Development and Pilot Testing of 24-Hour Multiple-Pass Recall to Assess Dietary Intake of Toddlers of Somali- and Iraqi-Born Mothers Living in Norway


Abstract
:1. Introduction
2. Methods
2.1. Subjects and Study Design
2.2. The 24-H Recall Method
2.2.1. Picture Library for Food Identification

{kind=link}
| Food Folder | Number of Pictures |
|---|---|
| Baby cereals | 16 |
| Snacks | 33 |
| Infant formula | 16 |
| Ready-made meals | 10 |
| Bread spreads | 19 |
| Dinner | 39 |
| Yoghurt and desserts | 29 |
| Oils and butter | 13 |
| Dairy products | 13 |
| Fruits and vegetables | 50 |
| Breads | 22 |
| Pasta, rice and beans | 17 |
| Supplements | 8 |
| Milk | 38 |
| Juice and nectar | 46 |
| Soda | 4 |
| Squash, lemonade, etc. | 17 |
| Meat | 4 |
| Biscuits | 11 |
| Total | 405 |
2.2.2. Photographic Booklet and Measuring Equipment for Portion Size Estimation
2.2.3. 24-H Recall Protocol and Registration Form
2.3. Training of Field Workers
2.4. Pilot Testing of the Procedures for 24-H Recall
| Source of Information | Evaluation Topic | Question Asked |
|---|---|---|
| Observation by researchers | Time spent by the field worker | Time spent on picture library (iPad)? Time spent on photographic booklet? Time spent on measuring equipment? Other notes? |
| Use of visual tools | Which pictures were used most frequently or not at all? | |
| Standardisation of methods/field workers | Did the field workers ask the questions in the same way? Did they follow the protocol? Did they use the visual tools? | |
| Questions to respondents | Clarity of questions | Were any of the questions difficult to answer/unclear? If yes, which and why? |
| Missing pictures | Did you miss pictures of any foods/beverages? Are there some foods/beverages you give your child often, but not yesterday? Are there any other foods/beverages you know Somali/Iraqi children often eat/drink? | |
| Portion sizes | Did the portion sizes in the booklet match the portion sizes your child usually eats? Was it easier to estimate the amount the child had eaten by using the booklet, measuring equipment or by showing it on/in the plate/cup used? | |
| Questions to field workers | 24-h recall protocol | Was the protocol easy to understand? If no, why not? How did you experience the different passes during the interview? Was it easy to distinguish these from each other? |
| Picture library | How did you experience using the picture library during the interview? Was it user friendly? If no, why not? | |
| Photographic booklet | How did you experience using the photographic booklet to estimate portion sizes? Did you miss photos of any foods/beverages? | |
