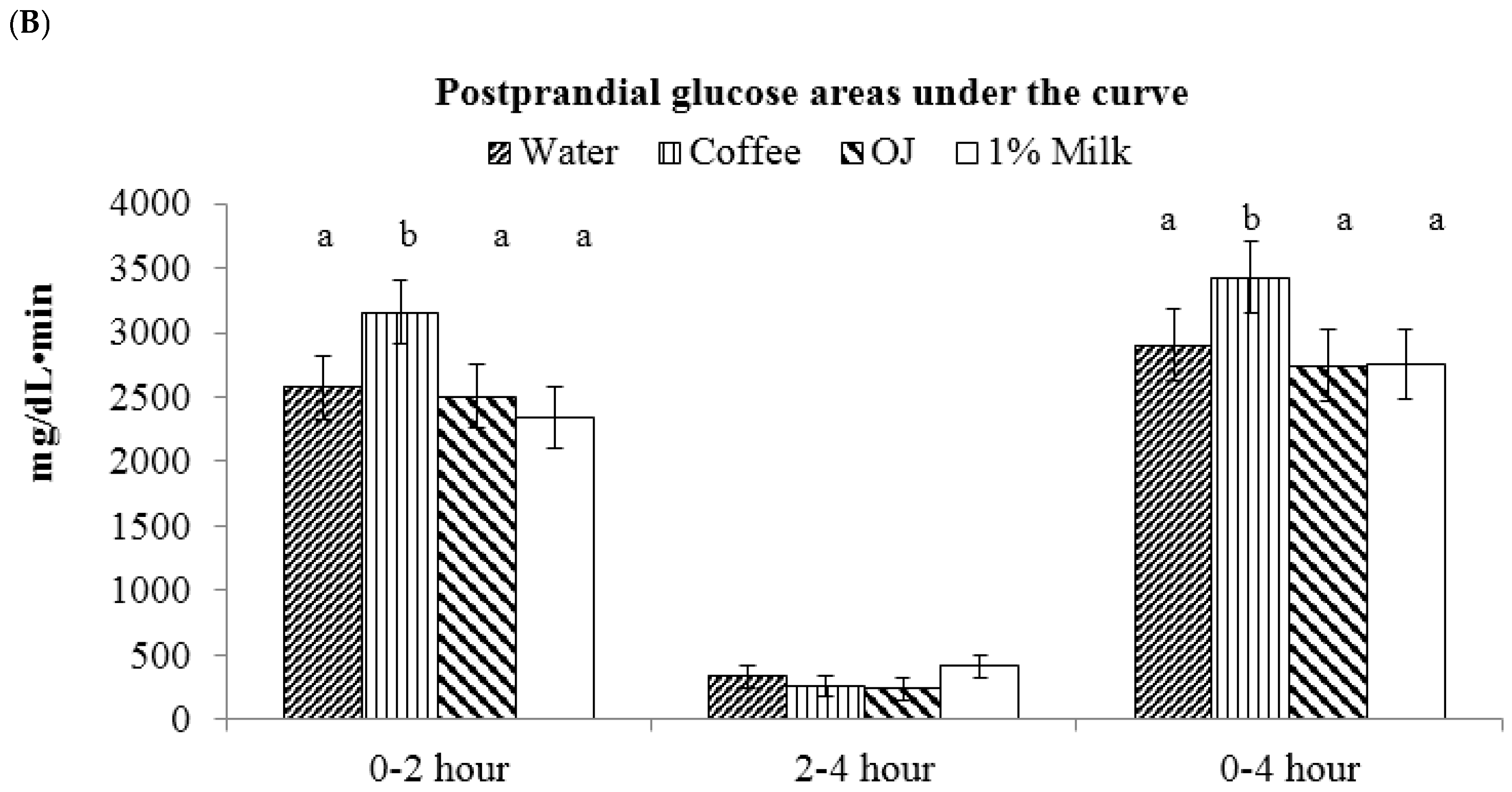
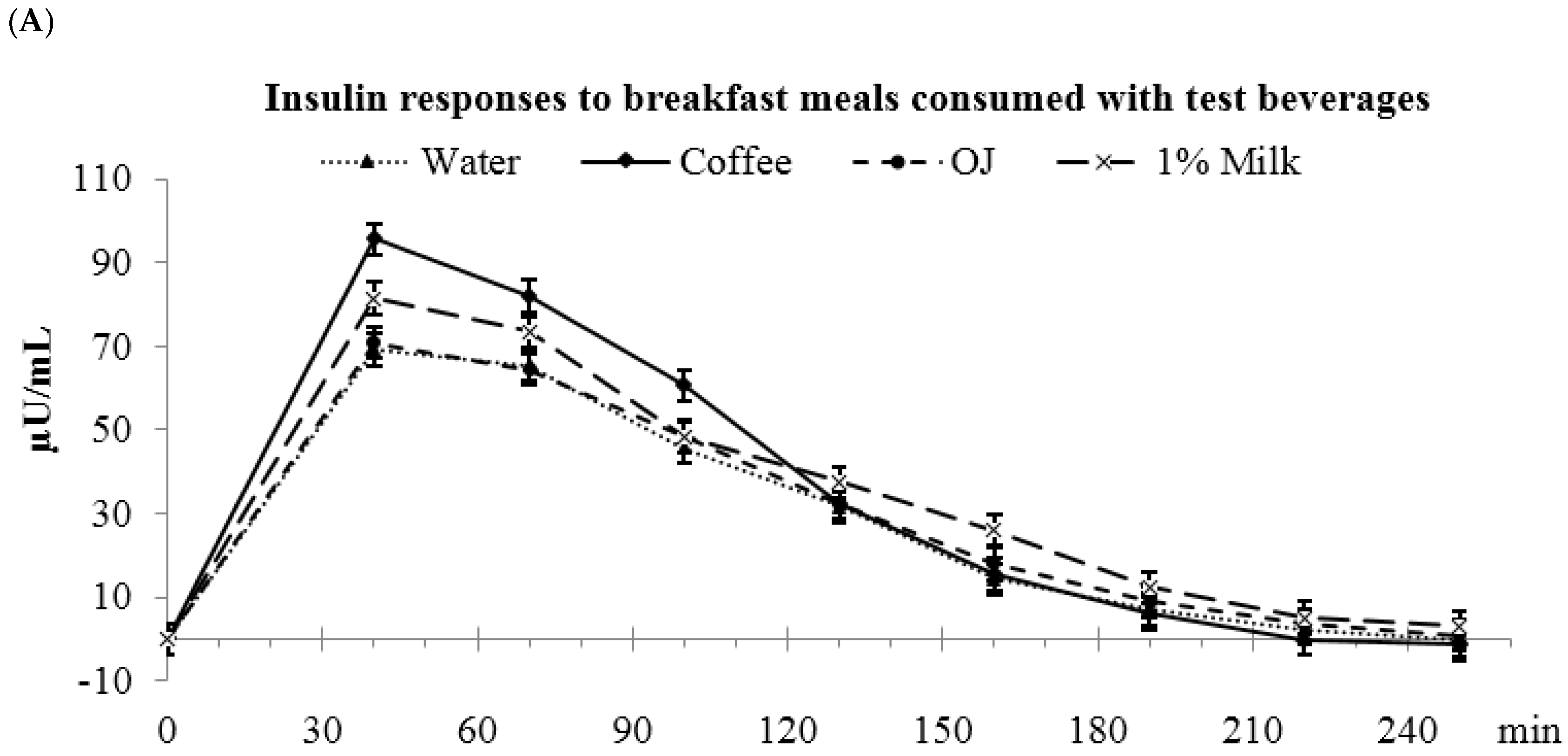
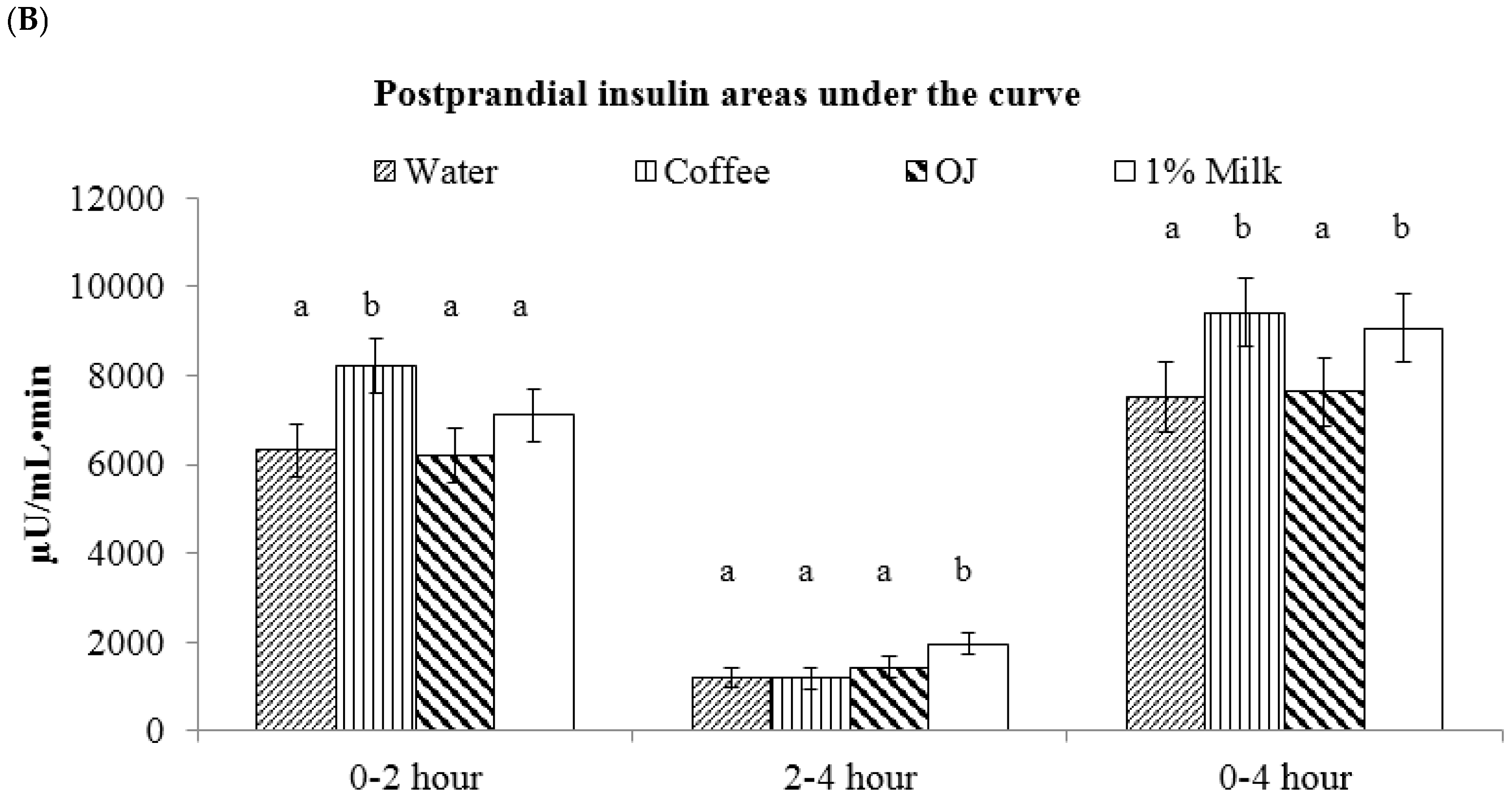
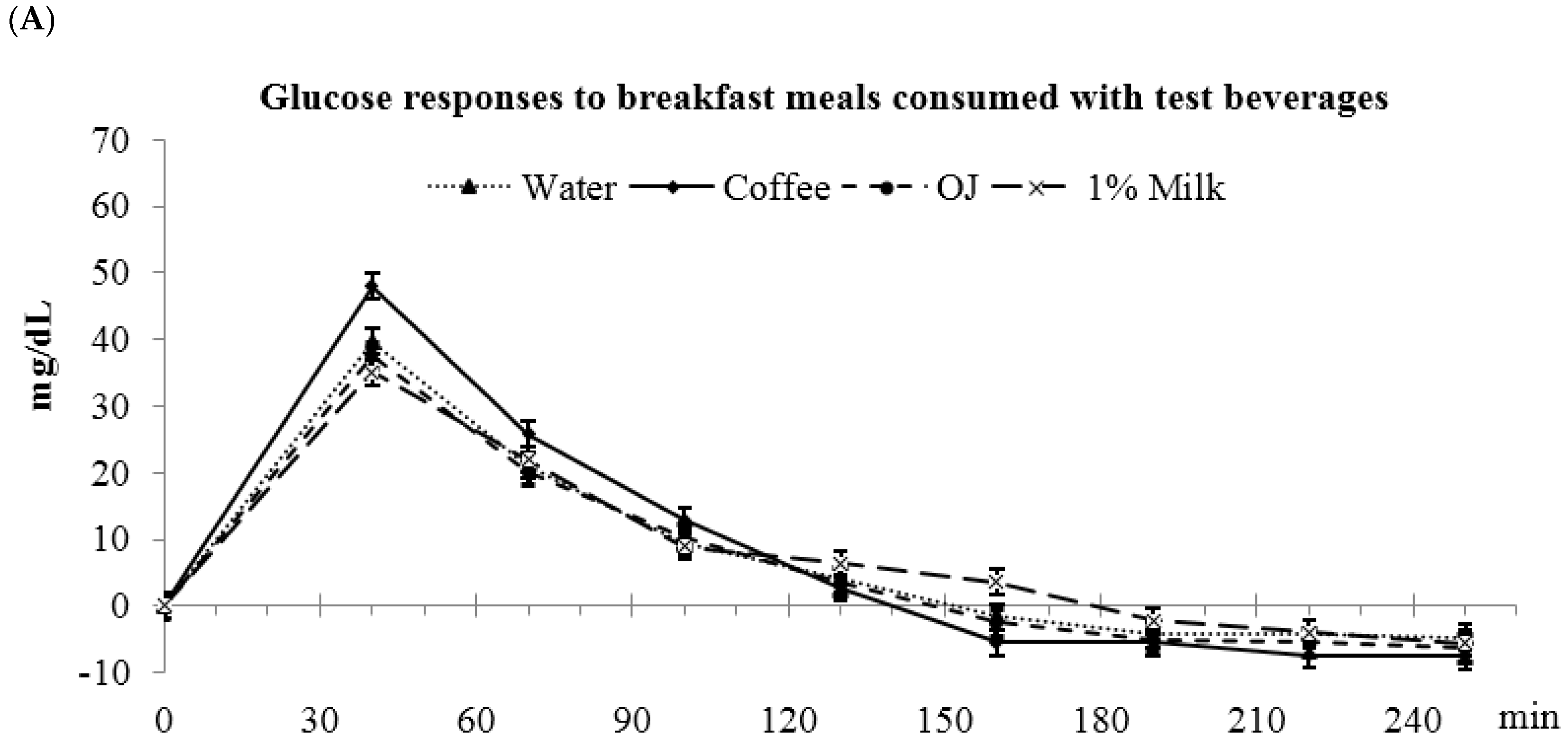
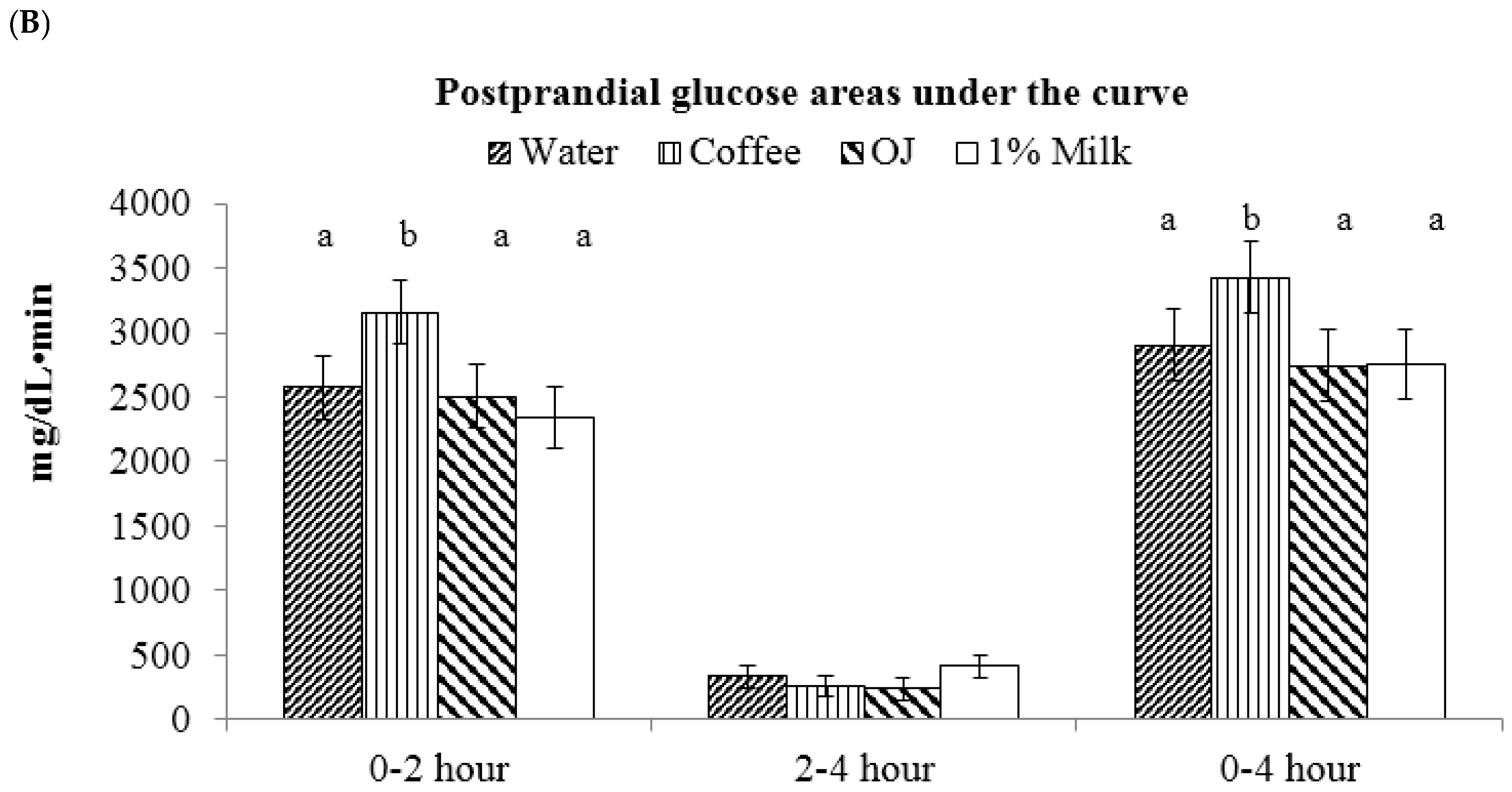
