Dietary Intake and Food Habits of Pregnant Women Residing in Urban and Rural Areas of Deyang City, Sichuan Province, China

Abstract
:1. Introduction
2. Participants and Methods
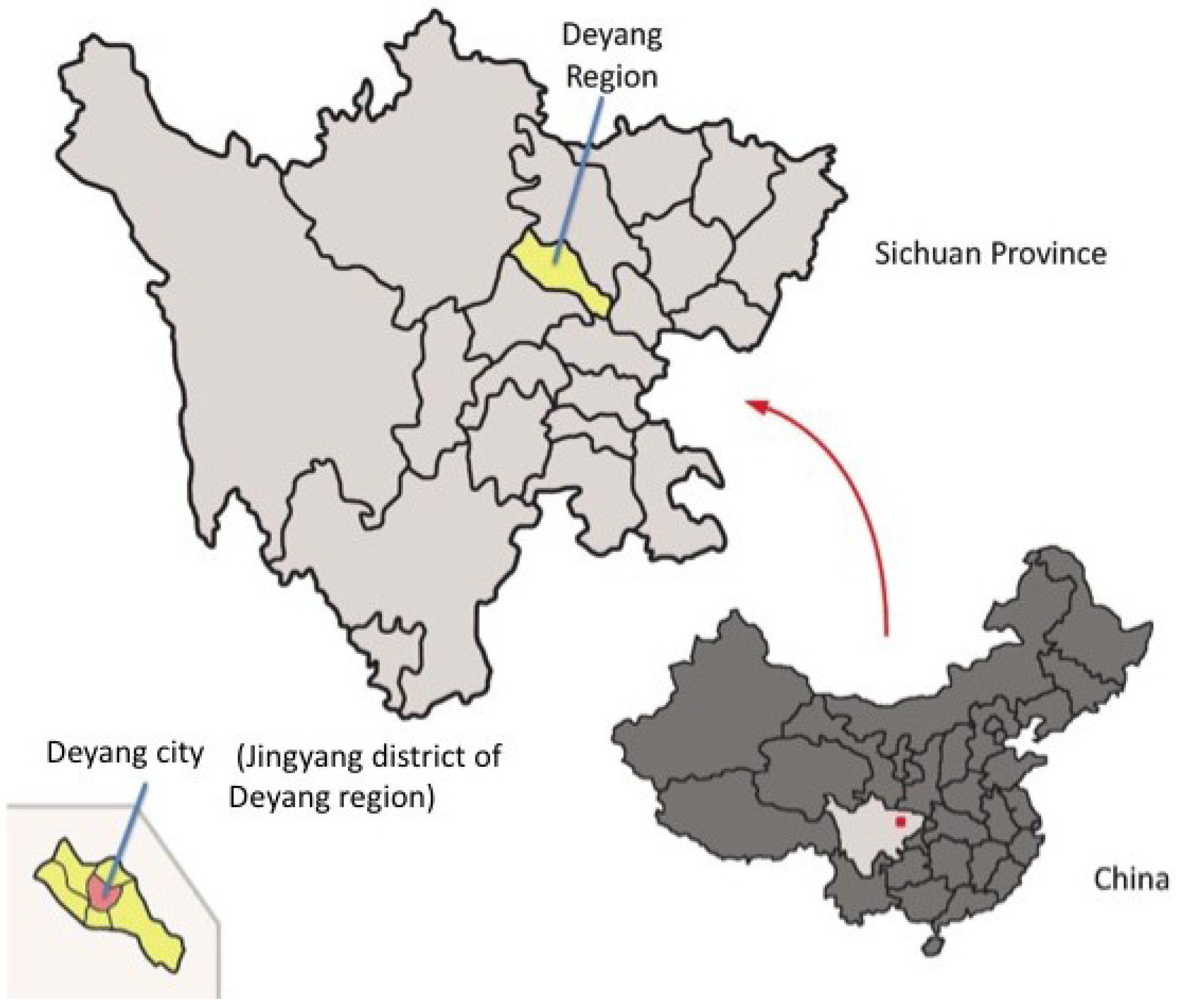
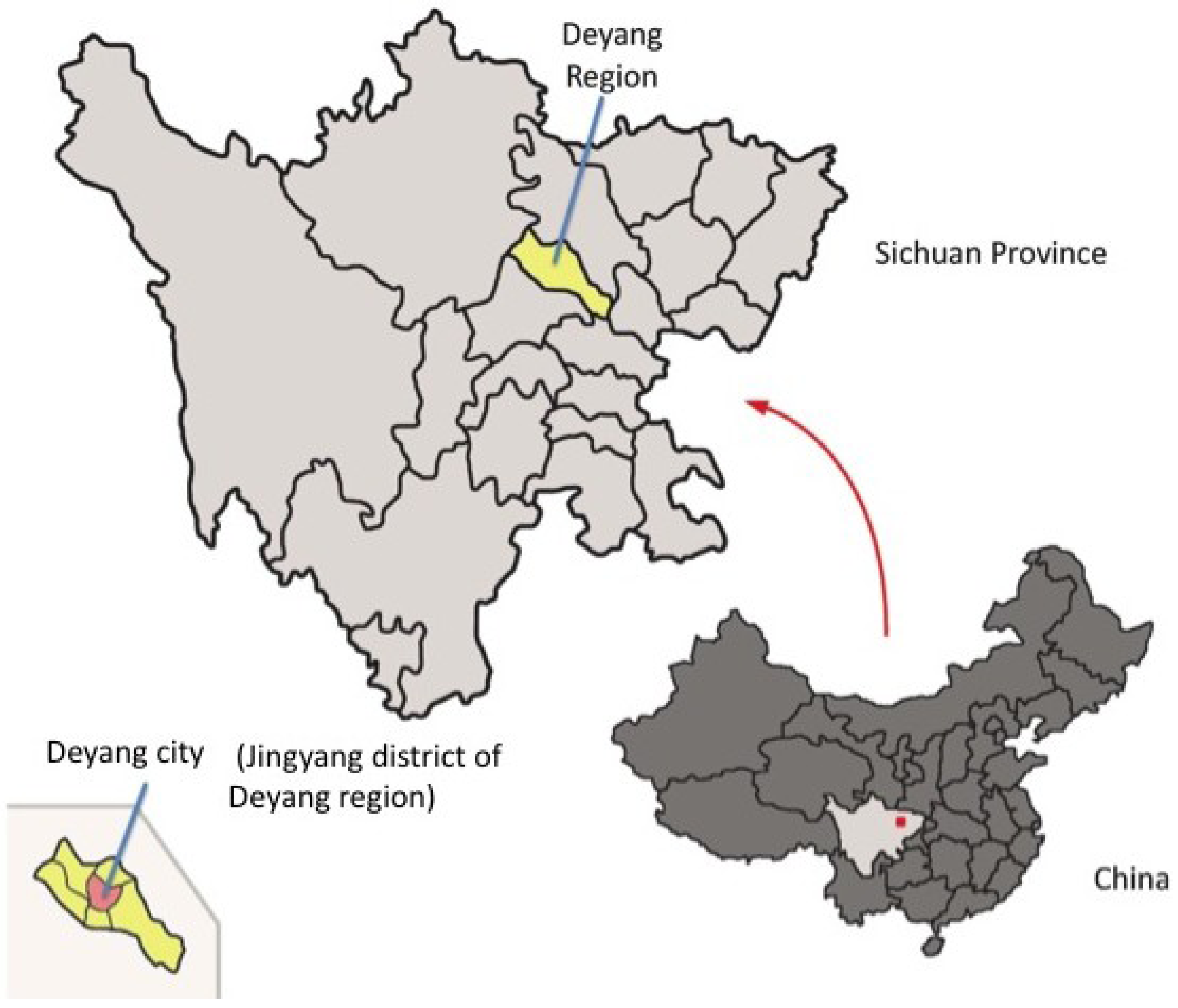
2.1. Study Design and Population
2.2. Dietary Assessment
2.3. Anthropometric Assessment
2.4. Statistical Methods and Food Intake Analyses
2.5. Ethical Clearance
3. Results
3.1. Socio-Demographic Characteristics
3.2. Antenatal Food Habits and the Cultural Beliefs and Fears Entailed

{kind=link}
| Food taboos during the pregnancy & qualitative analysis of cultural fears entailed | |||
|---|---|---|---|
| Urban n = 82 | Rural n = 60 | ||
| Metaphysically “cold” foods | n (%) | n (%) | |
| Crab | 0 | 1 (1.7) | May induce premature birth or miscarriage |
| Soft-shelled turtle | 0 | 1 (1.7) | |
| Snake | 1 (1.2) | 0 | |
| Ice cream | 0 | 1 (1.7) | |
| Sprite | 0 | 1 (1.7) | |
| “Cool” foods | 4 (4.9) | 8 (13.3) | |
| Metaphysically “hot” foods | n (%) | n (%) | |
| Dog | 1 (1.2) | 2 (3.3) | Dog flesh is hot in the hot-cold classification of foods.
