25-Hydroxyvitamin D and Its Relationship with Autonomic Dysfunction Using Time- and Frequency-Domain Parameters of Heart Rate Variability in Korean Populations: A Cross-Sectional Study



Abstract
:1. Introduction
2. Experimental Section
2.1. Study Population
2.2. Data Collection
2.3. Measurement of Serum 25-Hydroxyvitamin D
2.4. Heart Rate Variability Measurements
2.5. Statistical analysis
3. Results
3.1. Patients’ Characteristics

{kind=link}
| Variables | Total (n = 176) | 25-Hydroxyvitamin D Status | p-Value * | |
|---|---|---|---|---|
| Non-Deficient Group 25(OH)D ≥ 15 ng/mL (n = 126) | Deficient Group 25(OH)D < 15 ng/mL (n = 50) | |||
| Female (%) | 73 (41.5) | 42 (33.3) | 31 (62.0) | 0.001 |
| Age (year) | 55.3 ± 11.3 | 54.9 ± 11.7 | 55.9 ± 10.9 | 0.592 |
| BMI (kg/m2) | 24.0 ± 3.4 | 24.1 ± 3.2 | 23.8 ± 3.8 | 0.566 |
| WC (cm) | 83.8 ± 9.6 | 84.2 ± 9.4 | 82.2 ± 10.3 | 0.561 |
| SBP (mmHg) | 115.9 ± 12.7 | 115.2 ± 12.4 | 116.9 ± 13.3 | 0.510 |
| DBP (mmHg) | 71.4 ± 8.2 | 71.5 ± 7.7 | 71.5 ± 9.0 | 0.982 |
| TC (mg/dL) | 198.1 ± 36.7 | 199.8 ± 37.5 | 193.7 ± 34.5 | 0.323 |
| FPG (mg/dL) | 85.9 ± 11.9 | 86.1 ± 12.3 | 85.4 ± 11.3 | 0.753 |
| eGFR (mL/min/1.73 m2) | 90.1 ± 19.5 | 88.5 ± 1.8 | 94.1 ± 2.4 | 0.062 |
| Current smoker (%) | 49 (27.8) | 37 (29.4) | 12 (24.0) | 0.777 |
| Alcohol drinker (%) | 43 (24.4) | 34 (27.0) | 9 (18.0) | 0.247 |
| Regular exerciser (%) | 75 (42.6) | 54 (42.9) | 21 (42.0) | 0.527 |
| 25(OH)D (ng/mL) | 21.2 ± 9.9 | 25.2 ± 9.0 | 11.4 ± 2.5 | <0.001 |
| HRV time domain index | ||||
| Mean heart rate (bpm) | 70.0 ± 10.0 | 69.7 ± 10.7 | 70.6 ± 8.6 | 0.302 |
| SDNN (m/s) | 28.9 ± 14.5 | 30.2 ± 16.2 | 25.3 ± 8.4 | 0.044 |
| RMSSD (m/s) | 19.3 ± 13.2 | 20.0 ± 14.6 | 17.3 ± 8.3 | 0.235 |
| HRV frequency domain index | ||||
| Total power (log m/s2) | 6.13 ± 0.9 | 6.2 ± 0.9 | 6.0 ± 0.8 | 0.253 |
| VLF (log m/s2) | 5.43 ± 1.0 | 5.5 ± 1.0 | 5.3 ± 1.0 | 0.272 |
| LF (log m/s2) | 4.64 ± 1.2 | 4.7 ± 1.2 | 4.4 ± 1.1 | 0.120 |
| HF (log m/s2) | 4.01 ± 1.2 | 3.9 ± 1.2 | 4.0 ± 1.1 | 0.818 |
| LF/HF ratio | 4.18 ± 1.5 | 4.8 ± 1.2 | 2.6 ± 3.7 | 0.212 |

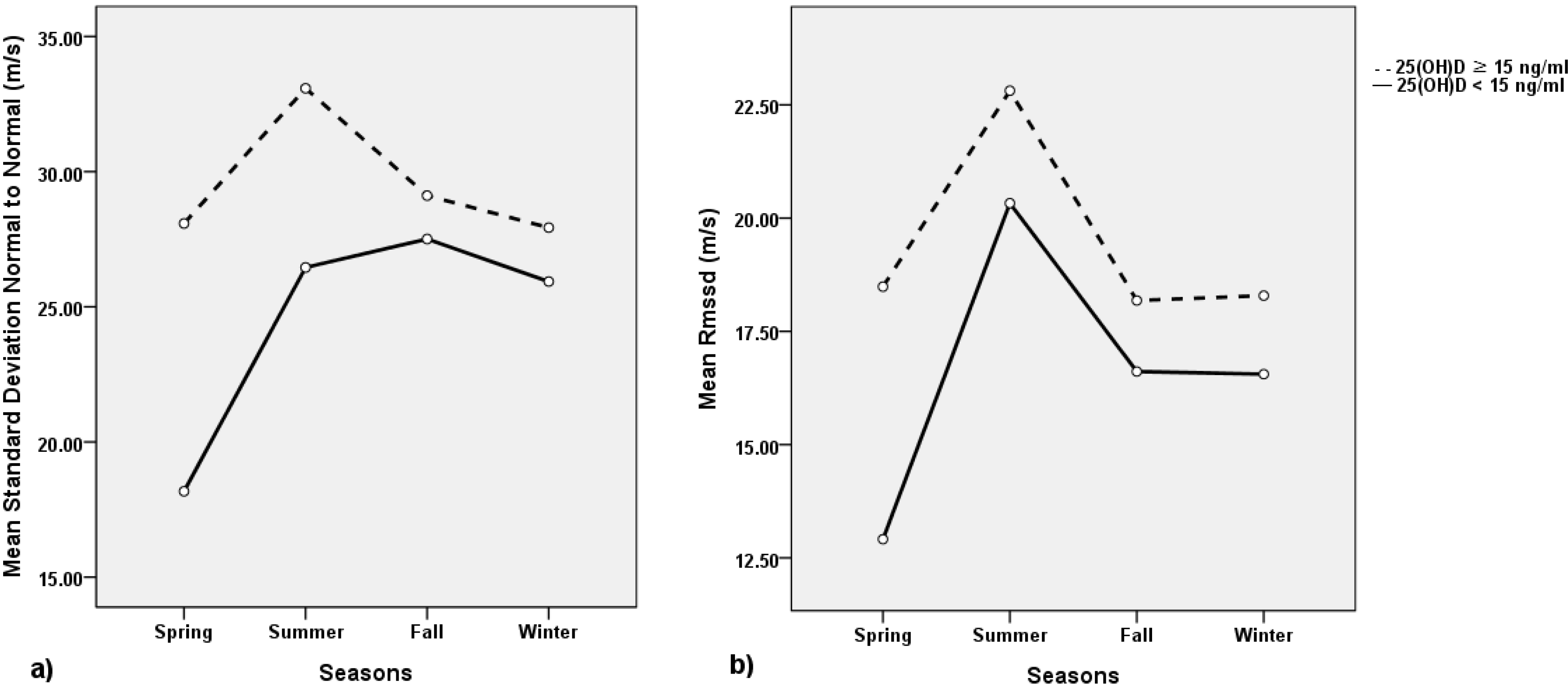
3.2. Associations of 25(OH)D Levels and HRV Time Domain
3.3. Associations of 25(OH)D Levels and HRV Frequency Domain
| Mean Heart Rate (bpm) | SDNN (m/s) | RMSSD (m/s) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| B ± SE | β | p-Value | B ± SE | β | p-Value | B ± SE | β | p-Value | |
| Univariate analysis | |||||||||
| Male | −1.014 ± 1.558 | −0.049 | 0.516 | −1.122 ± 2.232 | −0.038 | 0.616 | −1.890 ± 2.024 | −0.071 | 0.352 |
| Age (year) | −0.370 ± 0.061 | −0.419 | <0.001 | −0.158 ± 0.095 | −0.125 | 0.099 | 0.036 ± 0.087 | 0.032 | 0.676 |
