High Prevalence of Hyperhomocysteinemia and Its Association with Target Organ Damage in Chinese Patients with Chronic Kidney Disease

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Baseline Data Collection
2.3. Assessment of Target Organs
2.3.1. Renal Assessment
2.3.2. Transthoracic Echocardiography Evaluation
2.3.3. Carotid Ultrasonography
2.4. Definitions
2.5. Statistical Analyses
3. Results
3.1. Demographic and Clinical Characteristics of the Study Population
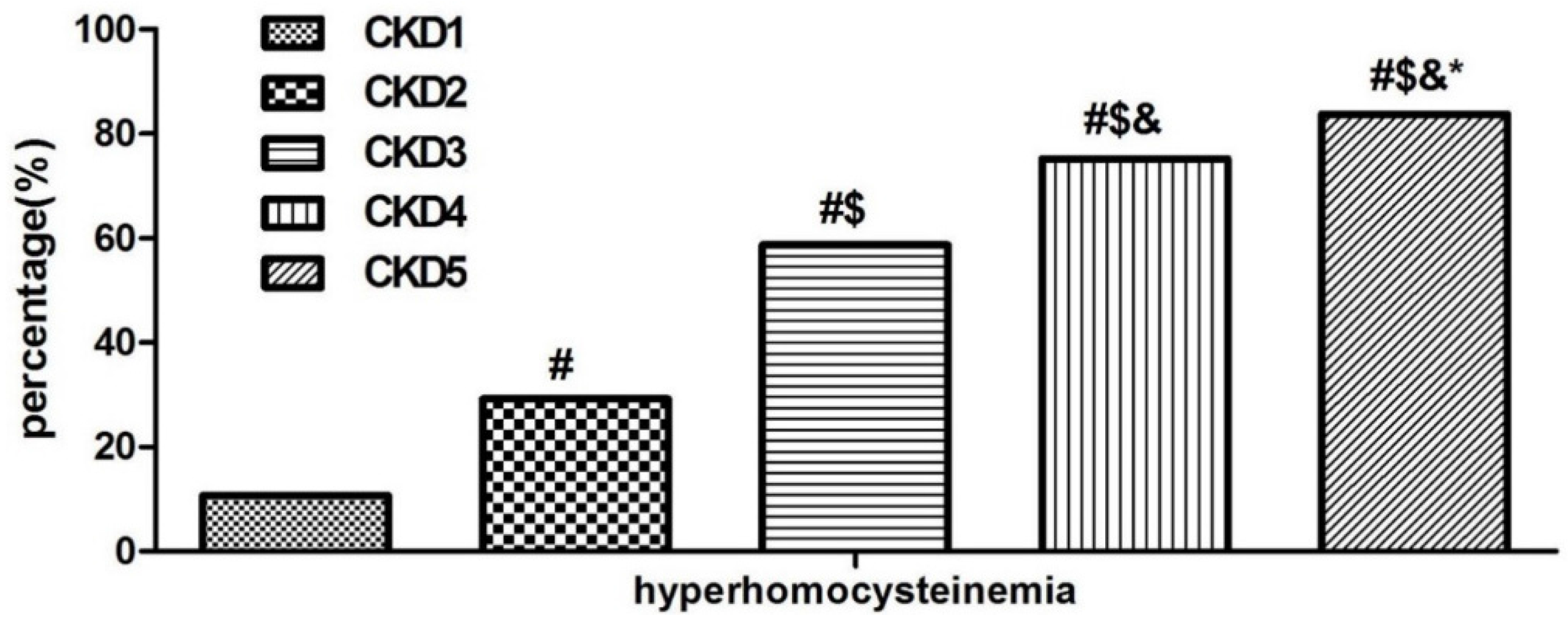
3.2. Prevalence of Hyperhomocysteinemia in Different CKD Stages
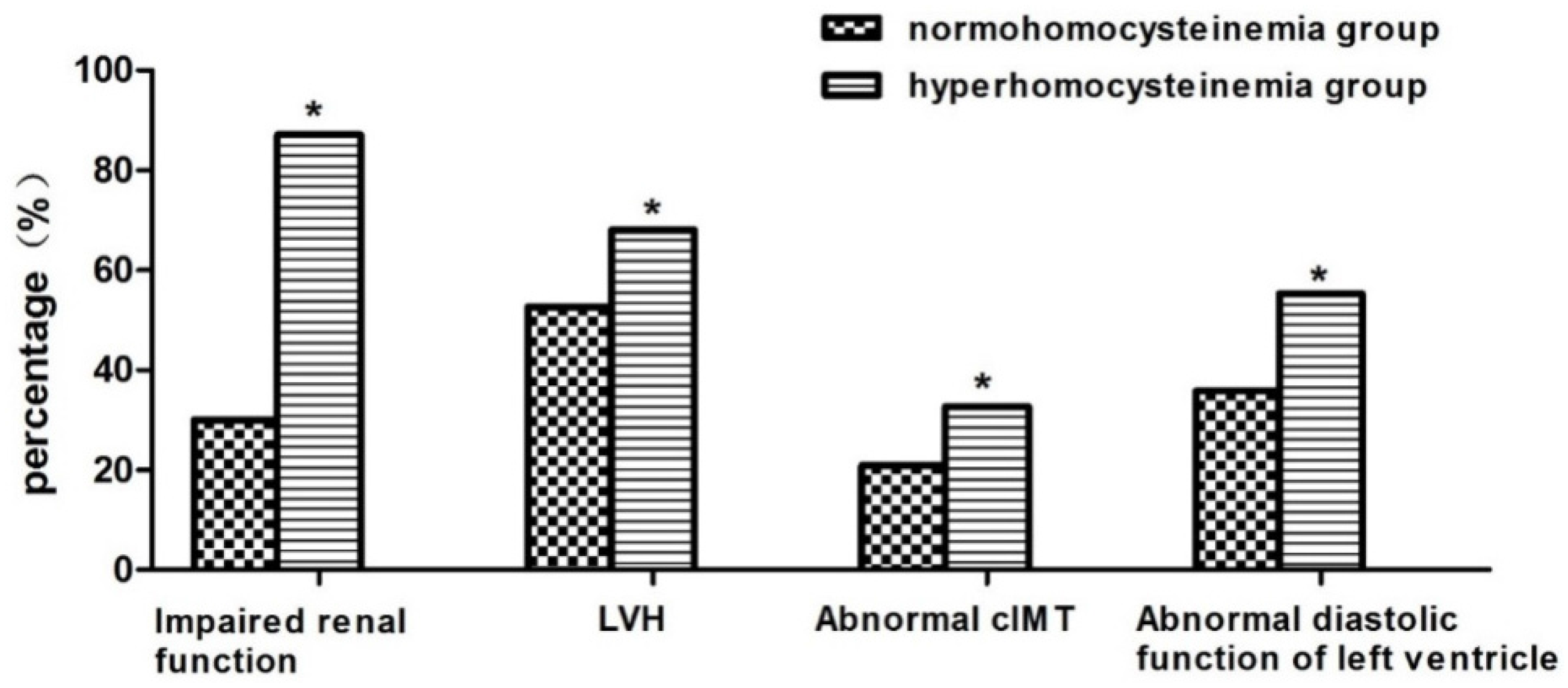
3.3. Comparison of Target Organ Damage in Patients with or without Hyperhomocysteinemia
3.4. Factors Associated with Target Organ Damage in CKD Patients
3.5. Factors Associated with Hyperhomocysteinemia and Proteinuria in CKD Patients
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Zhang, L.; Wang, F.; Wang, L.; Wang, W.; Liu, B.; Liu, J.; Chen, M.; He, Q.; Liao, Y.; Yu, X.; et al. Prevalence of chronic kidney disease in China: A cross-sectional survey. Lancet 2012, 379, 815–822. [Google Scholar] [CrossRef]
- Afsar, B.; Turkmen, K.; Covic, A.; Kanbay, M. An update on coronary artery disease and chronic kidney disease. Int. J. Nephrol. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, K.; Coresh, J.; Sang, Y.; Chalmers, J.; Fox, C.; Guallar, E.; Jafar, T.; Jassal, S.K.; Landman, G.W.; Muntner, P.; et al. Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: A collaborative meta-analysis of individual participant data. Lancet Diabetes Endocrinol. 2015, 3, 514–525. [Google Scholar] [CrossRef]
- Cai, Q.; Mukku, V.K.; Ahmad, M. Coronary artery disease in patients with chronic kidney disease: A clinical update. Curr. Cardiol. Rev. 2013, 9, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Leoncini, G.; Viazzi, F.; Parodi, D.; Ratto, E.; Vettoretti, S.; Vaccaro, V.; Ravera, M.; Deferrari, G.; Pontremoli, R. Mild renal dysfunction and cardiovascular risk in hypertensive patients. J. Am. Soc. Nephrol. JASN 2004, 15 (Suppl. 1), S88–S90. [Google Scholar] [CrossRef] [PubMed]
- Catena, C.; Cavarape, A.; Dotto, L.; Colussi, G.; Novehllo, M.; De Marchi, S.; Sechi, L.A. The emerging risk factors for cardiovascular disease: A review of the epidemiologic evidence for lipoprotein(a), homocysteine, and fibrinogen. Adv. Clin. Pathol. 2003, 7, 3–11. [Google Scholar]
