1. Introduction
Anemia is one of the most prevalent nutritional disorders, especially among preschool-aged children in developing countries [
1]. Although anemia is broadly influenced by a variety of factors including nutrition, infectious disease, and genetics, iron deficiency is the major cause of anemia, accounting for about half of the global incidence of anemia [
2,
3,
4]. In China, it is postulated that 90% of anemia in infants and young children results from iron deficiency [
5].
Iron deficiency anemia in the first years of life has been related to many adverse consequences. In the short term, infants with iron deficiency anemia are at higher risk of cognitive, social and emotional delays [
6,
7,
8,
9,
10,
11,
12,
13,
14]. In the longer run, it can negatively affect school performance and behavior, reduce overall educational attainment, and negatively affect work outcomes into adulthood; these consequences are irreversible even if the anemia is corrected in later childhood [
15,
16,
17,
18]. Many of these consequences can be avoided, however, simply through proper dietary intake in the first years of life; studies have shown that regular iron supplementation can reduce anemia rates by as much as 50% [
19].
Despite overall improvements in child health in China in recent decades, between 1992 and 2005 there was no significant decrease in the prevalence of anemia among children under 5 years old [
20,
21,
22,
23]. Recent studies have found consistently high rates of anemia among this population, even as standards of living improved. The prevalence of anemia among infants aged 6–12 months living in rural areas was 35% in 2005, while a national survey of both urban and rural children found the average anemia prevalence of 6–12 month olds to be 28.2% [
23,
24]. Other, more geographically focused studies have found similarly high rates, ranging from 23% (in Guangxi) [
25] to 58% (in Gansu) [
26].
Although there have been a number of studies measuring the prevalence of anemia among infants and young children in China, most of these studies have been based on relatively small sample sizes [
25,
27]. Further, few studies have sought to thoroughly assess correlates and risk factors of anemia in this population [
28,
29]. The correlational studies that do exist only consider a narrow set of potential correlates. Some studies, for instance, focused only on geographical location, comparing differences in infant anemia prevalence between rural and urban China while others have only considered the bivariate associations between anemia and basic infant and household characteristics [
23,
25,
26,
27,
28,
30,
31,
32]. Examining a richer set of correlates and risk factors is essential to painting a more complete picture of the population most at risk.
One factor of particular interest in this context is feeding practices. The relationship between feeding practices and anemia is of considerable policy relevance since feeding behaviors can—in theory—be affected through policy interventions more easily than can more permanent socioeconomic characteristics such as educational attainment or household income. Despite this, however, there is only a handful of large-scale studies that consider the relationship between infant anemia and feeding practices in rural China, with inconclusive results [
26,
27,
29,
32]. Only one of these studies used multiple regression analysis to control for potential confounding factors.
The overall goal of this study is to examine the prevalence of anemia among infants in China’s poor rural areas and to identify correlates of anemia. We find 54.3% anemia prevalence among the infants in our sample, and that children weaned after 6 months have significantly lower rates of anemia relative to children who are still exclusively or predominantly breastfed after 6 months.
2. Materials and Methods
2.1. Sample Selection
In 2013, we conducted a cluster-randomized cross-sectional study of anemia prevalence among infants aged 6–11 months in 11 nationally-designated poverty counties located in southern Shaanxi province in northwestern China. In each of these 11 counties, all townships (the middle level of administration between county and village) were selected to participate in the study. We excluded the township in each county that housed the county seat. In total, the sample included 174 townships in 11 sample counties.
We randomly selected one village from each sample township to participate in the study. A list of all registered births over the past 12 months was obtained from the local family planning official in each village. All babies in the sample village in our target age range (6–11 months) were enrolled in the study. To meet the power requirements of a larger, interventional study (not reported in this paper), we required a minimum of five babies in each township. With this requirement in mind, if a village had fewer than five eligible infants, we randomly selected an additional village in the same township for inclusion in the study. All eligible infants in this second village were also enrolled in the study. Overall then, our study included 948 infants in 351 villages across 174 townships. The survey was carried out over a 20 day period in April 2013.
2.2. Data Collection
With the assistance of trained nurses from Xi’an Jiaotong Medical School, we collected hemoglobin (Hb) concentrations from all participating infants. In order to measure Hb concentrations in sample infants, a single drop of capillary blood was obtained with pressure activated safety lancets and analyzed using a HemoCue Hb 201+ system (Hemocue, Inc, Ängelholm, Sweden). The HemoCue Hb 201+ system was selected for the study because it was fast, accurate, and convenient and was suitable for use in outpatient units [
33]. The nurses also measured the length of each infant to a precision of 0.1 cm and the weight of each infant to a precision of 0.1 kg, following the procedural guidelines recommended by the World Health Organization (WHO) [
34].
