
Evaluation of the Influence of Intervention Tools Used in Nutrition Education Programs: A Mixed Approach



Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
- Peer-reviewed studies involving human populations under the age of 18 years old;
- Experimental studies that investigated a nutrition education intervention;
- Studies that assessed, pre- and post-intervention, the population’s adherence to healthy diets;
- Studies published between January 2014 and November 2024.
2.3. Qualitative Analysis Phase: Data Collection and Extraction
2.4. Quantitative Analysis Phase: Data Collection, Extraction, and Coding
2.5. KIDMED Questionnaire
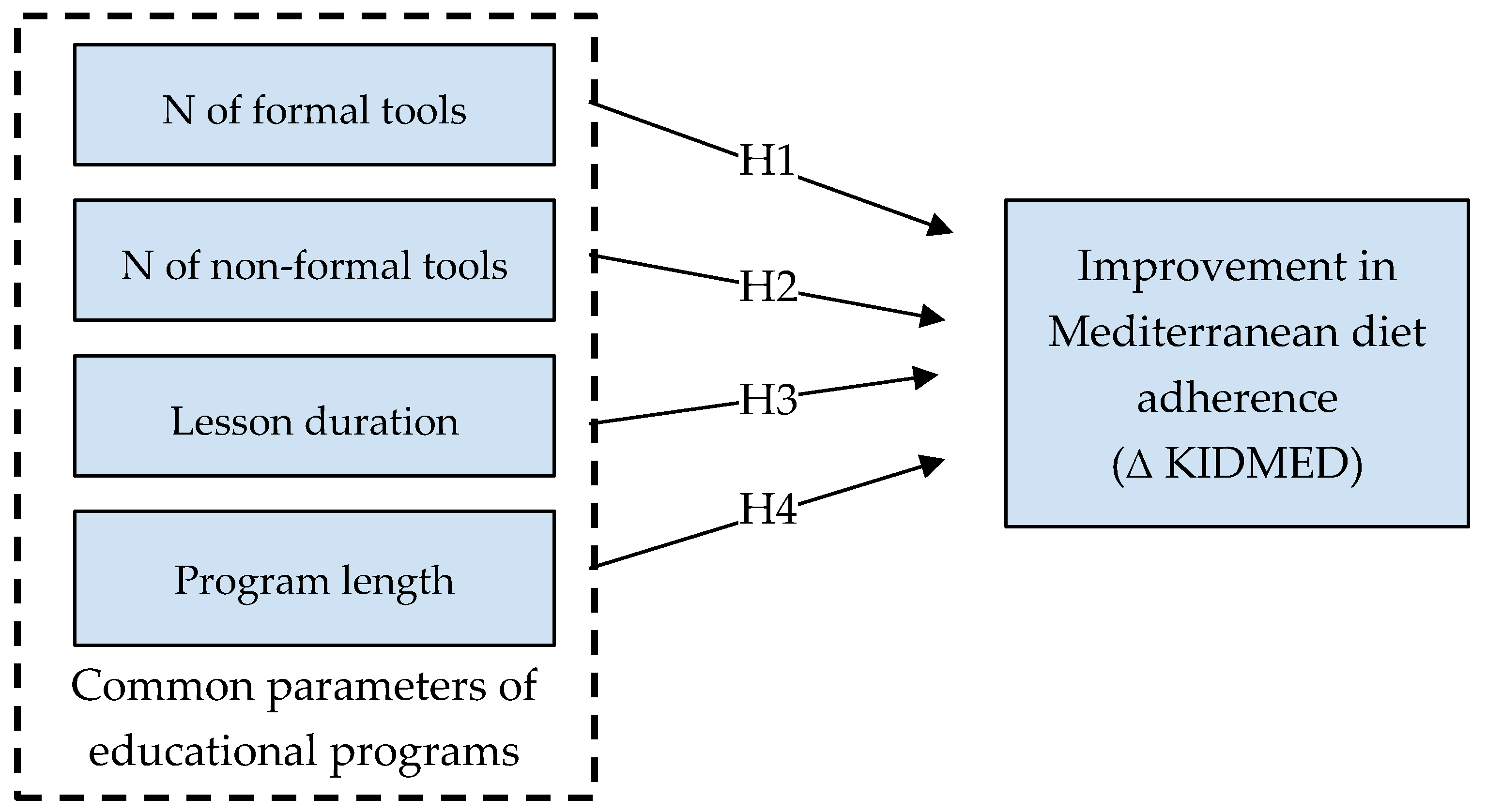
2.6. Evaluation of the Effectiveness
- Number of educational tools divided by category: formal (e.g., frontal teaching) or non-formal tools (e.g., active education tools);
- Duration of individual meetings;
- Total length of the educational intervention.
