
Bioelectrical Impedance Assessment in a Patient with Breast Cancer: A Case Report on the Effect of Integrative Therapies on Cellular Homeostasis


Abstract
1. Introduction
2. Materials and Methods
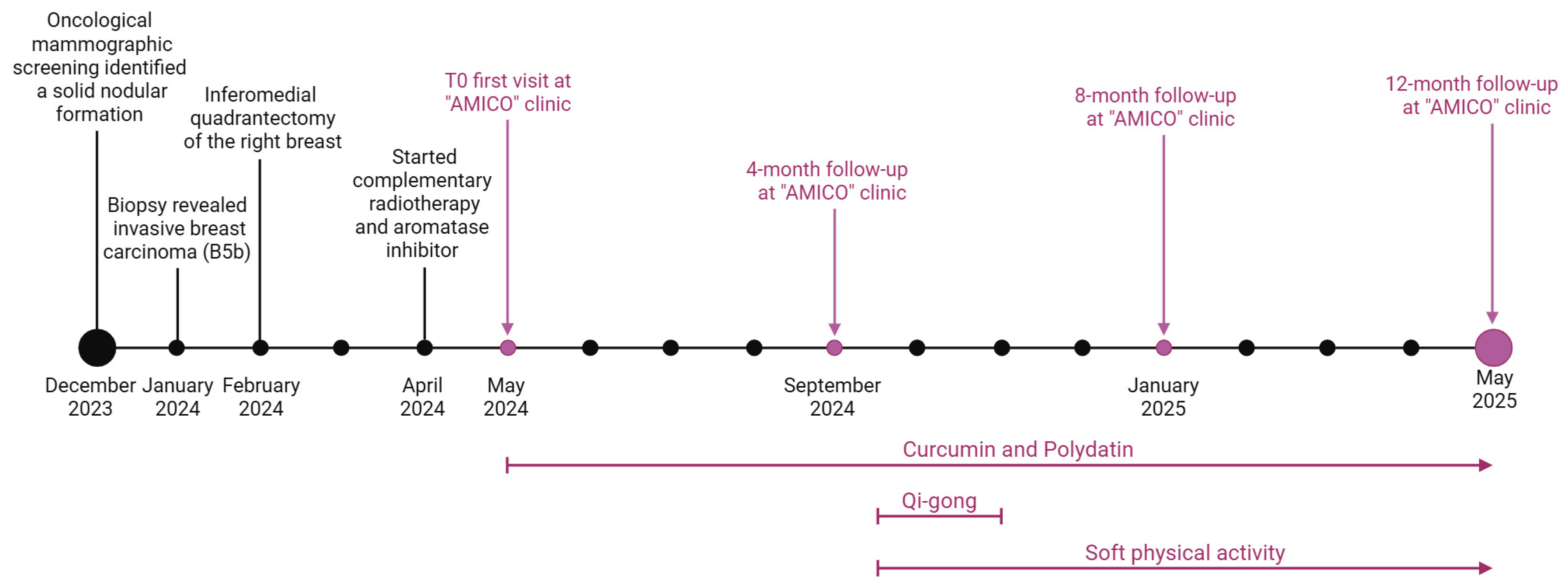
2.1. Patient Description
2.2. Study Intervention
2.2.1. Integrative Therapy Assessment
2.2.2. Bioelectrical Impedance Analysis (BIA)
2.2.3. Qigong Session
2.3. Measures and Findings Follow-Up
3. Results and Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACLM | American College of Lifestyle Medicine |
| AMICO | Ambulatorio di Medicina Integrata e Condotta in Oncologia |
| BC | Breast cancer |
| BIA | Bioelectrical impedance analysis |
| BMI | Body mass index |
| CRF | Cancer-related fatigue |
| ER | Oestrogen receptor |
| ECW | Extracellular water |
| FFM | Fat-free mass |
| FM | Fat mass |
| Gy | Gray |
| HER2 | Human epidermal growth factor receptor 2 |
| HP | Histopathological |
| ICW | Intracellular water |
| IHC | Immunohistochemical |
| Na+/K+ pump | Sodium-potassium pump |
| NST | No special type |
| PhA | Phase angle |
| PPSP | Persistent postsurgical pain |
| PR | Progesterone receptor |
| PUFAs | Polyunsaturated fatty acids |
| QMBE | Qigong Mind–Body Exercise |
| QoL | Quality of life |
| QTC | Qigong and Tai Chi |
| ROS | Reactive oxygen species |
| SIO | Society for Integrative Oncology |
| SMM | Skeletal muscle mass |
| TBW | Total body water |
References
- Barre, P.V.; Padmaja, G.; Rana, S.; Tiamongla. Stress and quality of life in cancer patients: Medical and psychological intervention. Indian J. Psychol. Med. 2018, 40, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Nardin, S.; Mora, E.; Varughese, F.M.; D’Avanzo, F.; Vachanaram, A.R.; Rossi, V.; Saggia, C.; Rubinelli, S.; Gennari, A. Breast Cancer Survivorship, Quality of Life, and Late Toxicities. Front. Oncol. 2020, 10, 864. [Google Scholar] [CrossRef]
- American Cancer Society. Breast Cancer Facts & Figure 2022 Figure 2023 Figure 2024. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-facts-and-figures/2022-2024-breast-cancer-fact-figures-acs.pdf (accessed on 5 May 2025).
