Metformin Treatment and Homocysteine: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Study Selection
2.2. Data Extraction and Quality Assessment
2.3. Statistical Methods
3. Results
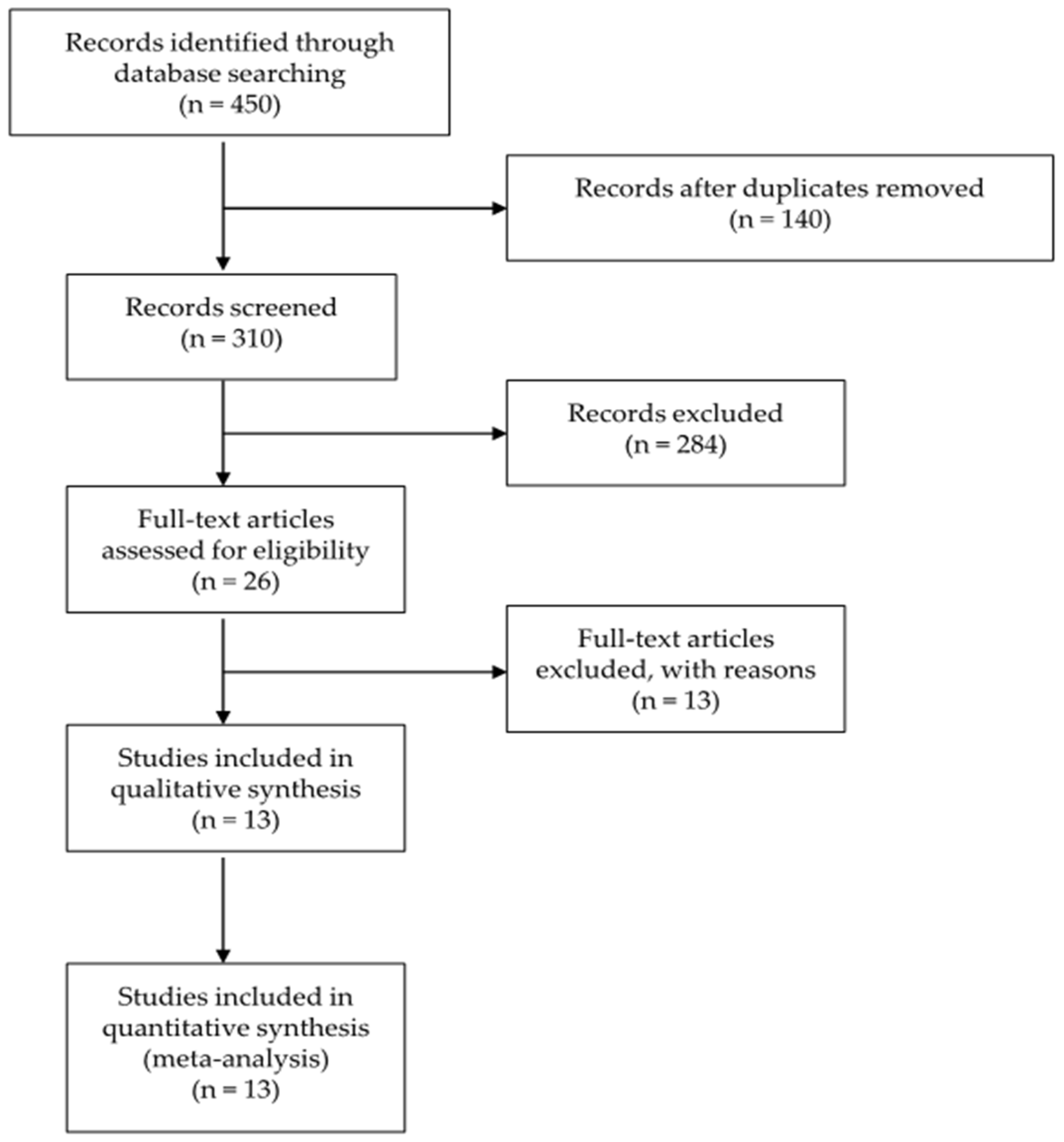
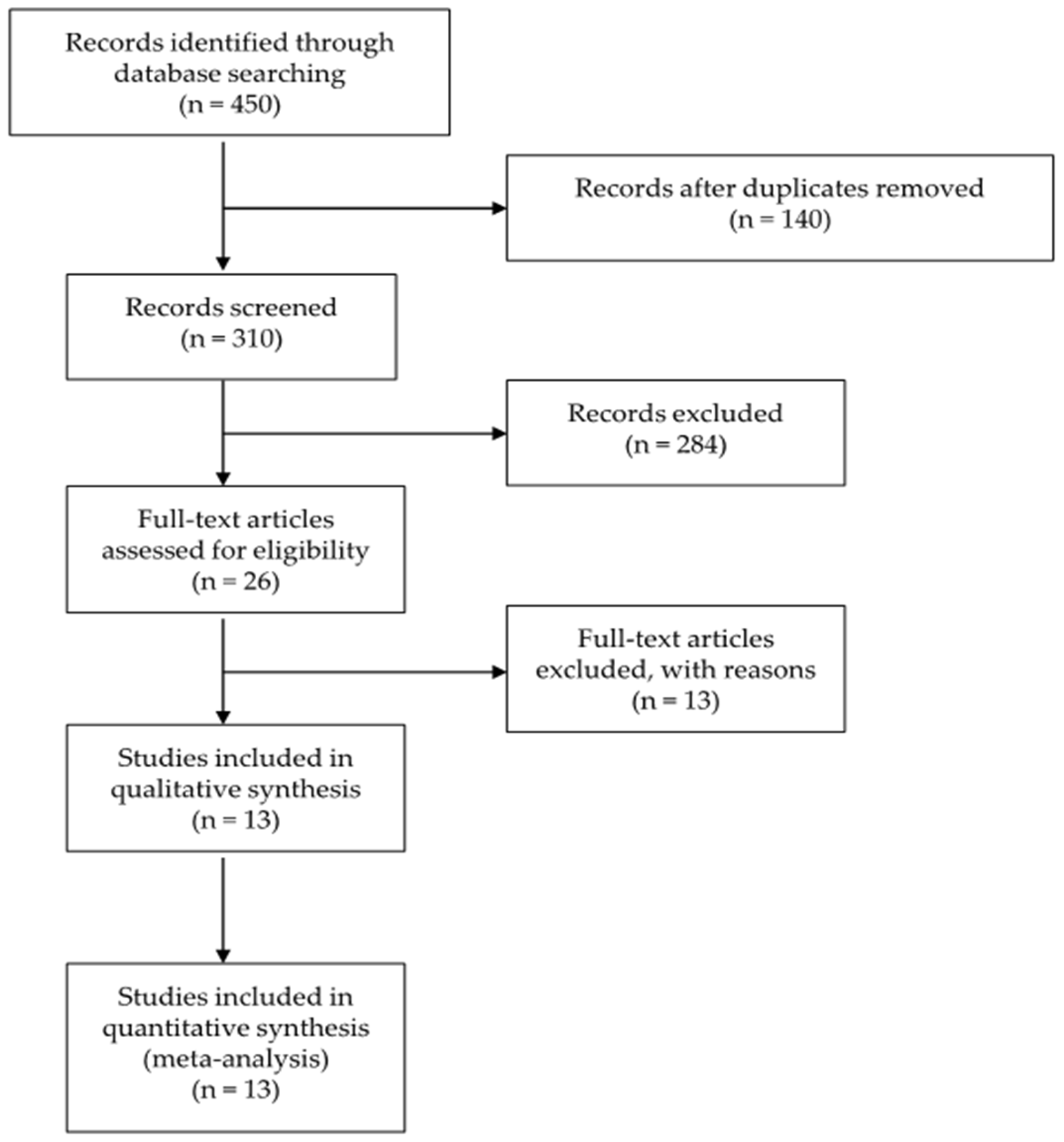
3.1. Search Results
3.2. Quality Assessment
