
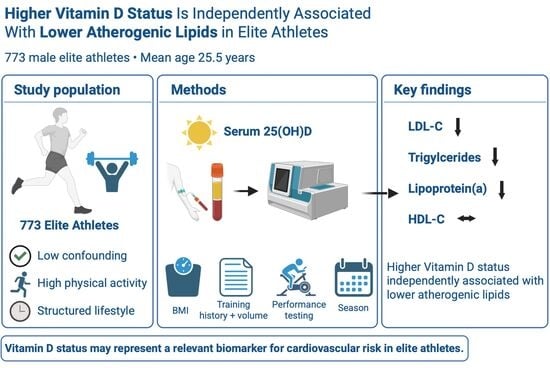
Vitamin D Status and Atherogenic Lipid Profiles, Including Lipoprotein(a), in Elite Athletes

 , , and
, , and
Abstract
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Eligibility Criteria and Clinical Assessment
2.3. Study Population Characteristics
2.4. Laboratory Analyses
2.5. Training-Related Variables
2.6. Statistical Analysis
3. Results
3.1. Study Population and Vitamin D Status
3.2. Group Differences According to Vitamin D Status
3.3. Univariate Correlations Between Serum 25(OH)D and Clinical Parameters
3.4. Multivariable Regression Analyses
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ao, T.; Kikuta, J.; Ishii, M. The Effects of Vitamin D on Immune System and Inflammatory Diseases. Biomolecules 2021, 11, 1624. [Google Scholar] [CrossRef] [PubMed]
- Aranow, C. Vitamin D and the Immune System. J. Investig. Med. 2011, 59, 881–886. [Google Scholar] [CrossRef] [PubMed]
- Al Mheid, I.; Patel, R.S.; Tangpricha, V.; Quyyumi, A.A. Vitamin D and cardiovascular disease: Is the evidence solid? Eur. Heart J. 2013, 34, 3691–3698. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, W.; Yang, Y.; Deng, J.; Zhang, Z. Vitamin D and bone health: From physiological function to disease association. Nutr. Metab. 2025, 22, 113. [Google Scholar] [CrossRef] [PubMed]
- de La Puente Yagüe, M.; Collado Yurrita, L.; Ciudad Cabañas, M.J.; Cuadrado Cenzual, M.A. Role of Vitamin D in Athletes and Their Performance: Current Concepts and New Trends. Nutrients 2020, 12, 579. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Yang, Y.; Jiang, Y.; Zhou, Z.; Zhang, J. Association between vitamin D deficiency and lipid profiles in overweight and obese adults: A systematic review and meta-analysis. BMC Public Health 2023, 23, 1653. [Google Scholar] [CrossRef] [PubMed]
- Cai, M.; Jiang, X.; Xu, X.; Zhao, S.; Sun, Y.; Yang, Y.; Gu, Y.; Huang, Y. Associations of vitamin D with lipid metabolism, inflammation, and mortality vary by glycemic status and gender: A nationwide prospective study. Front. Nutr. 2025, 12, 1597527. [Google Scholar] [CrossRef] [PubMed]
- Gholamzad, A.; Khakpour, N.; Kabipour, T.; Gholamzad, M. Association between serum vitamin D levels and lipid profiles: A cross-sectional analysis. Sci. Rep. 2023, 13, 21058. [Google Scholar] [CrossRef] [PubMed]
- Lupton, J.R.; Faridi, K.F.; Martin, S.S.; Sharma, S.; Kulkarni, K.; Jones, S.R.; Michos, E.D. Deficient serum 25-hydroxyvitamin D is associated with an atherogenic lipid profile: The Very Large Database of Lipids (VLDL-3) study. J. Clin. Lipidol. 2016, 10, 72–81.e1. [Google Scholar] [CrossRef] [PubMed]
- Kronenberg, F.; Mora, S.; Stroes, E.S.G.; A Ference, B.; Arsenault, B.J.; Berglund, L.; Dweck, M.R.; Koschinsky, M.; Lambert, G.; Mach, F.; et al. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: A European Atherosclerosis Society consensus statement. Eur. Heart J. 2022, 43, 3925–3946. [Google Scholar] [CrossRef] [PubMed]