- Guimond, A.J.; Ivers, H.; Savard, J. Clusters of Psychological Symptoms in Breast Cancer: Is There a Common Psychological Mechanism? Cancer Nurs. 2020, 43, 343–353. [Google Scholar] [CrossRef]
- Ng, C.G.; Mohamed, S.; Kaur, K.; Sulaiman, A.H.; Zainal, N.Z.; Taib, N.A. Perceived distress and its association with depression and anxiety in breast cancer patients. PLoS ONE 2017, 12, e0172975. [Google Scholar] [CrossRef] [PubMed]
- Leysen, L.; Lahousse, A.; Nijs, J.; Adriaenssens, N.; Mairesse, O.; Ivakhnov, S.; Bilterys, T.; Van Looveren, E.; Pas, R.; Beckwée, D. Prevalence and risk factors of sleep disturbances in breast cancersurvivors: Systematic review and meta-analyses. Support. Care Cancer 2019, 27, 4401–4433. [Google Scholar] [CrossRef]
- Fabi, A.; Rossi, A.; Mocini, E.; Cardinali, L.; Bonavolontà, V.; Cenci, C.; Magno, S.; Barberi, V.; Moretti, A.; Besharat, Z.M.; et al. An Integrated Care Approach to Improve Well-Being in Breast Cancer Patients. Curr. Oncol. Rep. 2024, 26, 346–358. [Google Scholar] [CrossRef] [PubMed]
- Latte-Naor, S.; Mao, J.J. Putting Integrative Oncology Into Practice: Concepts and Approaches. J. Oncol. Pract. 2019, 15, 7–14. [Google Scholar] [CrossRef]
- Cracolici, F.; Giallombardo, A.; Biancanelli, S.; Martignetti, A.; Fratarcangeli, C.; Falzetta, A.; Petreni, P.; Casi, C.; Farzad, M.; Fornai, G.; et al. Improving the quality of life of breast cancer patients with integrated medicine techniques. Int. J. Integr. Oncol. 2024, 1, 50–63. [Google Scholar]
- Greenlee, H.; Kwan, M.L.; Ergas, I.J.; Sherman, K.J.; Krathwohl, S.E.; Bonnell, C.; Lee, M.M.; Kushi, L.H. Complementary and alternative therapy use before and after breast cancer diagnosis: The Pathways Study. Breast Cancer Res. Treat. 2009, 117, 653–665. [Google Scholar] [CrossRef]
- Mecca, M.; Sichetti, M.; Giuseffi, M.; Giglio, E.; Sabato, C.; Sanseverino, F.; Marino, G. Synergic Role of Dietary Bioactive Compounds in Breast Cancer Chemoprevention and Combination Therapies. Nutrients 2024, 16, 1883. [Google Scholar] [CrossRef]
- Sichetti, M.; Giuseffi, M.; Giglio, E.; Marino, G.; Mecca, M. Effect of Natural Polyphenols on Breast Cancer Chemoprevention and Treatment. Mol. Nutr. Food Res. 2025, e70055. [Google Scholar] [CrossRef]
