
Effects of Dietary Habits on Markers of Oxidative Stress in Subjects with Hashimoto’s Thyroiditis: Comparison Between the Mediterranean Diet and a Gluten-Free Diet

 ,
,  , , ,
, , , Highlights
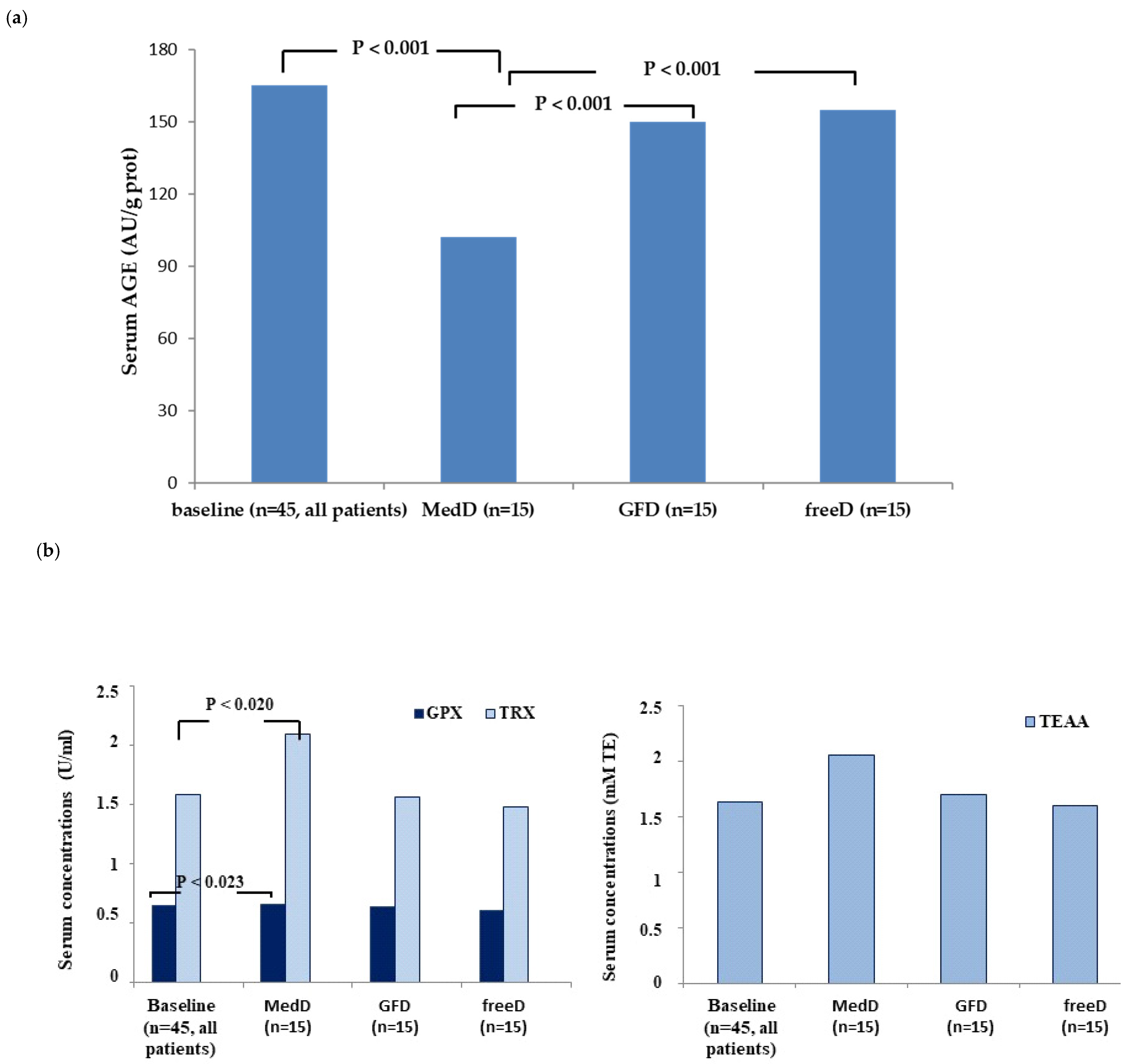
- Following the Mediterranean diet significantly improved oxidative status in patients with autoimmune thyroiditis.