| Measuring equipment | How did you experience to estimate amounts using the measuring equipment? Did you miss any equipment? | |
| Registration form for 24-h recall | How did you experience using the form? Was the order of items logical to you? Was there enough space to write? If no, where did you want more space? |
| ID | Sex | Estimated Average Daily Energy Requirements (kJ/kg) | Body Weight at 12 Months (g) | Age at Time of Interview (months) | Estimated Body Weight at Time of Interview (g) a | EER at Time of Interview (kJ/day) b | EEI at Time of Interview (kJ/day) c | Percentage Differences between EER and EEI (%) d |
|---|---|---|---|---|---|---|---|---|
| 1 | F | 333 | 8440 | 14 | 8855 | 2949 | 2843 | −4 |
| 2 | M | 337 | 11,600 | 13 | 11,864 | 3998 | 3486 | −14 |
| 3 | M | 337 | 11,083 | 21 | 13,268 | 4471 | 3649 | −20 |
| 4 | F | 333 | 8719 e | 11 | 8719 | 2903 | 4415 | 41 |
| 5 | M | 337 | 8300 | 12 | 8300 | 2797 | 3102 | 10 |
| 6 | F | 333 | 10,000 | 13 | 10,246 | 3412 | 4043 | 17 |
| 7 | M | 337 | 8200 | 12 | 8200 | 2763 | 2764 | 0 |
| 8 | F | 333 | 9970 | 14 | 10,460 | 3483 | 3157 | −10 |
| 9 | M | 337 | 10,000 | 14 | 10,466 | 3527 | 2232 | −45 |
| 10 | M | 337 | 11,000 | 14 | 11,513 | 3880 | 4635 | 18 |
| 11 | M | 337 | 9890 f | 10 | 10,509 | 3542 | 3556 | 0 |
| 12 | F | 333 | 9270 | 13 | 9498 | 3163 | 4636 | 38 |
| Mean | 335 | 9706 | 13 | 10,158 | 3407 | 3543 | 18 g | |
| SD | 2 | 1146 | 3 | 1544 | 527 | 773 | 15 g |
3. Results
3.1. Subjects
3.2. Results from the Evaluation Form
3.3. Results from the 24-H Recalls
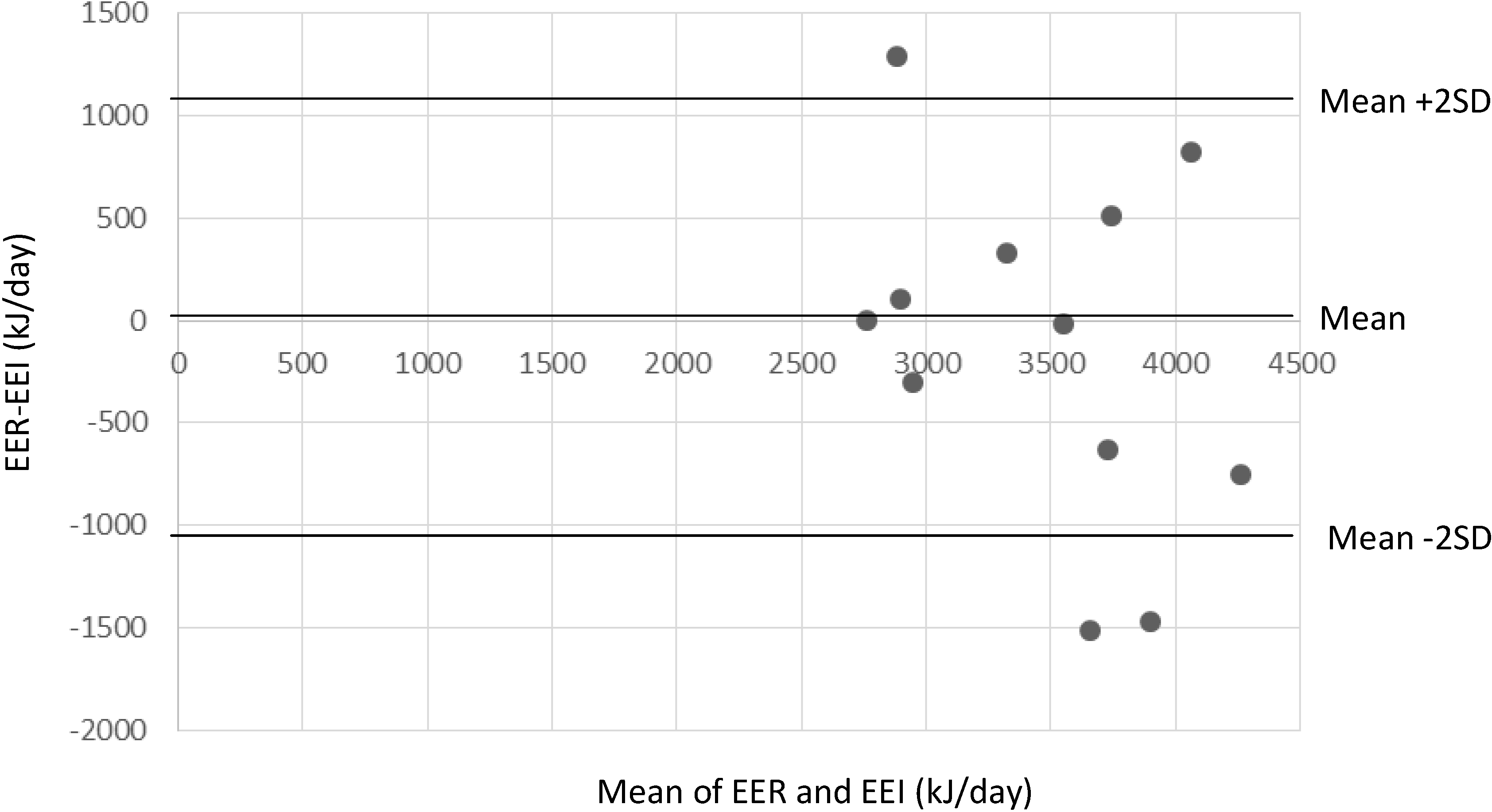
3.4. Results from Energy Intake Estimation

4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Gibson, R.S. Principles of Nutritional Assessment, 2nd ed.; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Gilbert, P.A.; Khokhar, S. Changing dietary habits of ethnic groups in Europe and implications for health. Nutr. Rev. 2008, 66, 203–215. [Google Scholar] [CrossRef]
- Holmboe-Ottesen, G.; Wandel, M. Changes in dietary habits after migration and consequences for health: A focus on South Asians in Europe. Food Nutr. Res. 2012, 56. [Google Scholar] [CrossRef]
- Landman, J.; Cruickshank, J.K. A review of ethnicity, health and nutrition-related diseases in relation to migration in the United Kingdom. Public Health Nutr. 2001, 4, 647–657. [Google Scholar]
- Kleiser, C.; Mensink, G.B.; Neuhauser, H.; Schenk, L.; Kurth, B.M. Food intake of young people with a migration background living in Germany. Public Health Nutr. 2010, 13, 324–330. [Google Scholar] [CrossRef]