- Kong, X.; Ma, X.; Cui, M.; Xu, D. Association of clustering of major cardiovascular risk factors with chronic kidney disease in the adult population. Clin. Nephrol. 2014, 82, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.S.; Wong, P.W.; Malinow, M.R. Hyperhomocyst(e)inemia as a risk factor for occlusive vascular disease. Annu. Rev. Nutr. 1992, 12, 279–298. [Google Scholar] [CrossRef] [PubMed]
- Ganguly, P.; Alam, S.F. Role of homocysteine in the development of cardiovascular disease. Nutr. J. 2015, 14. [Google Scholar] [CrossRef] [PubMed]
- McCully, K.S. Homocysteine and vascular disease. Nat. Med. 1996, 2, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Ueland, P.M.; Refsum, H. Plasma homocysteine, a risk factor for vascular disease: Plasma levels in health, disease, and drug therapy. J. Lab. Clin. Med. 1989, 114, 473–501. [Google Scholar] [PubMed]
- Wierzbicki, A.S. Homocysteine and cardiovascular disease: A review of the evidence. Diabetes Vasc. Dis. Res. 2007, 4, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Wald, D.S.; Law, M.; Morris, J.K. Homocysteine and cardiovascular disease: Evidence on causality from a meta-analysis. BMJ 2002, 325, 1202. [Google Scholar] [CrossRef] [PubMed]
- Jardine, M.J.; Kang, A.; Zoungas, S.; Navaneethan, S.D.; Ninomiya, T.; Nigwekar, S.U.; Gallagher, M.P.; Cass, A.; Strippoli, G.; Perkovic, V. The effect of folic acid based homocysteine lowering on cardiovascular events in people with kidney disease: Systematic review and meta-analysis. BMJ 2012, 344, e3533. [Google Scholar] [CrossRef] [PubMed]
- Suliman, M.E.; Lindholm, B.; Barany, P.; Qureshi, A.R.; Stenvinkel, P. Homocysteine-lowering is not a primary target for cardiovascular disease prevention in chronic kidney disease patients. Semin. Dial. 2007, 20, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Jamison, R.L.; Hartigan, P.; Kaufman, J.S.; Goldfarb, D.S.; Warren, S.R.; Guarino, P.D.; Gaziano, J.M.; Veterans Affairs Site Investigators. Effect of homocysteine lowering on mortality and vascular disease in advanced chronic kidney disease and end-stage renal disease: A randomized controlled trial. JAMA 2007, 298, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Huo, Y.; Li, J.; Qin, X.; Huang, Y.; Wang, X.; Gottesman, R.F.; Tang, G.; Wang, B.; Chen, D.; He, M.; et al. Efficacy of folic acid therapy in primary prevention of stroke among adults with hypertension in China: The CSPPT randomized clinical trial. JAMA 2015, 313, 1325–1335. [Google Scholar] [CrossRef] [PubMed]