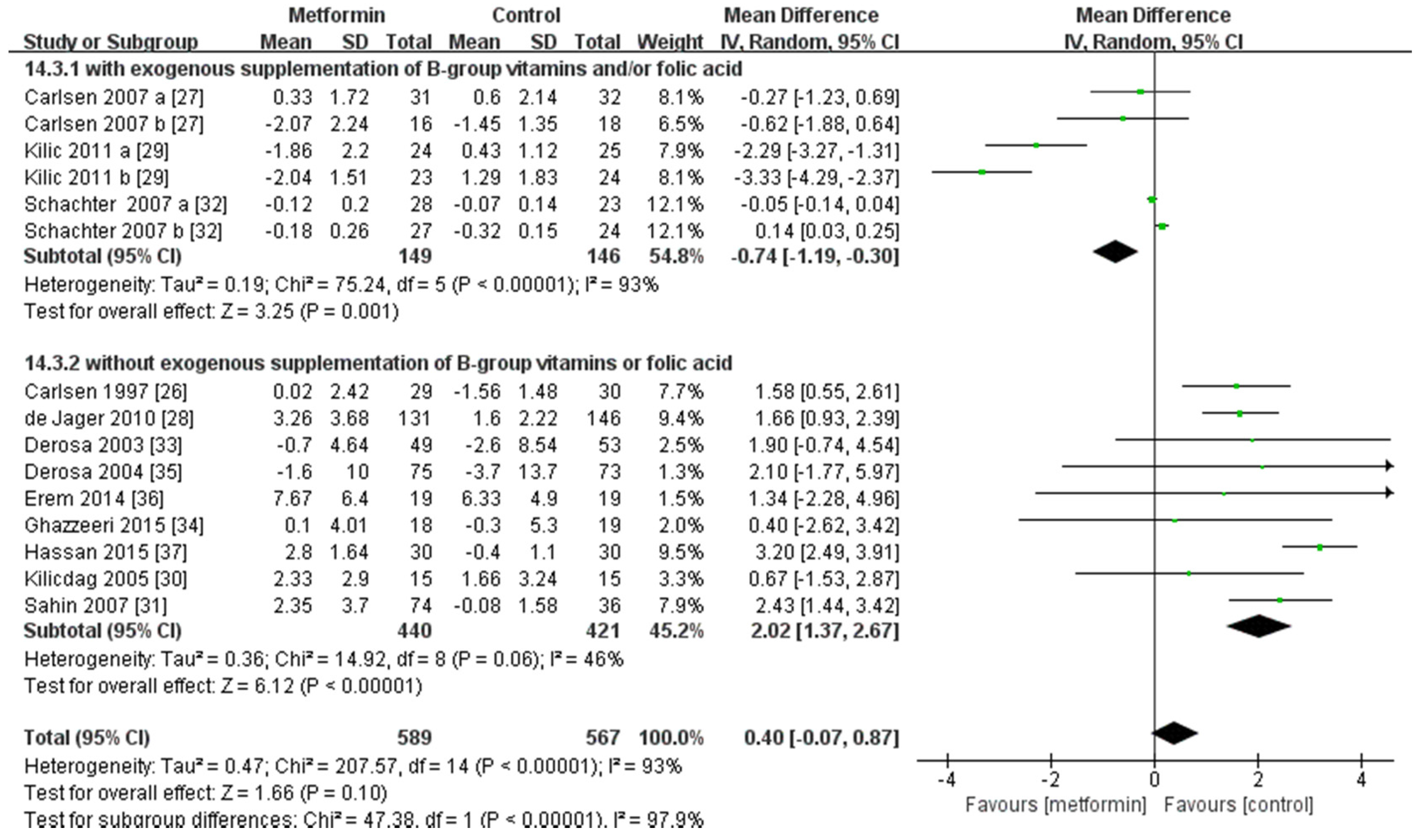
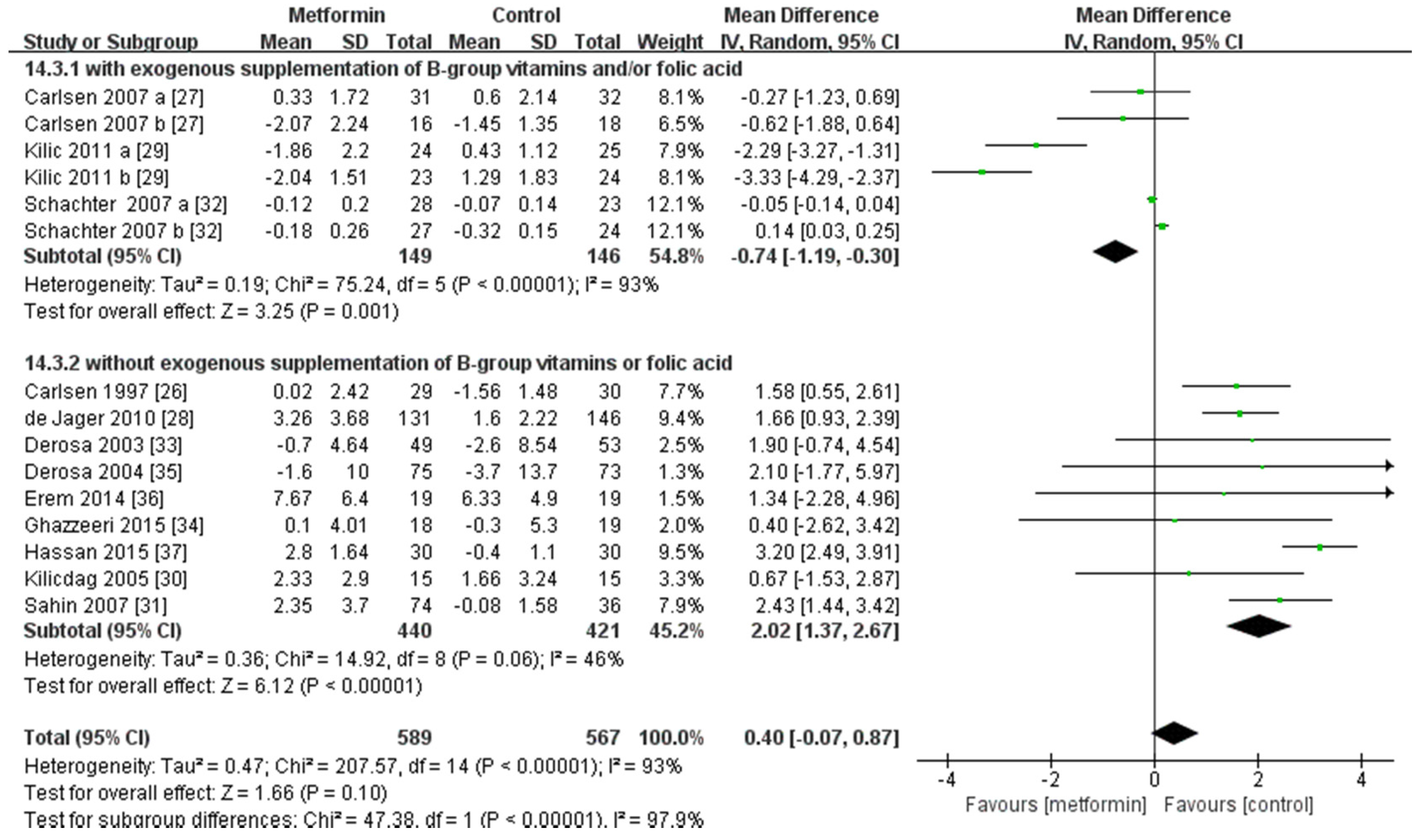
3.3. Metformin and Homocysteine
3.4. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of hyperglycemia in type 2 diabetes, 2015: A patient-centered approach: Update to a position statement of the american diabetes association and the european association for the study of diabetes. Diabetes Care 2015, 38, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Global Guideline for Type 2 Diabetes—2012. Available online: http://www.idf.org/new-global-guideline-type-2-diabetes-out-now-0 (accessed on 2 January 2016).