- A gluten-free diet demonstrated no consistent effects on markers of oxidative stress and/or thyroid autoimmunity/function parameters in patients with chronic thyroiditis without celiac disease.
- A larger study sample, along with an evaluation of symptom relief and changes in microbiota composition, could further broaden the insights provided by these findings.
- Clinicians and patients need to be more aware of the crucial role of good nutrition, particularly that provided by the MedD, in the prevention and progression of chronic diseases.
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Methods
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Caturegli, P.; De Remigis, A.; Rose, N.R. Hashimoto thyroiditis: Clinical and diagnostic criteria. Autoimmun. Rev. 2014, 13, 391–397. [Google Scholar] [CrossRef] [PubMed]
- McLeod, D.S.; Cooper, D.S. The incidence and prevalence of thyroid autoimmunity. Endocrine 2012, 42, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.; Jeremias, P.; Matthias, T. The world incidence and prevalence of autoimmune diseases is increasing. Int. J. Coeliac. Dis. 2015, 3, 151–155. [Google Scholar] [CrossRef]
- Scherlinger, M.; Mertz, P.; Sagez, F.; Meyer, A.; Felten, R.; Chatelus, E.; Javier, R.M.; Sordet, C.; Martin, T.; Korganow, A.S.; et al. Worldwide trends in all-cause mortality of auto-immune systemic diseases between 2001 and 2014. Autoimmun. Rev. 2020, 19, 102531. [Google Scholar] [CrossRef]
- Tolentino Júnior, D.S.; de Oliveira, C.M.; de Assis, E.M. Population-based Study of 24 Autoimmune Diseases Carried Out in a Brazilian Microregion. J. Epidemiol. Glob. Health 2019, 9, 243–251. [Google Scholar] [CrossRef]
- Burkitt, D.P. Some diseases characteristic of modern Western civilization. Br. Med. J. 1973, 1, 274–278. [Google Scholar] [CrossRef]
- Burkitt, D.P. Western diseases and their emergence related to diet. S. Afr. Med. J. 1982, 61, 1013–1015. [Google Scholar]
- Manzel, A.; Muller, D.N.; Hafler, D.A.; Erdman, S.E.; Linker, R.A.; Kleinewietfeld, M. Role of “Western diet” in inflammatory autoimmune diseases. Curr. Allergy Asthma Rep. 2014, 14, 404. [Google Scholar] [CrossRef]
- Christ, A.; Lauterbach, M.; Latz, E. Western Diet and the immune system: An inflammatory connection. Immunity 2019, 51, 794–811. [Google Scholar] [CrossRef]
- Mazzucca, C.B.; Raineri, D.; Cappellano, G.; Chiocchetti, A. How to Tackle the Relationship between Autoimmune Diseases and Diet: Well Begun Is Half-Done. Nutrients 2021, 13, 3956. [Google Scholar] [CrossRef]
- Mahmoudi, M.; Rezaei, N. (Eds.) Nutrition and Immunity; Springer Nature: Cham, Switzerland, 2019. [Google Scholar] [CrossRef]