Teams of trained enumerators collected socioeconomic and demographic data from all households participating in the study. During the interview, each infant’s primary caregiver was identified. The primary caregiver was identified in each sample household by asking which family member was most responsible for the infant’s care. (In over 98% of the cases, the primary caregiver was either the infant’s mother or paternal grandmother.) Enumerators administered a detailed survey on parental and household characteristics, including each infant’s gender and birth order. We also collected information on the mother’s age and level of education. Each family also reported whether they received Social Security Support (payments from China’s Minimum Living Standard Guarantee system), which we use as a household-specific indicator of poverty. China’s social security payments have been shown to be well-targeted and reliable indicators of poverty in China [
35]. Each infant’s age was obtained from his or her birth certificate.
The survey also included a detailed module on feeding practices, based on the “Indicators for assessing infant and young child feeding practices” [
36,
37] compiled by UNICEF, USAID, the World Health Organization, and others in the international community. Careful month-by-month histories of breastfeeding and formula feeding were taken from each household. Enumerators also documented the introduction of solid foods into the infant’s diet. Breastfeeding is defined to include both exclusive and predominant breastfeeding, per WHO definitions [
38].
The survey also collected infant health information from the caregiver; specifically, it asked whether the infant had had a fever or diarrhea at any time over the previous month.
2.3. Ethical Approval
This study received ethical approval from the Stanford University Institutional Review Board (IRB) (Protocol ID 25734), and from the Sichuan University Ethical Review Board (Protocol ID 2013005-01). All participating caregivers gave their oral consent for both their own and their infant’s involvement in the study. Children who were found to have severe anemia were referred to the local hospital for treatment.
2.4. Statistical Analysis
Anemia status was determined based on finger blood analysis for Hb concentrations. Since all of our sample villages were located below 1000 m, the Hb data did not require altitude adjustments. Following internationally accepted standards for our sample age group, anemia was defined as Hb < 110 g/L. We also analyzed the data by sub-category of the sample infants who were suffering from anemia. Mild anemia was defined as 100 g/L < Hb ≤ 110 g/L. Moderate anemia was defined as 70 g/L ≤ Hb < 100 g/L. Severe anemia was defined as Hb < 70 g/L [
39,
40].
Physical indicators of length and weight were compared with the 2006 WHO child growth standards [
41] to calculate length-for-age, weight-for-age, and weight-for-length Z-scores (LAZ, WAZ, WLZ). We followed internationally recognized cutoffs [
42] to consider children whose LAZ, WAZ, or WLZ fell more than two standard deviations below the international mean to be stunted, underweight, or wasted, respectively.
Low birth weight was defined to be birth weights below 2500 g.
All statistical analyses were performed using STATA 12.0 (StataCorp, College Station, TX, USA). Statistical significance of bivariate differences in Hb concentrations and anemia prevalence were assessed using ANOVA. Multiple linear regression and logistic regression models were both used in the multivariate analysis.
We considered the following variables as potential confounders in the multivariate analysis: gender, age, birth weight, birth order, whether the infant’s mother was identified as the primary caregiver, maternal educational level and age, whether the infant’s family received Social Security Support, and whether the infant had fever or diarrhea last month. We also clustered our standard errors at the village level to control for any possible intra-village correlation.
4. Discussion
This study showed that 54.3% of 6–11 month old infants in low-income areas of rural China are anemic. This is about twice as high as the 2011 average for East and Southeast Asia [
43]. Over 20% of sample infants suffered from moderate or severe anemia. These results are consistent with results of other studies of anemia among infants in poor rural China [
26,
27,
28,
31,
32]. The anemia prevalence that we identify in this study classifies anemia in our sample areas as a “severe public health problem” according to the WHO [
44]. The WHO further recommends that in communities where iron deficiency anemia prevalence exceeds 40%, all infants and toddlers should receive iron supplementation [
44]. This supplementation can take the form of traditional syrups, or home fortification powders.