- Ligibel, J.A.; Bohlke, K.; May, A.M.; Clinton, S.K.; Demark-Wahnefried, W.; Gilchrist, S.C.; Irwin, M.L.; Late, M.; Mansfield, S.; Marshall, T.F.; et al. Exercise, Diet, and Weight Management During Cancer Treatment: ASCO Guideline. J. Clin. Oncol. 2022, 40, 2491–2507. [Google Scholar] [CrossRef] [PubMed]
- Lyman, G.H.; Greenlee, H.; Bohlke, K.; Bao, T.; DeMichele, A.M.; Deng, G.E.; Fouladbakhsh, J.M.; Gil, B.; Hershman, D.L.; Mansfield, S.; et al. Integrative Therapies During and After Breast Cancer Treatment: ASCO Endorsement of the SIO Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 2647–2655. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.; Sharma, K.; Potters, L.; Wernicke, A.G.; Parashar, B. Evidence for the Role of Mindfulness in Cancer: Benefits and Techniques. Cureus 2019, 11, e4629. [Google Scholar] [CrossRef]
- Branco, M.G.; Mateus, C.; Capelas, M.L.; Pimenta, N.; Santos, T.; Mäkitie, A.; Ganhão-Arranhado, S.; Trabulo, C.; Ravasco, P. Bioelectrical Impedance Analysis (BIA) for the Assessment of Body Composition in Oncology: A Scoping Review. Nutrients 2023, 15, 4792. [Google Scholar] [CrossRef]
- Marra, M.; Sammarco, R.; De Lorenzo, A.; Iellamo, F.; Siervo, M.; Pietrobelli, A.; Donini, L.M.; Santarpia, L.; Cataldi, M.; Pasanisi, F.; et al. Assessment of Body Composition in Health and Disease Using Bioelectrical Impedance Analysis (BIA) and Dual Energy X-ray Absorptiometry (DXA): A Critical Overview. Contrast Media Mol. Imaging 2019, 2019, 3548284. [Google Scholar] [CrossRef]
- Son, J.W.; Han, B.D.; Bennett, J.P.; Heymsfield, S.; Lim, S. Development and clinical application of bioelectrical impedance analysis method for body composition assessment. Obes. Rev. 2025, 26, e13844. [Google Scholar] [CrossRef]
- Grundmann, O.; Yoon, S.L.; Williams, J.J. The value of bioelectrical impedance analysis and phase angle in the evaluation of malnutrition and quality of life in cancer patients—A comprehensive review. Eur. J. Clin. Nutr. 2015, 69, 1290–1297. [Google Scholar] [CrossRef] [PubMed]