2.7. Statistical Analysis
3. Results
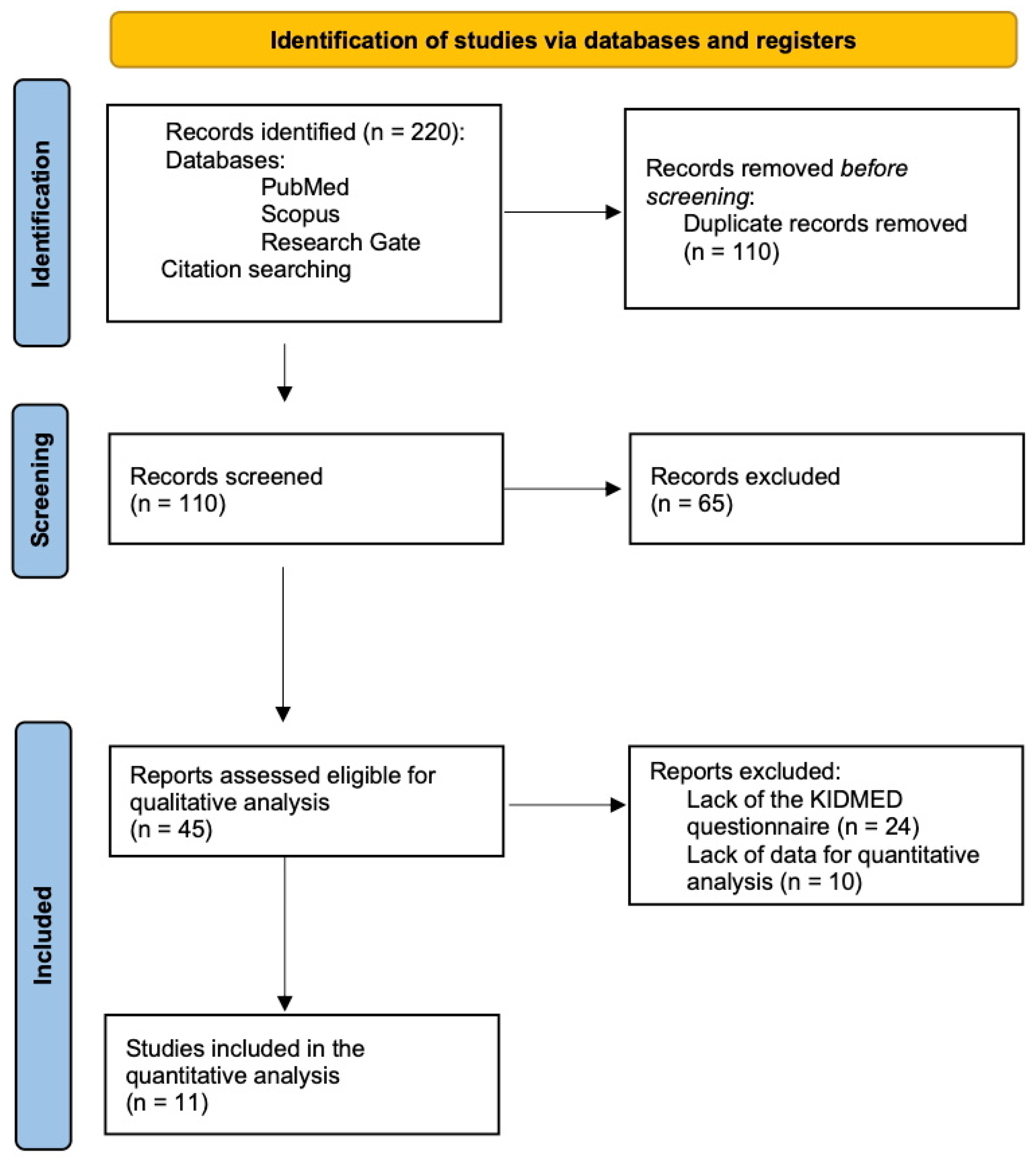
3.1. Study Selection
3.2. Qualitative Analysis
3.2.1. Population
3.2.2. Geographical Areas
3.2.3. Types of Interventions
3.2.4. Educational Strategies and Intervention Tools
3.2.5. Intervention Lengths and Single-Meeting Durations
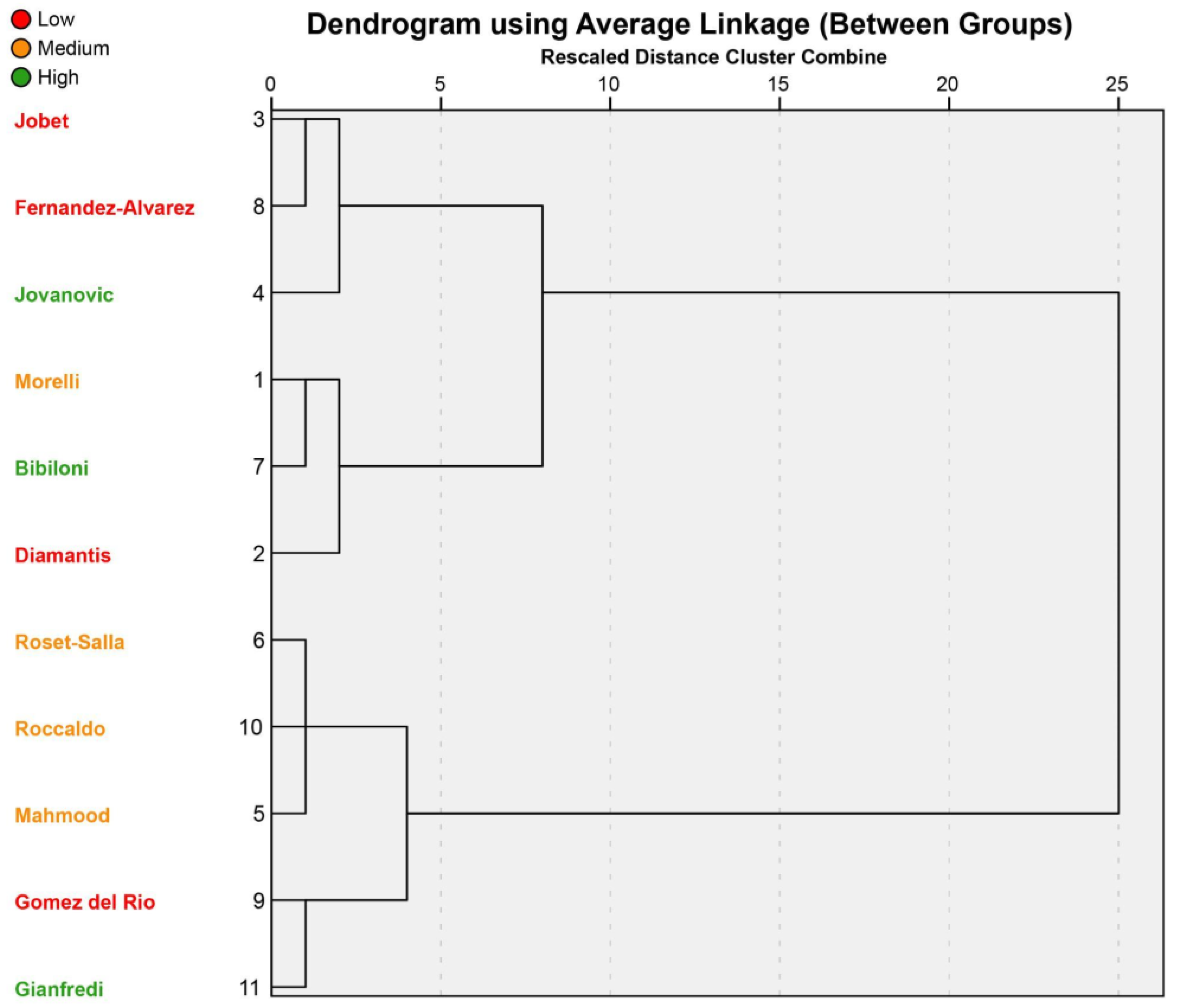
3.3. Evaluation and Quantification of Effectiveness
4. Discussion
- The adoption of a systemic, transdisciplinary, and multi-level approach, both in the design phase and during the implementation of NE programs;
- The analysis and reporting of the details of school and/or class context, e.g., size, socioeconomic composition, cultures, and values, to allow comparisons with other school settings;
- An overall and detailed description of the educational program;
- The description and respective justification for the themes addressed by the programs, even if they are related to the school context;
- The report of all intervention tools utilized within the program, dividing them into formal and non-formal, and possibly including a description or attachment of all graphic materials as the supplementary information;
- The report of seminar durations and frequency and interventions;
- The details of who delivers the lessons and/or who is in charge of each educational activity;
- The description of the eventual parents’ and teachers’ involvement;
- An analysis of barriers encountered during the implementation phase, including an evaluation of intervention tools;
- The use of validated systems for evaluating and quantifying the final effectiveness of interventions, taking into account common variables, using similar measurement criteria.
5. Strengths and Limits
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patra, E.; Kokkinopoulou, A.; Pagkalos, I. Focus of Sustainable Healthy Diets Interventions in Primary School-Aged Children: A Systematic Review. Nutrients 2023, 15, 2460. [Google Scholar] [CrossRef] [PubMed]
- Ghammachi, N.; Mihrshahi, S.; Ronto, R. Web-Based Experiential Nutrition Education Intervention “The Green Hub” to Promote Sustainable and Healthy Diets among Young Adults in Australia. Sustainability 2022, 14, 15207. [Google Scholar] [CrossRef]