- Chao, M.C.; Hu, S.L.; Hsu, H.S.; Davidson, L.E.; Lin, C.H.; Li, C.I.; Liu, C.S.; Li, T.C.; Lin, C.C.; Lin, W.Y. Serum homocysteine level is positively associated with chronic kidney disease in a Taiwan Chinese population. J. Nephrol. 2014, 27, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Chico, A.; Perez, A.; Cordoba, A.; Arcelus, R.; Carreras, G.; de Leiva, A.; Gonzalez-Sastre, F.; Blanco-Vaca, F. Plasma homocysteine is related to albumin excretion rate in patients with diabetes mellitus: A new link between diabetic nephropathy and cardiovascular disease? Diabetologia 1998, 41, 684–693. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.; Yuan, Y.; Guo, J.; Yang, S.; Xu, X.; Wang, Q.; Li, Y.; Qin, X.; Tang, G.; Huo, Y.; et al. Hyperhomocysteinemia predicts renal function decline: A prospective study in hypertensive adults. Sci. Rep. 2015, 5, 16268. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.C.; Zuo, L.; Chen, J.H.; Luo, Q.; Yu, X.Q.; Li, Y.; Xu, J.S.; Huang, S.M.; Wang, L.N.; Huang, W.; et al. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J. Am. Soc. Nephrol. JASN 2006, 17, 2937–2944. [Google Scholar] [CrossRef] [PubMed]
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- Devereux, R.B.; Alonso, D.R.; Lutas, E.M.; Gottlieb, G.J.; Campo, E.; Sachs, I.; Reichek, N. Echocardiographic assessment of left ventricular hypertrophy: Comparison to necropsy findings. Am. J. Cardiol. 1986, 57, 450–458. [Google Scholar] [CrossRef]
- Kjeldsen, S.E. 2003 European society of hypertension-European society of cardiology guidelines for the management of arterial hypertension. J. Hypertens. 2003, 21, 1011–1053. [Google Scholar] [CrossRef]
- Wang, C.; Deng, W.J.; Gong, W.Y.; Zhang, J.; Tang, H.; Peng, H.; Zhang, Q.Z.; Ye, Z.C.; Lou, T. High prevalence of isolated nocturnal hypertension in Chinese patients with chronic kidney disease. J. Am. Heart Assoc. 2015, 4, e002025. [Google Scholar] [CrossRef] [PubMed]
- The Department of Disease Control; Ministry of Health of the People’s Republic of China; The Chinese Diabetes Society. The Chinese guideline of diabetes prevention and treatment. Chin. J. Prev. Contr. Chron. Non-Commun. Dis. 2004, 12, 283–285. [Google Scholar]
