







Comparative Effectiveness of Exercise, Protein Supplementation, and Combined Interventions for Sarcopenia Management in Women: A Network Meta-Analysis


Abstract
1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Search Strategy and Study Selection
2.3. Eligibility Criteria
2.3.1. Population
2.3.2. Intervention
2.3.3. Comparator
2.3.4. Outcome
2.3.5. Study Design
2.4. Data Extraction
2.5. Measures of Treatment Effect
2.6. Quality Assessment of Evidence
2.7. Minimally Contextualized Framework
2.8. Statistical Analysis
3. Results
3.1. Literature Selection and Study Characteristics
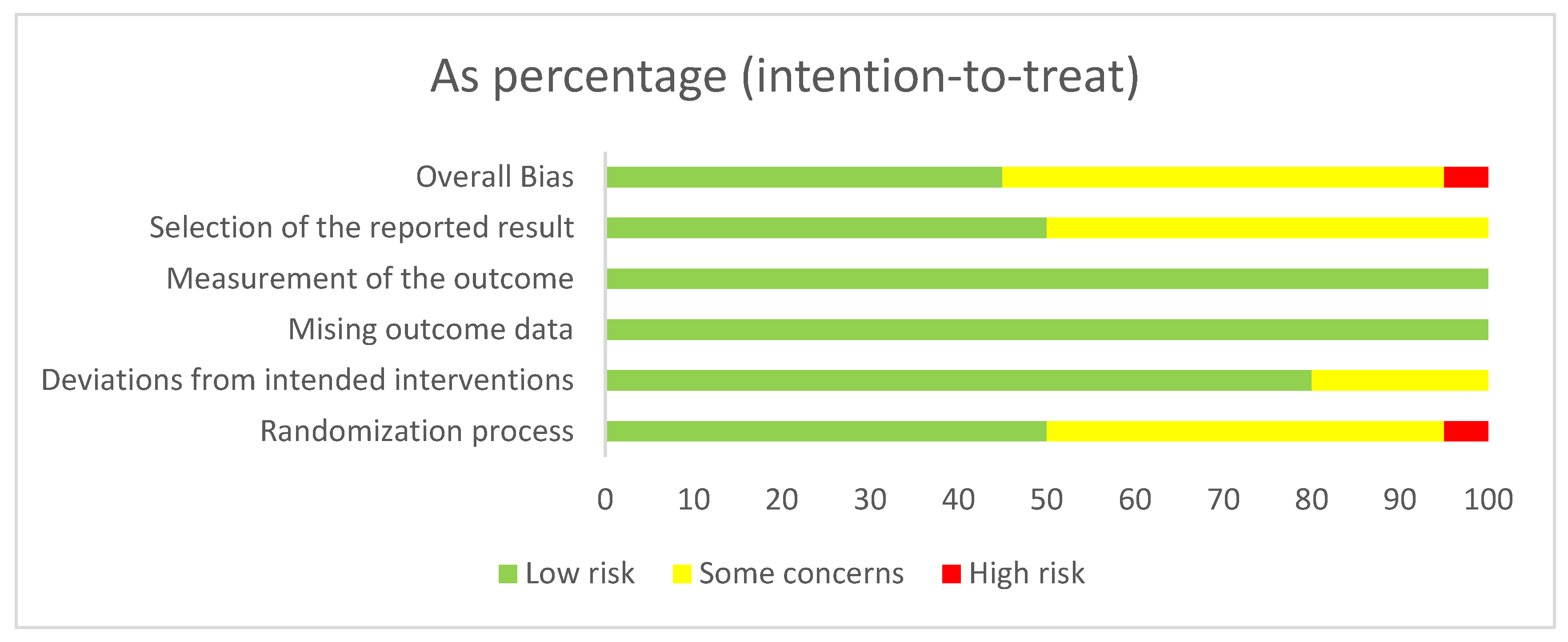
3.2. Risk of Bias, Certainty of Evidence, and Consistency
3.3. Muscle Strength
3.4. Physical Function
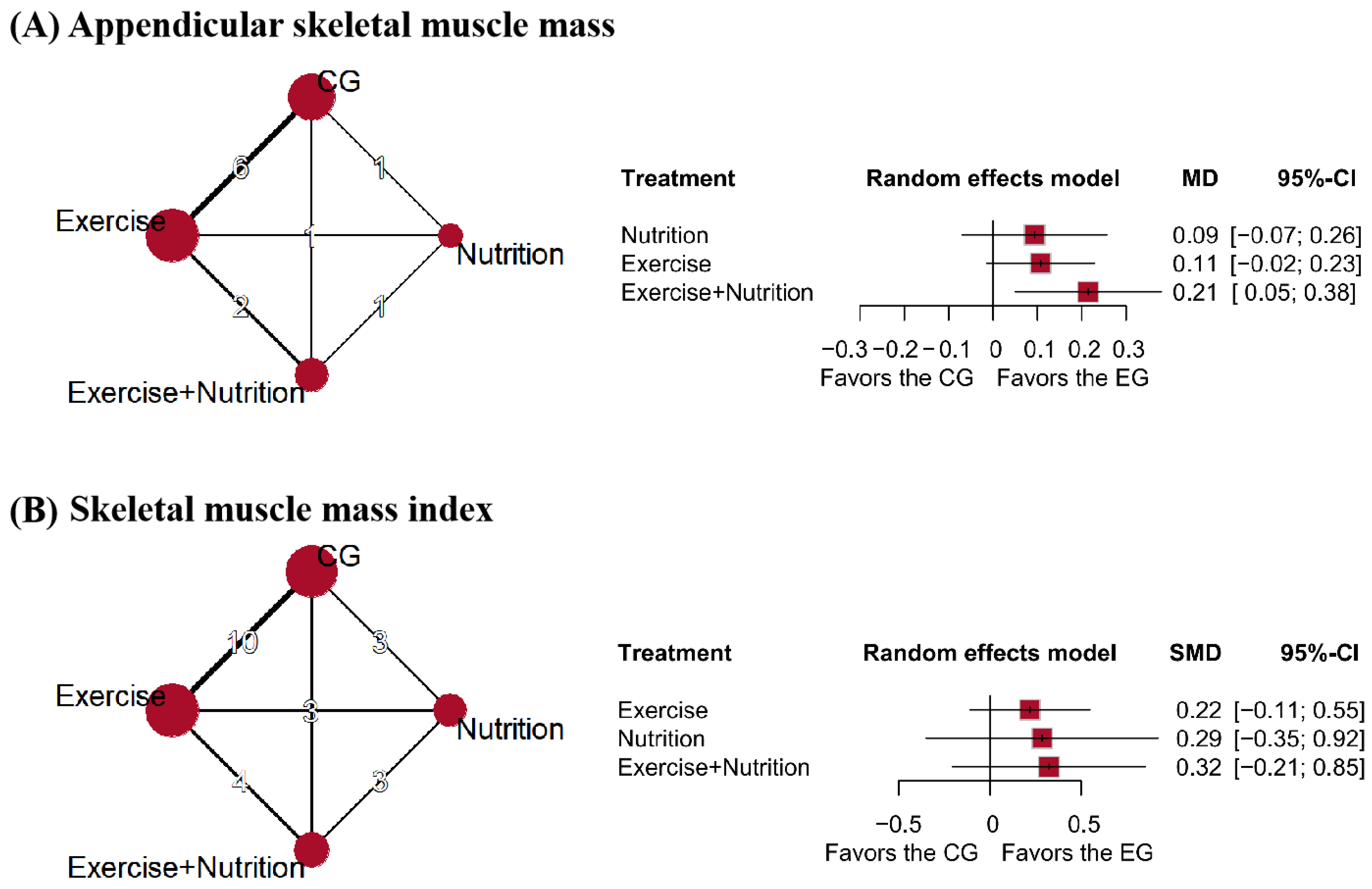
3.5. Muscle Mass
3.6. Subgroup Analysis
3.7. Sensitivity Analysis
4. Discussion
4.1. Main Findings
4.2. Comparison with Other Studies
4.3. Clinical Implications
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| RCTs | Randomized controlled trials |
| MD | Mean difference |
| SD | Standard deviations |
| SMD | Standardized Mean Difference |
| CI | Confidence interval |
| MID | Minimal important difference |
| SMI | Skeletal muscle mass index |
| ASM | Appendicular skeletal muscle mass |
| RT | Resistance training |
| RT + Nu | Resistance training and nutrition |
| RBT | Resistance balance training |
| ART | Aerobic resistance training |
References
- Yuan, S.; Larsson, S.C. Epidemiology of Sarcopenia: Prevalence, Risk Factors, and Consequences. Metabolism 2023, 144, 155533. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- PePetermann-Rocha, F.; Balntzi, V.; Gray, S.R.; Lara, J.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Global Prevalence of Sarcopenia and Severe Sarcopenia: A Systematic Review and Meta-Analysis. J. Cachexia Sarcopenia Muscle 2022, 13, 86–99. [Google Scholar] [CrossRef] [PubMed]