The baby may bite the mother |
| Metaphysically “toxic” foods | n (%) | n (%) | |
| Rabbit | 58 (70.7) | 40 (66.7) | Causes harelip or cleft palates in the fetus, rabbit head |
| Eel | 8 (9.8) | 10 (16.7) | Causes foaming at the mouth of the newborn |
| Beef | 20 (24.4) | 22 (36.7) | Child may have a stubborn temper like an ox |
| Fish | 1 (1.2) | 2 (3.3) | Baby may get bacterial infection of the skin more easily |
| Duck | 7 (8.5) | 9 (15) | Newborn’s neck will be weak or lack power. Causes duck head |
| Lamb, mutton, goat | 62 (75.6) | 49 (81.7) | Fetus will suffer from epilepsy |
| Sow | 1 (1.2) | 1 (1.7) | |
| Chinese anise | 1 (1.2) | 0 | Harmful due to lots of flavors, may contain rosin (colophony), not fresh enough, traditional reasons |
| Clove | 1 (1.2) | 0 | |
| Hot pot | 1 (1.2) | 0 | |
| Braised/stewed meat | 4 (4.9) | 0 | |
| Bacon | 1 (1.2) | 0 | |
| Leek | 1 (1.2) | 0 | |
| Sauerkraut | 1 (1.2) | 0 | |
3.3. Result of 24-h Recall
3.3.1. Dietary Intake of Participants at the Two Survey Sites (Urban vs. Rural)
| % of energy | AMDRs • | Total (n = 192) | Urban (n = 125) | Rural (n = 67) | p-Value 1 |
|---|---|---|---|---|---|
| Derived from protein | 10–15 | 12.1 ± 2.9 | 12.3 ± 2.8 | 11.6 ± 3 | 0.118 ns |
| Derived from fat | 20–30 | 39 ± 11.2 | 40.4 ± 10.8 | 36.6 ± 11.6 | 0.025 * |
| Derived from carbohydrate | 55–65 | 49.6 ± 11.4 | 48.1 ± 11.1 | 52.4 ± 11.7 | 0.012 * |
| Total (n = 192) | Urban (n = 125) | Rural (n = 67) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Energy and nutrient (unit/day) | RNIs/AIs • | Mean ± SD | % fulfillment
RNI | Range | Mean ± SD | % fulfillment
RNI | Range | Mean ± SD | % fulfillment
RNI | Range | p-Value 1 Mean ± SD |
| Energy (kcal) | 2300 | 2338 ± 844 | 101.7 | 566–5705 | 2441 ± 834 | 106.1 | 767–5705 | 2148 ± 837 | 93.4 | 565–4514 | 0.021 * |
| Protein (g) | 85 | 69.4 ± 26.7 | 81.6 | 15.3–171.2 | 73.9 ± 26.9 | 86.9 | 16.7–171.2 | 60.9 ± 24.4 | 71.6 | 15.3–130.6 | 0.001 *** |
| Fat (g) | 51–77 † | 105.7 ± 58 | 137.3 ‡ | 11.3–348.1 | 112.9 ± 57.8 | 146.6 ‡ | 11.3–348.1 | 92.2 ± 56.4 | 119.7 ‡ | 14.8–282.1 | 0.018 * |
| Carbohydrate (g) | 316–374 † | 281.5 ± 103.9 | 89.1 § | 89.1–670.6 | 286.5 ± 102.5 | 90.7 § | 124.2–616.6 | 272.1 ± 106.6 | 86.1 § | 89.1–670.6 | 0.311 ns |
| Vitamin A (µg RE) | 900 | 757.5 (±920.8) | 84.2 | 10–8520.7 | 849.1 (±1032) | 94.3 | 46.1–8520.7 | 586.4 (±638.1) | 65.2 | 10–3093 | 0.005 ** |
| Vitamin C (mg) | 130 | 104.3 (±110.1) | 80.2 | 1.6–744.1 | 106.8 (±112.4) | 82.2 | 1.6–744.1 | 99.7 (±106.4) | 76.7 | 7.28–697.8 | 0.589 ns |
| Thiamin (B1) (mg) | 1.5 | 0.81 ± 0.41 | 54 | 0.25–2.66 | 0.81 ± 0.39 | 54 | 0.25–2.53 | 0.79 ± 0.44 | 52.7 | 0.26–2.66 | 0.517 ns |
| Riboflavin (B2) (mg) | 1.7 | 1.19 ± 0.58 | 70 | 0.16–4.26 | 1.27 ± 0.58 | 74.7 | 0.16–4.26 | 1.02 ± 0.53 | 60 | 0.17–2.84 | 0.003 ** |
| Ca (mg) | 1200 | 602.1 ± 378.3 | 50.2 | 33.5–2788.4 | 660.8 ± 379.6 | 55.1 | 81.3–2788.4 | 492.5 ± 353 | 41 | 33.5–1530.9 | <0.001 *** |
| Mg (mg) | 400 | 300.4 ± 164.5 | 75.1 | 77.9–1202.8 | 311.5 ± 160.9 | 77.9 | 97.5–1127.6 | 279.8 ± 170.4 | 70 | 77.9–1202.8 | 0.069 ns |
| Fe (mg) | 35 | 18.7 ± 9.8 | 53.4 | 5.2–88.9 | 19.7 ± 10.4 | 56.3 | 5.2–88.9 | 16.8 ± 8.3 | 48 | 6.2–58.2 | 0.019 * |
| Zn (mg) | 16.5 | 11.2 ± 4.7 | 67.9 | 3.5–32.6 | 11.7 ± 4.8 | 70.9 | 4.3–32.6 | 10.2 ± 4.5 | 61.8 | 3.5–28 | 0.025 * |
3.3.2. Food Groups and Sources of Energy and Nutrients
| Amount (g/day) | In total | Urban | Rural | p-Value 1 |