- Liu, Q.; Li, S.; Quan, H.; Li, J. Vitamin B12 status in metformin treated patients: Systematic review. PLoS ONE 2014, 9, e100379. [Google Scholar] [CrossRef] [PubMed]
- Solomon, L.R. Disorders of cobalamin (vitamin B12) metabolism: Emerging concepts in pathophysiology, diagnosis and treatment. Blood Rev. 2007, 21, 113–130. [Google Scholar] [CrossRef] [PubMed]
- Selhub, J. 5-homocysteine metabolism. Annu. Rev. Nutr. 1999, 19, 217–246. [Google Scholar] [CrossRef] [PubMed]
- Mandaviya, P.R.; Stolk, L.; Heil, S.G. Homocysteine and DNA methylation: A review of animal and human literature. Mol. Genet. Metab. 2014, 113, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Strain, J.J.; Dowey, L.; Ward, M.; Pentieva, K.; McNulty, H. B-vitamins, homocysteine metabolism and CVD. Proc. Nutr. Soc. 2007, 63, 597–603. [Google Scholar] [CrossRef]
- Miller, J.W. Homocysteine. In Encyclopedia of Human Nutrition, 3rd ed.; Elsevier: Amsterdam, The Netherlands, 2013; pp. 424–430. [Google Scholar]
- Durand, P.P.M.; Loreau, N.; Lussier-Cacan, S.; Blache, D. Impaired homocysteine metabolism and atherothrombotic disease. Lab. Investig. 2011, 81, 645–672. [Google Scholar] [CrossRef]
- Debreceni, B.; Debreceni, L. The role of homocysteine-lowering B-vitamins in the primary prevention of cardiovascular disease. Cardiovasc. Ther. 2014, 32, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Fan, S.; Zhi, X.; Wang, Y.; Wang, Y.; Zheng, Q.; Sun, G. Prevalence of hyperhomocysteinemia in China: A systematic review and meta-analysis. Nutrients 2015, 7, 74–90. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Handbook for Systematic Reviews of Interventions. Available online: http://handbook.cochrane.org/ (accessed on 25 December 2015).