- Grosso, G.; Buso, P.; Mata, A.; Abdelkarim, O.; Aly, M.; Pinilla, J.; Fernandez, A.; Mendez, R.; Alvarez, A.; Valdes, N.; et al. Understanding consumer food choices & promotion of healthy and sustainable Mediterranean diet and lifestyle in children and adolescents through behavioural change actions: The DELICIOUS project. Int. J. Food Sci. Nutr. 2024, 75, 527–535. [Google Scholar] [CrossRef]
- Global Nutrition Report: Stronger Commitments for Greater Action; Development Initiatives; Global Nutrition Report: Bristol, UK, 2022.
- Bentham, J.; Singh, G.M.; Danaei, G.; Green, R.; Lin, J.K.; Stevens, G.A.; Farzadfar, F.; Bennett, J.E.; Di Cesare, M.; Dangour, A.D.; et al. Multidimensional characterization of global food supply from 1961 to 2013. Nat. Food 2020, 1, 70–75. [Google Scholar] [CrossRef]
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef]
- Popkin, B.M.; Ng, S.W. The nutrition transition to a stage of high obesity and noncommunicable disease prevalence dominated by ultra-processed foods is not inevitable. Obes. Rev. 2022, 23, e13366. [Google Scholar] [CrossRef]
- Lee, K.A.; Bai, Y.; Wunderlich, S.M. A pilot study for plant the seed: A nutrition education program using local food environment to put theory into action. Int. J. Sustain. Dev. Plan. 2016, 11, 1028–1036. [Google Scholar] [CrossRef]
- Suleiman-Martos, N.; García-Lara, R.A.; Martos-Cabrera, M.B.; Albendín-García, L.; Romero-Béjar, J.L.; Cañadas-De La Fuente, G.A.; Gómez-Urquiza, J.L. Gamification for the Improvement of Diet, Nutritional Habits, and Body Composition in Children and Adolescents: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2478. [Google Scholar] [CrossRef] [PubMed]
- Marques, C.; Lima, J.P.M.; Fialho, S.; Pinto, E.; Baltazar, A.L. Impact of a Food Education Session on Vegetables Plate Waste in a Portuguese School Canteen. Sustainability 2022, 14, 16674. [Google Scholar] [CrossRef]
- Spinelli & Mandolini. Gli Stili di Vita Dei Bambini e Delle Bambine. In Stato Ponderale e Stili di Vita di Bambine e Bambini: I Dati Italiani Della Sorveglianza “Okkio Alla SALUTE 2023” e il Contributo Dello Studio “EPaS-ISS”; EpiCentro ISS: Rome, Italy, 10 May 2024. [Google Scholar]
- WHO European Regional Obesity Report 2022; WHO Regional Office for Europe: Copenhagen, Denmark, 2022.