|---|---|---|---|---|
| (n = 192) | (n = 125) | (n = 67) | ||
| Rice/its products | 178.4 ± 94.5 | 176.6 ± 105.1 | 181.9 ± 71.2 | 0.101 ns |
| Wheat and other grains/their products | 57.5 ± 133.5 | 57.6 ± 93.2 | 57.4 ± 187.8 | 0.053 ns |
| Starchy tubers, roots | 30.6 ± 63.2 | 32.4 ± 66.8 | 27.3 ± 56.1 | 0.911 ns |
| Soy products | 56.1 ± 138.4 | 65.3 ± 151.6 | 38.9 ± 108.6 | 0.459 ns |
| Soya sauce and bean paste | 6.9 ± 6.2 | 7.4 ± 6.4 | 6.0 ± 5.7 | 0.123 ns |
| Vegetables | 164.7 ± 170.4 | 183.7 ± 186.9 | 129.3 ± 128.4 | 0.042 * |
| Preserved vegetables | 11.7 ± 52.4 | 15.6 ± 64.1 | 4.4 ± 12.2 | 0.083 ns |
| Fruits | 517.1 ± 626.3 | 498.6 ± 619.2 | 551.6 ± 642.6 | 0.332 ns |
| Nuts and seeds | 26.8 ± 52.0 | 29.0 ± 51.8 | 22.6 ± 52.6 | 0.202 ns |
| Pork | 100.8 ± 105.1 | 100.7 ± 96.5 | 101.0 ± 120.4 | 0.567 ns |
| Other meats/poultry/offal | 37.0 ± 58.8 | 41.0 ± 62.7 | 29.5 ± 50.4 | 0.120 ns |
| Cow’s milk | 147.3 ± 196.3 | 172.9 ± 203.9 | 99.5 ± 172.7 | 0.012 * |
| Chicken eggs | 55.0 ± 58.1 | 51.5 ± 53.6 | 61.7 ± 65.5 | 0.624 ns |
| Seafood | 16.8 ± 42.9 | 22.4 ± 50.2 | 6.4 ± 20.8 | 0.006 ** |
| Vegetable oil | 44.4 ± 37.0 | 49.2 ± 39.2 | 35.5 ± 30.7 | 0.016 * |
| Animal fats | 1.2 ± 4.8 | 1.6 ± 5.8 | 0.3 ± 1.9 | 0.026 * |
4. Discussion
4.1. Food Taboos and Special Foods Consumed during Pregnancy in Rural and Urban Areas
4.2. Dietary and Food Intake Patterns
4.2.1. Dietary Intake in Rural and Urban Areas
4.2.2. Food Group Consumption in Rural and Urban Area
4.2.3. Comparison of Dietary Patterns with Related Studies
| Food group (g/day) | 2002 NNHS
National level China Pregnant women (n = 310) (whole pregnancy period) | Deyang, 2010
Urban and rural areas Pregnant women (n = 192) (3rd trimester) | Recommendation
(Yang [51], 2008) | |||
|---|---|---|---|---|---|---|
| In Total
(n = 192) | Urban
(n = 125) | Rural
(n = 67) | p-Value 1 | |||
| Staples | 461 | 266.6 ± 179.4 | 266.6 ± 159.4 | 266.6 ± 213.1 | 0.882 ns | 250–400 |
| Soy products | 13 | 63.0 ± 138.6 | 72.7 ± 151.8 | 44.9 ± 108.5 | 0.114 ns | 30–50 |
| Vegetables | 285 | 176.4 ± 174.1 | 199.3 ± 190.8 | 133.8 ± 128.1 | 0.010 ** | 300–340 |
| Fruits | 81 | 517.1 ± 626.3 | 498.6 ± 619.2 | 551.6 ± 642.6 | 0.332 ns | 200–400 |
| Meats, fish | 96 | 154.6 ± 123.9 | 164.0 ± 124.3 | 137.0 ± 122.2 | 0.061 ns | 125–225 |
| Milk, dairy products | 19 | 158.7 ± 198.7 | 186.5 ± 207.0 | 106.9 ± 172.0 | 0.006 ** | 300 |
| Chicken eggs | 25 | 55.0 ± 58.1 | 51.5 ± 53.6 | 61.7 ± 65.5 | 0.624 ns | - • |
| Vegetable oil | 31 | 44.4 ± 37.0 | 49.2 ± 39.2 | 35.5 ± 30.7 | 0.016 * | 25 |
| NNHS
National level China Covering individuals of all ages | Deyang, 2010
Urban and rural areas Pregnant women (3rd trimester) | |||
|---|---|---|---|---|
| Food group (g/day) | 1982 | 1992 | 2002 | 2010 |
| Grains/its products | 510 | 440 | 402 | 236 |
| Vegetable & fruit | 368 | 369 | 331 | 724 |
| Animal sources | 61 | 117 | 160 | 368 |
| Visible oil and fat | 18 | 30 | 41 | 46 |
4.3. Recommendations to Improve Dietary Quality
4.3.1. Improving Nutrient Density of the Diet in Rural and Urban Areas
4.3.2. Improving the Intake of Micronutrients in Rural and Urban Area
4.4. Limitations of This Study
5. Conclusions
Acknowledgments
Conflict of Interest
References
- Nestlé Started Clinical Nutrition Management Project, 500,000 Pediatric Patients will Benefit from It. (in Chinese). Available online: http://shipin.people.com.cn/GB/17484602.html (accessed on 25 April 2012).