- Gatford, K.L.; Houda, C.M.; Lu, Z.X.; Coat, S.; Baghurst, P.A.; Owens, J.A.; Sikaris, K.; Rowan, J.A.; Hague, W.M. Vitamin B12 and homocysteine status during pregnancy in the metformin in gestational diabetes trial: Responses to maternal metformin compared with insulin treatment. Diabetes Obes. Metab. 2013, 15, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.; Forder, P.; Simes, J.; Whiting, M.; Kritharides, L.; Merrifield, A.; Donoghoe, M.; Colman, P.G.; Graham, N.; Haapamaki, H.; et al. Associations between the use of metformin, sulphonylureas, or diet alone and cardiovascular outcomes in 6005 people with type 2 diabetes in the field study. Diabetes Res. Clin. Pract. 2011, 94, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Wulffele, M.G.; Kooy, A.; Lehert, P.; Bets, D.; Ogterop, J.C.; Borger van der Burg, B.; Donker, A.J.; Stehouwer, C.D. Effects of short-term treatment with metformin on serum concentrations of homocysteine, folate and vitamin B12 in type 2 diabetes mellitus: A randomized, placebo-controlled trial. J. Intern. Med. 2003, 254, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Ham, A.C.; Enneman, A.W.; van Dijk, S.C.; Oliai Araghi, S.; Swart, K.M.; Sohl, E.; van Wijngaarden, J.P.; van der Zwaluw, N.L.; Brouwer-Brolsma, E.M.; Dhonukshe-Rutten, R.A.; et al. Associations between medication use and homocysteine levels in an older population, and potential mediation by vitamin B12 and folate: Data from the B-PROOF study. Drugs Aging 2014, 31, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Sahin, Y.; Unluhizarci, K.; Yilmazsoy, A.; Yikilmaz, A.; Aygen, E.; Kelestimur, F. The effects of metformin on metabolic and cardiovascular risk factors in nonobese women with polycystic ovary syndrome. Clin. Endocrinol. 2007, 67, 904–908. [Google Scholar] [CrossRef] [PubMed]
- Rajagopal, G.; Reddy, A.P.; Venkata Harinarayan, C.; Suresh, V.; Bitla, A.; Rao, S.P.V.L.N.; Sachan, A. Effect of lifestyle modification and metformin therapy on emerging cardiovascular risk factors in overweight indian women with polycystic ovary syndrome. Metab. Syndr. Relat. Disord. 2012, 10, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Russo, G.T.; Giandalia, A.; Romeo, E.L.; Marotta, M.; Alibrandi, A.; de Francesco, C.; Horvath, K.V.; Asztalos, B.; Cucinotta, D. Lipid and non-lipid cardiovascular risk factors in postmenopausal type 2 diabetic women with and without coronary heart disease. J. Endocrinol. Investig. 2014, 37, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, M.; Bukan, N.; Ayvaz, G.; Karakoc, A.; Toruner, F.; Cakir, N.; Arslan, M. The effects of rosiglitazone and metformin on oxidative stress and homocysteine levels in lean patients with polycystic ovary syndrome. Hum. Reprod. 2005, 20, 3333–3340. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.; Pena, A.S.; Sullivan, T.; Gent, R.; D’Arcy, B.; Olds, T.; Coppin, B.; Couper, J. Does metformin improve vascular health in children with type 1 diabetes? Protocol for a one year, double blind, randomised, placebo controlled trial. BMC Pediatr. 2013, 13, 108. [Google Scholar] [CrossRef] [PubMed]
- Wulffele, M.G.; Kooy, A.; Lehert, P.; Bets, D.; Donker, A.J.; Stehouwer, C.D. Does metformin decrease blood pressure in patients with type 2 diabetes intensively treated with insulin? Diabet. Med. 2005, 22, 907–913. [Google Scholar] [CrossRef] [PubMed]
- Luque-Ramirez, M.; Mendieta-Azcona, C.; del Rey Sanchez, J.M.; Maties, M.; Escobar-Morreale, H.F. Effects of an antiandrogenic oral contraceptive pill compared with metformin on blood coagulation tests and endothelial function in women with the polycystic ovary syndrome: Influence of obesity and smoking. Eur. J. Endocrinol. 2009, 160, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Luque-Ramirez, M.; Alvarez-Blasco, F.; Uriol Rivera, M.G.; Escobar-Morreale, H.F. Serum uric acid concentration as non-classic cardiovascular risk factor in women with polycystic ovary syndrome: Effect of treatment with ethinyl-estradiol plus cyproterone acetate versus metformin. Hum. Reprod. 2008, 23, 1594–1601. [Google Scholar] [CrossRef] [PubMed]
- Gharakhani, M.; Neghab, N.; Farimani, M. Is reducing ovarian volume in polycystic ovarian syndrome patients after administration of metformin associated with improving cardiovascular risk factors? Int. J. Fertil. Steril. 2011, 5, 90–95. [Google Scholar] [PubMed]