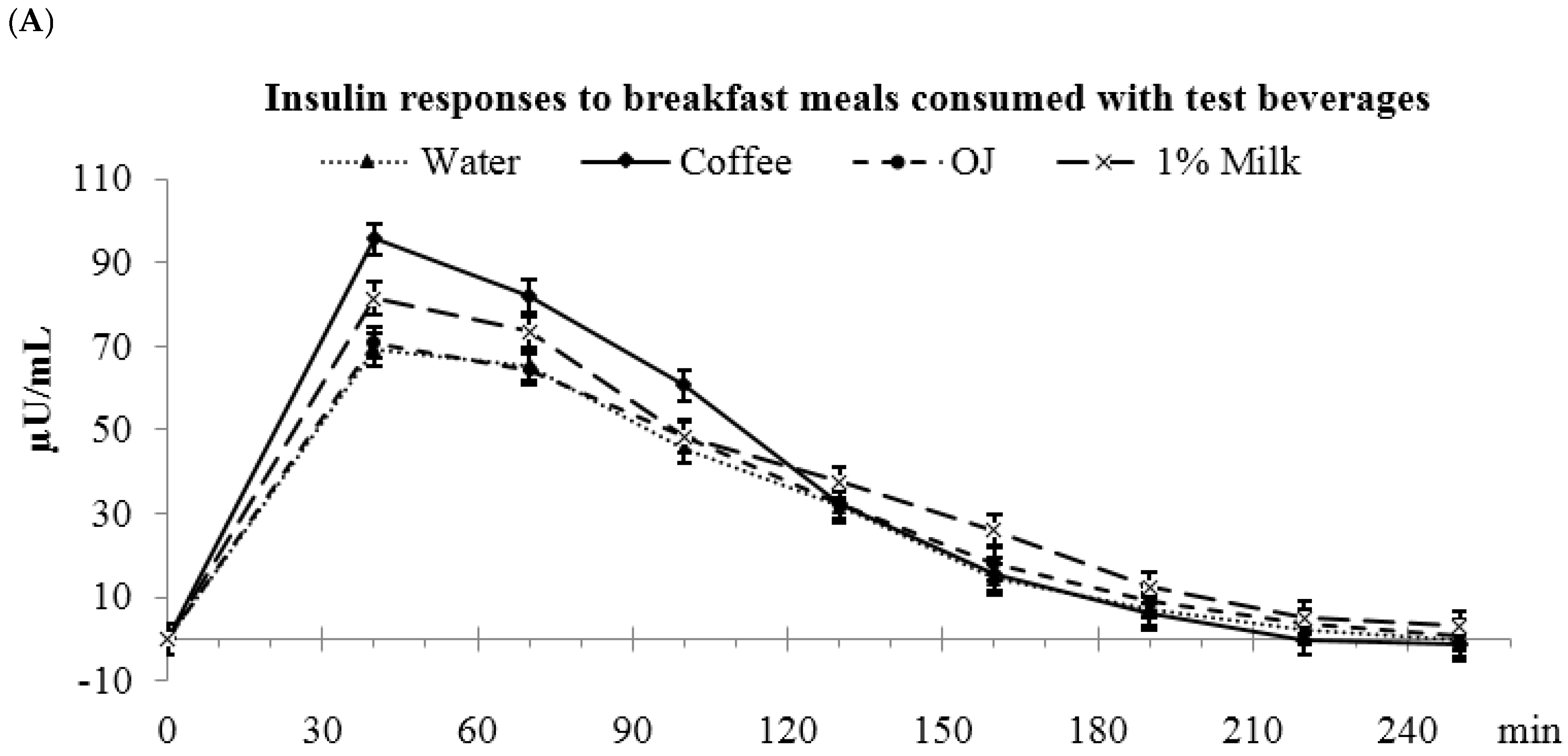
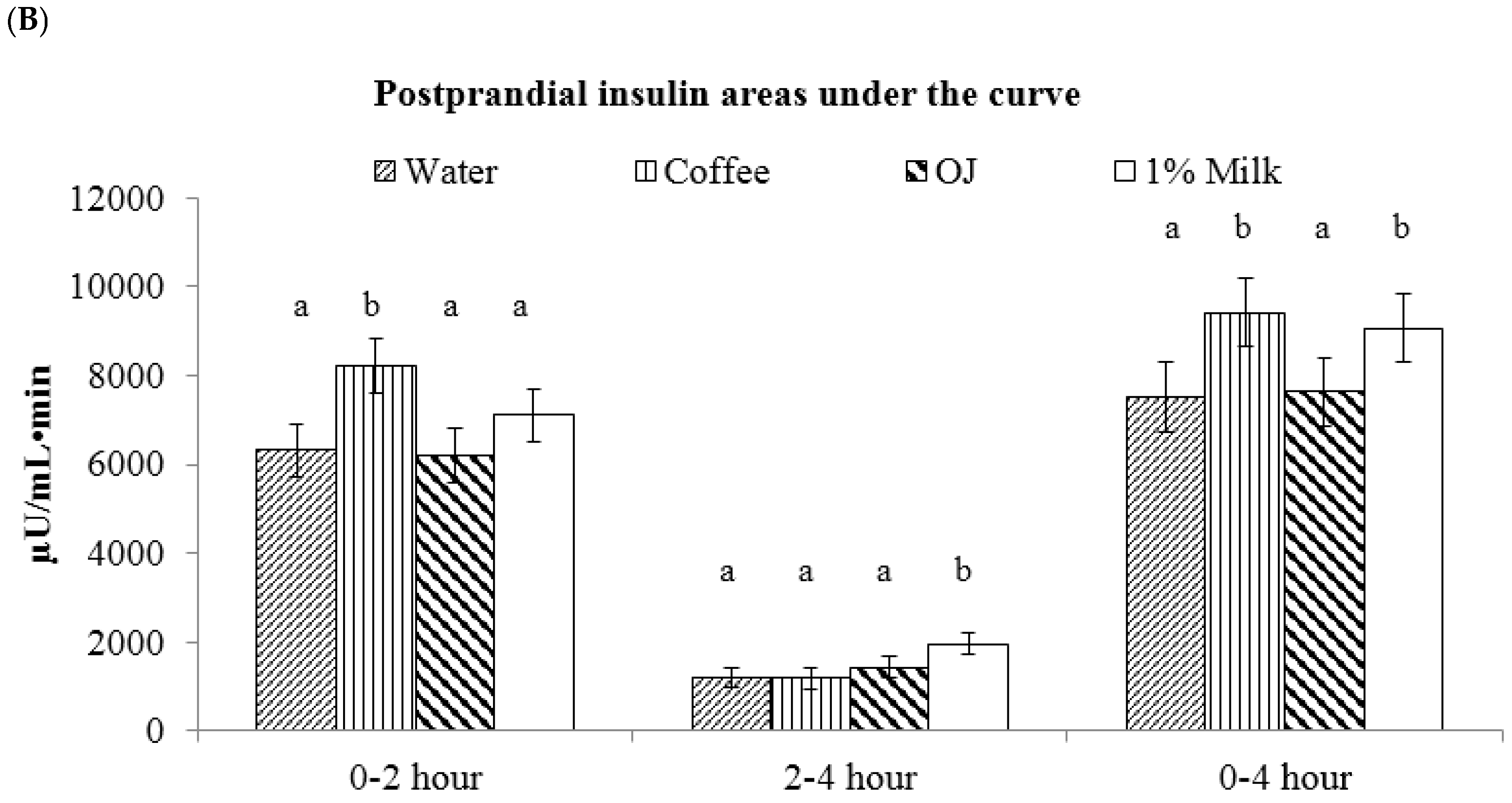
3.4. Low-Fat Milk vs. Sugar-Sweetened Coffee vs. Reduced-Energy Orange Juice
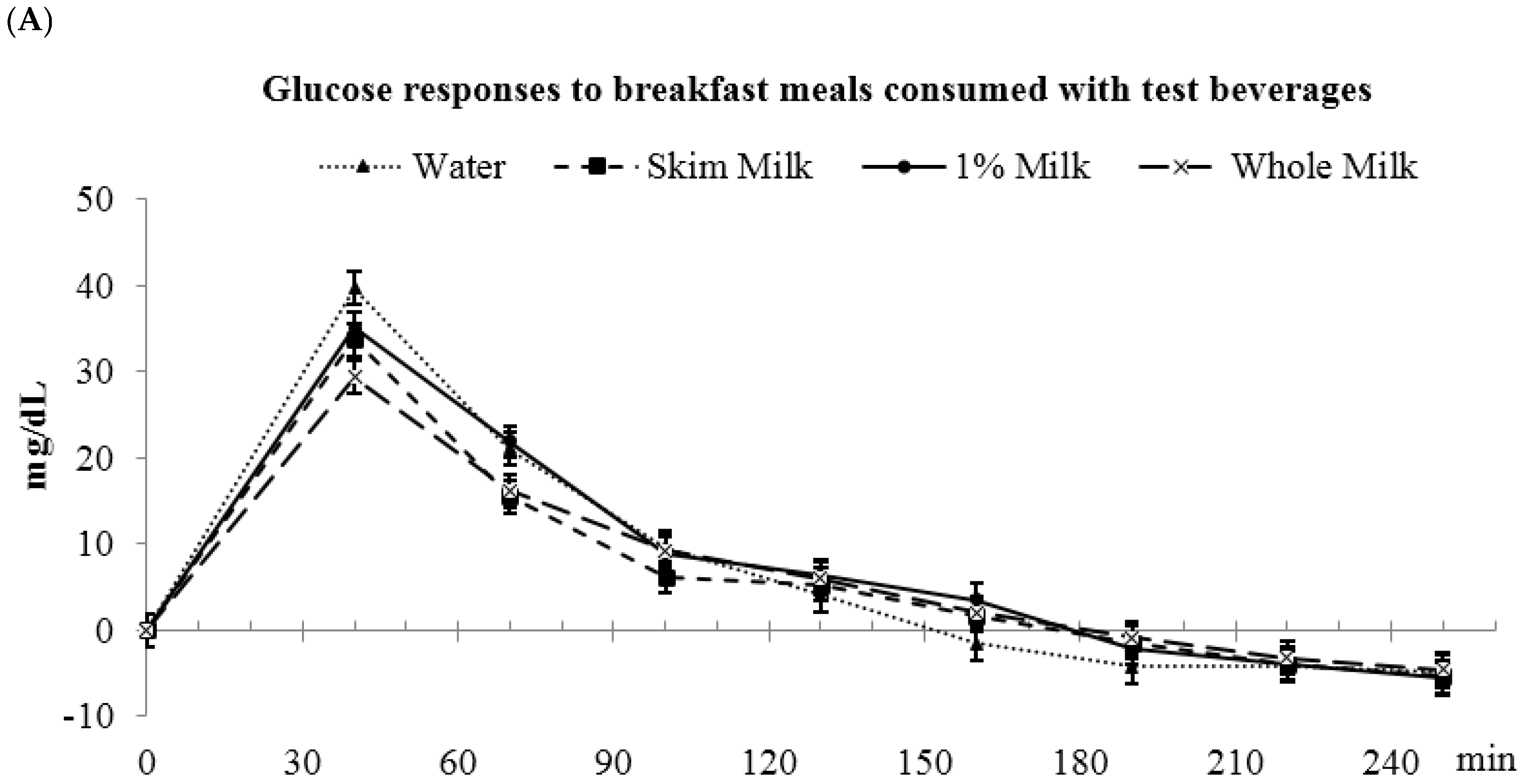