- UNICEF, Joint Review of Maternal and Child Survival Strategies in China; United Nations Children’s Fund: Beijing, China, 2006.
- Kruger, H.S. Maternal anthropometry and pregnancy outcomes: A proposal for the monitoring of pregnancy weight gain in outpatient clinics in South Africa. Curationis 2005, 28, 40–49. [Google Scholar] [CrossRef]
- Christian, P.; Stewart, C.P. Maternal micronutrient deficiency, fetal development, and the risk of chronic disease. J. Nutr. 2010, 13, 437–445. [Google Scholar]
- Ensuring Effective Caring Practices within the Family and Community. Available online: http://www.adeanet.org/adeaPortal/adea/biennial-2006/doc/document/C2_1_jallow_en.pdf (accessed on 20 March 2013).
- Aaltonen, J.; Ojala, T.; Laitinen, K.; Poussa, T.; Ozanne, S.; Isolauri, E. Impact of maternal diet during pregnancy and breastfeeding on infant metabolic programming: A prospective randomized controlled study. Eur. J. Clin. Nutr. 2011, 65, 10–19. [Google Scholar] [CrossRef]
- Chinese Nutrition Society. Monitoring of Nutrition and Health Status of Chinese Residents—Result of Maternal Monitoring in Many Big Cities in 2010. (in Chinese). In Proceedings of the Seminar for Reprinted Dietary Guidelines for Women and Children and Balanced Diet Pagoda Publicity Evaluation, Infant National Food Safety Standards, Xinglong, China, 01 December 2011.
- Yin, X.C.; Yin, S.A.; Hu, Y.M. Impact of Zn supplementation on the nutritional and health status of women at reproductive age. (in Chinese). J. Hyg. Res. 2011, 4, 391–396. [Google Scholar]
- Liu, L.; Kang, M.; Qing, P. Dietary and nutritional status of pregnant women in Chengdu. (in Chinese). J. Prev. Med. Inf. 2007, 23, 177–180. [Google Scholar]
- Ding, Z.M.; Wang, M.Z. Nutrition survey of pregnant women in the 2nd and 3rd trimester. (in Chinese). China Matern. Child Health 2004, 19, 21–22. [Google Scholar]
- Ministry of Health of China. Nutrition and Health Status of Chinese Residents. (in Chinese). 2004. Available online: http://news3.xinhuanet.com/forum/2004-10/12/content_2087980.htm (accessed on 23 July 2013).
- Zhong, D.H.; Liu, C.H.; Su, S.P. Dietary analysis and nutritional status of pregnant women in China. (in Chinese). Today Nurse 2010, 4, 28–30. [Google Scholar]
- Zhou, L.; Liu, X.H.; Hu, X.Y. Investigation and intervention on anemia in healthy pregnant women in Chengdu. (in Chinese). Chin. J. Obstet. Gynecol. Pediatr. 2010, 6, 93–95. [Google Scholar]
- World Health Organization, Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; World Health Organization: Geneva, Switzerland, 2011.
- Liu, Y.Y.; Dai, W.; Dai, X.Q.; Li, Z. Prepregnancy body mass index and gestational weight gain with the outcome of pregnancy: A 13-year study of 292,568 cases in China. Arch. Gynecol. Obstet. 2012, 286, 905–911. [Google Scholar] [CrossRef]
- Levy, A.; Fraser, D.; Katz, M.; Mazor, M.; Sheiner, E. Maternal anemia during pregnancy is an independent risk factor for low birthweight and preterm delivery. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 122, 182–186. [Google Scholar] [CrossRef]
- Wang, J.; Zhao, L.Y.; Tiao, J.H.; Zhang, J.; Yang, X.G.; Luo, J.; Yin, S.A. Nutrition and developmet status of neonate in 16 counties in 8 provinces in China. (in Chinese). J. Hyg. Res. 2011, 2, 67–70. [Google Scholar]
- The Double Burden of Malnutrition. Case Studies from Six Developing Countries. Available online: ftp://ftp.fao.org/docrep/fao/009/a0442e/a0442e00.pdf (accessed on 23 July 2013).