- Carlsen, S.M.; Folling, I.; Grill, V.; Bjerve, K.S.; Schneede, J.; Refsum, H. Metformin increases total serum homocysteine levels in non-diabetic male patients with coronary heart disease. Scand. J. Clin. Lab. Investig. 1997, 57, 521–527. [Google Scholar] [CrossRef]
- Carlsen, S.M.; Kjotrod, S.; Vanky, E.; Romundstad, P. Homocysteine levels are unaffected by metformin treatment in both nonpregnant and pregnant women with polycystic ovary syndrome. Acta Obstet. Gynecol. Scand. 2007, 86, 145–150. [Google Scholar] [CrossRef] [PubMed]
- De Jager, J.; Kooy, A.; Lehert, P.; Wulffele, M.G.; van der Kolk, J.; Bets, D.; Verburg, J.; Donker, A.J.; Stehouwer, C.D. Long term treatment with metformin in patients with type 2 diabetes and risk of vitamin B-12 deficiency: Randomised placebo controlled trial. BMJ 2010, 340, c2181. [Google Scholar] [CrossRef] [PubMed]
- Kilic, S.; Yilmaz, N.; Zulfikaroglu, E.; Erdogan, G.; Aydin, M.; Batioglu, S. Inflammatory-metabolic parameters in obese and nonobese normoandrogenemic polycystic ovary syndrome during metformin and oral contraceptive treatment. Gynecol. Endocrinol. 2011, 27, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Kilicdag, E.B.; Bagis, T.; Zeyneloglu, H.B.; Tarim, E.; Aslan, E.; Haydardedeoglu, B.; Erkanli, S. Homocysteine levels in women with polycystic ovary syndrome treated with metformin versus rosiglitazone: A randomized study. Hum. Reprod. 2005, 20, 894–899. [Google Scholar] [CrossRef] [PubMed]
- Sahin, M.; Tutuncu, N.B.; Ertugrul, D.; Tanaci, N.; Guvener, N.D. Effects of metformin or rosiglitazone on serum concentrations of homocysteine, folate, and vitamin B12 in patients with type 2 diabetes mellitus. J. Diabetes Complicat. 2007, 21, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Schachter, M.; Raziel, A.; Strassburger, D.; Rotem, C.; Ron-El, R.; Friedler, S. Prospective, randomized trial of metformin and vitamins for the reduction of plasma homocysteine in insulin-resistant polycystic ovary syndrome. Fertil. Steril. 2007, 88, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Derosa, G.; Mugellini, A.; Ciccarelli, L.; Crescenzi, G.; Fogari, R. Comparison of glycaemic control and cardiovascular risk profile in patients with type 2 diabetes during treatment with either repaglinide or metformin. Diabetes Res. Clin. Pract. 2003, 60, 161–169. [Google Scholar] [CrossRef]
- Ghazeeri, G.; Abbas, H.A.; Skaff, B.; Harajly, S.; Awwad, J. Inadequacy of initiating rosuvastatin then metformin on biochemical profile of polycystic ovarian syndrome patients. J. Endocrinol. Investig. 2015, 38, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Derosa, G.; Franzetti, I.; Gadaleta, G.; Ciccarelli, L.; Fogari, R. Metabolic variations with oral antidiabetic drugs in patients with type 2 diabetes: Comparison between glimepiride and metformin. Diabetes Nutr. Metab. 2004, 17, 143–150. [Google Scholar] [PubMed]
- Erem, C.; Ozbas, H.M.; Nuhoglu, I.; Deger, O.; Civan, N.; Ersoz, H.O. Comparison of effects of gliclazide, metformin and pioglitazone monotherapies on glycemic control and cardiovascular risk factors in patients with newly diagnosed uncontrolled type 2 diabetes mellitus. Exp. Clin. Endocrinol. Diabetes 2014, 122, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.H.; Abd-Allah, G.M. Effects of metformin plus gliclazide versus metformin plus glimepiride on cardiovascular risk factors in patients with type 2 diabetes mellitus. Pak. J. Pharm. Sci. 2015, 28, 1723–1730. [Google Scholar] [PubMed]
- Anderson, J.L.; Muhlestein, J.B.; Horne, B.D.; Carlquist, J.F.; Bair, T.L.; Madsen, T.E.; Pearson, R.R. Plasma homocysteine predicts mortality independently of traditional risk factors and C-reactive protein in patients with angiographically defined coronary artery disease. Circulation 2000, 102, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Bates, C.J.; Mansoor, M.A.; Pentieva, K.D.; Hamer, M.; Mishra, G.D. Biochemical risk indices, including plasma homocysteine, that prospectively predict mortality in older British people: The national diet and nutrition survey of people aged 65 years and over. Br. J. Nutr. 2010, 104, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Niafar, M.; Hai, F.; Porhomayon, J.; Nader, N.D. The role of metformin on vitamin B12 deficiency: A meta-analysis review. Intern. Emerg. Med. 2015, 10, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Caspary, W.F.; Creutzfeldt, W. Analysis of the inhibitory effect of biguanides on glucose absorption: Inhibition of active sugar transport. Diabetologia 1971, 7, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Caspary, W.F.; Zavada, I.; Reimold, W.; Deuticke, U.; Emrich, D.; Willms, B. Alteration of bile acid metabolism and vitamin-B12-absorption in diabetics on biguanides. Diabetologia 1977, 13, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Scarpello, J.H.; Greaves, M.; Sladen, G.E. Small intestinal transit in diabetics. Br. Med. J. 1976, 2, 1225–1226. [Google Scholar] [CrossRef] [PubMed]