- Lerner, A.; Matthias, T. Changes in intestinal tight junction permeability associated with industrial food additives explain the rising incidence of autoimmune disease. Autoimmun. Rev. 2015, 14, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Ruggeri, R.M.; Giovinazzo, S.; Barbalace, M.C.; Cristani, M.; Alibrandi, A.; Vicchio, T.M.; Giuffrida, G.; Aguennouz, M.H.; Malaguti, M.; Angeloni, C.; et al. Influence of Dietary Habits on Oxidative Stress Markers in Hashimoto’s Thyroiditis. Thyroid 2021, 31, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Tomasello, G.; Mazzola, M.; Leone, A.; Sinagra, E.; Zummo, G.; Farina, F.; Damiani, P.; Cappello, F.; Gerges Geagea, A.; Jurjus, A.; et al. Nutrition, oxidative stress and intestinal dysbiosis: Influence of diet on gut microbiota in inflammatory bowel diseases. Biomed. Pap. Med. 2016, 160, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Requena, T.; Martínez-Cuesta, M.C.; Peláez, C. Diet and microbiota linked in health and disease. Food Funct. 2018, 9, 688–704. [Google Scholar] [CrossRef]
- Rinninella, E.; Cintoni, M.; Raoul, P.; Lopetuso, L.R.; Scaldaferri, F.; Pulcini, G.; Miggiano, G.A.D.; Gasbarrini, A.; Mele, M.C. Food Components and Dietary Habits: Keys for a Healthy Gut Microbiota Composition. Nutrients 2019, 11, 2393. [Google Scholar] [CrossRef]
- Procaccini, C.; Carbone, F.; Galgani, M.; La Rocca, C.; De Rosa, V.; Cassano, S.; Matarese, G. Obesity and susceptibility to autoimmune diseases. Expert Rev. Clin. Immunol. 2011, 7, 287–294. [Google Scholar] [CrossRef]
- Le Moli, R.; Vella, V.; Tumino, D.; Piticchio, T.; Naselli, A.; Belfiore, A.; Frasca, F. Inflammasome activation as a link between obesity and thyroid disorders: Implications for an integrated clinical management. Front. Endocrinol. 2022, 13, 959276. [Google Scholar] [CrossRef]
- Lorenzo, P.M.; Sajoux, I.; Izquierdo, A.G.; Gomez-Arbelaez, D.; Zulet, M.A.; Abete, I.; Castro, A.I.; Baltar, J.; Portillo, M.P.; Tinahones, F.J.; et al. Immunomodulatory effect of a very-low-calorie ketogenic diet compared with bariatric surgery and a low-calorie diet in patients with excessive body weight. Clin. Nutr. 2022, 41, 1566–1577. [Google Scholar] [CrossRef]
- Kostoglou-Athanassiou, I.; Athanassiou, P. Editorial: Anti-inflammatory diet in autoimmune diseases. Front. Nutr. 2024, 22, 1497058. [Google Scholar] [CrossRef]
- Ruggeri, R.M.; Barbalace, M.C.; Croce, L.; Malaguti, M.; Campennì, A.; Rotondi, M.; Cannavò, S.; Hrelia, S. Autoimmune Thyroid Disorders: The Mediterranean Diet as a Protective Choice. Nutrients 2023, 15, 3953. [Google Scholar] [CrossRef]
- McCarty, M.F. Upregulation of lymphocyte apoptosis as a strategy for preventing and treating autoimmune disorders: A role for whole-food vegan, diets, fish oil and dopamine agonists. Med. Hypotheses. 2001, 57, 258–275. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [PubMed]
- Pobłocki, J.; Pańka, T.; Szczuko, M.; Telesiński, A.; Syrenicz, A. Whether a Gluten-Free Diet Should Be Recommended in Chronic Autoimmune Thyroiditis or Not? A 12-Month Follow-Up. J. Clin. Med. 2021, 10, 3240. [Google Scholar] [CrossRef]
- Szczuko, M.; Kacprzak, J.; Przybylska, A.; Szczuko, U.; Pobłocki, J.; Syrenicz, A.; Drozd, A. The Influence of an Anti-Inflammatory Gluten-Free Diet with EPA and DHA on the Involvement of Maresin and Resolvins in Hashimoto’s Disease. Int. J. Mol. Sci. 2024, 25, 11692. [Google Scholar] [CrossRef]