- Amano, K.; Bruera, E.; Hui, D. Diagnostic and prognostic utility of phase angle in patients with cancer. Rev. Endocr. Metab. Disord. 2023, 24, 479–489. [Google Scholar] [CrossRef]
- Bellido, D.; García-García, C.; Talluri, A.; Lukaski, H.C.; García-Almeida, J.M. Future lines of research on phase angle: Strengths and limitations. Rev. Endocr. Metab. Disord. 2023, 24, 563–583. [Google Scholar] [CrossRef]
- Matthews, L.; Bates, A.; Wootton, S.A.; Levett, D. The use of bioelectrical impedance analysis to predict postoperative complications in adult patients having surgery for cancer: A systematic review. Clin. Nutr. 2021, 40, 2914–2922. [Google Scholar] [CrossRef] [PubMed]
- Fajardo-Espinoza, F.S.; Cabrera-Nieto, S.A.; Espada-Vargas, A.L.; Pérez-Camargo, D.A.; Mohar, A.; Cruz-Ramos, M. Phase angle as a potential tool to evaluate chronic inflammatory state and predict quality of life deterioration in women with breast cancer and obesity: A narrative review. Nutrition 2024, 127, 112524. [Google Scholar] [CrossRef]
- Morlino, D.; Cioffi, I.; Marra, M.; Di Vincenzo, O.; Scalfi, L.; Pasanisi, F. Bioelectrical Phase Angle in Patients with Breast Cancer: A Systematic Review. Cancers 2022, 14, 2002. [Google Scholar] [CrossRef]
- Bejček, J.; Spiwok, V.; Kmoníčková, E.; Rimpelová, S. Na+/K+-ATPase Revisited: On Its Mechanism of Action, Role in Cancer, and Activity Modulation. Molecules 2021, 26, 1905. [Google Scholar] [CrossRef]
- Peruzzo, R.; Biasutto, L.; Szabò, I.; Leanza, L. Impact of intracellular ion channels on cancer development and progression. Eur. Biophys. J. 2016, 45, 685–707. [Google Scholar] [CrossRef] [PubMed]
- Khajah, M.A.; Mathew, P.M.; Luqmani, Y.A. Na+/K+ ATPase activity promotes invasion of endocrine resistant breast cancer cells. PLoS ONE 2018, 13, e0193779. [Google Scholar] [CrossRef]
- Felippe Gonçalves-de-Albuquerque, C.; Ribeiro Silva, A.; Ignácio da Silva, C.; Caire Castro-Faria-Neto, H.; Burth, P. Na/K Pump and Beyond: Na/K-ATPase as a Modulator of Apoptosis and Autophagy. Molecules 2017, 22, 578. [Google Scholar] [CrossRef] [PubMed]
- Mijatovic, T.; Dufrasne, F.; Kiss, R. Na+/K+-ATPase and cancer. Pharm. Pat. Anal. 2012, 1, 91–106. [Google Scholar] [CrossRef]