While it is beyond the scope of this paper to precisely identify the exact source of the high anemia prevalence we find in this study, one possible reason may be that infants in rural China are born with suboptimal iron stores [
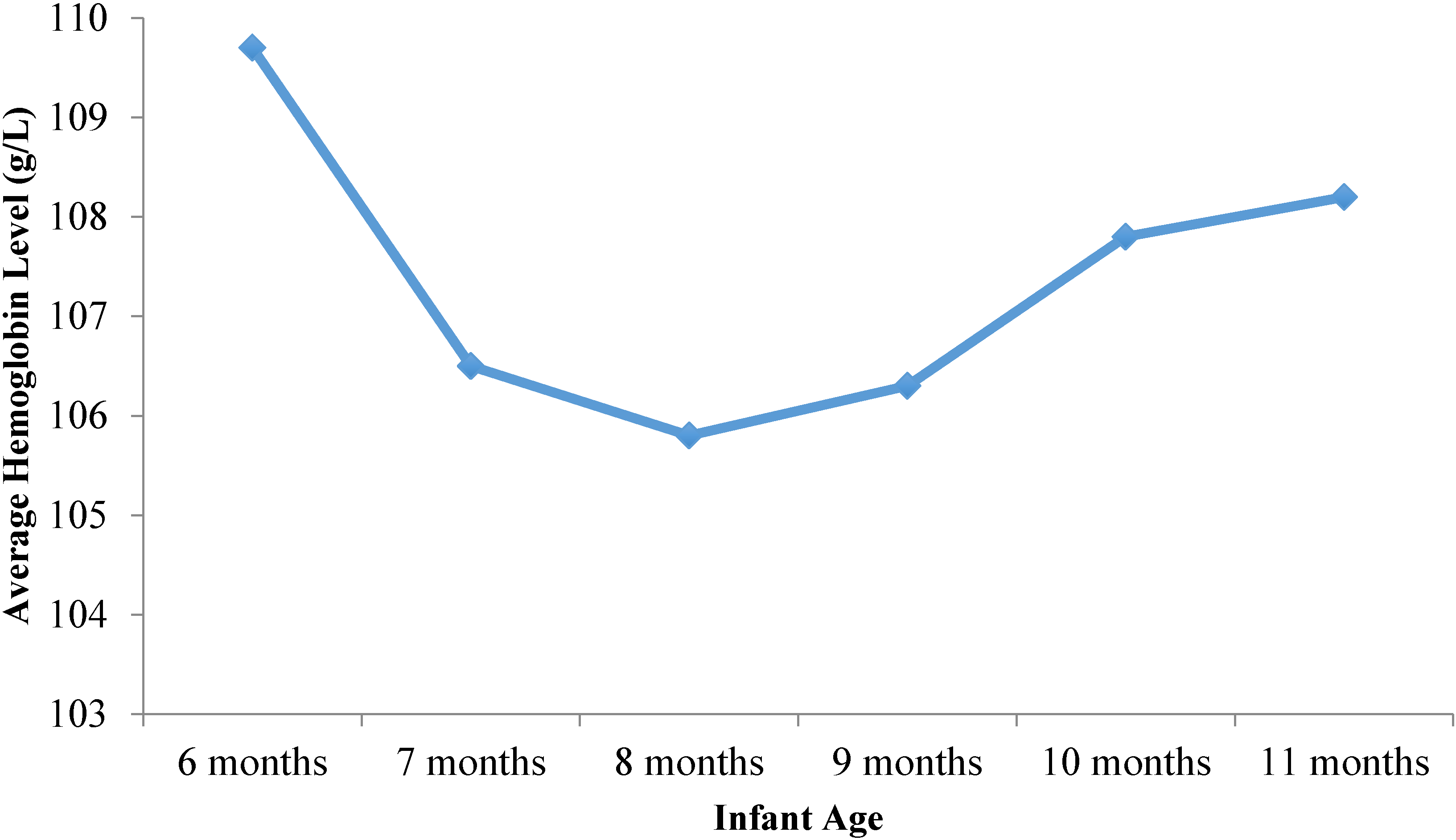
45]. It is known that iron needs during the first six months of life are primarily supplied by iron stores at birth; infants in well-nourished populations born at term and of normal birth weight typically have sufficient iron stores at birth to prevent iron deficiency until six months of age [
46]. The fact that our data show 50.7% anemia prevalence at age 6 months may therefore be indicative of poor maternal iron status during pregnancy. Given that 39% of our sample children were formula fed prior to 6 months of age (data not shown), and therefore would have been receiving additional iron supplementation, this high anemia prevalence at 6 months is even more troubling.
China’s infant nutrition problems appear to stem from poor quality weaning diets rather than insufficient energy intake. Child growth faltering, as measured by stunting, underweight and wasting, are at extremely low levels in the study population, ranging from only 1.2% to 3.4%. Such low rates are indicative of a population with virtually no linear growth failure. This contrast between the lack of linear growth failure and high anemia prevalence suggests that it is the quality of food, rather than the quantity, that is lacking in poor rural China today. This assertion is supported by our data on infant feeding practices, which show that while children seem to be introduced to complementary foods according to a timeline that fits with international guidelines, the typical weaning diet seems to be comprised primarily of staples, with less than one-quarter of sample children eating meat in the seven days prior to survey administration.