- Yang, B.; Fan, S.; Zhi, X.; Wang, Y.; Wang, Y.; Zheng, Q.; Sun, G. Prevalence of hyperhomocysteinemia in China: A systematic review and meta-analysis. Nutrients 2015, 7, 74–90. [Google Scholar] [CrossRef] [PubMed]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Bohm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: The task force for the management of arterial hypertension of the European society of hypertension (ESH) and of the european society of cardiology (ESC). J. Hypertens. 2013, 31, 1281–1357. [Google Scholar] [CrossRef] [PubMed]
- Simon, A.; Megnien, J.L.; Chironi, G. The value of carotid intima-media thickness for predicting cardiovascular risk. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 182–185. [Google Scholar] [CrossRef] [PubMed]
- Petersen, J.F.; Larsen, B.S.; Sabbah, M.; Nielsen, O.W.; Kumarathurai, P.; Sajadieh, A. Long-term prognostic significance of homocysteine in middle-aged and elderly. Biomarkers 2016, 21, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Homocysteine Studies Collaboration. Homocysteine and risk of ischemic heart disease and stroke: A meta-analysis. JAMA 2002, 288, 2015–2022. [Google Scholar]
- Wang, C.Y.; Chen, Z.W.; Zhang, T.; Liu, J.; Chen, S.H.; Liu, S.Y.; Han, L.Y.; Hui, Z.H.; Chen, Y.M. Elevated plasma homocysteine level is associated with ischemic stroke in Chinese hypertensive patients. Eur. J. Intern. Med. 2014, 25, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Li, X.; Qin, X.; Cai, Y.; He, M.; Sun, L.; Li, J.; Zhang, Y.; Tang, G.; Wang, B.; et al. Prevalence of hyperhomocysteinaemia and its major determinants in rural Chinese hypertensive patients aged 45–75 years. Br. J. Nutr. 2013, 109, 1284–1293. [Google Scholar] [CrossRef] [PubMed]
- Guttormsen, A.B.; Ueland, P.M.; Svarstad, E.; Refsum, H. Kinetic basis of hyperhomocysteinemia in patients with chronic renal failure. Kidney Int. 1997, 52, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Van Guldener, C.; Kulik, W.; Berger, R.; Dijkstra, D.A.; Jakobs, C.; Reijngoud, D.J.; Donker, A.J.; Stehouwer, C.D.; de Meer, K. Homocysteine and methionine metabolism in ESRD: A stable isotope study. Kidney Int. 1999, 56, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Liew, S.C.; Gupta, E.D. Methylenetetrahydrofolate reductase (MTHFR) c677t polymorphism: Epidemiology, metabolism and the associated diseases. Eur. J. Med. Genet. 