| Winter-Spring | 1.325 ± 1.625 | 0.062 | 0.416 | −3.745 ± 2.314 | −0.121 | 0.107 | −2.899 ± 2.112 | −0.103 | 0.172 |
| BMI (kg/m2) | −0.503 ± 0.226 | −0.167 | 0.027 | 0.204 ± 0.327 | 0.047 | 0.533 | 0.358 ± 0.297 | 0.091 | 0.228 |
| WC (cm) | −0.124 ± 0.079 | −0.118 | 0.119 | 0.056 ± 0.114 | 0.037 | 0.623 | 0.137 ± 0.103 | 0.100 | 0.187 |
| SBP (mmHg) | 0.056 ± 0.061 | 0.070 | 0.358 | −0.009 ± 0.087 | −0.008 | 0.917 | 0.025 ± 0.079 | 0.024 | 0.751 |
| DBP (mmHg) | 0.144 ± 0.094 | 0.115 | 0.129 | 0.025 ± 0.136 | 0.014 | 0.857 | 0.063 ± 0.124 | 0.038 | 0.613 |
| TC (mg/dL) | −0.012 ± 0.021 | −0.045 | 0.561 | −0.008 ± 0.030 | −0.021 | 0.784 | −0.020 ± 0.028 | −0.056 | 0.464 |
| FPG (mg/dL) | −0.081 ± 0.063 | −0.098 | 0.201 | −0.052 ± 0.093 | −0.043 | 0.576 | −0.012 ± 0.085 | −0.011 | 0.886 |
| eGFR (mL/min/1.73 m2) | 0.027 ± 0.039 | 0.053 | 0.486 | −0.066 ± 0.056 | −0.089 | 0.241 | −0.029 ± 0.051 | −0.043 | 0.571 |
| Current smoker | −1.588 ± 1.704 | −0.070 | 0.353 | −0.140 ± 2.445 | −0.004 | 0.954 | 1.645 ± 2.244 | 0.056 | 0.460 |
| Alcohol drinker | −1.205 ± 1.779 | −0.051 | 0.499 | −1.292 ± 2.549 | −0.038 | 0.613 | −0.785 ± 2.323 | −0.026 | 0.736 |
| Regular exerciser | −3.238 ± 1.524 | −0.159 | 0.035 | 4.185 ± 2.187 | 0.143 | 0.057 | 5.223 ± 1.974 | 0.196 | 0.009 |
| 25(OH)D (ng/mL) | 0.077 ± 0.077 | 0.075 | 0.322 | 0.396 ± 0.107 | 0.272 | <0.001 | 0.220 ± 0.099 | 0.165 | 0.028 |
| Multivariate analysis | |||||||||
| Male | −0.549 ± 1.429 | −0.027 | 0.701 | −1.012 ± 2.159 | −0.034 | 0.640 | −1.997 ± 2.008 | −0.075 | 0.321 |
| Age (year) | −0.369 ± 0.063 | −0.418 | < 0.001 | −0.095 ± 0.095 | −0.075 | 0.317 | 0.078 ± 0.088 | 0.068 | 0.380 |
| Winter-Spring | 0.856 ± 1.526 | 0.040 | 0.575 | −2.576 ± 2.305 | −0.083 | 0.265 | −1.981 ± 2.144 | −0.071 | 0.357 |
| 25(OH)D (ng/mL) | −0.007 ± 0.074 | −0.007 | 0.920 | 0.350 ± 0.111 | 0.240 | 0.002 | 0.220 ± 0.104 | 0.166 | 0.035 |
| R2 | 0.178 | 0.086 | 0.042 | ||||||
| Total Power (log m/s2) | HF (log m/s2) | LF (log m/s2) | VLF (log m/s2) | LF/HF Ratio (log) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B ± SE | β | p-Value | B ± SE | β | p-Value | B ± SE | β | p-Value | B ± SE | β | p-Value | B ± SE | β | p-Value | |
| Univariate analysis | |||||||||||||||
| Male | −0.090 ± 0.136 | −0.050 | 0.507 | −0.272 ± 0.187 | −0.110 | 0.147 | 0.124 ± 0.180 | 0.052 | 0.491 | −0.106 ± 0.157 | −0.051 | 0.500 | 0.392 ± 0.176 | 0.167 | 0.027 |
| Age (year) | −0.027 ± 0.005 | −0.349 | <0.001 | −0.015 ± 0.008 | −0.139 | 0.067 | −0.043 ± 0.007 | −0.421 | <0.001 | −0.024 ± 0.006 | −0.274 | <0.001 | −0.028 ± 0.007 | −0.280 | <0.001 |