- Diet, Nutrition and the Prevention of Chronic Diseases. Report of the Joint WHO/FAO Expert Consultation. Available online: http://www.who.int/dietphysicalactivity/publications/trs916/download/en/ (accessed on 23 July 2013).
- Ge, K. The status and trends of obesity in China. Int. J. Vitam. Nutr. Res. 2006, 76, 247–252. [Google Scholar] [CrossRef]
- Qu, J.B.; Zhang, Z.W.; Shimbo, S.; Liu, Z.M.; Cai, X.C.; Wang, L.Q.; Watanabe, T.; Nakatsuka, H.; Matsuda-Inoguchi, N.; Higashikawa, K.E.A. Nutrient intake of adult women in Jilin province, China, with special reference to urban-rural differences in nutrition in the Chinese continent. Eur. J. Clin. Nutr. 2000, 54, 741–748. [Google Scholar] [CrossRef]
- Tian, H.G.; Nan, Y.; Hu, G.; Dong, Q.N.; Yang, X.L. A dietary survey of the Chinese population in urban and rural areas of Tianjin. Asia Pac. J. Clin. Nutr. 1996, 5, 229–234. [Google Scholar]
- Gao, H.Y. Assessment of Infant Feeding Policies and Practice in Deyang City, Sichuan Province, China; University of Hohenheim: Stuttgart, Germany, 2008. [Google Scholar]
- Qu, S.Z. Nutrition and Health Aspects of Infants and Women during the Reproductive Period in Rural and Urban Areas of Deyang City, China; University of Hohenheim: Stuttgart, Germany, 2009. [Google Scholar]
- Lee, D.T.; Ngai, I.S.; Ng, M.M.; Lok, I.H.; Yip, A.S.; Chung, T.K. Antenatal taboos among Chinese women in Hong Kong. Midwifery 2009, 25, 104–113. [Google Scholar] [CrossRef]
- Children in an Urban World. The State of the World’s Children 2012. Available online: http://www.unicef.org/sowc2012/ (accessed on 23 July 2013).
- Lefèber, Y.; Voorhoeve, H.W.A. Indigenous Customs in Childbirth and Child Care; Van Gorcum: Assen, The Netherlands, 1998; p. 103. [Google Scholar]
- Ververs, M.T. Supplementation Programs for Pregnant and Lactating Women. Available online: http://fex.ennonline.net/7/supplementation (accessed on 23 July 2013).
- Husaini, M.A.; Husaini, Y.K.; Sandjaja, D.K.; Jahari, A.B.; Karyadi, D. Annex: Maternal anthropometry and pregnancy outcomes in Indonesia. Bull. World Health Organ. 1995, 73, 77–79. [Google Scholar]
- Liljestrand, J.; Bergström, S. Antenatal nutritional assessment: The value of upper arm circumference. Gynecol. Obstet. Investig. 1991, 32, 81–83. [Google Scholar] [CrossRef]
- Karim, E.; Mascie-Taylor, C.G. The association between birth weight, sociodemographic variable and maternal anthropometry in an urban sample from Dhaka, Bangladesh. Ann. Hum. Biol. 1997, 24, 387–401. [Google Scholar] [CrossRef]
- Olukoya, A.A. Identification of underweight women by measurement of the arm circumference. Int. J. Gynecol. Obstet. 1990, 31, 231–235. [Google Scholar] [CrossRef]
- Neumann, C.; Ferguson, L.; Bwibo, N.O. Annex: Maternal anthropometry as a risk predictor of pregnancy outcome: The nutrition CRSP in Kenya. Bull. World Health Organ. 1995, 73, 91–95. [Google Scholar]
- Maternal anthropometry and pregnancy outcomes. A WHO Collaborative Study. Bull. World Health Organ. 1995, 73, 1–98.
- UNHCR/WFP. Guidelines for Selective Feeding Programs in Emergency Situations. Available online: http://www.unsystem.org/scn/archives/rnis26/ch7.htm (accessed on 15 March 2013).
- James, W.P.T.; Mascie-Taylor, G.C.B.; Norgan, N.G.; Bistrian, B.R.; Shetty, P.S.; Ferro-Luzzi, A. The value of arm circumference measurements in assessing chronic energy deficiency in third world adults. Eur. J. Clin. Nutr. 1994, 48, 883–894. [Google Scholar]
- World Health Organization, The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; World Health Organization: Geneva, Switerzland, 2000.