- WHO. Childhood Overweight and Obesity; World Health Organization: Geneva, Switzerland, 2014; Available online: http://www.who.int/dietphysicalactivity/childhood/en/ (accessed on 19 April 2024).
- Mogre, V.; Sefogah, P.E.; Adetunji, A.W.; Olalekan, O.O.; Gaa, P.K.; Ayettey Anie, H.N.G.; Tayo, B. A school-based food and nutrition education intervention increases nutrition-related knowledge and fruit consumption among primary school children in northern Ghana. BMC Public Health 2024, 24, 1739. [Google Scholar] [CrossRef]
- Teo, C.H.; Chin, Y.S.; Lim, P.Y.; Masrom, S.A.H.; Shariff, Z.M. Impacts of a School-Based Intervention That Incorporates Nutrition Education and a Supportive Healthy School Canteen Environment among Primary School Children in Malaysia. Nutrients 2021, 13, 1712. [Google Scholar] [CrossRef] [PubMed]
- D’Egidio, V.; Lia, L.; Sinopoli, A.; Backhaus, I.; Mannocci, A.; Saulle, R.; Sestili, C.; Cocchiara, R.; Di Bella, O.; Yordanov, T.; et al. Results of the Italian project ‘GiochiAMO’ to improve nutrition and PA among children. J. Public Health 2021, 43, 405–412. [Google Scholar] [CrossRef]
- Maatoug, J.; Msakni, Z.; Zammit, N.; Bhiri, S.; Harrabi, I.; Boughammoura, L.; Slama, S.; Larbi, C.; Ghannem, H. School-Based Intervention as a Component of a Comprehensive Community Program for Overweight and Obesity Prevention, Sousse, Tunisia, 2009–2014. Prev. Chronic. Dis. 2015, 12, 140518. [Google Scholar] [CrossRef]
- Montella, L.; Liguori, N.; Tondini, L.; Castellone, L.; Pacella, D.; Del Prete, S.; Bove, P.; Berretta, M.; Vanni, M.; Facchini, G. The Easy Thing (ET) observational study: Evaluation of adherence to Mediterranean diet and role of a program of nutritional intervention performed by North Naples 2 Local Health Unit. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 2260–2269. [Google Scholar]
- Diamantis, D.V.; Shalit, A.; Katsas, K.; Zioga, E.; Zota, D.; Kastorini, C.M.; Veloudaki, A.; Kouvari, M.; Linos, A. Improving Children’s Lifestyle and Quality of Life through Synchronous Online Education: The Nutritional Adventures School-Based Program. Nutrients 2023, 15, 5124. [Google Scholar] [CrossRef]
- Aureli, V.; Rossi, L. Nutrition Knowledge as a Driver of Adherence to the Mediterranean Diet in Italy. Front. Nutr. 2022, 9, 804865. [Google Scholar] [CrossRef]
- Follong, B.M.; Verdonschot, A.; Prieto-Rodriguez, E.; Miller, A.; Collins, C.E.; Bucher, T. Nutrition across the curriculum: A scoping review exploring the integration of nutrition education within primary schools. Nutr. Res. Rev. 2022, 35, 181–196. [Google Scholar] [CrossRef] [PubMed]
- Rosi, A.; Brighenti, F.; Finistrella, V.; Ingrosso, L.; Monti, G.; Vanelli, M.; Vitale, M.; Volta, E.; Scazzina, F. Giocampus school: A “learning through playing” approach to deliver nutritional education to children. Int. J. Food Sci. Nutr. 2016, 67, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Jung, T.; Huang, J.; Eagan, L.; Oldenburg, D. Influence of school-based nutrition education program on healthy eating literacy and healthy food choice among primary school children. Int. J. Health Promot. Educ. 2019, 57, 67–81. [Google Scholar] [CrossRef]
- Creswell, J. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 4th ed.; SAGE Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Johnson, M.; Majewska, D. Formal, Non-Formal, and Informal Learning: What Are They, and How Can We Research Them? Cambridge University: Cambridge, UK, 2022. [Google Scholar]
- Młynarczuk-Sokołowska, A. Intercultural non-formal education: What the children think. Intercult. Educ. 2022, 33, 82–98. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- Arndt, S.; Turvey, C.; Andreasen, N.C. Correlating and predicting psychiatric symptom ratings: Spearmans r versus Kendalls tau correlation. J. Psychiatr. Res. 1999, 33, 97–104. [Google Scholar] [CrossRef]
- Bujang, M.A. An elaboration on sample size determination for correlations based on effect sizes and confidence interval width: A guide for researchers. Restor. Dent. Endod. 2024, 49, e21. [Google Scholar] [CrossRef]
- Jenkins, D.G.; Quintana-Ascencio, P.F. A solution to minimum sample size for regressions. PLoS ONE 2020, 15, e0229345. [Google Scholar] [CrossRef] [PubMed]
- Scherr, R.E.; Cox, R.J.; Feenstra, G.; Zidenberg-Cherr, S. Integrating local agriculture into nutrition programs can benefit children’s health. Calif. Agric. 2013, 67, 30–37. [Google Scholar] [CrossRef]