| Winter-Spring | 0.004 ± 0.142 | 0.002 | 0.979 | −0.125 ± 0.197 | −0.048 | 0.526 | −0.123 ± 0.188 | −0.049 | 0.515 | 0.146 ± 0.166 | 0.067 | 0.379 | 1.852 ± 1.690 | 0.083 | 0.275 |
| BMI (kg/m2) | −0.001 ± 0.020 | −0.004 | 0.955 | 0.011 ± 0.028 | 0.031 | 0.680 | −0.006 ± 0.026 | −0.017 | 0.823 | −0.011 ± 0.023 | −0.037 | 0.630 | −0.018 ± 0.026 | −0.051 | 0.497 |
| WC (cm) | −0.004 ± 0.007 | −0.046 | 0.546 | −0.001 ± 0.010 | −0.004 | 0.958 | −0.007 ± 0.009 | −0.057 | 0.450 | −0.006 ± 0.008 | −0.053 | 0.482 | −0.007 ± 0.009 | −0.057 | 0.455 |
| SBP (mmHg) | −0.004 ± 0.005 | −0.060 | 0.425 | 0.001 ± 0.007 | −0.002 | 0.974 | −0.008 ± 0.007 | −0.083 | 0.272 | −0.005 ± 0.006 | −0.056 | 0.462 | −0.008 ± 0.007 | −0.083 | 0.275 |
| DBP (mmHg) | 0.001 ± 0.008 | 0.011 | 0.886 | 0.001 ± 0.011 | −0.002 | 0.975 | −0.007 ± 0.011 | −0.045 | 0.550 | 0.003 ± 0.010 | 0.022 | 0.774 | −0.006 ± 0.011 | −0.044 | 0.564 |
| TC (mg/dL) | −0.001 ± 0.002 | −0.014 | 0.853 | −0.002 ± 0.003 | −0.056 | 0.462 | 0.001 ± 0.002 | −0.009 | 0.909 | 0.001 ± 0.002 | 0.009 | 0.907 | 0.002 ± 0.002 | 0.054 | 0.484 |
| FPG (mg/dL) | −0.007 ± 0.006 | −0.100 | 0.189 | −0.012 ± 0.008 | −0.121 | 0.113 | −0.014 ± 0.007 | −0.146 | 0.055 | −0.004 ± 0.007 | −0.048 | 0.527 | −0.002 ± 0.007 | −0.019 | 0.804 |
| eGFR (mL/min/1.73 m2) | 0.001 ± 0.003 | 0.026 | 0.728 | 0.008 ± 0.005 | 0.124 | 0.100 | 0.004 ± 0.005 | 0.069 | 0.361 | −0.001 ± 0.004 | −0.028 | 0.716 | −0.004 ± 0.004 | −0.061 | 0.420 |
| Current smoker | −0.070 ± 0.149 | −0.036 | 0.639 | −0.196 ± 0.206 | −0.072 | 0.353 | 0.021 ± 0.197 | 0.008 | 0.917 | −0.065 ± 0.174 | −0.028 | 0.711 | 0.223 ± 0.195 | 0.086 | 0.256 |
| Alcohol drinker | −0.043 ± 0.156 | −0.021 | 0.783 | −0.197 ± 0.215 | −0.069 | 0.360 | −0.024 ± 0.206 | −0.009 | 0.906 | −0.016 ± 0.182 | −0.007 | 0.929 | 0.173 ± 0.204 | 0.064 | 0.399 |
| Regular exerciser | 0.105 ± 0.135 | 0.059 | 0.437 | 0.243 ± 0.186 | 0.098 | 0.194 | 0.137 ± 0.178 | 0.058 | 0.441 | −0.025 ± 0.158 | −0.012 | 0.874 | −0.104 ± 0.177 | −0.044 | 0.559 |
| 25(OH)D (ng/mL) | 0.017 ± 0.007 | 0.195 | 0.010 | 0.006 ± 0.009 | 0.050 | 0.510 | 0.028 ± 0.009 | 0.234 | 0.002 | 0.019 ± 0.008 | 0.186 | 0.013 | 0.021 ± 0.009 | 0.179 | 0.017 |
| Multivariate analysis | |||||||||||||||
| Male | −0.057 ± 0.128 | −0.032 | 0.656 | −0.261 ± 0.187 | −0.105 | 0.164 | 0.172 ± 0.162 | 0.073 | 0.290 | −0.069 ± 0.151 | −0.033 | 0.647 | 0.430 ± 0.168 | 0.183 | 0.012 |
| Age (year) | −0.025 ± 0.006 | −0.320 | <0.001 | −0.014 ± 0.008 | −0.133 | 0.087 | −0.040 ± 0.007 | −0.395 | < 0.001 | −0.021 ± 0.007 | −0.237 | 0.002 | −0.026 ± 0.007 | −0.261 | < 0.001 |