- Metso, S.; Hyytiä-Ilmonen, H.; Kaukinen, K.; Huhtala, H.; Jaatinen, P.; Salmi, J.; Taurio, J.; Collin, P. Gluten-free diet and autoimmune thyroiditis in patients with celiac disease. A Prospect. Control. Study. Scand. J. Gastroenterol. 2012, 47, 43–48. [Google Scholar] [CrossRef]
- Lerner, A.; Freire de Carvalho, J.; Kotrova, A.; Shoenfeld, Y. Gluten-free diet can ameliorate the symptoms _of non-celiac autoimmune diseases. Nutr. Rev. 2022, 80, 525–543. [Google Scholar] [CrossRef]
- Szczuko, M.; Syrenicz, A.; Szymkowiak, K.; Przybylska, A.; Szczuko, U.; Pobłocki, J.; Kulpa, D. Doubtful Justification of the Gluten-Free Diet in the Course of Hashimoto’s Disease. Nutrients 2022, 14, 1727. [Google Scholar] [CrossRef]
- Passali, M.; Josefsen, K.; Frederiksen, J.L.; Antvorskov, J.C. Current Evidence on the Efficacy of Gluten-Free Diets in Multiple Sclerosis, Psoriasis, Type 1 Diabetes and Autoimmune Thyroid Diseases. Nutrients 2020, 12, 2316. [Google Scholar] [CrossRef]
- Ruggeri, R.M.; Giuffrida, G.; Campennì, A. Autoimmune endocrine diseases. Minerva Endocrinol. 2018, 43, 305–322. [Google Scholar] [CrossRef]
- Kupper, C. Dietary guidelines and implementation for celiac disease. Gastroenterology 2005, 128, S121–S127. [Google Scholar] [CrossRef] [PubMed]
- Codex Alimentarius Commission. Draft Revised Codex Standard for Foods for Special Dietary Use for Persons Intolerant to Gluten Joint FAO/WHO Food Standards Programme; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [PubMed]
- Ruggeri, R.M.; Vicchio, T.M.; Cristani, M.; Certo, R.; Caccamo, D.; Alibrandi, A.; Giovinazzo, S.; Saija, A.; Campennì, A.; Trimarchi, F.; et al. Oxidative stress and advanced glycation end products in Hashimoto’s thyroiditis. Thyroid 2016, 4, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Di Bella, G.; Veronese, N.; Barbagallo, M. Impact of Mediterranean Diet on Chronic Non-Communicable Diseases and Longevity. Nutrients 2021, 13, 2028. [Google Scholar] [CrossRef]
- Oteri, V.; Galeano, F.; Panebianco, S.; Piticchio, T.; Le Moli, R.; Frittitta, L.; Vella, V.; Baratta, R.; Gullo, D.; Frasca, F.; et al. Influence of Mediterranean Diet on Sexual Function in People with Metabolic Syndrome: A Narrative Review. Nutrients 2024, 16, 3397. [Google Scholar] [CrossRef]
- Zhang, X.; Chen, W.; Shao, S.; Xu, G.; Song, Y.; Xu, C.; Gao, L.; Hu, C.; Zhao, J. A High-Fat Diet Rich in Saturated and Mono-Unsaturated Fatty Acids Induces Disturbance of Thyroid Lipid Profile and Hypothyroxinemia in Male Rats. Mol. Nutr. Food Res. 2018, 62, e1700599. [Google Scholar] [CrossRef]
- Liao, Z.; Kong, Y.; Zeng, L.; Wan, Q.; Hu, J.; Cai, Y. Effects of high-fat diet on thyroid autoimmunity in the female rat. BMC Endocr. Disord. 2022, 22, 179. [Google Scholar] [CrossRef]
- Bahadoran, Z.; Mirmiran, P.; Ghasemi, A.; Kabir, A.; Azizi, F.; Hadaegh, F. Is dietary nitrate/nitrite exposure a risk factor for development of thyroid abnormality? A systematic review and meta-analysis. Nitric Oxide. 2015, 47, 65–76. [Google Scholar] [CrossRef]