- Antwi, J.; Ohemeng, A.; Boateng, L.; Quaidoo, E.; Bannerman, B. Primary school-based nutrition education intervention on nutrition knowledge, attitude and practices among school-age children in Ghana. Glob. Health Promot. 2020, 27, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Bibiloni, M.D.M.; Fernández-Blanco, J.; Pujol-Plana, N.; Surià Sonet, S.; Pujol-Puyané, M.C.; Mercadé Fuentes, S.; Ojer Fernández De Soto, L.; Tur, J.A. Reversión de sobrepeso y obesidad en población infantil de Vilafranca del Penedès: Programa ACTIVA’T (2012). Gac. Sanit. 2019, 33, 197–202. [Google Scholar] [CrossRef]
- Calvo-Malvar, M.; Benítez-Estévez, A.J.; Sánchez-Castro, J.; Leis, R.; Gude, F. Effects of a Community-Based Behavioral Intervention with a Traditional Atlantic Diet on Cardiometabolic Risk Markers: A Cluster Randomized Controlled Trial (“The GALIAT Study”). Nutrients 2021, 13, 1211. [Google Scholar] [CrossRef]
- Buyco, N.G.; Dorado, J.B.; Azaña, G.P.; Viajar, R.V.; Aguila, D.V.; Capanzana, M.V. Do school-based nutrition interventions improve the eating behavior of school-age children? Nutr. Res. Pract. 2022, 16, 217. [Google Scholar] [CrossRef]
- Del Río, N.G.; González-González, C.S.; Martín-González, R.; Navarro-Adelantado, V.; Toledo-Delgado, P.; García-Peñalvo, F. Effects of a Gamified Educational Program in the Nutrition of Children with Obesity. J. Med. Syst. 2019, 43, 198. [Google Scholar] [CrossRef]
- Roset-Salla, M.; Ramon-Cabot, J.; Salabarnada-Torras, J.; Pera, G.; Dalmau, A. Educational intervention to improve adherence to the Mediterranean diet among parents and their children aged 1–2 years. EniM clinical trial. Public Health Nutr. 2016, 19, 1131–1144. [Google Scholar] [CrossRef]
- Saaka, M.; Kizito, F.; Hoeschle-Zeledon, I. Effect of nutrition education on nutrition-related knowledge, attitudes, and consumption of diversified diets among families owning a home garden in northern Ghana. World Nutr. 2021, 12, 15–31. [Google Scholar] [CrossRef]
- Taniguchi, T.; Haslam, A.; Sun, W.; Sisk, M.; Hayman, J.; Jernigan, V.B.B. Impact of a Farm-to-School Nutrition and Gardening Intervention for Native American Families from the FRESH Study: A Randomized Wait-List Controlled Trial. Nutrients 2022, 14, 2601. [Google Scholar] [CrossRef]
- Liz Martins, M.; Rodrigues, S.S.; Cunha, L.M.; Rocha, A. Strategies to reduce plate waste in primary schools—Experimental evaluation. Public Health Nutr. 2016, 19, 1517–1525. [Google Scholar] [CrossRef]
- Antón-Peset, A.; Fernandez-Zamudio, M.-A.; Pina, T. Promoting Food Waste Reduction at Primary Schools. A Case Study. Sustainability 2021, 13, 600. [Google Scholar] [CrossRef]
- Ghammachi, N.; Dharmayani, P.N.A.; Mihrshahi, S.; Ronto, R. Investigating Web-Based Nutrition Education Interventions for Promoting Sustainable and Healthy Diets in Young Adults: A Systematic Literature Review. Int. J. Environ. Res. Public. Health 2022, 19, 1691. [Google Scholar] [CrossRef] [PubMed]
- Vos, M.; Deforche, B.; Van Kerckhove, A.; Michels, N.; Geuens, M.; Van Lippevelde, W. Intervention strategies to promote healthy and sustainable food choices among parents with lower and higher socioeconomic status. BMC Public Health 2022, 22, 2378. [Google Scholar] [CrossRef]
- Kendel Jovanović, G.; Janković, S.; Pavičić ŽeŽelj, S. The effect of nutritional and lifestyle education intervention program on nutrition knowledge, diet quality, lifestyle, and nutritional status of Croatian school children. Front. Sustain. Food Syst. 2023, 7, 1019849. [Google Scholar] [CrossRef]
- Herawati, H.D.; Kurniasari, Y.; Rahayu, H.K.; Hositanisita, H.; Afifah, E.; Isvianti, A.; Susilowati, N.S.; Batubara, S.; Sonia, P. Gardening-cooking based intervention for improving healthy eating habits in preschool children. Paediatr. Indones. 2024, 64, 218–226. [Google Scholar] [CrossRef]
- Harrison, L.; Herrmann, A.; Quitmann, C.; Stieglbauer, G.; Zeitz, C.; Franke, B.; Danquah, I. Effects of a cafeteria-based sustainable diet intervention on the adherence to the EAT-Lancet planetary health diet and greenhouse gas emissions of consumers: A quasi-experimental study at a large German hospital. Nutr. J. 2024, 23, 80. [Google Scholar] [CrossRef]
- Karpouzis, F.; Lindberg, R.; Walsh, A.; Shah, S.; Abbott, G.; Ball, K. Impact and process evaluation of a primary-school Food Education and Sustainability Training (FEAST) program in 10-12-year-old children in Australia: Pragmatic cluster non-randomized controlled trial. BMC Public Health 2024, 24, 657. [Google Scholar] [CrossRef] [PubMed]
- Torre, G.L.; Mannocci, A.; Saulle, R.; Sinopoli, A.; D’Egidio, V.; Sestili, C.; Manfuso, R.; Masala, D. GiochiAMO! Muoviamoci e mangiamo sano! La promozione dell’attività fisica e della piramide alimentare per i bambini: Protocollo di una sperimentazione di campo. Clin Ter 2016, 167, 152–155. [Google Scholar]
- Ogunsile, S.E.; Ogundele, B.O. Effect of game-enhanced nutrition education on knowledge, attitude and practice of healthy eating among adolescents in Ibadan, Nigeria. Int. J. Health Promot. Educ. 2016, 54, 207–216. [Google Scholar] [CrossRef]