| Winter-Spring | −0.018 ± 0.137 | 0.009 | 0.896 | −0.134 ± 0.199 | −0.052 | 0.503 | −0.092 ± 0.173 | −0.037 | 0.598 | 0.160 ± 0.161 | 0.074 | 0.994 | 0.037 ± 0.180 | 0.015 | 0.836 |
| 25(OH)D (ng/mL) | 0.011 ± 0.007 | 0.128 | 0.086 | 0.001 ± 0.010 | 0.011 | 0.893 | 0.017 ± 0.008 | 0.144 | 0.044 | 0.015 ± 0.008 | 0.148 | 0.052 | 0.015 ± 0.009 | 0.129 | 0.085 |
| R2 | 0.138 | 0.033 | 0.205 | 0.099 | 0.127 | ||||||||||
| 25(OH)D Status | SDNN (<30 m/s) | RMSSD (<10 m/s) |
|---|---|---|
| OR (95% Confidence Interval) | OR (95% Confidence Interval) | |
| Model 1 | ||
| 25(OH)D ≥ 15 ng/mL | 1.00 (reference) | 1.00 (reference) |
| 25(OH)D < 15 ng/mL | 2.38 (1.14–4.97) | 1.60 (0.68–3.79) |
| Model 2 | ||
| 25(OH)D ≥ 15 ng/mL | 1.00 (reference) | 1.00 (reference) |
| 25(OH)D < 15 ng/mL | 2.62 (1.19–5.72) | 1.78 (0.72–4.39) |
| Model 3 | ||
| 25(OH)D ≥ 15 ng/mL | 1.00 (reference) | 1.00 (reference) |
| 25(OH)D < 15 ng/mL | 3.07 (1.32–7.14) | 1.86 (0.70–4.96) |
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Nagpal, S.; Na, S.Q.; Rathnachalam, R. Noncalcemic actions of vitamin D receptor ligands. Endocr. Rev. 2005, 26, 662–687. [Google Scholar] [PubMed]
- Looker, A.C.; Pfeiffer, C.M.; Lacher, D.A.; Schleicher, R.L.; Picciano, M.F.; Yetley, E.A. Serum 25-hydroxyvitamin D status of the US population: 1988–1994 compared with 2000–2004. Am. J. Clin. Nutr. 2008, 88, 1519–1527. [Google Scholar] [CrossRef] [PubMed]
- Dobnig, H.; Pilz, S.; Scharnagl, H.; Renner, W.; Seelhorst, U.; Wellnitz, B.; Kinkeldi, J.; Boehm, B.O.; Weihrauch, G.; Maerz, W.; et al. Independent association of low serum 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D levels with all-cause and cardiovascular mortality. Arch. Intern. Med. 2008, 168, 1340–1349. [Google Scholar] [CrossRef]
- Shen, H.; Bielak, L.F.; Ferguson, J.F.; Streeten, E.A.; Yerges-Armstrong, L.M.; Liu, J.; Post, W.; O’Connell, J.R.; Hixson, J.E.; Kardia, S.L.; et al. Association of the vitamin D metabolism gene cyp24a1 with coronary artery calcification. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 2648–2654. [Google Scholar] [CrossRef]
- Chan, C.T.; Levin, N.W.; Chertow, G.M.; Larive, B.; Schulman, G.; Kotanko, P. The Frequent Hemodialysis Network Daily Trial Group. Determinants of Cardiac Autonomic Dysfunction in ESRD. Clin. J. Am. Soc. Nephrol. 2010, 5, 1821–1827. [Google Scholar] [CrossRef] [PubMed]