2015, 58, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Levi, A.; Cohen, E.; Levi, M.; Goldberg, E.; Garty, M.; Krause, I. Elevated serum homocysteine is a predictor of accelerated decline in renal function and chronic kidney disease: A historical prospective study. Eur. J. Intern. Med. 2014, 25, 951–955. [Google Scholar] [CrossRef] [PubMed]
- Spence, J.D.; Urquhart, B.L.; Bang, H. Effect of renal impairment on atherosclerosis: Only partially mediated by homocysteine. Nephrol. Dial. Transplant. 2016, 31, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Perna, A.F.; Ingrosso, D. Atherosclerosis determinants in renal disease: How much is homocysteine involved? Nephrol. Dial. Transplant. 2016, 31, 860–863. [Google Scholar] [CrossRef] [PubMed]
- Ostrakhovitch, E.A.; Tabibzadeh, S. Homocysteine in chronic kidney disease. Adv. Clin. Chem. 2015, 72, 77–106. [Google Scholar] [PubMed]
- Cao, L.; Lou, X.; Zou, Z.; Mou, N.; Wu, W.; Huang, X.; Tan, H. Folic acid attenuates hyperhomocysteinemia-induced glomerular damage in rats. Microvasc. Res. 2013, 89, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Yi, F.; dos Santos, E.A.; Xia, M.; Chen, Q.Z.; Li, P.L.; Li, N. Podocyte injury and glomerulosclerosis in hyperhomocysteinemic rats. Am. J. Nephrol. 2007, 27, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Hu, J.J.; Xia, M.; Boini, K.M.; Brimson, C.; Li, P.L. Redox signaling via lipid raft clustering in homocysteine-induced injury of podocytes. Biochim. Biophys. Acta 2010, 1803, 482–491. [Google Scholar] [CrossRef] [PubMed]
- Xia, M.; Conley, S.M.; Li, G.; Li, P.L.; Boini, K.M. Inhibition of hyperhomocysteinemia-induced inflammasome activation and glomerular sclerosis by NLRP3 gene deletion. Cell. Physiol. Biochem. 2014, 34, 829–841. [Google Scholar] [PubMed]
- Abais, J.M.; Xia, M.; Li, G.; Gehr, T.W.; Boini, K.M.; Li, P.L. Contribution of endogenously produced reactive oxygen species to the activation of podocyteNLRP3 inflammasomes in hyperhomocysteinemia. Free Radic. Biol. Med. 2014, 67, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Qin, X.; Li, Y.; Sun, D.; Wang, J.; Liang, M.; Wang, B.; Huo, Y.; Hou, F.F.; Investigators of the Renal Substudy of the China Stroke Primary Prevention Trial (CSPPT). Efficacy of folic acid therapy on the progression of chronic kidney disease: The renal substudy of the china stroke primary prevention trial. JAMA Intern. Med. 2016, 176, 1443–1450. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Total | Normohomocysteinemia | Hyperhomocysteinemia | p Value | |