- Keshani, P.; Mousavi, S.M.; Mirzaei, Z.; Hematdar, Z.; Maayeshi, N.; Mirshekari, M.; Ranjbaran, H.; Faghih, S. Effect of a School-based Nutrition Education Program on the Nutritional Status of Primary School Children. Nutr. Food Sci. Res. 2016, 3, 27–34. [Google Scholar] [CrossRef]
- Ng, C.M.; Kaur, S.; Koo, H.C.; Mukhtar, F. Examining the long-term effectiveness of a culinary nutrition education intervention on children’s dietary practices and variety. Hum. Nutr. Metab. 2024, 36, 200266. [Google Scholar] [CrossRef]
- Fernández-Álvarez, M.; Martín-Payo, R.; García-García, R.; Cuesta, M.; Carrasco-Santos, S. A nutrition education intervention in adolescents who play soccer: The IDEHA-F project. Psicothema 2020, 3, 359–365. [Google Scholar] [CrossRef]
- Franciscato, S.J.; Janson, G.; Machado, R.; Lauris, J.R.P.; Andrade, S.M.J.D.; Fisberg, M. Impact of the nutrition education Program Nutriamigos® on levels of awareness on healthy eating habits in school-aged children. J. Hum. Growth Dev. 2019, 29, 390–402. [Google Scholar] [CrossRef]
- Raut, S.; Kc, D.; Singh, D.R.; Dhungana, R.R.; Pradhan, P.M.S.; Sunuwar, D.R. Effect of nutrition education intervention on nutrition knowledge, attitude, and diet quality among school-going adolescents: A quasi-experimental study. BMC Nutr. 2024, 10, 35. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Bi, X.; Gao, T.; Yang, T.; Xu, P.; Gan, Q.; Xu, J.; Cao, W.; Wang, H.; Pan, H.; et al. Effect of School-Based Nutrition and Health Education for Rural Chinese Children. Nutrients 2022, 14, 3997. [Google Scholar] [CrossRef] [PubMed]
- Belando-Pedreño, N.; Blanco-García, M.E.; Chamorro, J.L.; García-Martí, C. Pilot Study on Satisfaction in Children and Adolescents after a Comprehensive Educational Program on Healthy Habits. Nutrients 2023, 15, 1161. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Bertarelli, G.; Minelli, L.; Nucci, D. Promoting healthy eating in childhood: Results from the Children PrOmOting Nutrition throUgh Theatre (COcONUT) project. Minerva Pediatr. 2024, 76, 464–472. [Google Scholar] [CrossRef]
- Mahmood, M.A.; Shaker, N.Z.; Ismael, S.A. Impact of family-based nutrition education intervention program on eating habit among obese school age children in Rania city/Iraq. Int. J. Health Sci. 2022, 6, 2059–2071. [Google Scholar] [CrossRef]
- Szczepańska, E.; Bielaszka, A.; Kiciak, A.; Wanat-Kańtoch, G.; Staśkiewicz, W.; Białek-Dratwa, A.; Kardas, M. The Project “Colourful Means Healthy” as an Educational Measure for the Prevention of Diet-Related Diseases: Investigating the Impact of Nutrition Education for School-Aged Children on Their Nutritional Knowledge. Int. J. Environ. Res. Public Health 2022, 19, 13307. [Google Scholar] [CrossRef] [PubMed]
- Jobet Bustos, E.; Loyola Alegría, M.I.; Ortiz Castro, C.; Rigotti, A.; Echeverría, G.; Mallea, C.; Barja, S. Improvement in adherence to Mediterranean diet in children attending preschool centers. Nutr. Hosp. 2024, 41, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Morelli, C.; Avolio, E.; Galluccio, A.; Caparello, G.; Manes, E.; Ferraro, S.; Caruso, A.; De Rose, D.; Barone, I.; Adornetto, C.; et al. Nutrition Education Program and Physical Activity Improve the Adherence to the Mediterranean Diet: Impact on Inflammatory Biomarker Levels in Healthy Adolescents From the DIMENU Longitudinal Study. Front. Nutr. 2021, 8, 685247. [Google Scholar] [CrossRef]
- Roccaldo, R.; Censi, L.; D’Addezio, L.; Berni Canani, S.; Gennaro, L. Improvement of Adherence to the Mediterranean Diet through a Nutrition Education Teaching Pack for Teachers within the “School Fruit Scheme” Program: An Italian Long-Term Trial in School Children. Nutrients 2024, 16, 2057. [Google Scholar] [CrossRef]
- Nury, E.; Stadelmaier, J.; Morze, J.; Nagavci, B.; Grummich, K.; Schwarzer, G.; Hoffmann, G.; Angele, C.M.; Steinacker, J.M.; Wendt, J.; et al. Effects of nutritional intervention strategies in the primary prevention of overweight and obesity in school settings: Systematic review and network meta-analysis. BMJ Med. 2022, 1, e000346. [Google Scholar] [CrossRef]
- Andrade, J.; Lotton, J.; Andrade, J. Systematic Review: Frameworks Used in School-Based Interventions, the Impact on Hispanic Children’s Obesity-Related Outcomes. J. Sch. Health 2018, 88, 847–858. [Google Scholar] [CrossRef]
- Shinde, S.; Wang, D.; Moulton, G.E.; Fawzi, W.W. School-based health and nutrition interventions addressing double burden of malnutrition and educational outcomes of adolescents in low- and middle-income countries: A systematic review. Matern. Child. Nutr. 2023, 21 (Suppl. 1), e13437. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lim, H. Nutritional Management in Childhood Obesity. J. Obes. Metab. Syndr. 2019, 28, 225–235. [Google Scholar] [CrossRef]