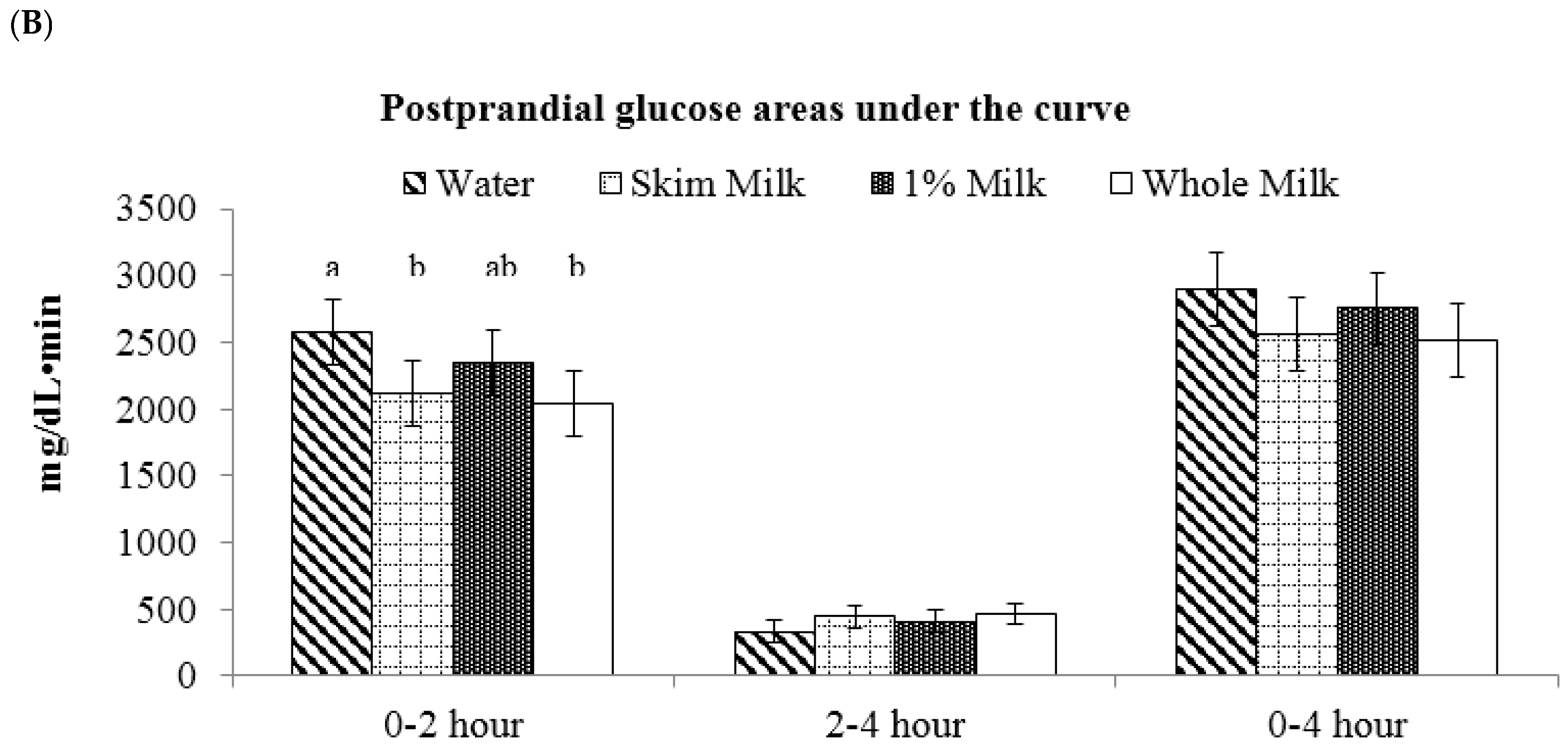
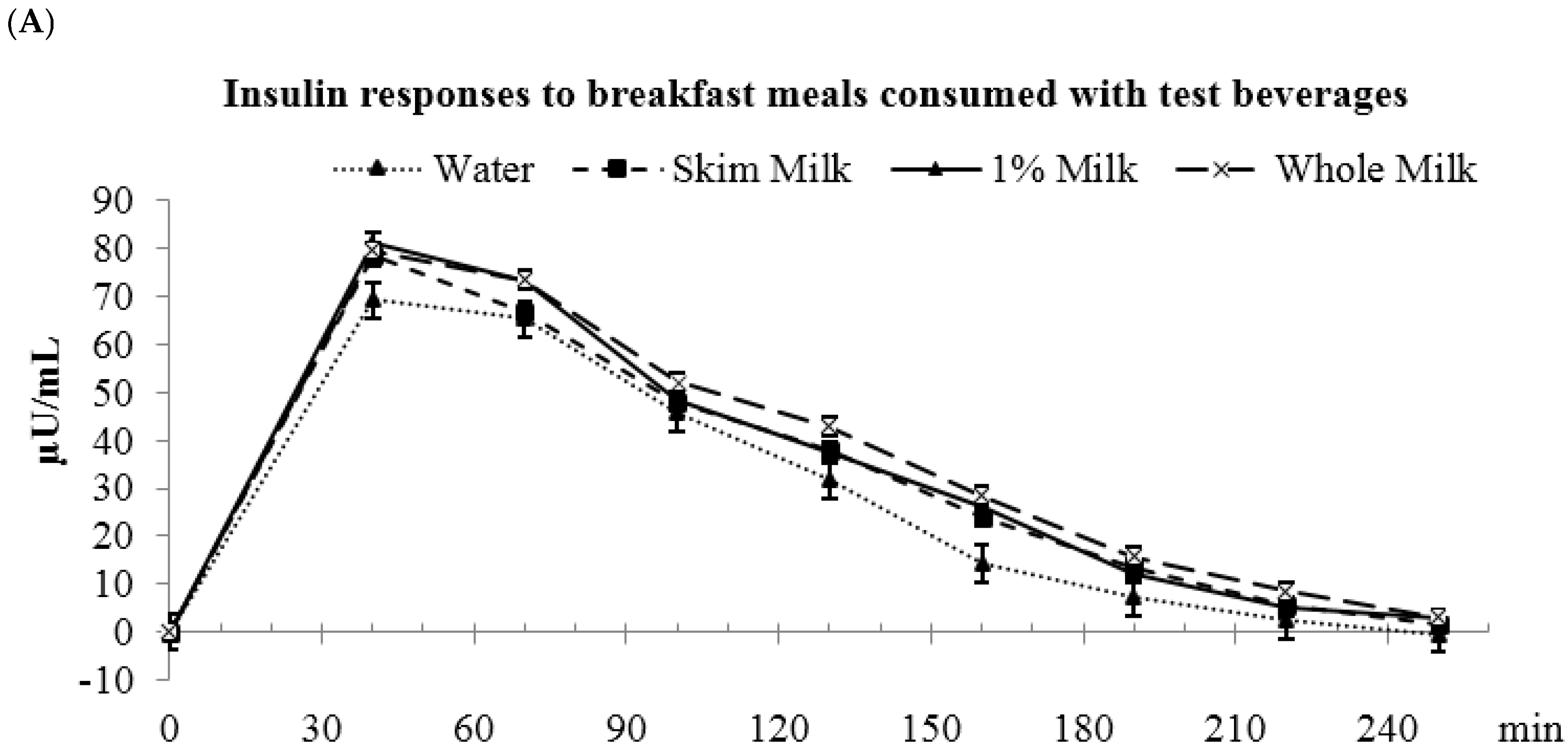
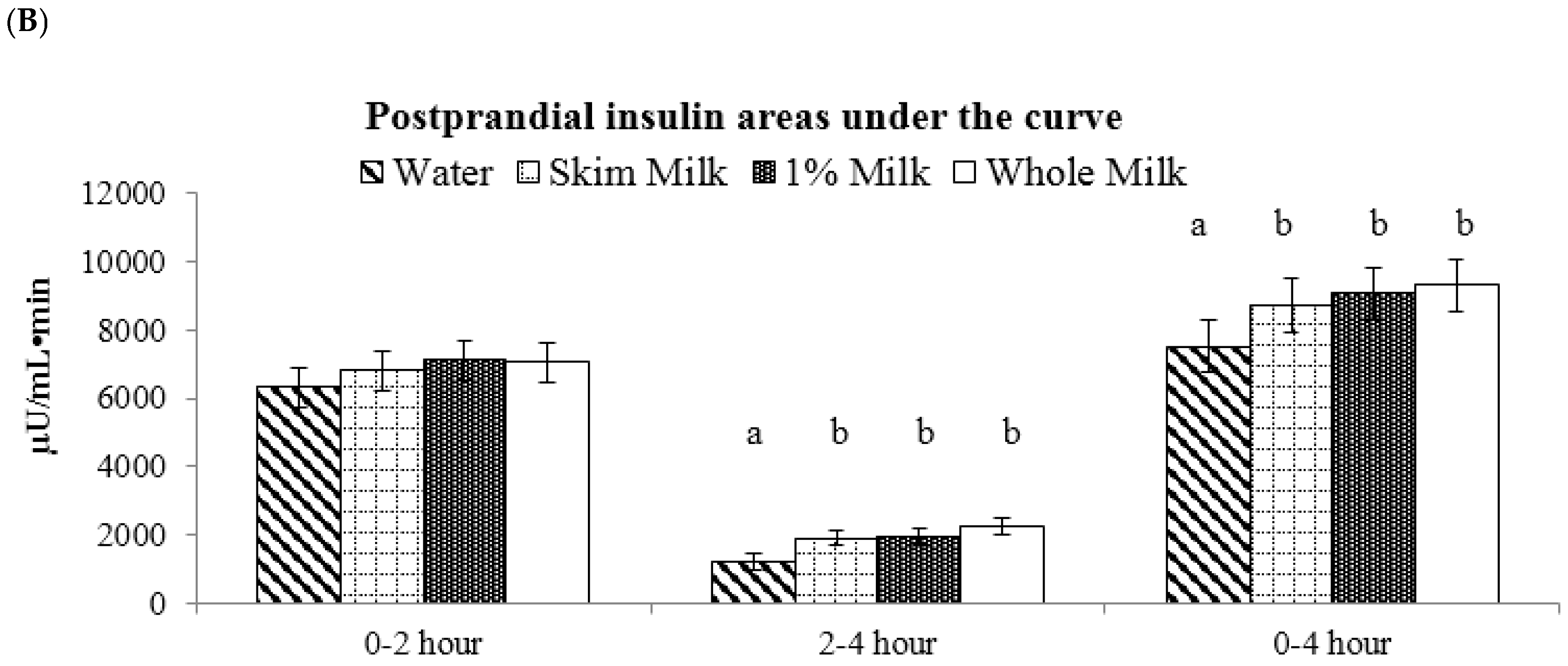
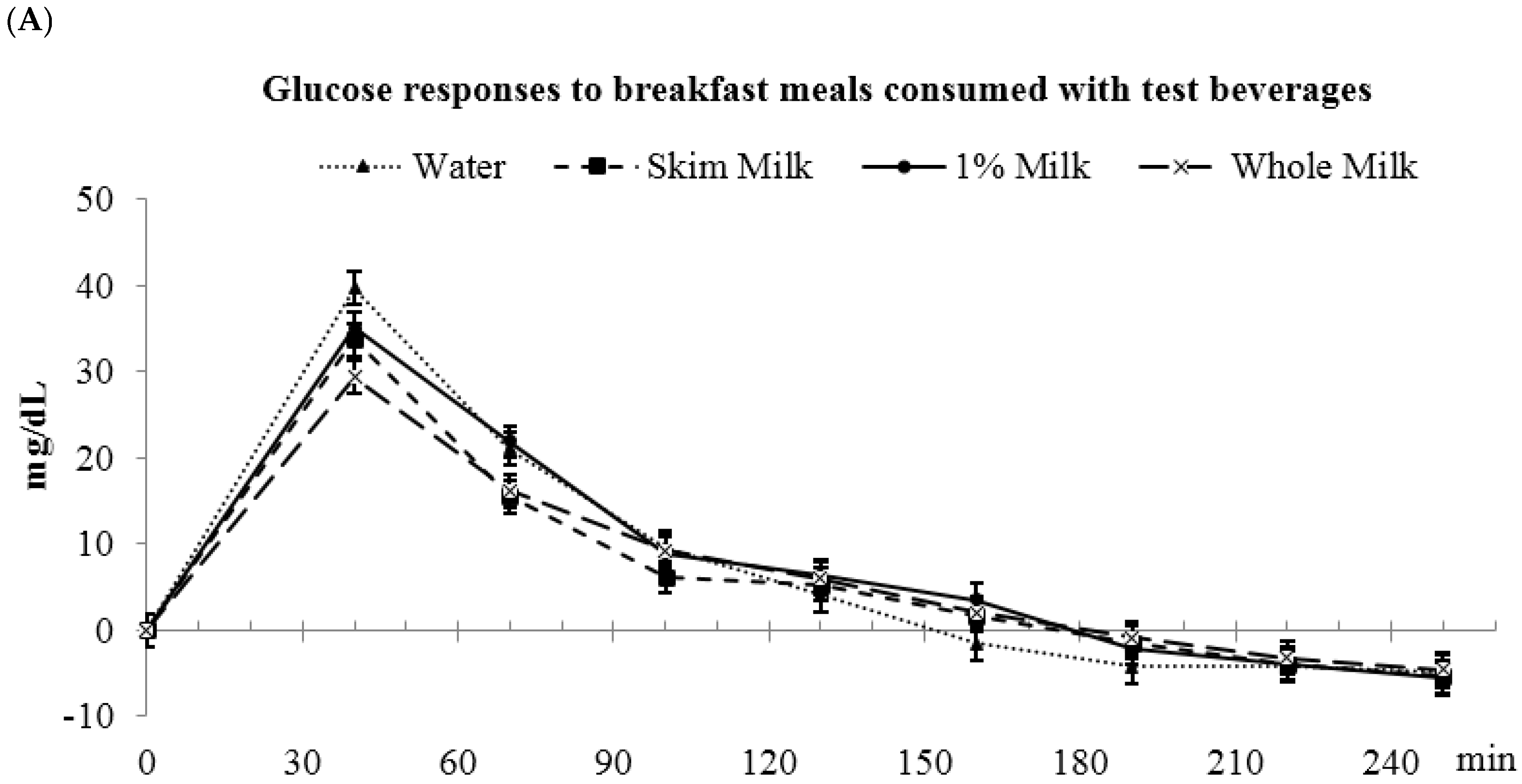
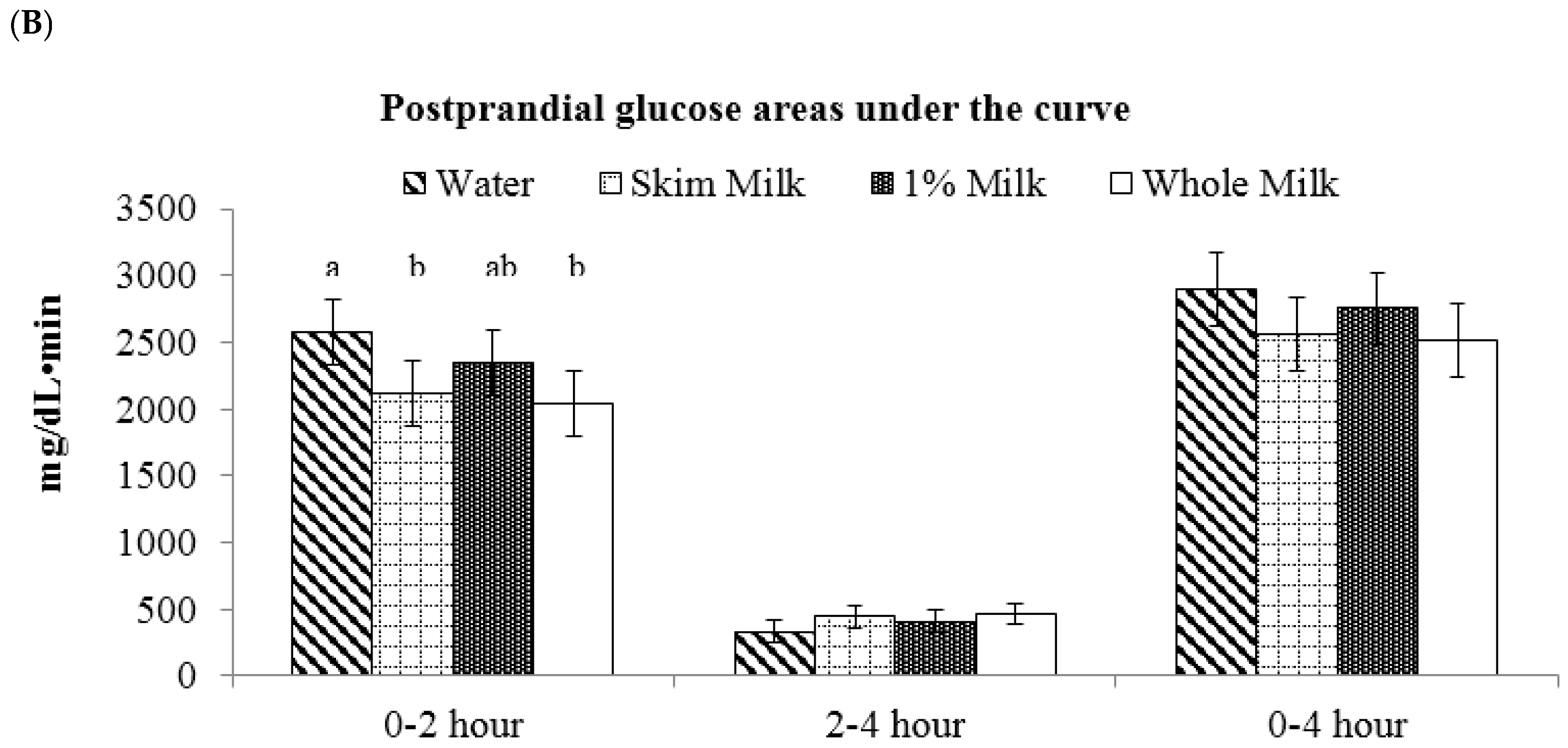