- Thanassoulis, G.; Anand, S.; Arsenault, B.J.; Bainey, K.R.; Bell, A.D.; Brunham, L.R.; Iatan, I.; Koschinsky, M.L.; Leiter, L.A.; Mehta, S.R.; et al. Clinical Care for Patients with Elevated Lipoprotein(a) Level in Canada: A Practical Framework for Screening, Risk Assessment, and Management. Can. J. Cardiol. 2026, 42, 867–884. [Google Scholar] [CrossRef] [PubMed]
- Surdu, A.M.; Pînzariu, O.; Ciobanu, D.-M.; Negru, A.-G.; Căinap, S.-S.; Lazea, C.; Iacob, D.; Săraci, G.; Tirinescu, D.; Borda, I.M.; et al. Vitamin D and Its Role in the lipid metabolism and the development of atherosclerosis. Biomedicines 2021, 9, 172. [Google Scholar] [CrossRef] [PubMed]
- Radkhah, N.; Zarezadeh, M.; Jamilian, P.; Ostadrahimi, A. The Effect of Vitamin D Supplementation on Lipid Profiles: An Umbrella Review of Meta-Analyses. Adv. Nutr. 2023, 14, 1479–1498. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Liang, Q.; Xi, Y. The effects of vitamin D supplementation on serum lipid profiles in people with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Front. Nutr. 2024, 11, 1419747. [Google Scholar] [CrossRef] [PubMed]
- Schwetz, V.; Scharnagl, H.; Trummer, C.; Stojakovic, T.; Pandis, M.; Grübler, M.R.; Verheyen, N.; Gaksch, M.; Zittermann, A.; Aberer, F.; et al. Vitamin D supplementation and lipoprotein metabolism: A randomized controlled trial. J. Clin. Lipidol. 2018, 12, 588–596.e4. [Google Scholar] [CrossRef] [PubMed]
- Mba, C.M.; Koulman, A.; Forouhi, N.G.; Sharp, S.J.; Imamura, F.; Jones, K.; Meadows, S.R.; Assah, F.; Mbanya, J.C.; Wareham, N.J. Association between circulating 25-hydroxyvitamin D and cardiometabolic risk factors in adults in rural and urban settings. Nutr. Diabetes 2022, 12, 34. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.; Kwon, O.; Kim, J. Vitamin D in athletes: Focus on physical performance and musculoskeletal injuries. Phys. Act. Nutr. 2021, 25, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Ference, B.A.; Braunwald, E.; Catapano, A.L. The LDL cumulative exposure hypothesis: Evidence and practical applications. Nat. Rev. Cardiol. 2024, 21, 701–716. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Giovannucci, E.; Willett, W.C.; Dietrich, T.; Dawson-Hughes, B. Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am. J. Clin. Nutr. 2006, 84, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Bauer, P.; Kraushaar, L.; Dörr, O.; Bauer, T.; Nef, H.; Hamm, C.W.; Most, A. Association of 25-hydroxy vitamin D level with the blood pressure response to a maximum exercise test among professional indoor athletes. Eur. J. Appl. Physiol. 2020, 120, 1931–1941. [Google Scholar] [CrossRef] [PubMed]
- Bauer, P.; Kraushaar, L.; Hölscher, S.; Tajmiri-Gondai, S.; Dörr, O.; Nef, H.; Hamm, C.; Most, A. Elite athletes as research model: Vitamin D insufficiency associates with elevated central blood pressure in professional handball athletes. Eur. J. Appl. Physiol. 2019, 119, 2265–2274. [Google Scholar] [CrossRef] [PubMed]
- Bauer, P.; Henni, S.; Dörr, O.; Bauer, T.; Hamm, C.W.; Most, A. High prevalence of vitamin D insufficiency in professional handball athletes. Physician Sportsmed. 2019, 47, 71–77. [Google Scholar] [CrossRef]