- Gradishar, W.J.; Anderson, B.O.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Blair, S.L.; Burstein, H.J.; Dang, C.; Elias, A.D.; et al. Breast cancer, version 3.2020, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Canc. Netw. 2020, 18, 452–478. [Google Scholar] [CrossRef]
- Pan, H.; Gray, R.; Braybrooke, J.; Davies, C.; Taylor, C.; McGale, P.; Peto, R.; Pritchard, K.I.; Bergh, J.; Dowsett, M.; et al. 20-Year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years. N. Engl. J. Med. 2017, 377, 1836–1846. [Google Scholar] [CrossRef]
- Divella, R.; Marino, G.; Infusino, S.; Lanotte, L.; Gadaleta-Caldarola, G.; Gadaleta-Caldarola, G. The mediterranean lifestyle to contrast low-grade inflammation behavior in cancer. Nutrients 2023, 15, 1667. [Google Scholar] [CrossRef]
- Turati, F.; Carioli, G.; Bravi, F.; Ferraroni, M.; Serraino, D.; Montella, M.; Giacosa, A.; Toffolutti, F.; Negri, E.; Levi, F.; et al. Mediterranean diet and breast cancer risk. Nutrients 2018, 10, 326. [Google Scholar] [CrossRef]
- Soltero, E.G.; Larkey, L.K.; Kim, W.S.; Chavez, J.B.R.; Lee, R.E. Latin dance and Qigong/Tai Chi effects on physical activity and body composition in breast cancer survivors: A pilot study. Complement. Ther. Clin. Pract. 2022, 47, 101554. [Google Scholar] [CrossRef]
- Yan, Y.; López-Alcalde, J.; Zhang, L.; Siebenhuener, A.R.; Witt, C.M.; Barth, J. Acupuncture for the prevention of chemotherapy-induced nausea and vomiting in cancer patients: A systematic review and meta-analysis. Cancer Med. 2023, 12, 12504–12517. [Google Scholar] [CrossRef]
- Lengacher, C.A.; Shelton, M.M.; Reich, R.R.; Barta, M.K.; Johnson-Mallard, V.; Moscoso, M.S.; Paterson, C.; Ramesar, S.; Budhrani, P.; Carranza, I.; et al. Mindfulness based stress reduction (MBSR (BC)) in breast cancer: Evaluating fear of recurrence (FOR) as a mediator of psychological and physical symptoms in a randomized control trial (RCT). J. Behav. Med. 2014, 37, 185–195. [Google Scholar] [CrossRef]
- Chlebowski, R.T.; Aragaki, A.K.; Anderson, G.L.; Pan, K.; Neuhouser, M.L.; Manson, J.E.; Thomson, C.A.; Mossavar-Rahmani, Y.; Lane, D.S.; Johnson, K.C.; et al. Dietary modification and breast cancer mortality: Long-term follow-up of the women’s health initiative randomized trial. J. Clin. Oncol. 2020, 38, 1419–1428. [Google Scholar] [CrossRef]
