Sources of Caffeine in Diets of US Children and Adults: Trends by Beverage Type and Purchase Location

Abstract
:1. Introduction
2. Methods
2.1. Dietary Intake Data
2.2. Classification of Caffeine Sources
2.3. Purchase Locations of Origin
2.4. Statistical Analysis
3. Results
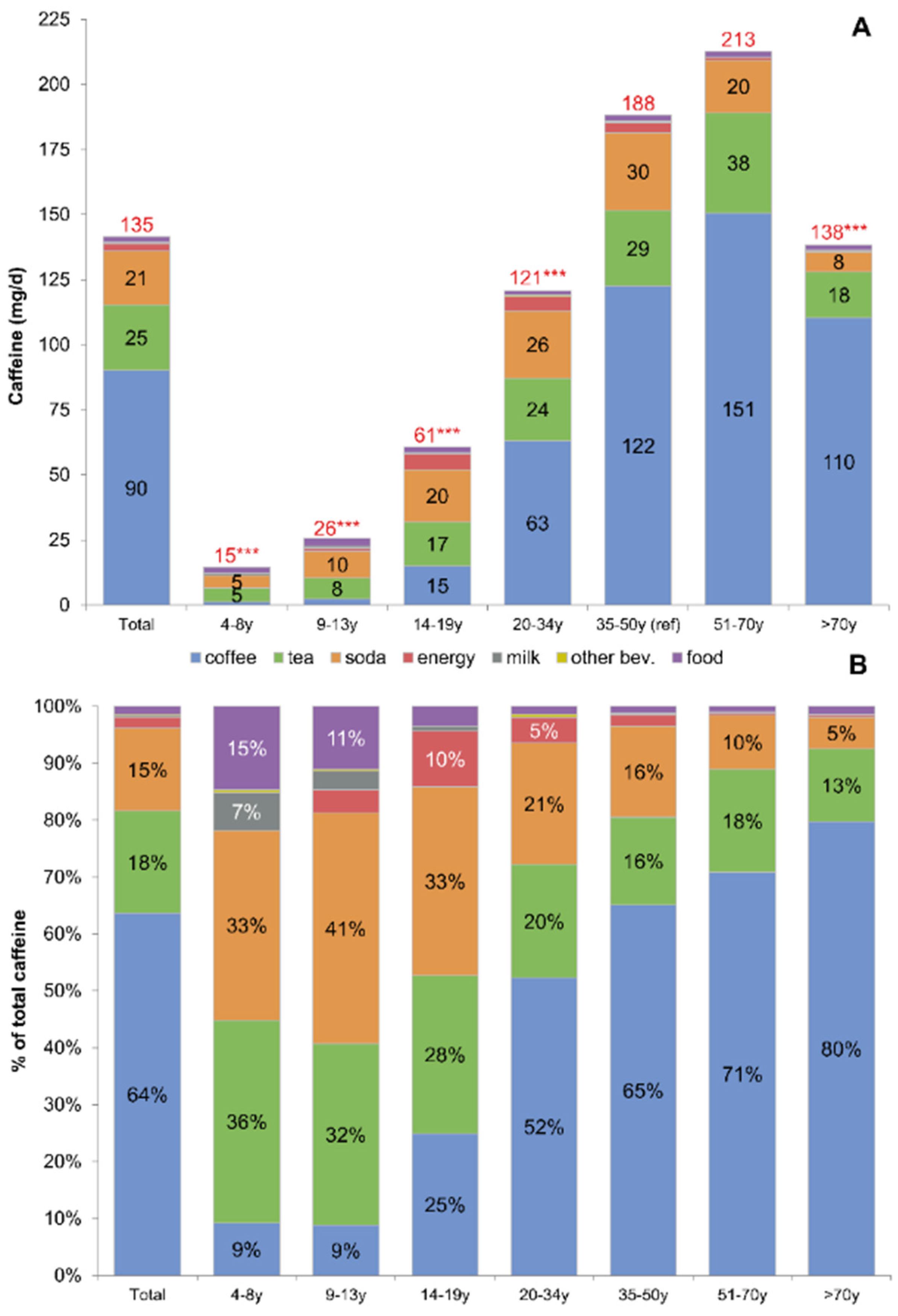
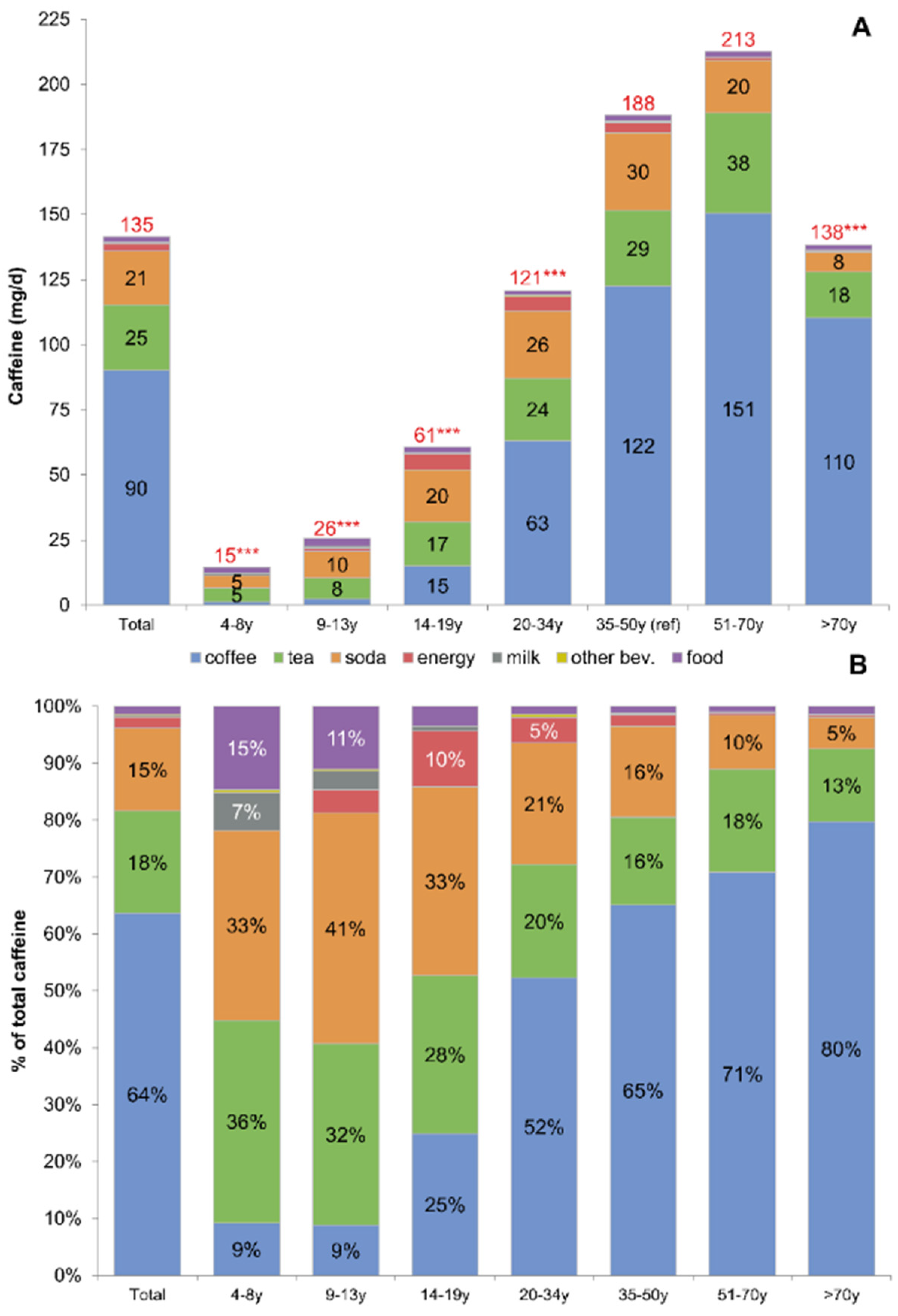
3.1. Current Patterns of Caffeine Consumption
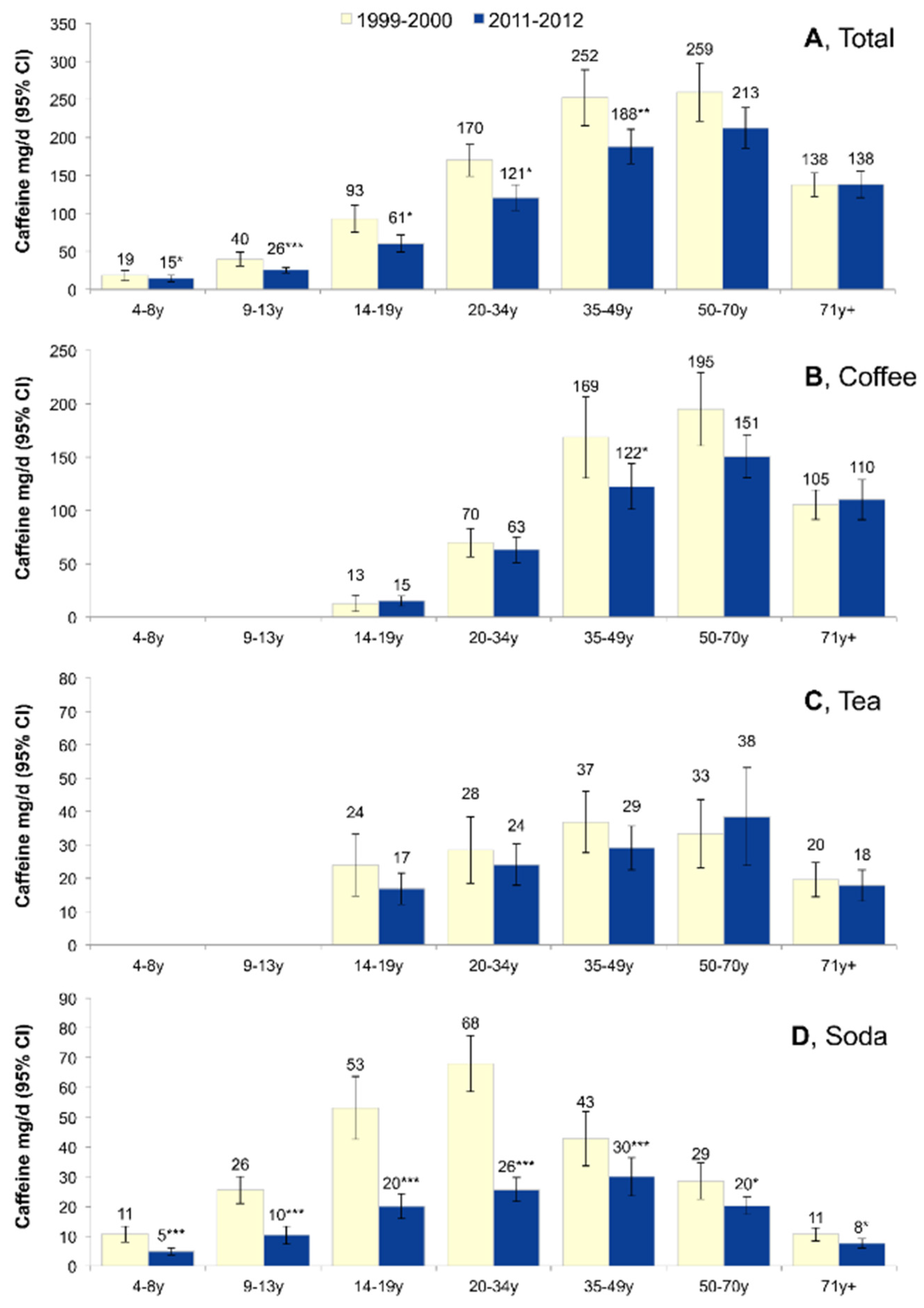
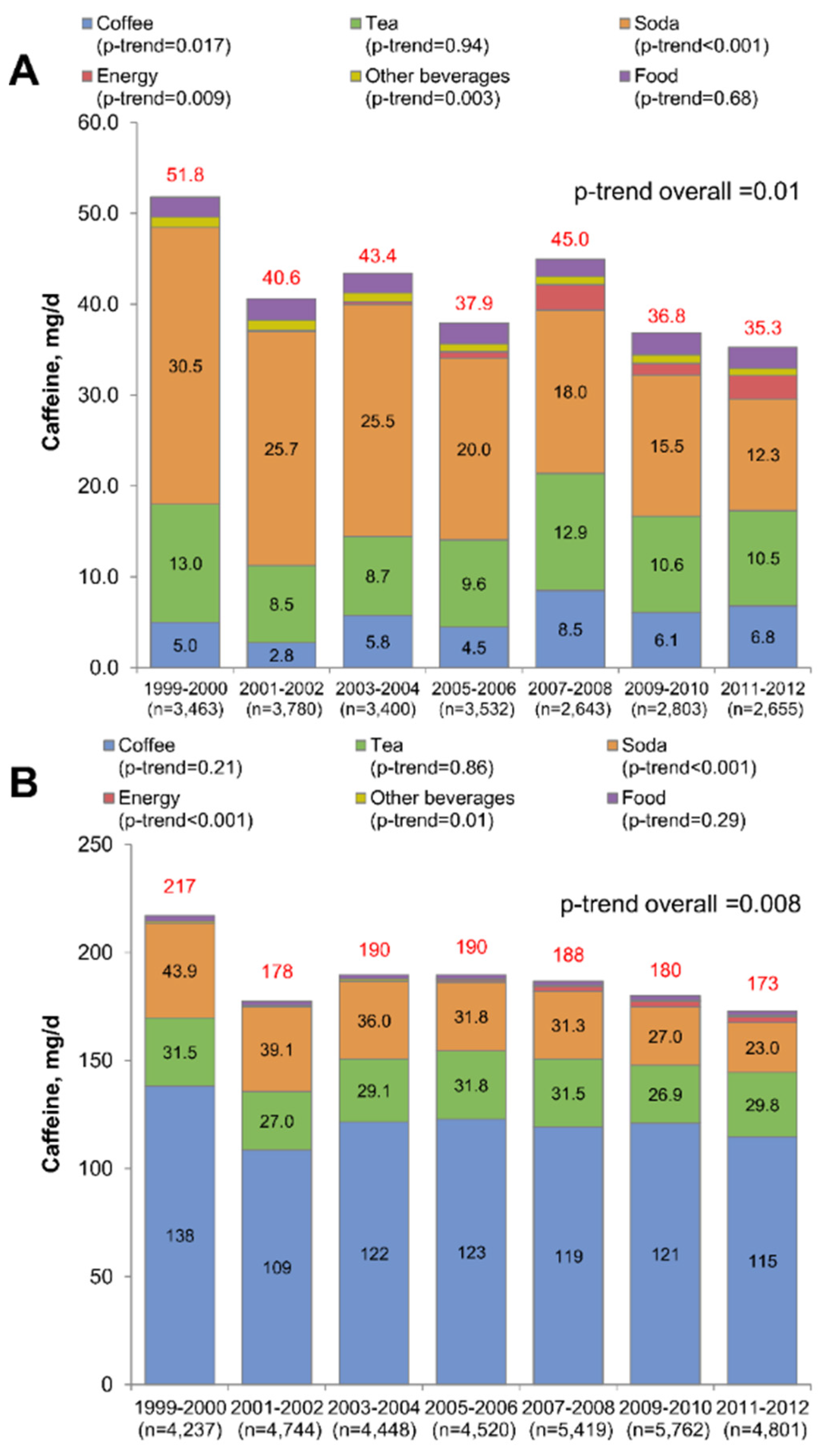
3.2. Fourteen-Year Trends in Caffeine Consumption
3.3. Fourteen-Year Trends in Caffeine Consumption by Age Group
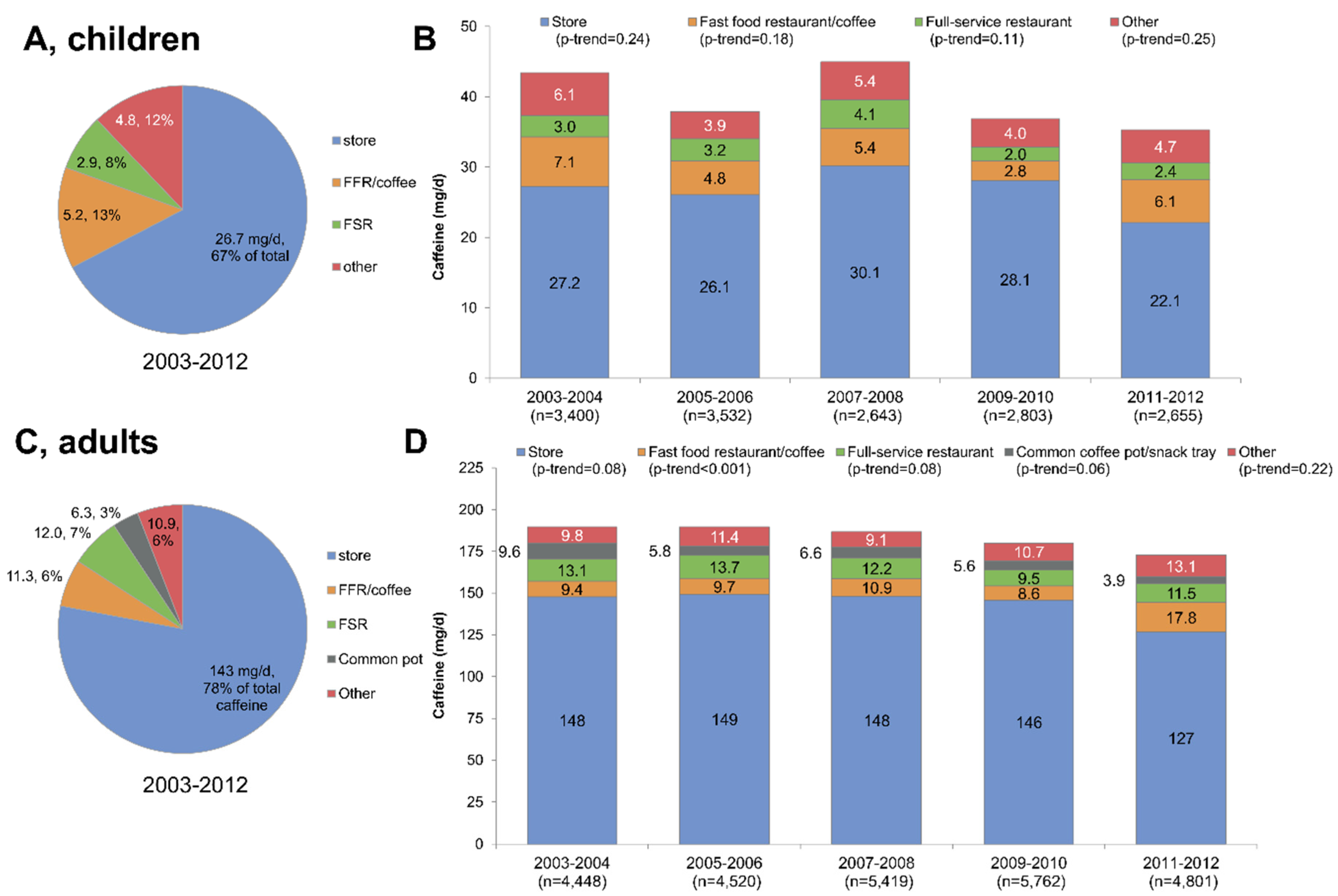
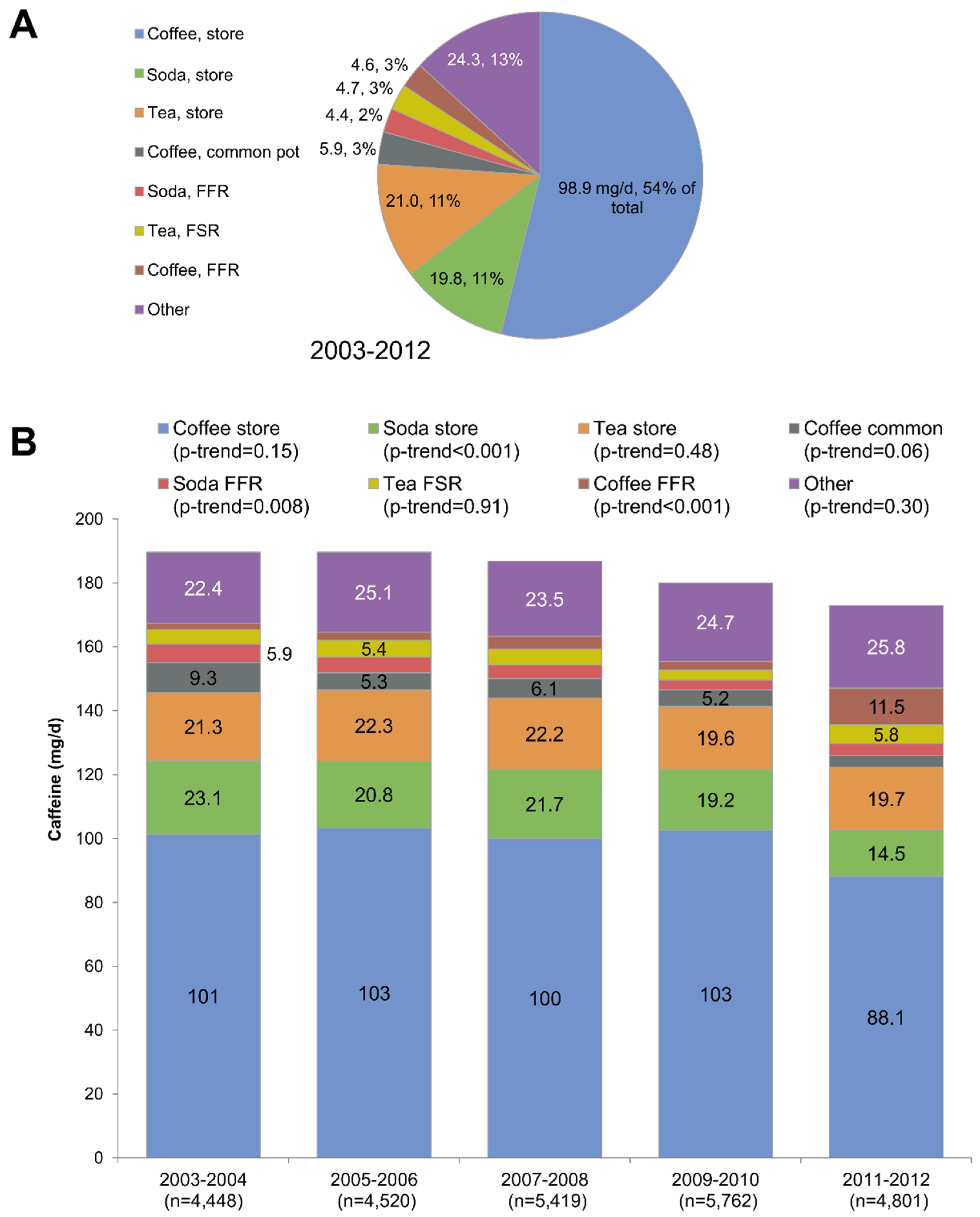
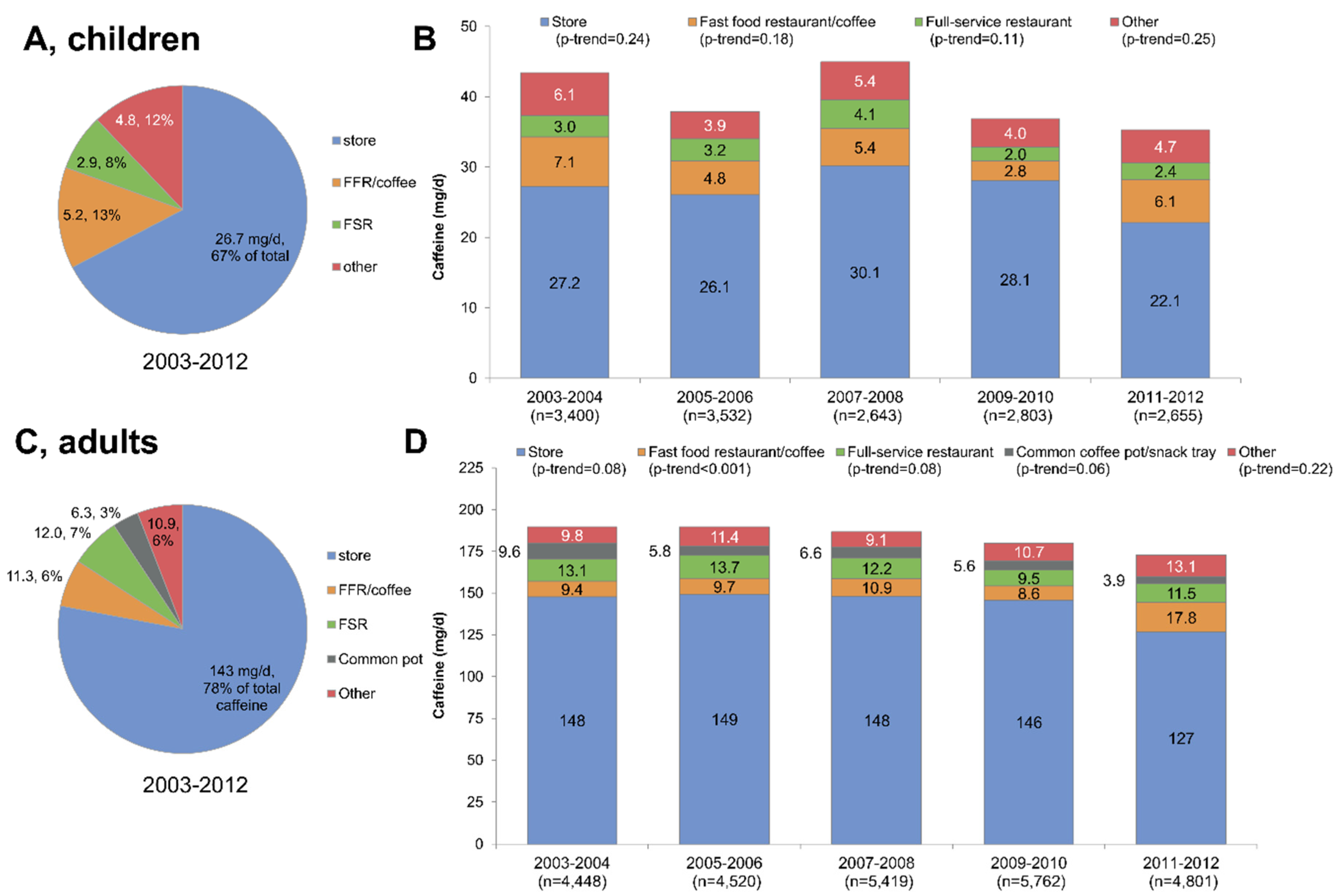
