Alcohol and Difficulty Conceiving in the SUN Cohort: A Nested Case-Control Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
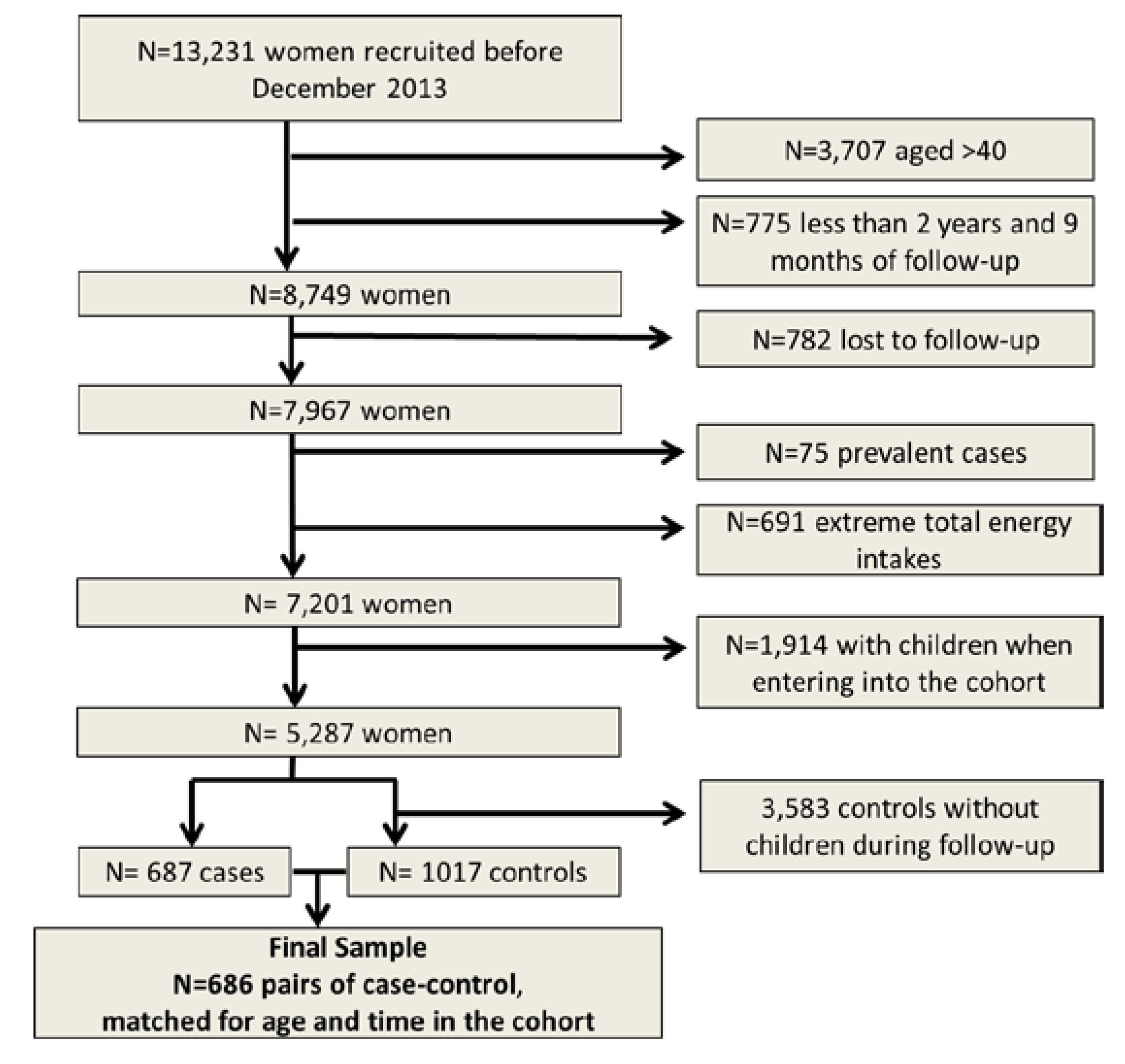
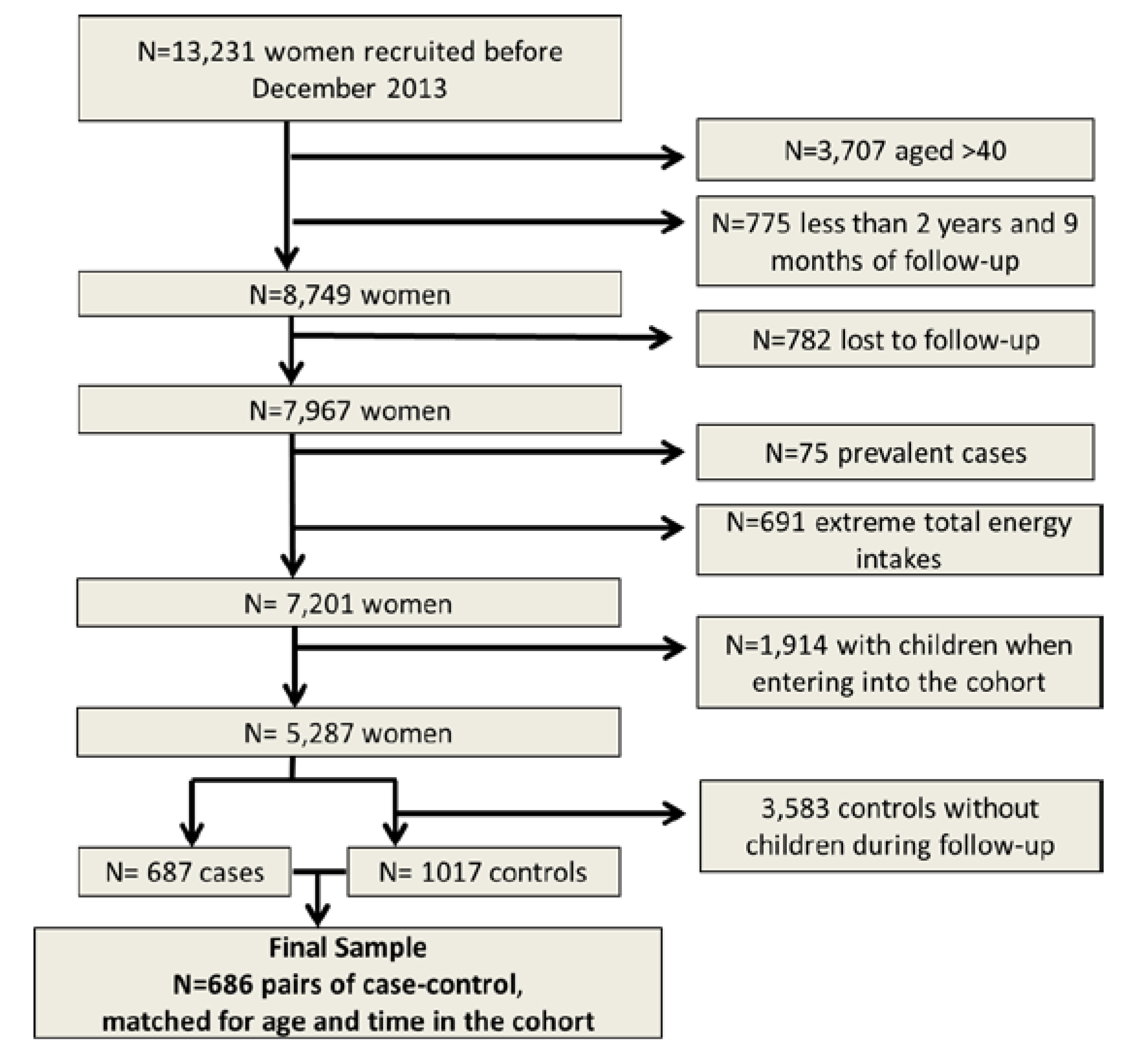
2.1. Study Population
2.2. Exposure Assessment
2.3. Covariate Assessment
2.4. Statistical Analysis
3. Results

{kind=link}
| Baseline Characteristics * | Cases (n = 686) | Matched Controls (n = 686) |
|---|---|---|
| Age, years | 29.3 (4.2) | 29.3 (4.2) |
| Body mass index, kg/m2 | 21.41 (2.70) | 21.26 (2.31) |
| Body mass index, n (%) | ||
| <18.5 | 56 (8.2) | 55 (8.1) |
| ≥18.5 to <25 | 567 (82.6) | 589 (85.8) |
| ≥25 to <30 | 50 (7.3) | 36 (5.2) |
| ≥30 | 13 (1.9) | 6 (0.9) |
| Smoking status, n (%) | ||
| Never smokers | 363 (53.9) | 356 (53.2) |
| Past smokers | 132(19.6) | 204 (30.4) |
| Current smokers | 179 (26.5) | 110 (16.4) |
| Alcohol intake, g/day | 0.35 (0.53) | 0.36 (0.60) |
| Number of alcoholic, drinks/day | ||
| Wine | 0.16 (0.39) | 0.17 (0.48) |
| Beer | 0.11 (0.21) | 0.11 (0.19) |
| Spirits | 0.07 (0.14) | 0.08 (0.15) |
| Physical activity, METs-h/week † | 18.7 (19.6) | 19.1 (21.9) |
| Adherence to Mediterranean Diet # | 3.7 (1.6) | 3.9 (1.5) |
| Use of vitamin supplements, n (%) | 134 (19.5) | 129 (18.8) |
| Total energy intake, Kcal/day | 2210.6 (571.5) | 2249.5 (546.9) |
| Consumption of Alcoholic Beverages (drinks/week) | |||||
|---|---|---|---|---|---|
| Never or seldom | ≤1/week | >1week to <5/week | ≥5/week | P for trend | |
| No. cases/controls | 152/150 | 154/147 | 284/288 | 96/101 | |
| Matched for age | 1 (ref.) | 1.04 (0.75–1.43) | 0.97 (0.74–1.29) | 0.94 (0.66–1.34) | 0.71 |
| Multivariable adjustment * | 1 (ref.) | 1.09 (0.78–1.53) | 1.02 (0.76–1.37) | 1.04 (0.72–1.51) | 0.97 |
| Consumption of wine (1 unit = 1 glass of wine = 100 mL) | |||||
| Never or seldom | ≤1/week | >1week to <5/week | ≥5/week | P for trend | |
| No. cases/controls | 312/317 | 177/164 | 156/166 | 41/39 | |
| Matched for age | 1 (ref.) | 1.10 (0.84–1.42) | 0.95 (0.72–1.25) | 1.07 (0.67–1.70) | 0.66 |
| Multivariable adjustment * | 1 (ref.) | 1.10 (0.84–1.43) | 0.97 (0.74–1.29) | 1.16 (0.72–1.88) | 0.84 |
| Consumption of beers (1 unit = 330 mL) | |||||