- Mousavi, S.M.; Milajerdi, A.; Varkaneh, H.K.; Gorjipour, M.M.; Esmaillzadeh, A. The effects of curcumin supplementation on body weight, body mass index and waist circumference: A systematic review and dose-response meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2020, 60, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Cheng, L.; Du, S.; Wang, K.; Liu, S. Antioxidant curcumin induces oxidative stress to kill tumor cells. Oncol. Lett. 2023, 27, 67. [Google Scholar] [CrossRef]
- Mele, L.; Paino, F.; Papaccio, F.; Regad, T.; Boocock, D.; Stiuso, P.; Lombardi, A.; Liccardo, D.; Aquino, G.; Barbieri, A.; et al. A new inhibitor of glucose-6-phosphate dehydrogenase blocks pentose phosphate pathway and suppresses malignant proliferation and metastasis in vivo. Cell Death Dis. 2018, 9, 572. [Google Scholar] [CrossRef] [PubMed]
- Mele, L.; la Noce, M.; Paino, F.; Regad, T.; Wagner, S.; Liccardo, D.; Papaccio, G.; Lombardi, A.; Caraglia, M.; Tirino, V.; et al. Glucose-6-phosphate dehydrogenase blockade potentiates tyrosine kinase inhibitor effect on breast cancer cells through autophagy perturbation. J. Exp. Clin. Cancer Res. 2019, 38, 160. [Google Scholar] [CrossRef] [PubMed]
- Hao, J.; Chen, C.; Huang, K.; Huang, J.; Li, J.; Liu, P.; Huang, H. Polydatin improves glucose and lipid metabolism in experimental diabetes through activating the Akt signaling pathway. Eur. J. Pharmacol. 2014, 745, 152–165. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Wu, J.; Mo, J.; Guo, L.; Wu, X.; Bao, Y. Polydatin Inhibits Adipose Tissue Inflammation and Ameliorates Lipid Metabolism in High-Fat-Fed Mice. BioMed Res. Int. 2019, 2019, 7196535. [Google Scholar] [CrossRef] [PubMed]
- Teich, T.; Pivovarov, J.A.; Porras, D.P.; Dunford, E.C.; Riddell, M.C. Curcumin limits weight gain, adipose tissue growth, and glucose intolerance following the cessation of exercise and caloric restriction in rats. J. Appl. Physiol. 2017, 123, 1625–1634. [Google Scholar] [CrossRef]