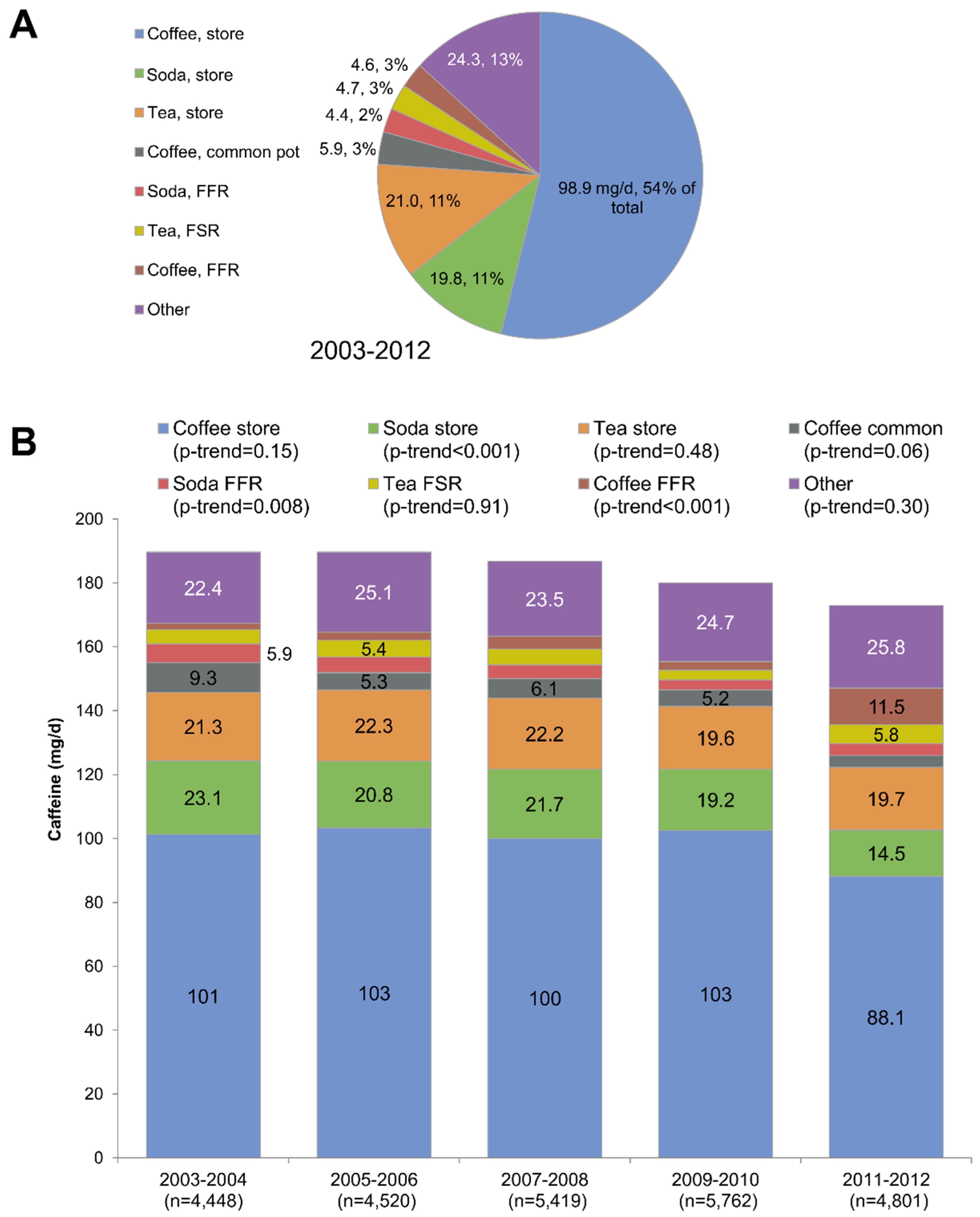
3.4. Trends in Location of Origin for Caffeine, 2003–2012
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| NHANES | National Health and Nutrition Examination Survey |
| USDA | United States Department of Agriculture |
| FNDDS | Food and Nutrient Database for Dietary Studies |
References
- Barone, J.J.; Roberts, H.R. Caffeine consumption. Food Chem. Toxicol. 1996, 34, 119–129. [Google Scholar] [CrossRef]
- Heckman, M.A.; Weil, J.; Gonzalez de Mejia, E. Caffeine (1,3,7-trimethylxanthine) in foods: A comprehensive review on consumption, functionality, safety, and regulatory matters. J. Food Sci. 2010, 75, R77–R87. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, D.C.; Knight, C.A.; Hockenberry, J.; Teplansky, R.; Hartman, T.J. Beverage caffeine intakes in the U.S. Food Chem. Toxicol. 2014, 63, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Knight, C.A.; Knight, I.; Mitchell, D.C.; Zepp, J.E. Beverage caffeine intake in US consumers and subpopulations of interest: Estimates from the Share of Intake Panel survey. Food Chem. Toxicol. 2004, 42, 1923–1930. [Google Scholar] [CrossRef] [PubMed]
- Knight, C.A.; Knight, I.; Mitchell, D.C. Beverage caffeine intakes in young children in Canada and the US. Can. J. Diet. Pract. Res. 2006, 67, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; Saldanha, L.G.; Gahche, J.J.; Dwyer, J.T. Estimating caffeine intake from energy drinks and dietary supplements in the United States. Nutr. Rev. 2014, 72, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Somogyi, L. Caffeine Intake by the U.S. Population. 2010. Available online: http://www.fda.gov/downloads/AboutFDA/CentersOffices/OfficeofFoods/CFSAN/CFSANFOIAElectronicReadingRoom/UCM333191.pdf (accessed on 6 August 2014). [Google Scholar]
- United States Food and Drug Administration. FDA to Investigate Added Caffeine. Available online: http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm350570.htm (accessed on 28 November 2014).
- LPDAAC. U.S. Department of Agriculture. Scientific Report of the 2015 Dietary Guidelines Advisory Committee. 