|---|---|---|---|---|
| (N = 1042) | (N = 492) | (N = 550) | ||
| Age (years) | 44.34 ± 16.53 | 39.94 ± 16.40 | 48.27 ± 15.65 | <0.001 |
| Male: Female ratio | 641:401 | 266:226 | 375:175 | <0.001 |
| Course (months) | 6 (1–24) | 4 (1–24) | 12 (1–36) | <0.001 |
| Diabetes mellitus (N/%) | 192 (18.43%) | 69 (14.02%) | 123 (22.36%) | <0.001 |
| Current smoker (N/%) | 218 (20.92%) | 87 (17.68%) | 131 (23.82%) | <0.05 |
| Alcohol intake (N/%) | 104 (9.98%) | 43 (8.74%) | 61 (11.09%) | 0.216 |
| BMI (kg/m2) | 23.24 ± 4.02 | 23.22 ± 4.14 | 23.27 ± 3.92 | 0.845 |
| Clinic-SBP (mmHg) | 145.38 ± 24.67 | 138.51 ± 22.67 | 151.52 ± 24.79 | <0.001 |
| Clinic-DBP (mmHg) | 86.95 ± 14.46 | 84.88 ± 13.19 | 88.81 ± 15.29 | <0.001 |
| Hemoglobin (g/L) | 112.77 ± 29.70 | 123.32 ± 27.02 | 103.33 ± 28.81 | <0.001 |
| Albumin (g/L) | 33.93 ± 8.26 | 31.31 ± 9.23 | 36.27 ± 6.45 | <0.001 |
| Calcium×Phosphate (mg2/dL2) | 38.54 ± 11.61 | 34.34 ± 8.98 | 42.26 ± 12.38 | <0.001 |
| iPTH (pg/mL) | 72.05 (37.70–230.09) | 42.44 (27.35–73.50) | 139.56 (58.44–330.48) | <0.001 |
| Serum fasting glucose (mmol/L) | 5.24 ± 1.93 | 5.15 ± 1.71 | 5.32 ± 2.11 | 0.179 |
| Cholesterol (mmol/L) | 5.75 ± 2.79 | 6.65 ± 3.28 | 4.94 ± 1.95 | <0.001 |
| Triglyceride (mmol/L) | 2.00 ± 1.68 | 2.10 ± 1.89 | 1.91 ± 1.46 | 0.066 |
| HDL-C (mmol/L) | 1.19 ± 0.44 | 1.30 ± 0.47 | 1.09 ± 0.39 | <0.001 |
| LDL-C (mmol/L) | 3.70 ± 2.13 | 4.41 ± 2.51 | 3.07 ± 1.45 | <0.001 |
| Homocysteine (μmol/L) | 18.14 ± 10.44 | 10.57 ± 2.88 | 24.93 ± 10.08 | <0.001 |
| Uric acid (mmol/L) | 477.96 ± 152.54 | 419.05 ± 124.80 | 530.31 ± 155.92 | <0.001 |
| Proteinuria (g/24 h) | 1.58 (0.52–4.03) | 2.03 (0.46–5.23) | 1.36 (0.55–2.90) | <0.001 |
| Urinary sodium excretion (mmol/24 h) | 123.83 ± 78.29 | 132.24 ± 87.15 | 115.31 ± 67.24 | <0.05 |
| Serum Cystatin C (mg/L) | 2.69 ± 2.03 | 1.57 ± 1.39 | 3.66 ± 1.99 | <0.001 |
| Blood urea nitrogen (mmol/L) | 9.87 (5.57–20.38) | 5.83 (4.33–8.98) | 17.20 (9.86–26.37) | <0.001 |
| Serum creatinine (μmol/L) | 158.70 (84.70–538.00) | 86.00 (66.57–133.07) | 428.00 (167.30–789.50) | <0.001 |