- Kubiak, K.; Szmidt, M.K.; Kaluza, J.; Zylka, A.; Sicinska, E. Do Dietary Supplements Affect Inflammation, Oxidative Stress, and Antioxidant Status in Adults with Hypothyroidism or Hashimoto’s Disease? A Systematic Review of Controlled Trials. Antioxidants 2023, 12, 1798. [Google Scholar] [CrossRef]
- da Silva, G.B.; Yamauchi, M.A.; Bagatini, M.D. Oxidative stress in Hashimoto’s thyroiditis: Possible adjuvant therapies to attenuate deleterious effects. Mol. Cell. Biochem. 2023, 478, 949–966. [Google Scholar] [CrossRef]
- Alehagen, U.; Alexander, J.; Aaseth, J.O.; Larsson, A.; Opstad, T.B. Supplementation with selenium and coenzyme Q10 in an elderly Swedish population low in selenium—Positive effects on thyroid hormones, cardiovascular mortality, and quality of life. BMC Med. 2024, 22, 191. [Google Scholar] [CrossRef] [PubMed]
- Naziroğlu, M.; Simşek, M. Effects of hormone replacement therapy with vitamin C and E supplementation on plasma thyroid hormone levels in postmenopausal women with Type 2 diabetes. Biomed. Pharmacother. 2009, 63, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Rabbani, E.; Golgiri, F.; Janani, L.; Moradi, N.; Fallah, S.; Abiri, B.; Vafa, M. Randomized Study of the Effects of Zinc, Vitamin A, and Magnesium Co-supplementation on Thyroid Function, Oxidative Stress, and hs-CRP in Patients with Hypothyroidism. Biol. Trace Elem. Res. 2021, 199, 4074–4083. [Google Scholar] [CrossRef] [PubMed]
- Rasheed, J.; Hassan, R.; Khalid, M.; Zafar, F. Frequency of autoimmune thyroiditis in children with Celiac disease and effect of gluten free diet. Pak. J. Med. Sci. 2020, 36, 1280–1284. [Google Scholar] [CrossRef]
- Collin, P.; Kaukinen, K.; Välimäki, M.; Salmi, J. Endocrinological disorders and celiac disease. Endocr. Rev. 2002, 23, 464–483. [Google Scholar] [CrossRef]
- Dore, M.P.; Fanciulli, G.; Rouatbi, M.; Mereu, S.; Pes, G.M. Autoimmune Thyroid Disorders Are More Prevalent in Patients with Celiac Disease: A Retrospective Case-Control Study. J. Clin. Med. 2022, 11, 6027. [Google Scholar] [CrossRef]
- Carroccio, A.; D’Alcamo, A.; Cavataio, F.; Soresi, M.; Seidita, A.; Sciumè, C.; Geraci, G.; Iacono, G.; Mansueto, P. High Proportions of People with Nonceliac Wheat Sensitivity Have Autoimmune Disease or Antinuclear Antibodies. Gastroenterology 2015, 149, 596–603.e1. [Google Scholar] [CrossRef]
- Hadithi, M.; de Boer, H.; Meijer, J.W.; Willekens, F.; Kerckhaert, J.A.; Heijmans, R.; Peña, A.S.; Stehouwer, C.D.; Mulder, C.J. Coeliac disease in Dutch patients with Hashimoto’s thyroiditis and vice versa. World J. Gastroenterol. 2007, 13, 1715–1722. [Google Scholar] [CrossRef]
- Kahaly, G.J.; Frommer, L.; Schuppan, D. Celiac disease and endocrine autoimmunity—The genetic link. Autoimmun. Rev. 2018, 17, 1169–1175. [Google Scholar] [CrossRef]
- Fasano, A. Leaky gut and autoimmune diseases. Clin. Rev. Allergy Immunol. 2012, 42, 71–78. [Google Scholar] [CrossRef]