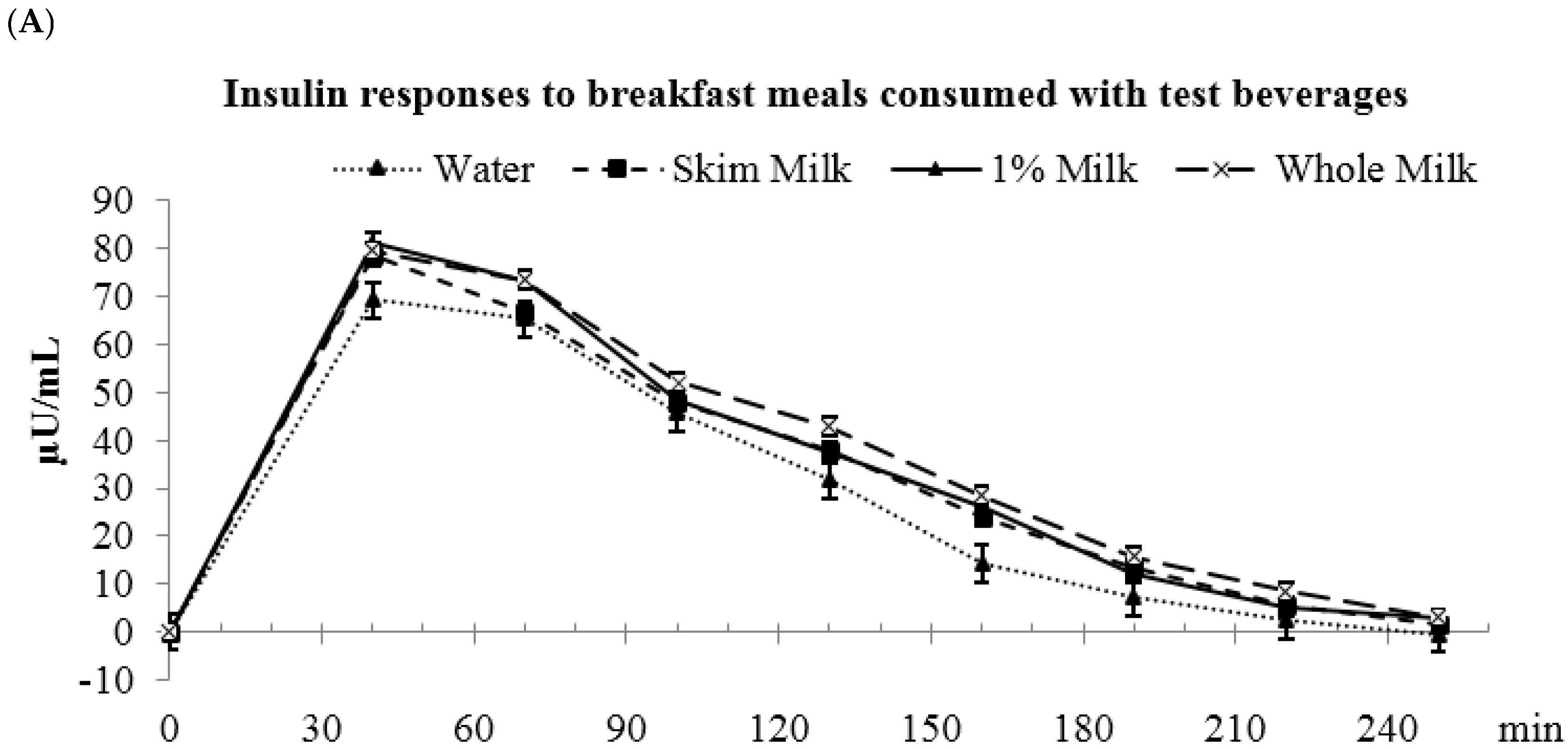
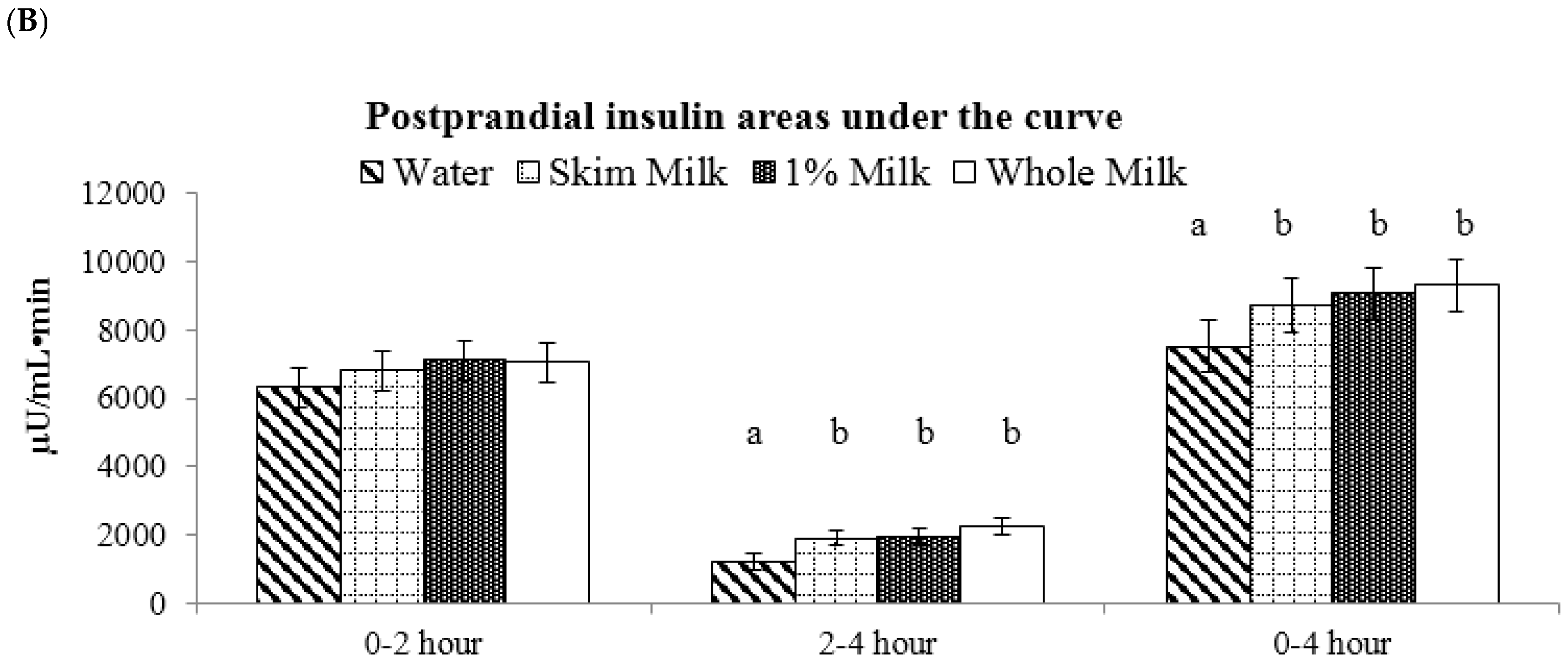
3.5. Fat-Free vs. Low-Fat vs. Whole Milk
4. Discussion
4.1. Aim 1: Low-Fat Milk vs. Sugar-Sweetened Coffee vs. Reduced-Energy Orange Juice
4.2. Aim 2: Fat-Free vs. Low-Fat vs. Whole Milk
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| AUC | Incremental area under the curve |
| OJ | Reduced-energy orange juice |
| HOMA-IR | Homeostatic model assessment-Insulin resistance |
| HOMA-β | Homeostatic model assessment-β cell function |
References
- LaComb, R.P.; Sebastian, S.R.; Enns, C.W.; Goldman, J.D. Beverage Choices of U.S. Adults: What We Eat in America, NHANES 2007–2008; Food Surveys Research Group Dietary Data Brief No. 6; U.S. Department of Agriculture: Washington, DC, USA, 2011.