- Uzşen, H.; Didar Başbakkal, Z. A Game-based Nutrition Education: Teaching Healthy Eating to Primary School Students. J. Pediatr. Res. 2019, 6, 18–23. [Google Scholar] [CrossRef]
- Teo, C.H.; Chin, Y.S.; Lim, P.Y.; Masrom, S.A.H.; Shariff, Z.M. School-based intervention that integrates nutrition education and supportive healthy school food environment among Malaysian primary school children: A study protocol. BMC Public Health 2019, 19, 1427. [Google Scholar] [CrossRef] [PubMed]
- Asakura, K.; Mori, S.; Sasaki, S.; Nishiwaki, Y. A school-based nutrition education program involving children and their guardians in Japan: Facilitation of guardian-child communication and reduction of nutrition knowledge disparity. Nutr. J. 2021, 20, 92. [Google Scholar] [CrossRef] [PubMed]
- De Vlieger, N.M.; Sainsbury, L.; Smith, S.P.; Riley, N.; Miller, A.; Collins, C.E.; Bucher, T. Feasibility and Acceptability of ‘VitaVillage’: A Serious Game for Nutrition Education. Nutrients 2021, 14, 189. [Google Scholar] [CrossRef] [PubMed]
- Love, P.; Booth, A.; Margerison, C.; Nowson, C.; Grimes, C. Food and nutrition education opportunities within Australian primary schools. Health Promot. Int. 2020, 35, 1291–1301. [Google Scholar] [CrossRef] [PubMed]
- Eustachio Colombo, P.; Patterson, E.; Lindroos, A.K.; Parlesak, A.; Elinder, L.S. Sustainable and acceptable school meals through optimization analysis: An intervention study. Nutr. J. 2020, 19, 61. [Google Scholar] [CrossRef]
- Murimi, M.W.; Moyeda-Carabaza, A.F.; Nguyen, B.; Saha, S.; Amin, R.; Njike, V. Factors that contribute to effective nutrition education interventions in children: A systematic review. Nutr. Rev. 2018, 76, 553–580. [Google Scholar] [CrossRef]
- D’Adamo, C.; McArdle, P.; Balick, L.; Peisach, E.; Ferguson, T.; Diehl, A.; Bustad, K.; Bowden, B.; Pierce, B.; Berman, B. Spice MyPlate: Nutrition Education Focusing Upon Spices and Herbs Improved Diet Quality and Attitudes Among Urban High School Students. Am. J. Health Promot. 2015, 9, 150709150949009. [Google Scholar] [CrossRef]
- Chetty, R.; Friedman, J.; Rockoff, J. The Long-Term Impacts of Teachers: Teacher Value-Added and Student Outcomes in Adulthood; National Bureau of Economic Research: Cambridge, MA, USA, 2011; w17699p, Available online: http://www.nber.org/papers/w17699.pdf (accessed on 12 May 2025).
- McLean, L.; Espinoza, P.; Janssen, J.; Jimenez, M.; Lindstrom Johnson, S. Relationships between elementary teachers’ enjoyment and students’ engagement across content areas and among student groups. Sch. Psychol. 2025, 40, 419–430. [Google Scholar] [CrossRef]
- Jayanthi, M.; Gersten, R.; Taylor, M.J.; Smolkowski, K.; Dimino, J. Impact of the Developing Mathematical Ideas Professional Development Program on Grade 4 Students’ and Teachers’ Understanding of Fractions (REL 2017-256); U.S. Department of Education, Institute of Education Sciences, National Center for Education Evaluation and Regional Assistance, Regional Educational Laboratory Southeast: Washington, DC, USA, 2017. Available online: https://ies.ed.gov/rel-southeast/2025/01/main-publication-file (accessed on 14 May 2025).
- FAO (Food and Agriculture Organization). Evaluation of FAO’s Contributions to Sustainable Development Goal 2—Nutrition Education; FAO: Rome, Italy, 2021. [Google Scholar]
- Charlton, K.; Comerford, T.; Deavin, N.; Walton, K. Characteristics of successful primary school-based experiential nutrition programmes: A systematic literature review. Public Health Nutr. 2021, 24, 4642–4662. [Google Scholar] [CrossRef]
- Ülker, M.T.; Elmacıoğlu, F.; Büyükateş, H.S.; Özdemir, A.; Kuşcu Sezen, H.; Gündüz, S.N. The effect of sustainable food literacy education on primary school nutrition attitudes and behaviours. Toros Univ. J. Food Nutr. Gastron. 2024, 3, 29–34. [Google Scholar] [CrossRef]
- Lamas, S.; Rebelo, S.; Da Costa, S.; Sousa, H.; Zagalo, N.; Pinto, E. The Influence of Serious Games in the Promotion of Healthy Diet and Physical Activity Health: A Systematic Review. Nutrients 2023, 15, 1399. [Google Scholar] [CrossRef] [PubMed]
- Schreinemachers, P.; Rai, B.B.; Dorji, D.; Chen, H.; Dukpa, T.; Thinley, N.; Sherpa, P.L.; Yang, R.-Y. School gardening in Bhutan: Evaluating outcomes and impact. Food Secur. 2017, 9, 635–648. [Google Scholar] [CrossRef]
- Prescott, M.P.; Burg, X.; Metcalfe, J.J.; Lipka, A.E.; Herritt, C.; Cunningham-Sabo, L. Healthy Planet, Healthy Youth: A Food Systems Education and Promotion Intervention to Improve Adolescent Diet Quality and Reduce Food Waste. Nutrients 2019, 11, 1869. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Scoring | |