- Pumprla, J.; Howorka, K.; Groves, D.; Chester, M.; Nolan, J. Functional assessment of heart rate variability: Physiological basis and practical applications. Int. J. Cardiol. 2002, 84, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Dekker, J.M.; Crow, R.S.; Folsom, A.R.; Hannan, P.J.; Liao, D.; Swenne, C.A.; Schouten, E.G. Low heart rate variability in a 2-minute rhythm strip predicts risk of coronary heart disease and mortality from several causes: The ARIC Study. Circulation 2000, 102, 1239–1244. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Hansen, A.L.; Saus-Rose, E.; Johnsen, B.H. Heart rate variability, prefrontal neural function, and cognitive performance: The neurovisceral integration perspective on self-regulation, adaptation, and health. Ann. Behav. Med. 2009, 37, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.B. Depression, heart rate related variables and cardiovascular disease. Int. J. Psychophysiol. 2010, 78, 80–88. [Google Scholar] [CrossRef] [PubMed]
- La Rovere, M.T.; Pinna, G.D.; Maestri, R.; Mortara, A.; Capomolla, S.; Febo, O.; Ferrari, R.; Franchini, M.; Gnemmi, M.; Opasich, C.; et al. Short-term heart rate variability strongly predicts sudden cardiac death in chronic heart failure patients. Circulation 2003, 107, 565–570. [Google Scholar] [CrossRef]
- Corrao, G.; Bagnardi, V.; Zambon, A.; la Vecchia, C. A meta-analysis of alcohol consumption and the risk of 15 diseases. Prev. Med. 2004, 38, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Haapanen, N.; Miilunpalo, S.; Pasanen, M.; Oja, P.; Vuori, I. Association between leisure time physical activity and 10-yr body mass change among working-aged men and women. Int. J. Obes. Relat. Metab. Disord. 1997, 21, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, S.J. Vitamin D metabolism and the clinical aspects of measuring metabolites. Ann. Clin. Biochem. 1994, 31, 109–124. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Pencina, M.J.; Booth, S.L.; Jacques, P.F.; Ingelsson, E.; Lanier, K.; Benjamin, E.J.; D’Agostino, R.B.; Wolf, M.; Vasan, R.S.; et al. Vitamin D deficiency and risk of cardiovascular disease. Circulation 2008, 117, 503–511. [Google Scholar] [CrossRef]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart rate variability standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar]
- Metelka, R. Heart rate variability—Current diagnosis of the cardiac autonomic neuropathy. A review. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech. Repub. 2014, 158. [Google Scholar] [CrossRef]
- Bilchick, K.C.; Berger, R.D. Heart rate variability. J. Cardiovasc. Electrophysiol. 2006, 17, 691–394. [Google Scholar] [CrossRef] [PubMed]