- Owens, D.J.; Allison, R.; Close, G.L. Vitamin D and the Athlete: Current Perspectives and New Challenges. Sports Med. 2018, 48, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Pludowski, P.; Holick, M.F.; Grant, W.B.; Konstantynowicz, J.; Mascarenhas, M.R.; Haq, A.; Povoroznyuk, V.; Balatska, N.; Barbosa, A.P.; Karonova, T.; et al. Vitamin D supplementation guidelines. J. Steroid Biochem. Mol. Biol. 2018, 175, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Grant, W.B.; Boucher, B.J.; Cheng, R.Z.; Pludowski, P.; Wimalawansa, S.J. Vitamin D and Cardiovascular Health: A Narrative Review of Risk Reduction Evidence. Nutrients 2025, 17, 2102. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rodríguez, E.; Ortega, R.M.; González-Rodríguez, L.G.; López-Sobaler, A.M. Vitamin D deficiency is an independent predictor of elevated triglycerides in Spanish school children. Eur. J. Nutr. 2011, 50, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.-P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef] [PubMed]
- Carbone, F.; Liberale, L.; Libby, P.; Montecucco, F. Vitamin D in atherosclerosis and cardiovascular events. Eur. Heart J. 2023, 44, 2078–2094. [Google Scholar] [CrossRef] [PubMed]
- Melguizo-Rodríguez, L.; Costela-Ruiz, V.J.; García-Recio, E.; De Luna-Bertos, E.; Ruiz, C.; Illescas-Montes, R. Role of Vitamin D in the Metabolic Syndrome. Nutrients 2021, 13, 830. [Google Scholar] [CrossRef] [PubMed]
- Hagström, E.; Hellman, P.; Larsson, T.E.; Ingelsson, E.; Berglund, L.; Sundström, J.; Melhus, H.; Held, C.; Lind, L.; Michaëlsson, K.; et al. Plasma Parathyroid Hormone and the Risk of Cardiovascular Mortality in the Community. Circulation 2009, 119, 2765–2771. [Google Scholar] [CrossRef] [PubMed]
- Claessen, G.; Eijsvogels, T.M.H.; Albert, C.M.; Baggish, A.L.; Levine, B.D.; Marijon, E.; Michos, E.D.; La Gerche, A. Coronary atherosclerosis in athletes: Emerging concepts and preventive strategies. Eur. Heart J. 2025, 46, 890–903. [Google Scholar] [CrossRef] [PubMed]
- D’aScenzi, F.; Caselli, S.; Alvino, F.; Digiacinto, B.; Lemme, E.; Piepoli, M.; Pelliccia, A. Cardiovascular risk profile in Olympic athletes: An unexpected and underestimated risk scenario. Br. J. Sports Med. 2019, 53, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Molani-Gol, R.; Rafraf, M.; Safari, S. Effects of vitamin D supplementation on metabolic parameters, anthropometric measures, and diabetes risk in patients with prediabetes: An umbrella review of meta-analyses of randomized controlled trials. Nutr. Metab. 2025, 22, 99. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Sena, T.; Soluyanova, P.; Guzmán, C.; Valdivielso, J.M.; Castell, J.V.; Jover, R. The Vitamin D Receptor Regulates Glycerolipid and Phospholipid Metabolism in Human Hepatocytes. Biomolecules 2020, 10, 493. [Google Scholar] [CrossRef] [PubMed]