| Never or seldom | ≤1/week | >1/week | |||
| No. cases/controls | 326/334 | 152/140 | 208/212 | ||
| Matched for age | 1 (ref.) | 1.11 (0.84–1.45) | 1.01 (0.78–1.29) | 0.71 | |
| Multivariable adjustment * | 1 (ref.) | 1.15 (0.87–1.52) | 1.06 (0.82–1.37) | 0.98 | |
| Consumption of spirits (1 unit = 50 mL) | |||||
| Never or seldom | ≤1/week | >1/week | |||
| No. cases/controls | 377/392 | 156/154 | 153/140 | ||
| Matched for age | 1 (ref.) | 1.05 (0.81–1.36) | 1.13 (0.87–1.47) | 0.86 | |
| Multivariable adjustment* | 1 (ref.) | 1.11 (0.85–1.45) | 1.24 (0.84–1.64) | 0.78 | |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mascarenhas, M.N.; Flaxman, S.R.; Boerma, T.; Vanderpoel, S. Stevens GA National, regional, and global trends in infertility prevalence since 1990: A systematic analysis of 277 health surveys. PLoS Med. 2012, 9, e1001356. [Google Scholar] [CrossRef] [PubMed]
- Slama, R.; Hansen, O.K.H.; Ducot, B.; Bohet, A.; Sorensen, D.; Giorgis Allemand, L.; Eijkemans, M.J.C.; Rosetta, L.; Thalabard, J.C.; Keiding, N.; Bouyer, J. Estimation of the frequency of involuntary infertility on a nation-wide basis. Hum. Reprod. 2012, 27, 1489–1498. [Google Scholar] [CrossRef] [PubMed]
- Thoma, M.E.; McLain, A.C.; Louis, J.F.; King, R.B.; Trumble, A.C.; Sundaram, R.; Buck Louis, G.M. Prevalence of infertility in the United States as estimated by the current duration approach and a traditional constructed approach. Fertil. Steril. 2013, 99, 1324–1331. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Biedenharn, K.R.; Fedor, J.M.; Agarwal, A. Lifestyle factors and reproductive health: Taking control of your fertility. Reprod. Biol. Endocrin. 2013, 11, 66. [Google Scholar] [CrossRef] [PubMed]
- Eggert, J.; Theobald, H.; Engfeldt, P. Effects of alcohol consumption on female fertility during an 18-year period. Fertil. Steril. 2004, 81, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Tolstrup, J.S.; Kjaer, S.K.; Holst, C.; Sharif, H.; Munk, C.; Osler, M.; Schmidt, L.; Andersen, A.M.; Gronbaek, M. Alcohol use as predictor for infertility in a representative population of Danish women. Acta Obstet. Gynecol. Scand. 2003, 82, 744–749. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.A.; Killick, S.R. Negative lifestyle is associated with a significant reduction in fecundity. Fertil. Steril. 2004, 81, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Jensen, T.K.; Hjollund, N.H.; Henriksen, T.B.; Scheike, T.; Kolstad, H.; Giwercman, A.; Ernst, E.; Bonde, J.P.; Skakkebaek, N.E.; Olsen, J. Does moderate alcohol consumption affect fertility? Follow up study among couples planning first pregnancy. BMJ 1998, 317, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Hakim, R.B.; Gray, R.H.; Zacur, H. Alcohol and caffeine consumption and decreased fertility. Fertil. Steril. 1998, 70, 632–637. [Google Scholar] [CrossRef]
- Chavarro, J.E.; Rich-Edwards, J.W.; Rosner, B.A.; Willett, W.C. Caffeinated and alcoholic beverage intake in relation to ovulatory disorder infertility. Epidemiology 2009, 20, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Curtis, K.M.; Savitz, D.A.; Arbuckle, T.E. Effects of cigarette smoking, caffeine consumption, and alcohol intake on fecundability. Am. J. Epidemiol. 1997, 146, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Parazzini, F.; Chatenoud, L.; Di Cintio, E.; La Vecchia, C.; Benzi, G.; Fedele, L. Alcohol consumption is not related to fertility in Italian women. BMJ 1999, 318, 397. [Google Scholar] [CrossRef] [PubMed]
- Olsen, J.; Bolumar, F.; Boldsen, J.; Bisanti, L. Does moderate alcohol intake reduce fecundability? A European multicenter study on infertility and subfecundity. European Study Group on Infertility and Subfecundity. Alcohol. Clin. Exp. Res. 1997, 21, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Juhl, M.; Nyboe Andersen, A-M.; Grønbæk, M.; Olsen, J. Moderate alcohol consumption and waiting time to pregnancy. Hum. Reprod. 2001, 16, 2705–2709. [Google Scholar] [CrossRef] [PubMed]
- Juhl, M.; Olsen, J.; Nybo Andersen, A.M.; Grønbæk, M. Intake of wine, beer and spirits and waiting time to pregnancy. Hum. Reprod. 2003, 18, 1967–1971. [Google Scholar] [CrossRef] [PubMed]