2015. Available online: http://www.health.gov/dietaryguidelines/2015-scientific-report/PDFs/Scientific-Report-of-the-2015-Dietary-Guidelines-Advisory-Committee.pdf (accessed on 17 March 2015). [Google Scholar]
- Higdon, J.V.; Frei, B. Coffee and health: A review of recent human research. Crit. Rev. Food Sci. Nutr. 2006, 46, 101–123. [Google Scholar] [CrossRef] [PubMed]
- Branum, A.M.; Rossen, L.M.; Schoendorf, K.C. Trends in caffeine intake among U.S. children and adolescents. Pediatrics 2014, 133, 386–393. [Google Scholar] [CrossRef] [PubMed]
- Heckman, M.A.; Sherry, K.; de Mejia, E.G. Energy Drinks: An Assessment of Their Market Size, Consumer Demographics, Ingredient Profile, Functionality, and Regulations in the United States. Compr. Rev. Food Sci. Food Saf. 2010, 9, 303–317. [Google Scholar] [CrossRef]
- Lieberman, H.R.; Stavinoha, T.; McGraw, S.; White, A.; Hadden, L.; Marriott, B.P. Caffeine use among active duty US Army soldiers. J. Acad. Nutr. Diet. 2012, 112, 902–912. [Google Scholar] [CrossRef] [PubMed]
- Kit, B.K.; Fakhouri, T.H.; Park, S.; Nielsen, S.J.; Ogden, C.L. Trends in sugar-sweetened beverage consumption among youth and adults in the United States: 1999–2010. Am. J. Clin. Nutr. 2013, 98, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, N.; Herrick, K.; Moshfegh, A.; Rybak, M. Caffeine intake in children in the United States and 10-year trends: 2001–2010. Am. J. Clin. Nutr. 2014, 100, 1124–1132. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). NHANES Response Rates and Population Totals. 2013. Available online: http://www.cdc.gov/nchs/nhanes/response_rates_CPS.htm (accessed on 15 July 2013). [Google Scholar]
- Centers for Disease Control and Prevention (CDC); National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data (2003–4; 2005–6; 2007–8). 2014. Available online: http://www.cdc.gov/nchs/nhanes/nhanes_questionnaires.htm (accessed on 7 July 2013). [Google Scholar]
- Centers for Disease Control and Prevention (CDC); National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey 2003–2004: Documentation, Codebook and Frequencies, Dietary Interview and Individual Foods (First Day). Available online: http://www.cdc.gov/nchs/data/nhanes/nhanes_03_04/dr1iff_c.pdf (accessed on 8 July 2013).