- Schafer, G. Some new aspects on the interaction of hypoglycemia-producing biguanides with biological membranes. Biochem. Pharmacol. 1976, 25, 2015–2024. [Google Scholar] [CrossRef]
- Carmel, R.; Rosenberg, A.H.; Lau, K.S.; Streiff, R.R.; Herbert, V. Vitamin B12 uptake by human small bowel homogenate and its enhancement by intrinsic factor. Gastroenterology 1969, 56, 548–555. [Google Scholar] [PubMed]
- Mashavi, M.; Hanah, R.; Boaz, M.; Gavish, D.; Matas, Z.; Fux, A.; Shargorodsky, M. Effect of homocysteine-lowering therapy on arterial elasticity and metabolic parameters in metformin-treated diabetic patients. Atherosclerosis 2008, 199, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Mazokopakis, E.E.; Starakis, I.K. Recommendations for diagnosis and management of metformin-induced vitamin B12 (Cbl) deficiency. Diabetes Res. Clin. Pract. 2012, 97, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Filioussi, K.; Bonovas, S.; Katsaros, T. Should we screen diabetic patients using biguanides for megaloblastic anaemia? Aust. Fam. Phys. 2003, 32, 383–384. [Google Scholar]
- Moore, E.M.; Mander, A.G.; Ames, D.; Kotowicz, M.A.; Carne, R.P.; Brodaty, H.; Woodward, M.; Boundy, K.; Ellis, K.A.; Bush, A.I.; et al. Increased risk of cognitive impairment in patients with diabetes is associated with metformin. Diabetes Care 2013, 36, 2981–2987. [Google Scholar] [CrossRef] [PubMed]
- Obeid, R.; Jung, J.; Falk, J.; Herrmann, W.; Geisel, J.; Friesenhahn-Ochs, B.; Lammert, F.; Fassbender, K.; Kostopoulos, P. Serum vitamin B12 not reflecting vitamin B12 status in patients with type 2 diabetes. Biochimie 2013, 95, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Garber, A.J.; Abrahamson, M.J.; Barzilay, J.I.; Blonde, L.; Bloomgarden, Z.T.; Bush, M.A.; Dagogo-Jack, S.; Davidson, M.B.; Einhorn, D.; Garvey, W.T.; et al. American association of clinical endocrinologists’ comprehensive diabetes management algorithm 2013 consensus statement. Endocr. Pract. 2013, 19, 536–557. [Google Scholar] [CrossRef] [PubMed]
- Yegnanarayan, R.; Suryavanshi, M.; Singh, M.; Desai, S. A comparative study of the glycemic control of various antidiabetic agents and the role of homocysteine in the therapy of type 2 diabetes mellitus. J. Diabetes Complicat. 2008, 22, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Hoogeveen, E.K.; Kostense, P.J.; Jakobs, C.; Bouter, L.M.; Heine, R.J.; Stehouwer, C.D. Does metformin increase the serum total homocysteine level in non-insulin-dependent diabetes mellitus? J. Intern. Med. 1997, 242, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Krysiak, R.; Gilowski, W.; Okopien, B. The effect of testosterone on cardiovascular risk factors in men with type 2 diabetes and late-onset hypogonadism treated with metformin or glimepiride. Pharmacol. Rep. 2016, 68, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Ouchi, K.; Funase, Y.; Yamauchi, K.; Aizawa, T. Relationship between metformin use, vitamin B12 deficiency, hyperhomocysteinemia and vascular complications in patients with type 2 diabetes. Endocr. J. 2013, 60, 1275–1280. [Google Scholar] [CrossRef] [PubMed]
- Wile, D.J.; Toth, C. Association of metformin, elevated homocysteine, and methylmalonic acid levels and clinically worsened diabetic peripheral neuropathy. Diabetes Care 2010, 33, 156–161. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Study | Country | Patients, N (I/C) | BMI, (kg/m2) | Age (Years) | Participants | Women (%) |
|---|---|---|---|---|---|---|
| Carlsen 1997 [26] | Norway | 29/30 | NA | 53 | CHD without diabetes | All men |
| Carlsen 2007a [27] | Norway and Turkey | 31/32 | NA | NA | PCOS, infertile | All women |
| Carlsen 2007b [27] | Norway and Turkey | 16/18 | NA | NA | PCOS, pregnant | All women |
| de Jager 2010 * [28] Wulffele 2003 * [15] | The Netherlands | 131/146 | 30 | 61.4 | Insulin-treated T2DM | 75.5 |
| Kilic 2011a [29] | Turkey | 24/25 | 29.6 | 28.9 | PCOS with IGT, BMI > 25 kg/m2 | All women |