- Segui-Gomez, M.; de la Fuente, C.; Vazquez, Z.; de Irala, J.; Martinez-Gonzalez, M.A. Cohort profile: The ‘Seguimiento Universidad de Navarra’ (SUN) study. Int. J. Epidemiol. 2006, 35, 1417–1422. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Stampfer, M.J. Implications of total energy intake for epidemiologic analyses. In Nutritional Epidemiology; Willett, W.C., Ed.; Oxford University Press: New York, NY, USA, 1998; pp. 273–301. [Google Scholar]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and validation of a food frequency questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Moreiras, O.; Carbajal, Á.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos. Pirámide: Madrid, Spain, 2009. [Google Scholar]
- Bes-Rastrollo, M.; Perez Valdivieso, J.R.; Sánchez-Villegas, A.; Alonso, A.; Martinez-Gonzalez, M.A. Validacion del peso e indice de masa corporal auto-declarados de los participantes de una cohorte de graduados universitarios. Rev. Esp. Obes. 2005, 3, 183–189. (In Spanish) [Google Scholar]
- Martinez-Gonzalez, M.A.; Lopez-Fontana, C.; Varo, J.J.; Sanchez-Villegas, A.; Martinez, J.A. Validation of the Spanish version of the physical activity questionnaire used in the Nurses’ Health Study and the Health Professionals’ Follow-up Study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. New Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Grodstein, F.; Goldman, M.B.; Cramer, D.W. 1994 Infertility in women and moderate alcohol use. Am. J. Public Health 1994, 84, 1429–1432. [Google Scholar] [CrossRef] [PubMed]
- Parazzini, F.; Cipriani, S.; Bravi, F.; Pelucchi, C.; Chiaffarino, F.; Ricci, E.; Viganò, P. A metaanalysis on alcohol consumption and risk of endometriosis. Am. J. Obstet. Gynecol. 2013, 209, 106.e101–106.e110. [Google Scholar] [CrossRef] [PubMed]
- Shust, G.F.; Cho, S.; Kim, M.; Madan, R.P.; Guzman, E.M.; Pollack, M.; Epstein, J.; Cohen, H.W.; Keller, M.J.; Herold, B.C. Female genital tract secretions inhibit herpes simplex virus infection: Correlation with soluble mucosal immune mediators and impact of hormonal contraception. Am. J. Reprod. Immunol. 2010, 63, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Olsen, J.; Skov, T. Design options and methodological fallacies in the studies of reproductive failures. Environ. Health Persp. 1993, 101 (Suppl. 2), 145–152. [Google Scholar] [CrossRef]