- Reilly, N.R. The Gluten-Free Diet: Recognizing Fact, Fiction, and Fad. J. Pediatr. 2016, 175, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Piticchio, T.; Frasca, F.; Malandrino, P.; Trimboli, P.; Carrubba, N.; Tumminia, A.; Vinciguerra, F.; Frittitta, L. Effect of gluten-free diet on autoimmune thyroiditis progression in patients with no symptoms or histology of celiac disease: A meta-analysis. Front. Endocrinol. 2023, 14, 1200372. [Google Scholar] [CrossRef] [PubMed]
- Ülker, M.T.; Çolak, G.A.; Baş, M.; Erdem, M.G. Evaluation of the effect of gluten-free diet and Mediterranean diet on autoimmune system in patients with Hashimoto’s thyroiditis. Food Sci. Nutr. 2023, 12, 1180–1188. [Google Scholar] [CrossRef] [PubMed]
- Hrelia, S.; Barbalace, M.C.; Cannavò, S.; Ruggeri, R.M. Commentary: Fish and the thyroid: A Janus Bifrons relationship caused by pollutants and the omega-3 polyunsaturated fatty acids. Front. Endocrinol. 2023, 14, 1138245. [Google Scholar] [CrossRef]
- Liu, J.; Yu, L.L.; Wu, Y. Bioactive Components and Health Beneficial Properties of Whole Wheat Foods. J. Agric. Food Chem. 2020, 68, 12904–12915. [Google Scholar] [CrossRef]
- Biskup, I.; Gajcy, M.; Fecka, I. The potential role of selected bioactive compounds from spelt and common wheat in glycemic control. Adv. Clin. Exp. Med. 2017, 26, 1013–1019. [Google Scholar] [CrossRef]
- Obadi, M.; Sun, J.; Xu, B. Highland barley: Chemical composition, bioactive compounds, health effects, and applications. Food Res. Int. 2021, 140, 110065. [Google Scholar] [CrossRef]
- Virili, C.; Stramazzo, I.; Bagaglini, M.F.; Carretti, A.L.; Capriello, S.; Romanelli, F.; Trimboli, P.; Centanni, M. The relationship between thyroid and human-associated microbiota: A systematic review of reviews. Rev. Endocr. Metab. Disord. 2024, 25, 215–237. [Google Scholar] [CrossRef]
- Vici, G.; Belli, L.; Biondi, M.; Polzonetti, V. Gluten free diet and nutrient deficiencies: A review. Clin. Nutr. 2016, 35, 1236–1241. [Google Scholar] [CrossRef]
- Lebwohl, B.; Cao, Y.; Zong, G.; Hu, F.B.; Green, P.H.R.; Neugut, A.I.; Rimm, E.B.; Sampson, L.; Dougherty, L.W.; Giovannucci, E.; et al. Long term gluten consumption in adults without celiac disease and risk of coronary heart disease: Prospective cohort study. BMJ 2017, 357, j1892. [Google Scholar] [CrossRef]
- Piticchio, T.; Savarino, F.; Volpe, S.; Prinzi, A.; Costanzo, G.; Gamarra, E.; Frasca, F.; Trimboli, P. Inflammatory Profile Assessment in a Highly Selected Athyreotic Population Undergoing Controlled and Standardized Hypothyroidism. Biomedicines 2024, 12, 239. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| MedD | GFD | freeD | p Value | |
|---|---|---|---|---|
| Sex Male Female | 5 10 | 5 10 | 5 10 | |
| Age, yr median (range) | 42 (25–65) | 42 (24–65) | 41 (22–65) | 0.988 |
| Body weight (kg) | 63 (53–85) | 63 (47–80) | 62 (51–78) | 0.979 |
| BMI (kg/m2) | 24 (18–29.5) | 23 (20–29) | 23 (21–29.5) | 0.811 |
| W/H Ratio | 0.84 (0.70–0.95) | 0.85 (0.7–0.94) | 0.85 (0.75–0.90) | 0.958 |
| Fasting glucose (mg/dL) | 78 (65–90) | 80 (64–97) | 79 (70–94) | 0.924 |
| Basal fasting insulin (µIU/L) | 6.8 (4–10) | 7.7 (4–13) | 7.61 (5–11.5) | 0.758 |