- Ngo, J.; Gurinovic, M.; Frost-Anderson, L.; Serra-Majem, L. How dietary intake methodology is adapted for use in European immigrant population groups—A review. Br. J. Nutr. 2009, 101, S86–S94. [Google Scholar] [CrossRef]
- Livingstone, M.B.; Robson, P.J.; Wallace, J.M. Issues in dietary intake assessment of children and adolescents. Br. J. Nutr. 2004, 92, S213–S222. [Google Scholar] [CrossRef]
- Øverby, N.C.; Kristiansen, A.L.; Andersen, L.F. Spedkost—6 Måneder. Landsomfattende Kostholdsundersøkelse Blant 6 Måneder Gamle Barn; Helsedirektoratet, Mattilsynet and Universitetet i Oslo: Oslo, Norway, 2008. [Google Scholar]
- Øverby, N.C.; Kristiansen, A.L.; Andersen, L.F.; Lande, B. Spedkost—12 Måneder. Landsomfattende Kostholdsundersøkelse Blant 12 Måneder Gamle Barn; Helsedirektoratet, Mattilsynet and Universitetet i Oslo: Oslo, Norway, 2009. [Google Scholar]
- Kristiansen, A.L.; Andersen, L.F.; Lande, B. Småbarnskost—2 år. Landsomfattende Kostholdesundersøkelse Blant 2 år Gamle Barn; Helsedirektoratet, Mattilsynet and Universitetet i Oslo: Oslo, Norway, 2009. [Google Scholar]
- Lande, B.; Andersen, L.F.; Baerug, A.; Trygg, K.; Lund-Larsen, K.; Bjørneboe, G.-E. Development of a method for use in a national representative dietary survey among Norwegian infants and children—Spedkost/Småbarnskost. Nor. J. Epidemiol. 2000, 10, 43–50. [Google Scholar]
- Statistics Norway. Population 1 January 2012 and 2013 and Changes in 2012, by Immigration Category and Country Background. Absolute Numbers. Private communication, 2013. [Google Scholar]
- Khokhar, S.; Ashkanani, F.; Garduno-Diaz, S.D.; Husain, W. Application of ethnic food composition data for understanding the diet and nutrition of South Asians in the UK. Food Chem. 2013, 140, 436–442. [Google Scholar] [CrossRef]
- Abu-Saad, K.; Shahar, D.R.; Vardi, H.; Fraser, D. Importance of ethnic foods as predictors of and contributors to nutrient intake levels in a minority population. Eur. J. Clin. Nutr. 2010, 64, S88–S94. [Google Scholar] [CrossRef]
- Thompson, F.E.; Subar, A.F. Dietary assessment methodology. In Nutrition in the Prevention and Treatment of Disease; Coulston, A.M., Boushey, C.J., Eds.; Academic Press: San Diego, CA, USA, 2008; pp. 5–6. [Google Scholar]
- Rutishauser, I.H. Dietary intake measurements. Public Health Nutr. 2005, 8, 1100–1107. [Google Scholar] [CrossRef]
- Butte, N.F.; Lopez-Alarcon, M.G.; Garza, C. Nutrient Adequacy of Exclusive Breastfeeding for the Term Infant during the First Six Months of Life; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Nordic Council of Ministers. Nordic Nutrition Recommendations 2012 Part 1: Summary, Principles and Use; Nordic Council of Ministers: Copenhagen, Norway, 2013. [Google Scholar]