- Rinaldi, S.; Peeters, P.H.; Bezemer, I.D.; Dossus, L.; Biessy, C.; Sacerdote, C.; Berrino, F.; Panico, S.; Palli, D.; Tumino, R.; et al. Relationship of alcohol intake and sex steroid concentrations in blood in pre- and post-menopausal women: The European Prospective Investigation into Cancer and Nutrition. Cancer Causes Control 2006, 17, 1033–1043. [Google Scholar] [CrossRef] [PubMed]
- Gill, J. The effects of moderate alcohol consumption on female hormone levels and reproductive function. Alcohol. 2000, 35, 417–423. [Google Scholar] [CrossRef]
- Eagon, P.K. Alcoholic liver injury: Influence of gender and hormones. World J. Gastroenterol. 2010, 16, 1377–1384. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Camargo, C.A., Jr.; Manson, J.E.; Willett, W.C.; Rimm, E.B. Alcohol drinking patterns and risk of type 2 diabetes mellitus among younger women. Arch. Intern. Med. 2003, 163, 1329–1336. [Google Scholar] [CrossRef] [PubMed]
- Azziz, R.; Ehrmann, D.; Legro, R.S.; Whitcomb, R.W.; Hanley, R.; Fereshetian, A.G.; O’Keefe, M.; Ghazzi, M.N. Troglitazone improves ovulation and hirsutism in the polycystic ovary syndrome: A multicenter, double blind, placebo-controlled trial. J. Clin. Endocrinol. MeTable 2001, 86, 1626–1632. [Google Scholar] [CrossRef]
- Chiva-Blanch, G.; Urpi-Sarda, M.; Ros, E.; Valderas-Martinez, P.; Casas, R.; Arranz, S.; Guillén, M.; Lamuela-Raventós, R.M.; Llorach, R.; Andres-Lacueva, C.; Estruch, R. Effects of red wine polyphenols and alcohol on glucose metabolism and the lipid profile: A randomized clinical trial. Clin. Nutr. 2013, 32, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Arranz, S.; Chiva-Blanch, G.; Valderas-Martinez, P.; Medina-Remon, A.; Lamuela-Raventos, R.M.; Estruch, R. Wine, beer, alcohol and polyphenols on cardiovascular disease and cancer. Nutrients 2012, 4, 759–781. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, E.L.; Jensen, H.H.; Sanders, S.A.; Reinisch, J.M. Better psychological functioning and higher social status may largely explain the apparent health benefits of wine: A study of wine and beer drinking in young Danish adults. Arch. Intern. Med. 2001, 161, 1844–1848. [Google Scholar] [CrossRef] [PubMed]