- Tishkoff, D.X.; Nibbelink, K.A.; Holmberg, K.H.; Dandu, L.; Simpson, R.U. Functional vitamin D receptor (VDR) in the t-tubules of cardiac myocytes: VDR knockout cardiomyocyte contractility. Endocrinology 2008, 149, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Xiang, W.; Kong, J.; Chen, S.; Cao, L.P.; Qiao, G.; Zheng, W.; Liu, W.; Li, X.; Gardner, D.G.; Li, Y.C.; et al. Cardiac hypertrophy in vitamin D receptor knockout mice: Role of the systemic and cardiac reninangiotensin systems. Am. J. Physiol. Endocrinol. Metab. 2005, 288, 125–132. [Google Scholar] [CrossRef]
- Nigwekar, S.U.; Thadhani, R. Vitamin D receptor activation: Cardiovascular and renal implications. Kidney Int. Suppl. 2013, 3, 427–430. [Google Scholar] [CrossRef]
- Cozzolino, M.; Ketteler, M.; Zehnder, D. The vitamin D system: A crosstalk between the heart and kidney. Eur. J. Heart Fail. 2010, 12, 1031–1041. [Google Scholar] [CrossRef] [PubMed]
- Brewster, U.C.; Setaro, J.F.; Perazella, M.A. The renin-angiotensin-aldosterone system: Cardiorenal effects and implications for renal and cardiovascular disease states. Am. J. Med. Sci. 2003, 326, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Van Ballegooijen, A.J.; Visser, M.; Snijder, M.B.; Dekker, J.M.; Nijpels, G.; Stehouwer, C.D.A.; Diamant, M.; Brouwer, I.A. Serum 25-hydroxyvitamin D and parathyroid hormone in relation to plasma B-type natriuretic peptide: The Hoorn Study. Endocr. Connect. 2012, 1, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Kendrick, J.; Targher, G.; Smits, G.; Chonchol, M. 25-Hydroxyvitamin D deficiency is independently associated with cardiovascular disease in the Third National Health and Nutrition Examination Survey. Atherosclerosis 2009, 205, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Giovannucci, E.; Liu, Y.; Hollis, B.W.; Rimm, E.B. 25-hydroxyvitamin D and risk of myocardial infarction in men: A prospective study. Arch. Intern. Med. 2008, 168, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, K.; Terui, N.; Kollai, M. Effect of cardiac vagal and sympathetic nerve activity on heart rate in rhythmic fluctuations. J. Auton. Nerv. Syst. 1985, 12, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.; Batin, P.D.; Andrews, R.; Lindsay, S.J.; Brooksby, P.; Mullen, M.; Baig, W.; Flapan, A.D.; Cowley, A.; Prescott, R.J.; et al. Prospective study of heart rate variability and mortality in chronic heart failure: Results of the United Kingdom heart failure evaluation and assessment of risk trial (UK-Heart). Circulation 1998, 98, 1510–1516. [Google Scholar] [CrossRef]
- Hu, J.; Gao, J.; Tung, W.W.; Cao, Y. Multiscale Analysis of Heart Rate Variability: A Comparison of Different Complexity Measures. Ann. Biomed. Eng. 2010, 38, 854–864. [Google Scholar] [CrossRef] [PubMed]