- de Oliveira, M.R.; Jardim, F.R.; Setzer, W.N.; Nabavi, S.M.; Nabavi, S.F. Curcumin, mitochondrial biogenesis, and mitophagy: Exploring recent data and indicating future needs. Biotechnol. Adv. 2016, 34, 813–826. [Google Scholar] [CrossRef]
- Meng, T.; Hu, S.F.; Cheng, Y.Q.; Ye, M.N.; Wang, B.; Wu, J.J.; Chen, H.F. Qigong for women with breast cancer: An updated systematic review and meta-analysis. Complement. Ther. Med. 2021, 60, 102743. [Google Scholar] [CrossRef]
- Osypiuk, K.; Ligibel, J.; Giobbie-Hurder, A.; Vergara-Diaz, G.; Bonato, P.; Quinn, R.; Ng, W.; Wayne, P.M. Qigong Mind-Body Exercise as a Biopsychosocial Therapy for Persistent Post-Surgical Pain in Breast Cancer: A Pilot Study. Integr. Cancer Ther. 2020, 19, 1534735419893766. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Li, H.; Sze, D.M.; Chan, V.W.S.; Yang, A.W.H. Effectiveness of qigong and tai chi in the quality of life of patients with cancer: Protocol for an umbrella review. BMJ Open 2022, 12, e057980. [Google Scholar] [CrossRef]
- Zeng, Q.; Li, C.; Yu, T.; Zhang, H. Comparative Effects of Exercise Interventions and Mindfulness-Based Interventions for Cognitive Impairment and Quality of Life in Breast Cancer Survivors During or After Cancer Treatment: A Systematic Review and Bayesian Network Meta-analysis. Am. J. Phys. Med. Rehabil. 2024, 103, 777–788. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, J.; Hu, D.; Gao, L.; Huang, T. Which specific modes of exercise training are most effective for breast related cancer fatigue? Network meta-analysis. Front. Oncol. 2025, 15, 1491634. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Demographics | |
| Age (years) | 73 |
| Gender | Female |
| Ethnicity | White |
| Smoking | No |
| Alcohol | No |
| Drugs | Bisphosphonates |
| Health measures | |
| Weight (kg) | 64 |
| Height (cm) | 160 |
| BMI | 25.0 |
| Parameter | T0 | 4 Months | 8 Months | 12 Months | Reference Range |
|---|---|---|---|---|---|
| Haematochemical | |||||
| Red blood cells | 5.22 | 5.10 | 5.11 | 5.05 | 4.20–6.10 × 106/µL |
| Haemoglobin | 15.3 | 15.0 | 15.2 | 15.0 | 12–18 g/dL |
| Mean corpuscular volume | 86.9 | 88.1 | 85.6 | 86.6 | 88–99 fL |