| Kilic 2011b [29] | Turkey | 23/24 | 22.4 | 26.5 | PCOS with IGT, BMI < 25 kg/m2 | All women |
| Kilicdag 2005 [30] | Turkey | 15/15 | 27.7 | 24.8 | PCOS | All women |
| Sahin 2007 [31] | Turkey | 74/36 | 28.9 | 58.6 | Newly diagnosed T2DM | 58.2 |
| Schachter 2007a [32] | Israel | 28/23 | NA | NA | PCOS with IR | All women |
| Schachter 2007b [32] | Israel | 27/24 | NA | NA | PCOS with IR | All women |
| Derosa 2003 [33] | Italy | 49/53 | 25.0 | 53.6 | Drug naïve T2DM | 50.0 |
| Ghazeeri 2015 [34] | Lebanon | 18/19 | NA | 25.8 | PCOS | All women |
| Derosa 2004 [35] | Italy | 75/73 | 27.9 | NA | Newly diagnosed T2DM | 51.2 |
| Erem 2014 [36] | Turkey | 19/19 | 32.4 | 52.4 | Newly diagnosed T2DM | 71.1 |
| Hassan 2015 [37] | Egypt | 30/30 | 27.3 | NA | Newly diagnosed T2DM | All men |
| Study ID | Intervention | Control | Primary Treatment | Washout Period | Background Treatment | Follow-up | Assay Method of Hcy | B12 Supplement | Folic Acid Supplement |
|---|---|---|---|---|---|---|---|---|---|
| Carlsen 1997 [26] | Metformin (2000 mg/day) 1 | Blank | Coronary artery bypass surgery or angioplasty | Lifestyle intervention and lovastatin, 40 mg daily | Lovastatin, 40 mg daily | 40 weeks | HPLC | No | No |
| Carlsen 2007a 2 [27] | Metformin (2000 mg/day) | Placebo | NS | No | Lifestyle intervention, folic acid 0.4 mg/day and a daily multivitamin tablet | 16 weeks | HPLC | 1 μg/day | 0.4 mg/day |
| Carlsen 2007b 2 [27] | Metformin (1700 mg/day) | Placebo | NS | No | Lifestyle intervention, folate 1 mg/day and a daily multi-vitamin tablet | 16 weeks | HPLC | 1 μg/day | 1 mg/day |
| de Jager 2010 [28]/ Wulffele 2003 3 [15] | Metformin (2550 mg/day) 4 | Placebo | Insulin | Insulin (12 weeks) | Insulin | 224 weeks | Chromsystems kit | No | No |
| Kilic 2011a 5 [29] | Metformin (1700 mg/day) | Oral contraceptive | NS | No | B-group vitamins | 24 weeks | CLI | 2000 mg/day | No |
| Kilic 2011b 5 [29] | Metformin (1700 mg/day) | Oral contraceptive | NS | No | B-group vitamins | 24 weeks | CLI | 2000 mg/day | No |
| Kilicdag 2005 [30] | Metformin (1700 mg/day) | Rosiglitazone (4 mg/day) | NS | No | No | 12 weeks | FPI | No | No |
| Sahin 2007 [31] | Metformin (1700 mg/day) | Blank | Lifestyle intervention | Lifestyle intervention (4 weeks) | Lifestyle intervention | 6 weeks | CLI | No | No |
| Schachter 2007a 6 [32] | Metformin (1700 mg/day) | Blank | NS | No | Infertility treatment and folic acid 0.4 mg daily | Three cycles of treatment 7 | FPI | No | 0.4 mg/day |
| Schachter 2007b 6 [32] | Metformin (1700 mg/day) | Blank | NS | No | Infertility treatment and B-group vitamins | Three cycles of treatment 7 | FPI | 0.5 mg/day | 0.4 mg/day |
| Derosa 2003 [33] | Metformin (1500–2500 mg/day) 8 | Repaglinide (2–4 mg/day) 8 | NS | Placebo | Lifestyle intervention | 60 weeks | HPLC | No | No |
| Ghazeeri 2015 [34] | Metformin (1700 mg/day) | placebo | NS | 3 months of rosuvastatin (10 mg/day) | Rosuvastatin (10 mg/day) | 24 weeks | NA | No | No |
| Derosa 2004 [35] | Metformin (1000–3000 mg/day) 9 | Glimepiride (1–4 mg/day) 9 | NS | No | Lifestyle intervention | 56 weeks | HPLC and fluorescence detection | No | No |
| Erem 2014 [36] | Metformin (2000 mg/day) | Pioglitazone (15–45 mg/day) 10 | No | No | Lifestyle intervention | 12 months | ELISA | No | No |
| Hassan 2015 [37] | Metformin (1000 mg/day) | moderately calorie-restricted diet and an active lifestyle | No | No | No | 3 months | enzyme-linked immunoassay and an automated fluorescence polarization analyzer | No | No |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Q.; Li, S.; Li, L.; Li, Q.; Ren, K.; Sun, X.; Li, J. Metformin Treatment and Homocysteine: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2016, 8, 798. https://doi.org/10.3390/nu8120798
Zhang Q, Li S, Li L, Li Q, Ren K, Sun X, Li J. Metformin Treatment and Homocysteine: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2016; 8(12):798. https://doi.org/10.3390/nu8120798
Chicago/Turabian StyleZhang, Qianying, Sheyu Li, Ling Li, Qianrui Li, Kaiyun Ren, Xin Sun, and Jianwei Li. 2016. "Metformin Treatment and Homocysteine: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Nutrients 8, no. 12: 798. https://doi.org/10.3390/nu8120798
APA StyleZhang, Q., Li, S., Li, L., Li, Q., Ren, K., Sun, X., & Li, J. (2016). Metformin Treatment and Homocysteine: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients, 8(12), 798. https://doi.org/10.3390/nu8120798