- Hoseini, R.; Damirchi, A.; Babaei, P. Vitamin D increases PPARγ expression and promotes beneficial effects of physical activity in metabolic syndrome. Nutrition 2017, 36, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Dibaba, D.T. Effect of vitamin D supplementation on serum lipid profiles: A systematic review and meta-analysis. Nutr. Rev. 2019, 77, 890–902. [Google Scholar] [CrossRef] [PubMed]
- Most, A.; Dörr, O.; Nef, H.; Hamm, C.; Bauer, T.; Bauer, P. Influence of 25-Hydroxy-Vitamin D Insufficiency on Maximal Aerobic Power in Elite Indoor Athletes: A Cross-Sectional Study. Sports Med.-Open 2021, 7, 74. [Google Scholar] [CrossRef] [PubMed]
- Książek, A.; Zagrodna, A.; Słowińska-Lisowska, M. Vitamin D, Skeletal Muscle Function and Athletic Performance in Athletes—A Narrative Review. Nutrients 2019, 11, 1800. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Mean ± SD/Median (IQR) | n | |
|---|---|---|
| Age (years) | 25.54 ± 4.97 | 773 |
| BMI (kg/m2) | 25.50 ± 2.08 | 773 |
| 25(OH)D (ng/mL) | 34.25 ± 14.19 | 773 |
| Total cholesterol (mg/dL) | 162.61 ± 30.48 | 713 |
| LDL cholesterol (mg/dL) | 97.65 ± 29.27 | 773 |
| HDL cholesterol (mg/dL) | 50.19 ± 10.68 | 773 |
| Triglycerides (mg/dL) | 99.73 ± 54.86 | 712 |
| Lipoprotein(a) (mg/dL) | 1.00 (0.00–24.00) | 773 |
| HbA1c (%) | 5.24 ± 0.26 | 773 |
| CRP (mg/L) | 0.67 ± 2.07 | 773 |
| Training volume (min/week) | 1150.96 ± 235.77 | 764 |
| Training history (years) | 8.62 ± 5.05 | 764 |
| Peak performance (watts/kg) | 3.93 ± 1.08 | 773 |
| 25(OH)D < 30 ng/mL (n = 296) | 25(OH)D ≥ 30 ng/mL (n = 477) | p | |
|---|---|---|---|
| Age (years) | 25.35 ± 5.03 | 25.62 ± 4.97 | 0.473 |
| BMI (kg/m2) | 25.54 ± 2.20 | 25.47 ± 2.00 | 0.649 |
| 25(OH)D (ng/mL) | 21.36 ± 6.54 | 42.25 ± 11.51 | <0.001 * |
| Total cholesterol (mg/dL) | 165.33 ± 32.00 | 160.76 ± 29.48 | 0.052 |
| LDL cholesterol (mg/dL) | 101.06 ± 31.22 | 95.08 ± 27.77 | 0.006 * |
| HDL cholesterol (mg/dL) | 50.15 ± 11.94 | 50.10 ± 9.83 | 0.953 |
| Triglycerides (mg/dL) | 105.96 ± 64.52 | 96.11 ± 47.69 | 0.020 * |
| Lipoprotein(a) (mg/dL) | 2.00 (1.00–39.00) | 1.00 (0.00–23.00) | 0.003 |
| HbA1c (%) | 5.26 ± 0.25 | 5.22 ± 0.26 | 0.057 |
| CRP (mg/L) | 0.622 ± 2.00 | 0.70 ± 2.13 | 0.610 |
| Calcium (mmol/L) | 2.34 ± 0.12 | 2.36 ± 0.10 | 0.010 * |
| Parathyroid hormone (pg/mL) | 40.14 ± 51.23 | 29.79 ± 15.70 | <0.001 * |
| Training volume (h/week) | 19.36 ± 4.01 | 19.16 ± 3.83 | 0.500 |
| Training history (years) | 8.25 ± 5.07 | 8.88 ± 5.04 | 0.099 |
| Peak performance (watts/kg) | 3.36 ± 0.68 | 4.29 ± 1.15 | <0.001 * |
| 25(OH)D < 30 ng/mL (n = 296) | 25(OH)D 30–50 ng/mL (n = 389) | 25(OH)D > 50 ng/mL (n = 87) | p | |
|---|---|---|---|---|
| Age (years) | 25.35 ± 5.03 | 25.59 ± 5.01 | 25.44 ± 4.50 | 0.918 |
| BMI (kg/m2) | 25.54 ± 2.20 | 25.41 ± 1.95 | 25.77 ± 2.20 | 0.296 |
| 25(OH)D (ng/mL) | 21.36 ± 6.54 | 38.33 ± 5.13 | 60.23 ± 14.48 | <0.001 * (a, b, c) |
| Total cholesterol (mg/dL) | 165.33 ± 32.00 | 160.85 ± 29.27 | 157.95 ± 26.79 | 0.037* |
| LDL cholesterol (mg/dL) | 101.06 ± 31.22 | 95.53 ± 27.69 | 91.40 ± 25.96 | 0.004 * (a, b) |