|---|---|
| +1 | Takes a fruit or fruit juice every day |
| +1 | Has a second fruit every day |
| +1 | Has fresh or cooked vegetables regularly once a day |
| +1 | Has fresh or cooked vegetables more than once a day |
| +1 | Consumes fish regularly (at least 2–3 times per week) |
| −1 | Goes more than once a week to a fast-food (hamburger) restaurant |
| +1 | Likes pulses and eats them more than once a week |
| +1 | Consumes pasta or rice almost every day (5 or more times per week) |
| +1 | Has cereals or grains (bread, etc.) for breakfast |
| +1 | Consumes nuts regularly (at least 2–3 times per week) |
| +1 | Uses olive oil at home |
| −1 | Skips breakfast |
| +1 | Has a dairy product for breakfast (yoghurt, milk, etc.) |
| −1 | Has commercially baked goods or pastries for breakfast |
| +1 | Takes two yoghurts and/or some cheese (40 g) daily |
| −1 | Takes sweets and candy several times every day |
| First Author (Year) | Population | Intervention Methods | Lesson Duration/ Program Length | KIDMED at Baseline | Results (Δ KIDMED) | KIDMED Improvement (%) |
|---|---|---|---|---|---|---|
| Bibiloni, M.D.M. (2017) [33] | 319 (3–7 y.o.); parents | Cartoons, group discussions, drawings, creation of graphics, crosswords. | 15′ (children), 30′ (adults)/3 years | 6.51 | 1.89 | 15.77 |
| del Río, N.G. (2019) [36] | 64 (6–12 y.o.) | Physical activity, video gaming, ClassDojo. | 2 h/12 weeks | 7.67 | 0.08 | 0.77 |
| Diamantis, D. (2023) [19] | 12.451 (7–11 y.o.) | Puzzles, crosswords, quizzes, booklets, diaries. Textbook, storytelling, physical activity. | 1 h/1 month | 5.50 | 0.20 | 1.67 |
| Fernández-Álvarez, M. (2020) [52] | 319 (14–19 y.o.) | Posters, food wheel, food pyramid, web app, group activities, recipe preparation. | no lessons/6 months | 6.34 | 0.05 | 0.40 |
| Gianfredi, V. (2024) [57] | 18 (5–12 y.o.) | Educational laboratories, cooking classes, workshops, interactive games, theatre laboratories, healthy snacks and gadgets. | 2 h/1 year | 6.28 | 1.61 | 13.43 |
| Jobet, E. (2024) [60] | 95 (≥18 m.o.) | Infographics, didactic material. | no lessons/5 months | 7.40 | 0.50 | 4.17 |
| Kendel Jovanovic, G. (2023) [44] | 2709 (10–12 y.o.) | Presentations, brochures, infographics, posters, website, school meetings. | 20′/3 weeks + 6–9 weeks of follow-up | 6.77 | 1.18 | 9.83 |
| Mahmood, M.A. (2022) [58] | 70 (8–12 y.o.) | Classes, video, workshops, games, physical activity. | 90′/12 weeks | N.R. | 0.69 | 5.75 |
| Morelli, C. (2021) [61] | 85 (14–17 y.o.) | Seminars, interactive laboratories, official website, Facebook page. | 35′/1 year | 6.03 | 0.93 | 7.75 |
| Roccaldo, R. (2017) [62] | 494 (10–11 y.o.) | Classes. | 1 h/6 weeks | 6.00 | 1.00 | 8.33 |
| Roset-Salla, M. (2016) [37] | 206 (1–2 y.o.); 195 parents | Workshops, group games, card games. | 90′/6 months | 6.50 | 0.60 | 5.00 |
| Formal Intervention Strategies | Non-Formal Intervention Strategies | Class Duration | Intervention Length | KIDMED Improvement | ||
|---|---|---|---|---|---|---|
| Formal Intervention Strategies | tau coefficient | -- | ||||
| Sig. (2-tailed) | . | |||||
| Non-formal Intervention Strategies | tau coefficient | 0.099 | -- | |||
| Sig. (2-tailed) | 0.720 | . | ||||
| Class Duration | tau coefficient | −0.436 | 0.173 | -- | ||
| Sig. (2-tailed) | 0.101 | 0.502 | . | |||
| Intervention Length | tau coefficient | −0.046 | −0.086 | 0.000 | -- | |
| Sig. (2-tailed) | 0.863 | 0.737 | 1.000 | . | ||
| KIDMED Improvement | tau coefficient | 0.000 | 0.021 | 0.114 | 0.076 | -- |
| Sig. (2-tailed) | 1.000 | 0.934 | 0.635 | 0.752 | . |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muzzioli, L.; Gimbo, C.; Pintavalle, M.; Migliaccio, S.; Donini, L.M. Evaluation of the Influence of Intervention Tools Used in Nutrition Education Programs: A Mixed Approach. Nutrients 2025, 17, 2460. https://doi.org/10.3390/nu17152460
Muzzioli L, Gimbo C, Pintavalle M, Migliaccio S, Donini LM. Evaluation of the Influence of Intervention Tools Used in Nutrition Education Programs: A Mixed Approach. Nutrients. 2025; 17(15):2460. https://doi.org/10.3390/nu17152460
Chicago/Turabian StyleMuzzioli, Luca, Costanza Gimbo, Maria Pintavalle, Silvia Migliaccio, and Lorenzo M. Donini. 2025. "Evaluation of the Influence of Intervention Tools Used in Nutrition Education Programs: A Mixed Approach" Nutrients 17, no. 15: 2460. https://doi.org/10.3390/nu17152460
APA StyleMuzzioli, L., Gimbo, C., Pintavalle, M., Migliaccio, S., & Donini, L. M. (2025). Evaluation of the Influence of Intervention Tools Used in Nutrition Education Programs: A Mixed Approach. Nutrients, 17(15), 2460. https://doi.org/10.3390/nu17152460