- World Health Organization. The WHO Child Growth Standards. 2013. Available online: http://www.who.int/childgrowth/standards/en/ (accessed on 1 August 2013).
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Ovaskainen, M.L.; Paturi, M.; Reinivuo, H.; Hannila, M.L.; Sinkko, H.; Lehtisalo, J.; Pynnönen-Polari, O.; Männistö, S. Accuracy in the estimation of food servings against the portions in food photographs. Eur. J. Clin. Nutr. 2008, 62, 674–681. [Google Scholar] [CrossRef]
- De Keyzer, W.; Huybrechts, I.; de Maeyer, M.; Ocké, M.; Slimani, N.; van’t Peer, P.; de Henauw, S. Food photographs in nutritional surveillance: Errors in portion size estimation using drawings of bread and photographs of margarine and beverages consumption. Br. J. Nutr. 2011, 105, 1073–1083. [Google Scholar] [CrossRef]
- Trolle, E.; Vandevijvere, S.; Ruprich, J.; Ege, M.; Dofková, M.; de Boer, E.; Ocké, M. Validation of a food quantification picture book targeting children of 0–10 years of age for pan-European and national dietary surveys. Br. J. Nutr. 2013, 110, 2298–2308. [Google Scholar] [CrossRef]
- Lillegaard, I.T.; Overby, N.C.; Andersen, L.F. Can children and adolescents use photographs of food to estimate portion sizes? Eur. J. Clin. Nutr. 2005, 59, 611–617. [Google Scholar] [CrossRef]
- Burrows, T.L.; Martin, R.J.; Collins, C.E. A systematic review of the validity of dietary assessment methods in children when compared with the method of doubly labeled water. J. Am. Diet. Assoc. 2010, 110, 1501–1510. [Google Scholar] [CrossRef]
- Garduno-Diaz, S.D.; Husain, W.; Ashkanani, F.; Kokhar, S. Meeting challenges related to the dietary assessment of ethnic minority populations. J. Hum. Nutr. Diet. 2013. [Google Scholar] [CrossRef]
- Donin, A.S.; Nightingale, C.M.; Owen, C.G.; Rudnicka, A.R.; McNamara, M.C.; Prynne, C.J.; Stephen, A.M.; Whicup, P.H. Nutritional composition of the diets of South Asian, black African-Caribbean and white European children in the United Kingdom: The Child Heart and Health Study in England (CHASE). Br. J. Nutr. 2010, 104, 276–285. [Google Scholar] [CrossRef]
- Satia-Abouta, J.; Patterson, R.E.; Neuhouser, M.L.; Elder, J. Dietary acculturation: Applications to nutrition research and dietetics. J. Am. Diet. Assoc. 2002, 102, 1105–1118. [Google Scholar]
- Biro, G.; Hulshof, K.F.; Ovesen, L.; Amorim Cruz, J.A.; EFCOSUM Group. Selection of methodology to assess food intake. Eur. J. Clin. Nutr. 2002, 56, S25–S32. [Google Scholar]