- Guzzetti, S.; Cogliati, C.; Turiel, M.; Crema, C.; Lombardi, F.; Malliani, A. Sympathetic predominance followed by functional denervation in the progression of chronic heart failure. Eur. Heart J. 1995, 16, 1100–1107. [Google Scholar] [PubMed]
- Galinier, M.; Fourcade, J.; Ley, N.; Boveda, S.; Solera, S.; Solera, M.L.; Masabuau, P.; Elhabaj, S.; Fauvel, J.M.; Valdiquie, P.; et al. Hyperinsulinism, heart rate variability and circadian variability of arterial pressure in obese hypertensive patients. Arch. Mal. Coeur. Vaiss. 1999, 92, 1105–1109. [Google Scholar]
- Brian, O.; Hani, N.S.; Hauptman, P.J.; Colucci, W.S. Parasympathetic Nervous System and Heart Failure: Pathophysiology and Potential Implications for Therapy. Circulation 2008, 118, 863–871. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Tomaschitz, A.; Drechsler, C.; Dekker, J.M.; Marz, W. Vitamin D deficiency and myocardial diseases. Mol. Nutr. Food Res. 2010, 54, 1103–1113. [Google Scholar] [PubMed]
- Bigger, J.T.; Fleiss, J.L.; Steinman, R.C.; Rolnitzky, L.M.; Kleiger, R.E.; Rottman, J.N. Frequency domain measures of heart period variability and mortality after myocardial infarction. Circulation 1992, 85, 164–171. [Google Scholar] [CrossRef] [PubMed]
- La Rovere, M.T.; Bigger, J.T.; Marcus, F.I.; Mortara, A.; Schwartz, P.J. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Tone and Reflexes after Myocardial Infarction) Investigators. Lancet 1998, 351, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Bittner, V.; Wenger, N.K.; Waters, D.D.; DeMicco, D.A.; Messig, M.; LaRosa, J.C. Vitamin D levels do not predict cardiovascular events in statin-treated patients with stable coronary disease. Am. Heart J. 2012, 164, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Yiu, Y.F.; Yiu, K.H.; Siu, C.W.; Chan, Y.H.; Li, S.W.; Wong, L.Y.; Lee, S.W.; Tam, S.; Wong, E.W.; Lau, C.P.; et al. Randomized controlled trial of vitamin D supplement on endothelial function in patients with type 2 diabetes. Atherosclerosis 2013, 227, 140–146. [Google Scholar] [CrossRef]
- Alele, J.D.; Luttrell, L.M.; Hollis, B.W.; Luttrell, D.K.; Hunt, K.J.; VADT Study Group. Relationship between vitamin D status and incidence of vascular events in the Veterans Affairs Diabetes Trial. Atherosclerosis 2013, 228, 502–507. [Google Scholar] [CrossRef]
- Mann, M.C.; Exner, D.V.; Hemmelgarn, B.R.; Sola, D.Y.; Turin, T.C.; Ellis, L.; Ahmed, S.B. Vitamin D Levels Are Associated with Cardiac Autonomic Activity in Healthy Humans. Nutrients 2013, 5, 2114–2127. [Google Scholar] [CrossRef] [PubMed]
- Cetin, M.; Kozdag, G.; Ural, D.; Kahraman, G.; Yilmaz, I.; Akay, Y.; Onuk, R.; Dursun, N. Could decreased vitamin D levels be related with impaired cardiac autonomic functions in patients with chronic heart failure: An observational study. Anadolu Kardiyol. Derg. 2014, 14. [Google Scholar] [CrossRef]