| Platelets | 176 | 210 | 198 | 178 | 130–400 × 103/µL |
| White blood cells | 2.98 | 2.94 | 2.96 | 3.36 | 5.20–12.40 × 103/µL |
| Glucose | 93 | 91 | 85 | 91 | 74–109 mg/dL |
| Cholesterol | 261 | 250 | 247 | 217 | <200 mg/dL |
| AST | 24 | 24 | 18 | 20 | 0–35 U/L |
| ALT | 31 | 22 | 14 | 16 | 0–35 U/L |
| Gamma-GT | 18 | 38 | 32 | 23 | 6–42 U/L |
| Calcium | 10.19 | 10.01 | 10.13 | 10.10 | 8.60–10.20 mg/dL |
| Vitamin D | 28.8 | 48.2 | 49.4 | 55.6 | 30–100 µg/L |
| BIA | |||||
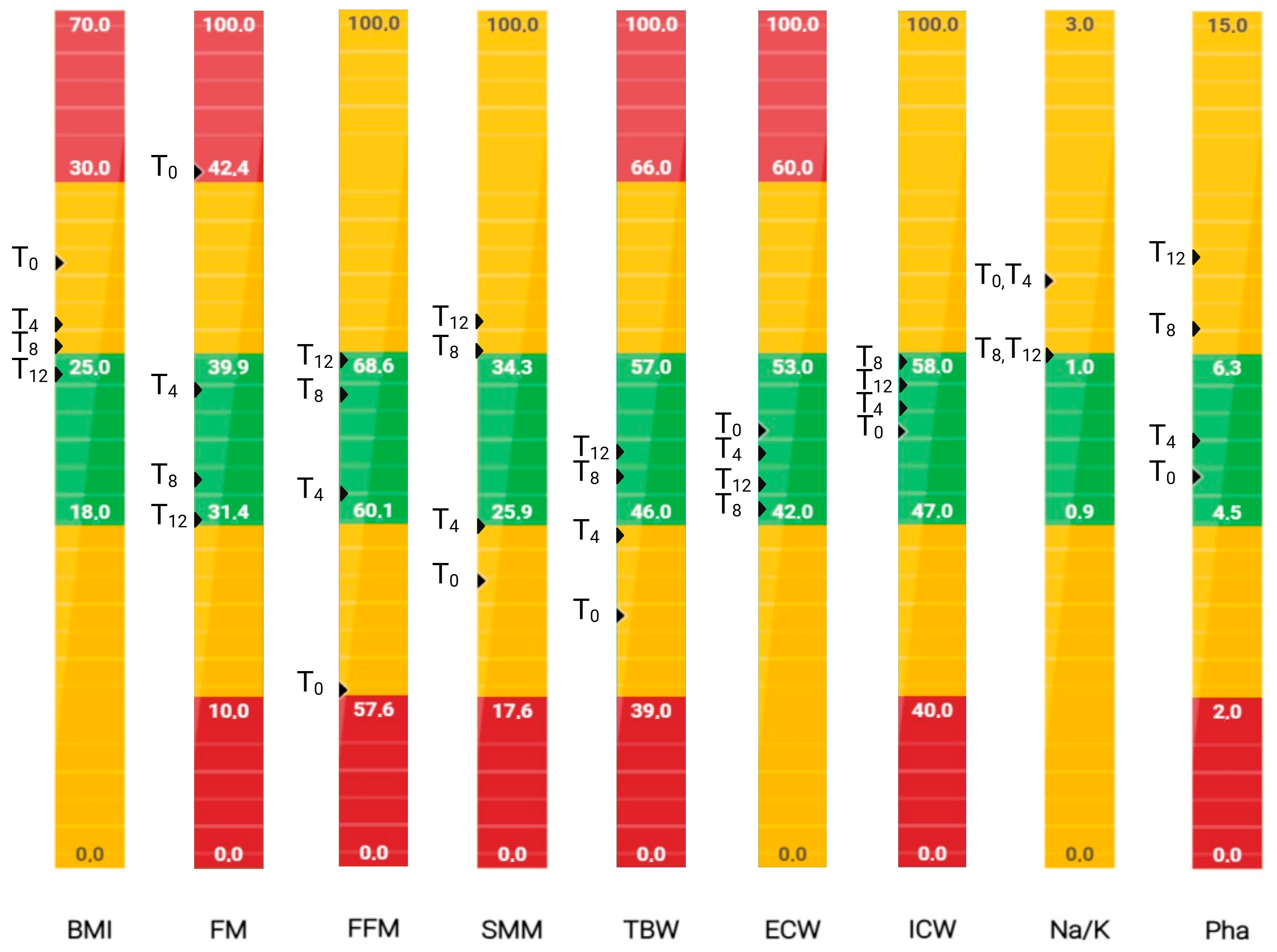
| BMI | 27.4 | 25.6 | 25.2 | 24.4 | 18–25 |
| FM (%) | 43.1 | 38.2 | 33.2 | 31.6 | 31.4–39.9 |
| FFM (%) | 56.9 | 61.8 | 66.8 | 68.4 | 60.1–68.6 |
| SMM (%) | 22.9 | 25.9 | 34.4 | 37.9 | 25.9–34.3 |
| ICW (%) | 52.4 | 53.1 | 57.1 | 56.0 | 47.0–58.0 |
| ECW (%) | 47.6 | 46.9 | 42.9 | 44.0 | 42.0–53.0 |
| TBW (%) | 42.0 | 45.5 | 49.0 | 50.1 | 46.0–57.0 |
| Na/K | 1.4 | 1.4 | 1.0 | 1.0 | 0.9–1.0 |
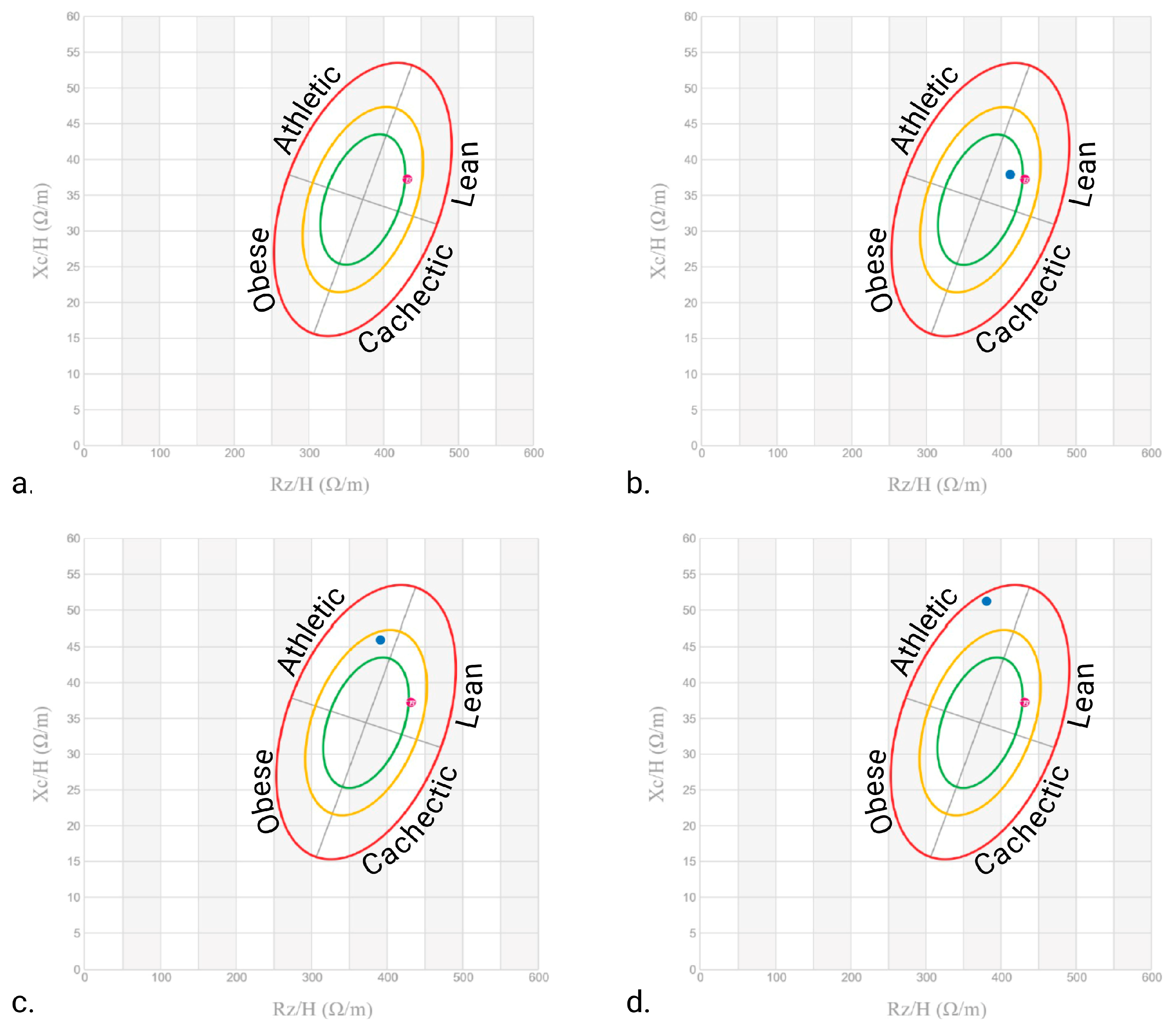
| PhA | 4.9 | 5.3 | 7.1 | 9.0 | 4.5–6.3° |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marino, G.; Pace, G.; Sabato, L.; Sichetti, M.; Mecca, M. Bioelectrical Impedance Assessment in a Patient with Breast Cancer: A Case Report on the Effect of Integrative Therapies on Cellular Homeostasis. Nutrients 2025, 17, 2506. https://doi.org/10.3390/nu17152506
Marino G, Pace G, Sabato L, Sichetti M, Mecca M. Bioelectrical Impedance Assessment in a Patient with Breast Cancer: A Case Report on the Effect of Integrative Therapies on Cellular Homeostasis. Nutrients. 2025; 17(15):2506. https://doi.org/10.3390/nu17152506
Chicago/Turabian StyleMarino, Graziella, Giovanni Pace, Lucia Sabato, Marzia Sichetti, and Marisabel Mecca. 2025. "Bioelectrical Impedance Assessment in a Patient with Breast Cancer: A Case Report on the Effect of Integrative Therapies on Cellular Homeostasis" Nutrients 17, no. 15: 2506. https://doi.org/10.3390/nu17152506
APA StyleMarino, G., Pace, G., Sabato, L., Sichetti, M., & Mecca, M. (2025). Bioelectrical Impedance Assessment in a Patient with Breast Cancer: A Case Report on the Effect of Integrative Therapies on Cellular Homeostasis. Nutrients, 17(15), 2506. https://doi.org/10.3390/nu17152506