- Jiang, H.; Qian, X.; Li, M.; Lynn, H.; Fan, Y.; Jiang, H.; He, F.; He, G. Can physical activity reduce excessive gestational weight gain? Findings from a Chinese urban pregnant women cohort study. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 12. [Google Scholar] [CrossRef]
- Institute of Nutrition and Food Safety, China, China Food Composition Table 2002 (Book 1), 2nd ed.; Peking University Medical Press: Beijing, China, 2002.
- Institute of Nutrition and Food Safety, China, China Food Composition Table 2004 (Book 2); Peking University Medical Press: Beijing, China, 2004.
- DGE. DGE-statement: Vitamin Supply in Germany. (in German). Available online: http://www.dge.de/modules.php?name=News&file=print&sid=344 (accessed on 10 January 2013).
- Chen, Y.C. Chinese values, health and nursing. J. Adv. Nurs. 2001, 36, 270–273. [Google Scholar] [CrossRef]
- Food in Chinese Culture: Anthropological and Historical Perspectives; Chang, K.C. (Ed.) Yale University Press: New Haven, CT, USA, 1977; p. 9.
- Tung, W.C. Doing the month and Asian cultures: Implications for health care. Home Health Care Manag. Pract. 2010, 22, 369–371. [Google Scholar] [CrossRef]
- Raven, J.H.; Chen, Q.; Tolhurst, R.J.; Garner, P. Traditional beliefs and practices in the postpartum period in Fujian province, China: A qualitative study. BMC Pregnancy Childbirth 2007, 7, 8. [Google Scholar] [CrossRef]
- Notes on Food in Nutrition and Health in Traditional China. In Food in China: A Cultural and Historical Inquiry; Simoons, F.J. (Ed.) CRC Press: Boston, MA, USA, 1991; pp. 469–515.
- Institute of Medicine of the National Academies, Appendix: Applications of Dietary Reference Intakes for Macronutrients. In IOM, Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; National Academy Press: Washington, DC, USA, 2005.
- Uncertainties Associated with Energy and Protein. In Principles of Nutritional Assessment, 2nd ed.; Gibson, R.S. (Ed.) Oxford University Press: New York, NY, USA, 1990; pp. 81–83.
- Wang, Z.; Dang, S.; Yan, H. Nutrient intakes of rural Tibetan mothers: A cross-sectional survey. Public Health Nutr. 2010, 10, 801. [Google Scholar]
- Nutrition and Health Data of Women in Reproductive Age, Pregnant Women, and of Women in Lactation, No. 11. (in Chinese). In China National Nutrition and Health Survey 2002; People’s Medical Publishing House: Beijing, China, 2009; p. 68.
- Yang, Y.X. Chapter 2. In A Practical Guidance for Designing Dietary Advice and Dietary Evaluation; (in Chinese). People’s Medical Publishing House: Beijing, China, 2008. [Google Scholar]
- Drewnowski, A. Concept of a nutritious food: Toward a nutrient density score. Am. J. Clin. Nutr. 2005, 82, 721–732. [Google Scholar]
- Michaelsen, K.F.; Weaver, L.; Branca, F.; Robertson, A. Feeding and Nutrition of Infants and Young Children: Guidelines of the WHO European Region with Emphasis on the Former Soviet Countries; World Health Organization: Geneva, Switerzland, 2003. [Google Scholar]
- Cheng, Y.; Dibley, M.J.; Zhang, X.; Zeng, L.; Yan, H. Assessment of dietary intake among pregnant women in a rural area of Western China. Public Health Nutr. 2009, 9, 222. [Google Scholar]
- Du, S.; Mroz, T.A.; Zhai, F.; Popkin, B.M. Rapid income growth adversely affects diet quality in China-particularly for the poor! J. Soc. Sci. Med. 2004, 59, 1505–1515. [Google Scholar] [CrossRef]
- Biesalski, H.K.; Grimm, P. Pocket Guide of Nutrition(in German), 4th ed.; Thieme: Stuttgart, Germany, 2007. [Google Scholar]
- Fiebig, H.J. Fatty Acid Composition of Important Plant- and Animal-Based Fats-Oils. (in German). Available online: http://www.dgfett.de/material/fszus.php (accessed on 16 April 2012).
- Ma, G.; Jin, Y.; Li, Y.; Zhai, F.; Kok, F.J. Fe and Zn deficiencies in China: What is a feasible and cost-effective strategy? Public Health Nutr. 2007, 11, 632–638. [Google Scholar]
- Xiu, C.; Klein, K.K. Melamine in milk products in China: Examining the factors that led to deliberate use of the contaminant. Food Policy 2010, 35, 463–470. [Google Scholar] [CrossRef]
- Li, J.R.; Hsieh, Y.H.P. Traditional Chinese food technology and cuisine. Asia Pac. J. Clin. Nutr. 2004, 13, 147–155. [Google Scholar]
- Weaver, C.M.; Heaney, R.P.; Connor, L.; Martin, B.R.; Smith, D.L.; Nielson, S. Bioavailability of Ca from tofu as compared with milk in premenopausal women. J. Food Sci. 2002, 67, 3144–3147. [Google Scholar] [CrossRef]
- Lu, E. Radical Shifts in China’s Milk Market. Available online: http://china.org.cn/business/news/2009-01/14/content_17105973.htm (accessed on 23 July 2013).