- Centers for Disease Control and Prevention (CDC); National Center for Health Statistics. NCHS Research Ethics Review Board (ERB) Approval. 2012. Available online: http://www.cdc.gov/nchs/nhanes/irba98.htm (accessed on 28 November 2014). [Google Scholar]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [PubMed]
- U.S. Department of Agriculture. The USDA Food and Nutrient Database for Dietary Studies, 2.0. 2006. Available online: http://www.ars.usda.gov/SP2UserFiles/Place/80400530/pdf/fndds2_doc.pdf (accessed on 10 April 2014). [Google Scholar]
- United States Department of Agriculture; Agricultural Research Service; Food Surveys Research Group. Overview of the What We Eat in America Food Categories. Available online: http://www.ars.usda.gov/services/docs.htm?docid=23429 (accessed on 28 November 2014).
- Drewnowski, A.; Rehm, C.D. Consumption of added sugars among US children and adults by food purchase location and food source. Am. J. Clin. Nutr. 2014, 100, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Fulgoni, V.L.; Keast, D.R.; Lieberman, H.R. Trends in intake and sources of caffeine in the diets of US adults: 2001–2010. Am. J. Clin. Nutr. 2015, 101, 1081–1087. [Google Scholar] [CrossRef] [PubMed]
- Lachenmeier, D.W.; Wegert, K.; Kuballa, T.; Schneider, R.; Ruge, W.; Reusch, H.; Alexy, U.; Kersting, M.; Winkler, G. Caffeine intake from beverages in German children, adolescents, and adults. J. Caffeine Res. 2013, 3, 47–53. [Google Scholar] [CrossRef]
- Drewnowski, A.; Rehm, C.D. Socio-demographic correlates and trends in low-calorie sweetener use among adults in the United States from 1999 to 2008. Eur. J. Clin. Nutr. 2015, 69, 1035–1041. [Google Scholar] [CrossRef] [PubMed]
- Frary, C.D.; Johnson, R.K.; Wang, M.Q. Food sources and intakes of caffeine in the diets of persons in the United States. J. Am. Diet. Assoc. 2005, 105, 110–113. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age 4–19 Years (n = 2655) | Age ≥ 20 Years (n = 4801) | |||||
|---|---|---|---|---|---|---|
| n | Mean | 95% CI | n | Mean | 95% CI | |
| Total | 2655 | 35 | 31, 39 | 4801 | 173 | 154, 192 |
| Gender | ||||||
| Male (ref) | 1357 | 36 | 31, 43 | 2394 | 196 | 165, 226 |
| Female | 1298 | 34 | 28, 40 | 2407 | 151 *** | 138, 164 |
| Race/ethnicity a | ||||||
| Non-Hispanic White (ref) | 605 | 47 | 38, 55 | 1842 | 205 | 185, 225 |
| Non-Hispanic Black | 784 | 20 *** | 15, 25 | 1274 | 78 *** | 65, 92 |
| Non-Hispanic Asian | 317 | 26 *** | 18, 34 | 610 | 108 *** | 93, 122 |
| Mexican American | 504 | 23 *** | 17, 29 | 467 | 117 *** | 96, 139 |
| Other Hispanic | 303 | 24 *** | 20, 29 | 465 | 110 *** | 86, 135 |
| Family income-to-poverty ratio | ||||||
| <1.3 | 1167 | 36 | 26, 47 | 1564 | 146 * | 117, 176 |
| 1.3–1.849 | 335 | 38 | 26, 51 | 594 | 164 | 138, 191 |
| 1.85–2.99 | 350 | 31 | 22, 40 | 702 | 186 | 159, 214 |
| ≥3.0 (ref) | 617 | 33 | 27, 40 | 1574 | 189 | 165, 213 |
| Educational attainment b | ||||||
| <HS | 1044 | 171 | 131, 212 | |||
| High school | 904 | 185 | 150, 221 | |||
| Some college | 1210 | 198 * | 176, 220 | |||
| ≥College graduate (ref) | 1158 | 173 | 152, 194 | |||
| Employment status | ||||||
| Employed (ref) | 2565 | 186 | 171, 200 | |||
| Not employed | 2235 | 158 * | 131, 184 | |||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drewnowski, A.; Rehm, C.D. Sources of Caffeine in Diets of US Children and Adults: Trends by Beverage Type and Purchase Location. Nutrients 2016, 8, 154. https://doi.org/10.3390/nu8030154
Drewnowski A, Rehm CD. Sources of Caffeine in Diets of US Children and Adults: Trends by Beverage Type and Purchase Location. Nutrients. 2016; 8(3):154. https://doi.org/10.3390/nu8030154
Chicago/Turabian StyleDrewnowski, Adam, and Colin D. Rehm. 2016. "Sources of Caffeine in Diets of US Children and Adults: Trends by Beverage Type and Purchase Location" Nutrients 8, no. 3: 154. https://doi.org/10.3390/nu8030154
APA StyleDrewnowski, A., & Rehm, C. D. (2016). Sources of Caffeine in Diets of US Children and Adults: Trends by Beverage Type and Purchase Location. Nutrients, 8(3), 154. https://doi.org/10.3390/nu8030154