- Collier, G.R.; Wolever, T.M.; Wong, G.S.; Josse, R.G. Prediction of glycemic response to mixed meals in noninsulin-dependent diabetic subjects. Am. J. Clin. Nutr. 1986, 44, 349–352. [Google Scholar] [PubMed]
- Wolever, T.M.; Nuttall, F.Q.; Lee, R.; Wong, G.S.; Josse, R.G.; Csima, A.; Jenkins, D.J. Prediction of the relative blood glucose response of mixed meals using the white bread glycemic index. Diabetes Care 1985, 8, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Panahi, S.; Luhovyy, B.L.; Liu, T.T.; Akhavan, T.; El Khoury, D.; Goff, H.D.; Anderson, G.H. Energy and macronutrient content of familiar beverages interact with pre-meal intervals to determine later food intake, appetite and glycemic response in young adults. Appetite 2013, 60, 154–161. [Google Scholar] [PubMed]
- Atkinson, F.S.; Foster-Powell, K.; Brand-Miller, J.C. International tables of glycemic index and glycemic load values: 2008. Diabetes Care 2008, 31, 2281–2283. [Google Scholar] [CrossRef] [PubMed]
- Hoyt, G.; Hickey, M.S.; Cordain, L. Dissociation of the glycaemic and insulinaemic responses to whole and skimmed milk. Br. J. Nutr. 2005, 93, 175–177. [Google Scholar] [CrossRef] [PubMed]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [PubMed]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2012, 35 (Suppl. 1), S64–S71. [Google Scholar]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Wolever, T.M. Effect of blood sampling schedule and method of calculating the area under the curve on validity and precision of glycaemic index values. Br. J. Nutr. 2004, 91, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Liljeberg Elmstahl, H.; Bjorck, I. Milk as a supplement to mixed meals may elevate postprandial insulinaemia. Eur. J. Clin. Nutr. 2001, 55, 994–999. [Google Scholar] [CrossRef] [PubMed]
- Moisey, L.L.; Kacker, S.; Bickerton, A.C.; Robinson, L.E.; Graham, T.E. Caffeinated coffee consumption impairs blood glucose homeostasis in response to high and low glycemic index meals in healthy men. Am. J. Clin. Nutr. 2008, 87, 1254–1261. [Google Scholar] [PubMed]
- Robinson, L.E.; Savani, S.; Battram, D.S.; McLaren, D.H.; Sathasivam, P.; Graham, T.E. Caffeine ingestion before an oral glucose tolerance test impairs blood glucose management in men with type 2 diabetes. J. Nutr. 2004, 134, 2528–2533. [Google Scholar] [PubMed]
- Graham, T.E.; Sathasivam, P.; Rowland, M.; Marko, N.; Greer, F.; Battram, D. Caffeine ingestion elevates plasma insulin response in humans during an oral glucose tolerance test. Can. J. Physiol. Pharmacol. 2001, 79, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Ostman, E.M.; Liljeberg Elmstahl, H.G.; Bjorck, I.M. Inconsistency between glycemic and insulinemic responses to regular and fermented milk products. Am. J. Clin. Nutr. 2001, 74, 96–100. [Google Scholar] [PubMed]
- Nilsson, M.; Stenberg, M.; Frid, A.H.; Holst, J.J.; Bjorck, I.M. Glycemia and insulinemia in healthy subjects after lactose-equivalent meals of milk and other food proteins: The role of plasma amino acids and incretins. Am. J. Clin. Nutr. 2004, 80, 1246–1253. [Google Scholar] [PubMed]
- Van Meijl, L.E.; Mensink, R.P. Effects of milk and milk constituents on postprandial lipid and glucose metabolism in overweight and obese men. Br. J. Nutr. 2013, 110, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Ghanim, H.; Sia, C.L.; Upadhyay, M.; Korzeniewski, K.; Viswanathan, P.; Abuaysheh, S.; Mohanty, P.; Dandona, P. Orange juice neutralizes the proinflammatory effect of a high-fat, high-carbohydrate meal and prevents endotoxin increase and toll-like receptor expression. Am. J. Clin. Nutr. 2010, 91, 940–949. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.J.; Leeds, A.R.; Gassull, M.A.; Cochet, B.; Alberti, G.M. Decrease in postprandial insulin and glucose concentrations by guar and pectin. Ann. Intern. Med. 1977, 86, 20–23. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Beverage Consumed with Meal | Beverage Only | Whole Meal (Beverage + Sandwich) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Energy (kcal) | Total CHO * (g) | CHO Source | Dietary Fiber (g) | Fat (g) | Protein (g) | Energy (kcal) | Total CHO (g) | Dietary Fiber | |
| Water (Control) | 0 | 0 | NA | 0 | 0 | 0 | 422 | 48 | 2.0 |
| Sugar-Sweetened Coffee | 50 | 12 | Sucrose | 0.1 | 0.1 | 0.3 | 472 (422 + 50) | 60 | 2.1 |
| Orange Juice (Trop 50) | 50 | 12 | Sucrose, fructose, glucose | 0.2 | 0 | 0.6 | 472 (422 + 50) | 60 | 2.2 |
| Fat-Free Milk | 82 | 12 | Lactose | 0 | 0 | 8 | 504 (422 + 82) | 60 | 2.0 |
| Low-Fat Milk | 101 | 12 | Lactose | 0 | 2 | 8 | 523 (422 + 101) | 60 | 2.0 |
| Whole Milk | 159 | 12 | Lactose | 0 | 9 | 9 | 581 (422 + 159) | 60 | 2.0 |
| Parameter | All * (n = 46) | Normal (n = 29) | Prediabetes (n = 17) | p # |
|---|---|---|---|---|
| Age (year) | 50 ± 1.4 | 50 ± 1.8 | 49 ± 2.5 | 0.85 |
| Gender | 33F/13M | 20F/9M | 13F/4M | |
| BMI & (kg/m2) | 32.5 ± 0.7 | 32.2 ± 0.8 | 33.0 ± 1.2 | 0.57 |
| Glucose, serum (mg/dL) | 94.0 ± 1.4 | 89.6 ± 1.5 | 95.3 ± 2.0 | 0.02 |
| Glycated hemoglobin A1c (%) ‡ | 5.6 ± 0.04 | 5.4 ± 0 | 5.9 ± 0.1 | <0.0001 |
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Janle, E.; Campbell, W.W. Postprandial Glycemic and Insulinemic Responses to Common Breakfast Beverages Consumed with a Standard Meal in Adults Who Are Overweight and Obese. Nutrients 2017, 9, 32. https://doi.org/10.3390/nu9010032
Li J, Janle E, Campbell WW. Postprandial Glycemic and Insulinemic Responses to Common Breakfast Beverages Consumed with a Standard Meal in Adults Who Are Overweight and Obese. Nutrients. 2017; 9(1):32. https://doi.org/10.3390/nu9010032
Chicago/Turabian StyleLi, Jia, Elsa Janle, and Wayne W. Campbell. 2017. "Postprandial Glycemic and Insulinemic Responses to Common Breakfast Beverages Consumed with a Standard Meal in Adults Who Are Overweight and Obese" Nutrients 9, no. 1: 32. https://doi.org/10.3390/nu9010032
APA StyleLi, J., Janle, E., & Campbell, W. W. (2017). Postprandial Glycemic and Insulinemic Responses to Common Breakfast Beverages Consumed with a Standard Meal in Adults Who Are Overweight and Obese. Nutrients, 9(1), 32. https://doi.org/10.3390/nu9010032