- Alonso, A.; Beunza, J.J.; Delgado-Rodriguez, M.; Martinez-Gonzalez, M.A. Validation of self reported diagnosis of hypertension in a cohort of university graduates in Spain. BMC Public Health 2005, 5, 94. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Montero, A.; Beunza, J.J.; Bes-Rastrollo, M.; Barrio, M.T.; de la Fuente-Arrillaga, C.; Moreno-Galarraga, L.; Martinez-Gonzalez, M.A. Validity of self-reported metabolic syndrome components in a cohort study. Gac Sanit. 2011, 25, 303–307. [Google Scholar] [PubMed]
- Sanchez-Villegas, A.; Schlatter, J.; Ortuno, F.; Lahortiga, F.; Pla, J.; Benito, S.; Martinez-Gonzalez, M.A. Validity of a self-reported diagnosis of depression among participants in a cohort study using the Structured Clinical Interview for DSM-IV (SCID-I). BMC Psychiatry 2008, 8, 43. [Google Scholar] [CrossRef] [PubMed]
- Riley, E.P.; Infante, M.A.; Warren, K.R. Fetal alcohol spectrum disorders: An overview. Neuropsychol. Rev. 2011, 21, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Feldman, H.S.; Jones, K.L.; Lindsay, S.; Slymen, D.; Klonoff-Cohen, H.; Kao, K.; Rao, S.; Chambers, C. Prenatal alcohol exposure patterns and alcohol-related birth defects and growth deficiencies: A prospective study. Alcohol. Clin. Exp. Res. 2012, 36, 670–676. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burgo, C.L.-d.; Gea, A.; De Irala, J.; Martínez-González, M.A.; Chavarro, J.E.; Toledo, E. Alcohol and Difficulty Conceiving in the SUN Cohort: A Nested Case-Control Study. Nutrients 2015, 7, 6167-6178. https://doi.org/10.3390/nu7085278
Burgo CL-d, Gea A, De Irala J, Martínez-González MA, Chavarro JE, Toledo E. Alcohol and Difficulty Conceiving in the SUN Cohort: A Nested Case-Control Study. Nutrients. 2015; 7(8):6167-6178. https://doi.org/10.3390/nu7085278
Chicago/Turabian StyleBurgo, Cristina Lopez-del, Alfredo Gea, Jokin De Irala, Miguel A. Martínez-González, Jorge E. Chavarro, and Estefania Toledo. 2015. "Alcohol and Difficulty Conceiving in the SUN Cohort: A Nested Case-Control Study" Nutrients 7, no. 8: 6167-6178. https://doi.org/10.3390/nu7085278
APA StyleBurgo, C. L.-d., Gea, A., De Irala, J., Martínez-González, M. A., Chavarro, J. E., & Toledo, E. (2015). Alcohol and Difficulty Conceiving in the SUN Cohort: A Nested Case-Control Study. Nutrients, 7(8), 6167-6178. https://doi.org/10.3390/nu7085278