- Lazarte, C.E.; Encinas, M.E.; Alegre, C.; Granfeldt, Y. Validation of digital photographs, as a tool in 24-h recall, for the improvement of dietary assessment among rural populations in developing countries. Nutr. J. 2012, 11, 61. [Google Scholar] [CrossRef]
- Arab, L.; Estrin, D.; Kim, D.H.; Burke, J.; Goldman, J. Feasibility testing of an automated image-capture method to aid dietary recall. Eur. J. Clin. Nutr. 2011, 65, 1156–1162. [Google Scholar]
- Frobisher, C.; Maxwell, S.M. The estimation of food portion sizes: A comparison between using descriptions of portion sizes and a photographic food atlas by children and adults. J. Hum. Nutr. Diet. 2003, 16, 181–188. [Google Scholar]
- Huybregts, L.; Roberfroid, D.; Lachat, C.; van Camp, J.; Kolsteren, P. Validity of photographs for food portion estimation in a rural West African setting. Public Health Nutr. 2008, 11, 581–587. [Google Scholar]
- Klesges, R.C.; Klesges, L.M.; Brown, G.; Frank, G.C. Validation of the 24-hour dietary recall in preschool children. J. Am. Diet. Assoc. 1987, 87, 1383–1385. [Google Scholar]
- Wiskin, A.E.; Davies, J.H.; Wootton, S.A.; Beattie, R.M. Energy expenditure, nutrition and growth. Arch. Dis. Child. 2011, 96, 567–572. [Google Scholar] [CrossRef]
- Dodd, K.W.; Guenther, P.M.; Freedman, L.S.; Subar, A.F.; Kipnis, V.; Midthune, D.; Tooze, J.A.; Krebs-Smith, S.M. Statistical methods for estimating usual intake of nutrients and foods: A review of the theory. J. Am. Diet. Assoc. 2006, 106, 1640–1650. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Grewal, N.K.; Mosdøl, A.; Aunan, M.B.; Monsen, C.; Torheim, L.E. Development and Pilot Testing of 24-Hour Multiple-Pass Recall to Assess Dietary Intake of Toddlers of Somali- and Iraqi-Born Mothers Living in Norway. Nutrients 2014, 6, 2333-2347. https://doi.org/10.3390/nu6062333
Grewal NK, Mosdøl A, Aunan MB, Monsen C, Torheim LE. Development and Pilot Testing of 24-Hour Multiple-Pass Recall to Assess Dietary Intake of Toddlers of Somali- and Iraqi-Born Mothers Living in Norway. Nutrients. 2014; 6(6):2333-2347. https://doi.org/10.3390/nu6062333
Chicago/Turabian StyleGrewal, Navnit Kaur, Annhild Mosdøl, Marte Bergsund Aunan, Carina Monsen, and Liv Elin Torheim. 2014. "Development and Pilot Testing of 24-Hour Multiple-Pass Recall to Assess Dietary Intake of Toddlers of Somali- and Iraqi-Born Mothers Living in Norway" Nutrients 6, no. 6: 2333-2347. https://doi.org/10.3390/nu6062333
APA StyleGrewal, N. K., Mosdøl, A., Aunan, M. B., Monsen, C., & Torheim, L. E. (2014). Development and Pilot Testing of 24-Hour Multiple-Pass Recall to Assess Dietary Intake of Toddlers of Somali- and Iraqi-Born Mothers Living in Norway. Nutrients, 6(6), 2333-2347. https://doi.org/10.3390/nu6062333