| Total | Normohomocysteinemia | Hyperhomocysteinemia | p Value | |
|---|---|---|---|---|
| (N = 1042) | (N = 492) | (N = 550) | ||
| eGFR-MDRD (mL/min/1.73 m2) | 38.12 (8.52–90.08) | 87.68 (49.22–119.84) | 11.63 (5.52–35.56) | <0.001 |
| LVMI (g/m2) | 124.68 ± 37.35 | 116.19 ± 39.92 | 128.99 ± 35.26 | <0.001 |
| E/A | 1.11 ± 0.45 | 1.20 ± 0.43 | 1.02 ± 0.45 | <0.001 |
| cIMT (mm) | 0.75 ± 0.34 | 0.71 ± 0.31 | 0.78 ± 0.35 | <0.05 |
| Variables | Unstandardized Coefficients B (95% Confidence Interval) | Standardized Coefficients Beta | p Value |
|---|---|---|---|
| Dependent variable: Lg (eGFR by MDRD formula) (Adjusted R2 = 0.806) | |||
| iPTH (per 1 pg/mL) | −0.001 (−0.001–0.001) | −0.297 | <0.001 |
| Hemoglobin (per 1 g/L) | 0.005 (0.004–0.006) | 0.285 | <0.001 |
| Homocysteine (per 1 μmol/L) | −0.01 (−0.012–0.007) | −0.204 | <0.001 |
| Age (per 1 year) | −0.011 (−0.014–0.008) | −0.217 | <0.001 |
| Calcium×Phosphate (mg2/dL2) | −0.004 (−0.006–0.002) | −0.116 | <0.001 |
| Uric acid (per 1 mmol/L) | 0.000 (−0.001–0.000) | −0.111 | <0.001 |
| Clinic-SBP (per 1 mmHg) | −0.002 (−0.003–0.001) | −0.090 | <0.001 |
| Urinary sodium excretion (per 1 mmol/24 h) | 0.000 (0.000–0.001) | 0.048 | 0.038 |
| Dependent variable: LVMI (kg/m2) (Adjusted R2 = 0.266) | |||
| iPTH (per 1 pg/mL) | 0.032 (0.022–0.042) | 0.291 | <0.001 |
| Hemoglobin (per 1 g/L) | −0.291 (−0.414–0.167) | −0.227 | <0.001 |
| Clinic-SBP (per 1 mmHg) | 0.283 (0.152–0.415) | 0.188 | <0.001 |
| Gender (female = 0; male = 1) | 11.872 (5.022–18.723) | 0.150 | 0.001 |
| Age (per 1 year) | 0.233 (0.015–0.450) | 0.094 | 0.036 |
| Dependent variable: cIMT (mm) (Adjusted R2 = 0.295) | |||
| Age (per 1 year) | 0.009 (0.007–0.012) | 0.390 | <0.001 |
| Clinic-SBP (per 1 mmHg) | 0.002 (0.001–0.004) | 0.152 | 0.001 |
| Current smoker (no = 0, yes = 1) | 0.125 (0.045–0.204) | 0.140 | 0.002 |
| Diabetes mellitus (no = 0, yes = 1) | 0.105 (0.021–0.189) | 0.120 | 0.015 |
| Dependent variable: E/A (Adjusted R2 = 0.295) | |||
| Age (per 1 year) | −0.016 (−0.018–0.014) | −0.580 | <0.001 |
| Clinic-SBP (per 1 mmHg) | 0.000 (0.000–0.000) | −0.078 | 0.036 |
| Current smoker (no = 0, yes = 1) | −0.002 (−0.004–0.001) | −0.160 | <0.001 |
| Diabetes mellitus (no = 0, yes = 1) | −0.005 (−0.008–0.001) | −0.114 | 0.006 |