| HOMA index | 1.8 (1.3–2.9) | 2.1 (1–3.4) | 2 (1–3.5) | 0.751 |
| Total cholesterol (mg/dL) | 171 (140–215) | 178 (140–220) | 179 (151–220) | 0.816 |
| LDL cholesterol (mg/dL) | 89 (60–123) | 91 (55–128) | 90 (84–120) | 0.983 |
| HDL cholesterol (mg/dL) | 62 (41–84) | 59 (54–91) | 59 (53–83) | 0.877 |
| Triglycerides (mg/dL) | 86 (52–104) | 89 (50–105) | 87 (36–148) | 0.977 |
| TSH (mIU/L) * | 1.6 (0.8–3.2) | 1.8 (0.7–3.1) | 1.85 (0.8–3.8) | 0.858 |
| FT4 (pml/L) * | 13.6 (12–16) | 13.8 (12.2–15.8) | 13.2 (12–14.8) | 0.636 |
| Tg-Ab (IU/L) | 469 (136–4000) | 368 (150–8070) | 402 (134–2659) | 0.994 |
| TPO-Ab (IU/L) * | 244 (45–4890) | 288 (140–3890) | 255 (134–4126) | 0.998 |
| Parameters | Baseline (T0) | After 12 Weeks (T1) | p Value |
|---|---|---|---|
| TSH | 1.8 (0.7–3.1) | 1.8 (0.9–3.2) | 0.929 |
| FT4 | 13.6 (12–16) | 13.5 (12–16.3) | 0.496 |
| Tg-Ab | 368 (150–8070) | 355 (133–3680) | 0.207 |
| TPO-Ab | 288 (140–3890) | 251.85 (110–3460) | 0.020 |
| OXIDATIVE STRESS PARAMETERS | |||||
|---|---|---|---|---|---|
| AGE | GPx | TRx | TEAA | p Value # | |
| T0 all patients (n = 45) | 165 (78–393) | 0.59 (0.3–0.84) | 1.58 (0.5–3.6) | 1.63 (0–1.8) | NS |
| T1 MedD (n = 15) | 102.7 (30–325) | 0.68 (0.5–1.0) | 2.09 (0.7–5.6) | 2.06 (0.7–2.4) | vs. T0, <0.05 * |
| T1 GFD (n = 15) | 165 (95–231) | 0.63 (0.30–0.9) | 1.56 (0.5–3.6) | 1.7 (0.1–1.9) | vs. T0, NS |
| T1 freeD (n = 15) | 168 (78–354) | 0.60 (0.3–0.8) | 1.48 (0.6–3.3) | 1.63 (0–1.8) | vs. T0, NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laganà, M.; Piticchio, T.; Alibrandi, A.; Le Moli, R.; Pallotti, F.; Campennì, A.; Cannavò, S.; Frasca, F.; Ruggeri, R.M. Effects of Dietary Habits on Markers of Oxidative Stress in Subjects with Hashimoto’s Thyroiditis: Comparison Between the Mediterranean Diet and a Gluten-Free Diet. Nutrients 2025, 17, 363. https://doi.org/10.3390/nu17020363
Laganà M, Piticchio T, Alibrandi A, Le Moli R, Pallotti F, Campennì A, Cannavò S, Frasca F, Ruggeri RM. Effects of Dietary Habits on Markers of Oxidative Stress in Subjects with Hashimoto’s Thyroiditis: Comparison Between the Mediterranean Diet and a Gluten-Free Diet. Nutrients. 2025; 17(2):363. https://doi.org/10.3390/nu17020363
Chicago/Turabian StyleLaganà, Martina, Tommaso Piticchio, Angela Alibrandi, Rosario Le Moli, Francesco Pallotti, Alfredo Campennì, Salvatore Cannavò, Francesco Frasca, and Rosaria Maddalena Ruggeri. 2025. "Effects of Dietary Habits on Markers of Oxidative Stress in Subjects with Hashimoto’s Thyroiditis: Comparison Between the Mediterranean Diet and a Gluten-Free Diet" Nutrients 17, no. 2: 363. https://doi.org/10.3390/nu17020363
APA StyleLaganà, M., Piticchio, T., Alibrandi, A., Le Moli, R., Pallotti, F., Campennì, A., Cannavò, S., Frasca, F., & Ruggeri, R. M. (2025). Effects of Dietary Habits on Markers of Oxidative Stress in Subjects with Hashimoto’s Thyroiditis: Comparison Between the Mediterranean Diet and a Gluten-Free Diet. Nutrients, 17(2), 363. https://doi.org/10.3390/nu17020363