| HDL cholesterol (mg/dL) | 50.15 ± 11.94 | 49.77 ± 9.63 | 51.10 ± 10.62 | 0.542 |
| Triglycerides (mg/dL) | 105.96 ± 64.52 | 97.44 ± 47.90 | 89.15 ± 45.42 | 0.022 * (b) |
| Lipoprotein(a) (mg/dL) | 2.00 (1.00–39.00) | 1.00 (0.00–24.00) | 11.00 (0.00–22.00) | 0.047 * |
| HbA1c (%) | 5.26 ± 0.25 | 5.23 ± 0.26 | 5.18 ± 0.30 | 0.051 |
| CRP (mg/L) | 0.62 ± 2.00 | 0.64 ± 1.83 | 0.97 ± 3.16 | 0.368 |
| Calcium (mmol/L) | 2.34 ± 0.12 | 2.35 ± 0.10 | 2.39 ± 0.11 | 0.002 * (b, c) |
| Parathyroid hormone (pg/mL) | 40.14 ± 51.23 | 30.84 ± 15.77 | 25.01 ± 14.50 | <0.001 * (a, b) |
| Training volume (h/week) | 19.36 ± 4.01 | 19.03 ± 3.90 | 19.85 ± 3.39 | 0.193 |
| Training history (years) | 8.25 ± 5.07 | 8.77 ± 5.11 | 9.06 ± 4.26 | 0.407 |
| Peak performance (watts/kg) | 3.36 ± 0.68 | 4.19 ± 1.01 | 4.73 ± 1.32 | <0.001 * (a, b, c) |
| r (95–CI) | p | |
|---|---|---|
| Age (years) | 0.042 (−0.029–0.112) | 0.243 |
| BMI (kg/m2) | 0.012 (−0.058–0.083) | 0.735 |
| Total cholesterol (mg/dL) | −0.080 (−0.152–−0.006) | 0.034 * |
| LDL cholesterol (mg/dL) | −0.122 (−0.191–−0.052) | <0.001 * |
| HDL cholesterol (mg/dL) | 0.061 (−0.009–0.131) | 0.089 |
| Triglycerides (mg/dL) | −0.104 (−0.176–−0.030) | 0.006 * |
| Lipoprotein(a) (mg/dL) | −0.120 (−0.190–−0.050) | <0.001 * |
| HbA1c (%) | −0.085 (−0.155–−0.014) | 0.019 * |
| CRP (mg/L) | 0.037 (−0.033–0.108) | 0.301 |
| Calcium (mmol/L) | 0.108 (0.037–0.177) | 0.003 * |
| Parathyroid hormone (pg/mL) | −0.188 (−0.255–−0.118) | <0.001 * |
| Training volume (h/week) | 0.012 (−0.060–0.084) | 0.738 |
| Training history (years) | 0.089 (0.017–0.160) | 0.015 * |
| Peak performance (watts/kg) | 0.440 (0.381–0.495) | <0.001 * |
| Lipid Parameter | β (95–CI) per 1 ng/mL Increase in 25(OH)D | p |
|---|---|---|
| Cholesterol | −0.231 (−0.419–−0.043) | 0.016 * |
| LDL cholesterol | −0.194 (−0.368–−0.021) | 0.028 * |
| HDL cholesterol | −0.020 (−0.085–0.046) | 0.559 |
| Triglycerides | −0.568 (−0.919–−0.216) | 0.002 * |
| Lipoprotein(a) | −0.011 (−0.021–−0.001) | 0.036 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Share and Cite
Groesser, V.; Most, A.; Sedighi, J.; Böttger, P.; Sossalla, S.; Bauer, P. Vitamin D Status and Atherogenic Lipid Profiles, Including Lipoprotein(a), in Elite Athletes. Nutrients 2026, 18, 2013. https://doi.org/10.3390/nu18122013
Groesser V, Most A, Sedighi J, Böttger P, Sossalla S, Bauer P. Vitamin D Status and Atherogenic Lipid Profiles, Including Lipoprotein(a), in Elite Athletes. Nutrients. 2026; 18(12):2013. https://doi.org/10.3390/nu18122013
Chicago/Turabian StyleGroesser, Vincent, Astrid Most, Jamschid Sedighi, Priyanka Böttger, Samuel Sossalla, and Pascal Bauer. 2026. "Vitamin D Status and Atherogenic Lipid Profiles, Including Lipoprotein(a), in Elite Athletes" Nutrients 18, no. 12: 2013. https://doi.org/10.3390/nu18122013
APA StyleGroesser, V., Most, A., Sedighi, J., Böttger, P., Sossalla, S., & Bauer, P. (2026). Vitamin D Status and Atherogenic Lipid Profiles, Including Lipoprotein(a), in Elite Athletes. Nutrients, 18(12), 2013. https://doi.org/10.3390/nu18122013