- Ge, K.Y.; Chang, S.Y. Dietary intake of some essential micronutrients in China. Biomed. Environ. Sci. 2001, 14, 318–324. [Google Scholar]
- Institute of Medicine of the National Academies, Dietary Reference Intakes: Applications in Dietary Assessment; National Academy of Sciences: Washington, DC, USA, 2000.
- Measuring Food Consumption of Individuals. In Principles of Nutritional Assessment; Gibson, R.S. (Ed.) Oxford University Press: New York, NY, USA, 2005.
- Institute of Medicine of the National Academies, Energy. In Dietary Reference Intakes for Energy, Carbohydrates, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; National Academy Press: Washington, DC, USA, 2005.
- Johnson, R.K.; Soultanakis, R.P.; Matthews, D.E. Literacy and body fatness are associated with underreporting of energy intakes in US low-income women using the multiple-pass 24-hour recall: A doubly labeled water study. J. Am. Diet. Assoc. 1998, 98, 1136–1140. [Google Scholar] [CrossRef]
- Thompson, F.E.; Byers, T. Dietary assessment resource manual. J. Nutr. 1994, 124, 2245S–2317S. [Google Scholar]
- MacIntyre, U.E. Measuring Food Intake. In Introduction to Human Nutrition, 2nd ed.; Gibney, M.J., Lanham-New, S.A., Cassidy, A., Vorster, H.H., Eds.; Wiley-Blackwell: Chichester, England, 2009. [Google Scholar]
- Allen, L.H. Harmonizing Micronutrient Recommendations World-Wide. Available online: https://ew.uni-hohenheim.de/fileadmin/einrichtungen/hiddenhunger/Praesis_Mittwoch/Allen_2013_03_06.pdf (accessed on 05 May 2013).
- Block, G. Human dietary assessment: Methods and issues. Prev. Med. 1989, 18, 653–660. [Google Scholar] [CrossRef]
- Guenther, P.M.; Kott, P.S.; Carriquiry, A.L. Development of an approach for estimating usual nutrient intake distributions at the population level. J. Nutr. 1997, 127, 1106–1112. [Google Scholar]
- Popkin, B.M.; Lu, B.; Zhai, F. Part G. Advances in methodological issues in the use of international food datasets. Understanding the nutrition transition: Measuring rapid dietary changes in transitional countries. Public Health Nutr. 2002, 5, 947–953. [Google Scholar] [CrossRef]
- Ministry of Health, People’s Republic of China. Background Paper for the High-Level Meeting on Child Rights, Beijing, November 4–6, 2010. Progress towards Achieving the Millennium Development Goal 4 and 5 Targets on Child and Maternal Mortality in China, with Equity. Available online: http://www.unicef.org/eapro/Background_paper_on_achieving_MDGs_4_5_with_equity_-_MoH_China_FINAL.pdf (accessed on 10 May 2013).
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Gao, H.; Stiller, C.K.; Scherbaum, V.; Biesalski, H.K.; Wang, Q.; Hormann, E.; Bellows, A.C. Dietary Intake and Food Habits of Pregnant Women Residing in Urban and Rural Areas of Deyang City, Sichuan Province, China. Nutrients 2013, 5, 2933-2954. https://doi.org/10.3390/nu5082933
Gao H, Stiller CK, Scherbaum V, Biesalski HK, Wang Q, Hormann E, Bellows AC. Dietary Intake and Food Habits of Pregnant Women Residing in Urban and Rural Areas of Deyang City, Sichuan Province, China. Nutrients. 2013; 5(8):2933-2954. https://doi.org/10.3390/nu5082933
Chicago/Turabian StyleGao, Haoyue, Caroline K. Stiller, Veronika Scherbaum, Hans Konrad Biesalski, Qi Wang, Elizabeth Hormann, and Anne C. Bellows. 2013. "Dietary Intake and Food Habits of Pregnant Women Residing in Urban and Rural Areas of Deyang City, Sichuan Province, China" Nutrients 5, no. 8: 2933-2954. https://doi.org/10.3390/nu5082933
APA StyleGao, H., Stiller, C. K., Scherbaum, V., Biesalski, H. K., Wang, Q., Hormann, E., & Bellows, A. C. (2013). Dietary Intake and Food Habits of Pregnant Women Residing in Urban and Rural Areas of Deyang City, Sichuan Province, China. Nutrients, 5(8), 2933-2954. https://doi.org/10.3390/nu5082933