| Variables | Unstandardized Coefficients B (95% Confidence Interval) | Standardized Coefficients Beta | p Value |
|---|---|---|---|
| Adjusted R2 = 0.397 | |||
| eGFR-MDRD (per 1 mL/min/1.73 m2) | −0.063 (−0.081–0.046) | −0.313 | <0.001 |
| Uric acid (per 1 mmol/L) | 0.011 (0.006–0.016) | 0.164 | <0.001 |
| Albumin (per 1 g/L) | 0.234 (0.155–0.313) | 0.194 | <0.001 |
| Gender (female = 0; male = 1) | 3.467 (2.078–4.857) | 0.164 | <0.001 |
| Hemoglobin (per 1 g/L) | −0.038 (−0.066–0.010) | −0.111 | 0.008 |
| Calcium×Phosphate (mg2/dL2) | 0.088 (0.017–0.159) | 0.091 | 0.015 |
| Variables | Unstandardized Coefficients B (95% Confidence Interval) | Standardized Coefficients Beta | p Value |
|---|---|---|---|
| Dependent variable: Lg(proteinuria by MDRD formula) (g/L) (Adjusted R2 = 0.454) | |||
| Age (per 1 year) | −0.007 (−0.011–0.003) | −0.165 | 0.001 |
| Diabetes mellitus (no = 0, yes = 1) | 0.181 (0.033–0.329) | 0.017 | 0.017 |
| Albumin (per 1 g/L) | −0.051 (−0.058–0.044) | −0.612 | <0.001 |
| Triglyceride (per 1 mmol/L) | 0.068 (0.030–0.106) | 0.149 | <0.001 |
| eGFR-MDRD (per 1 mL/min/1.73 m2) | −0.003 (−0.004–0.001) | −0.193 | <0.001 |
| Clinic-SBP (per 1 mmHg) | 0.003 (0.000–0.005) | 0.106 | 0.019 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ye, Z.; Zhang, Q.; Li, Y.; Wang, C.; Zhang, J.; Ma, X.; Peng, H.; Lou, T. High Prevalence of Hyperhomocysteinemia and Its Association with Target Organ Damage in Chinese Patients with Chronic Kidney Disease. Nutrients 2016, 8, 645. https://doi.org/10.3390/nu8100645
Ye Z, Zhang Q, Li Y, Wang C, Zhang J, Ma X, Peng H, Lou T. High Prevalence of Hyperhomocysteinemia and Its Association with Target Organ Damage in Chinese Patients with Chronic Kidney Disease. Nutrients. 2016; 8(10):645. https://doi.org/10.3390/nu8100645
Chicago/Turabian StyleYe, Zengchun, Qunzi Zhang, Yan Li, Cheng Wang, Jun Zhang, Xinxin Ma, Hui Peng, and Tanqi Lou. 2016. "High Prevalence of Hyperhomocysteinemia and Its Association with Target Organ Damage in Chinese Patients with Chronic Kidney Disease" Nutrients 8, no. 10: 645. https://doi.org/10.3390/nu8100645
APA StyleYe, Z., Zhang, Q., Li, Y., Wang, C., Zhang, J., Ma, X., Peng, H., & Lou, T. (2016). High Prevalence of Hyperhomocysteinemia and Its Association with Target Organ Damage in Chinese Patients with Chronic Kidney Disease. Nutrients, 8(10), 645. https://doi.org/10.3390/nu8100645