We were a bit surprised to see that there was no difference in anemia rates or Hb levels between low birth weight and normal birth weight infants, as the literature suggests otherwise [
47,
48]. We suspect that the absence of significant difference in our sample may stem from our small sample of low birth weight infants, accounting for only 5.0% of the total sample.
Our results also show that breastfeeding beyond 6 months of age is associated with significantly higher rates of anemia among sample children, although it is important to note that the quality of the weaning diet among the sample population was generally poor. These findings are similar to studies in Mexico and the U.S. in which exclusive breastfeeding for 6 months was associated with an increased risk of infant anemia (compared with exclusive breastfeeding for less than 6 months) [
46,
49]. Other studies have also identified weaning after 6 months as a risk factor for iron deficiency anemia in resource-limited countries, where infants are more likely to have lower iron stores at birth [
50,
51,
52].
The lower risk of anemia and higher Hb concentrations associated with formula feeding is perhaps not surprising as most infant formulas are fortified with iron and other micronutrients. The negative association between formula feeding and anemia has been reported in several other studies [
53,
54].
Our findings should not imply any deviation from WHO breastfeeding recommendations. It is well known that there are many benefits to breastfeeding, including protection against infectious morbidity, lower mortality, and promotion of adequate growth and development [
38,
55]. As a live substance, breast milk is uniquely suited to infants’ nutritional needs, and contains unparalleled immunological and anti-inflammatory properties that protect against a host of illnesses and diseases for both mothers and children. Formula feeding and early weaning from breast milk are linked to higher rates of a number of serious health conditions, ranging from ear infections and diarrhea to leukemia and sudden infant death syndrome [
56]. Our results may suggest, however, the importance of either iron supplementation or home fortification systems (possibly including other micronutrients) for breastfeeding infants in developing settings. At the very least, the quality of the weaning diet should be improved to include more and better sources of dietary iron. More study on this important issue is needed.
We have devoted some thought to potentially confounding exogenous factors that may have influenced our study results. One possibility may be that there are seasonal or temporal factors affecting our data that we may have overlooked. Based on previous studies of anemia among school-aged children in sample areas very similar to the ones used in this study, we know that anemia rates tend to be slightly lower in the spring than in the fall [
57,
58], likely due to the Chinese Spring Festival holiday, at which time many rural families slaughter the family hog and enjoy higher rates of meat consumption than at other times during the year. Given the low rate of meat consumption we observe among our sample infants, however, it is unclear if this same trend applies to the infant population used in this study. Overall, then, while we do not have any hard data on this question, we suspect that seasonal bias is not a significant issue, and if anything, the Hb levels we report in this study should be considered an upper bound, since our data was collected in the spring (April).
Another possibility we considered was whether other health conditions might be causing the high rates of anemia we observed in our study areas, such as thalassemia or hookworm. As it turns out, however, thalassemia in China typically occurs only in areas of China south of the Yangtze River, not in Shaanxi Province, where our study was conducted. Indeed, a search of hospital records in two of the largest teaching hospitals in Shaanxi Province and of the scientific literature on China’s northwestern provinces indicate no cases or suspected cases of thalassemia major in the past 30 years. Regarding hookworm, data from the National Survey of Human Parasites in China indicates a national average hookworm prevalence of 6.12%, with rates highest in the humid, tropical regions of southern China and lowest in the dry regions of northwest China, where our study was conducted [
59]. While data on hookworm prevalence was not published separately by province, it is safe to assume that hookworm prevalence in the survey areas is well below 6% overall, and likely even lower for children in our age group who are not independently mobile. It is therefore unlikely that either of these two diseases is behind the anemia prevalence we report in this study.
Another possible explanation for the high anemia prevalence we observe might be malaria; however, since malaria is not prevalent in the sample area [
60], we suspect that other factors, such as dietary insufficiencies, are more likely to be the root cause of the high anemia prevalence we report here.
One limitation of the study is its cross-sectional design, which does not allow us to identify causal relationships. Moreover, we were unable to conduct whole blood testing for nutritional deficiencies, and are therefore limited to considering hemoglobin as our sole indicator of micronutrient deficiency. Finally, since our data on infant feeding practices is based on caregiver recall, we cannot rule out the possibility of recall bias.
Another possible source of bias stems from the fact that our study children were identified based on a list of registered infants provided by the village family planning official, thus systematically excluding all unregistered children. The number of unregistered children has drastically declined in recent years, due to a combination of naturally declining fertility rates and loosening government policies. Indeed, a 2010 survey found the rate of unregistered children to be only around 0.12% [
61]. We therefore believe that this bias is negligible.



{kind=link}