- Pilz, S.; Marz, W.; Wellnitz, B.; Seelhorst, U.; Fahrleitner-Pammer, A.; Dimai, H.P.; Boehm, B.O.; Dobnig, H. Association of vitamin D deficiency with heart failure and sudden cardiac death in a large cross-sectional study of patients referred for coronary angiography. J. Clin. Endocrinol. Metab. 2008, 93, 3927–3935. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.W.; Park, C.W.; Shin, Y.S.; Kim, Y.S.; Shin, S.J.; Kim, Y.S.; Choi, E.J.; Chang, Y.S.; Bang, B.K. Calcitriol regresses cardiac hypertrophy and QT dispersion in secondary hyperparathyroidism on hemodialysis. Nephron Clin. Pract. 2006, 102, 21–29. [Google Scholar] [CrossRef]
- Saleh, F.N.; Schirmer, H.; Sundsfjord, J.; Jorde, R. Parathyroid hormone and left ventricular hypertrophy. Eur. Heart J. 2003, 24, 2054–2060. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Chen, C.; Liu, H.L.; Qian, G. Vitamin D, Parathyroid hormone and heart failure in a Chinese elderly. Endocr. Pract. 2014, 6, 1–42. [Google Scholar]
- Geleijnse, J.M. Vitamin D and the prevention of hypertension and cardiovascular diseases: A review of the current evidence. Am. J. Hypertens. 2011, 24, 253–262. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tak, Y.J.; Lee, J.G.; Kim, Y.J.; Lee, S.Y.; Cho, B.M. 25-Hydroxyvitamin D and Its Relationship with Autonomic Dysfunction Using Time- and Frequency-Domain Parameters of Heart Rate Variability in Korean Populations: A Cross-Sectional Study. Nutrients 2014, 6, 4373-4388. https://doi.org/10.3390/nu6104373
Tak YJ, Lee JG, Kim YJ, Lee SY, Cho BM. 25-Hydroxyvitamin D and Its Relationship with Autonomic Dysfunction Using Time- and Frequency-Domain Parameters of Heart Rate Variability in Korean Populations: A Cross-Sectional Study. Nutrients. 2014; 6(10):4373-4388. https://doi.org/10.3390/nu6104373
Chicago/Turabian StyleTak, Young Jin, Jeong Gyu Lee, Yun Jin Kim, Sang Yeoup Lee, and Byung Mann Cho. 2014. "25-Hydroxyvitamin D and Its Relationship with Autonomic Dysfunction Using Time- and Frequency-Domain Parameters of Heart Rate Variability in Korean Populations: A Cross-Sectional Study" Nutrients 6, no. 10: 4373-4388. https://doi.org/10.3390/nu6104373
APA StyleTak, Y. J., Lee, J. G., Kim, Y. J., Lee, S. Y., & Cho, B. M. (2014). 25-Hydroxyvitamin D and Its Relationship with Autonomic Dysfunction Using Time- and Frequency-Domain Parameters of Heart Rate Variability in Korean Populations: A Cross-Sectional Study. Nutrients, 6(10), 4373-4388. https://doi.org/10.3390/nu6104373