- Dennison, E.M.; Sayer, A.A.; Cooper, C. Epidemiology of Sarcopenia and Insight into Possible Therapeutic Targets. Nat. Rev. Rheumatol. 2017, 13, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Sayer, A.A.; Cooper, R.; Arai, H.; Cawthon, P.M.; Ntsama Essomba, M.-J.; Fielding, R.A.; Grounds, M.D.; Witham, M.D.; Cruz-Jentoft, A.J. Sarcopenia. Nat. Rev. Dis. Primers 2024, 10, 68. [Google Scholar] [CrossRef] [PubMed]
- Dent, E.; Morley, J.E.; Cruz-Jentoft, A.J.; Arai, H.; Kritchevsky, S.B.; Guralnik, J.; Bauer, J.M.; Pahor, M.; Clark, B.C.; Cesari, M.; et al. International Clinical Practice Guidelines for Sarcopenia (ICFSR): Screening, Diagnosis and Management. J. Nutr. Health Aging 2018, 22, 1148–1161. [Google Scholar] [CrossRef] [PubMed]
- Soares, W.J.S.; Lima, C.A.; Bilton, T.L.; Ferrioli, E.; Dias, R.C.; Perracini, M.R. Association among Measures of Mobility-Related Disability and Self-Perceived Fatigue among Older People: A Population-Based Study. Braz. J. Phys. Ther. 2015, 19, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Karabay, D.; Emük, Y.; Özer Kaya, D. Muscle Activity Ratios of Scapular Stabilizers during Closed Kinetic Chain Exercises in Healthy Shoulders: A Systematic Review. J. Sport. Rehabil. 2020, 29, 1001–1018. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Júnior, H.J.; Picca, A.; Calvani, R.; Marzetti, E. Prescription of Resistance Training for Sarcopenic Older Adults: Does It Require Specific Attention? Ageing Res. Rev. 2022, 81, 101720. [Google Scholar] [CrossRef] [PubMed]
- Dodds, R.M.; Granic, A.; Robinson, S.M.; Sayer, A.A. Sarcopenia, Long-Term Conditions, and Multimorbidity: Findings from UK Biobank Participants. J. Cachexia Sarcopenia Muscle 2020, 11, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Shi, Q.; Nong, K.; Li, S.; Yue, J.; Huang, J.; Dong, B.; Beauchamp, M.; Hao, Q. Exercise for Sarcopenia in Older People: A Systematic Review and Network Meta-analysis. J. Cachexia Sarcopenia Muscle 2023, 14, 1199–1211. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-K.; Lee, W.-J.; Peng, L.-N.; Liu, L.-K.; Arai, H.; Akishita, M.; Asian Working Group for Sarcopenia. Recent Advances in Sarcopenia Research in Asia: 2016 Update from the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2016, 17, 767.e1–767.e7. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, Y.; Wakabayashi, H.; Yamada, M.; Kim, H.; Harada, A.; Arai, H. Interventions for Treating Sarcopenia: A Systematic Review and Meta-Analysis of Randomized Controlled Studies. J. Am. Med. Dir. Assoc. 2017, 18, 553.e1–553.e16. [Google Scholar] [CrossRef] [PubMed]
- Prokopidis, K.; Giannos, P.; Katsikas Triantafyllidis, K.; Kechagias, K.S.; Mesinovic, J.; Witard, O.C.; Scott, D. Effect of Vitamin D Monotherapy on Indices of Sarcopenia in Community-dwelling Older Adults: A Systematic Review and Meta-analysis. J. Cachexia Sarcopenia Muscle 2022, 13, 1642–1652. [Google Scholar] [CrossRef] [PubMed]
- Papanicolaou, D.A.; Ather, S.N.; Zhu, H.; Zhou, Y.; Lutkiewicz, J.; Scott, B.B.; Chandler, J. A Phase IIA Randomized, Placebo-Controlled Clinical Trial to Study the Efficacy and Safety of the Selective Androgen Receptor Modulator (SARM), MK-0773 in Female Participants with Sarcopenia. J. Nutr. Health Aging 2013, 17, 533–543. [Google Scholar] [CrossRef] [PubMed]
- Garcia, J.M.; Boccia, R.V.; Graham, C.D.; Yan, Y.; Duus, E.M.; Allen, S.; Friend, J. Anamorelin for Patients with Cancer Cachexia: An Integrated Analysis of Two Phase 2, Randomised, Placebo-Controlled, Double-Blind Trials. Lancet Oncol. 2015, 16, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E. Pharmacologic Options for the Treatment of Sarcopenia. Calcif. Tissue Int. 2016, 98, 319–333. [Google Scholar] [CrossRef] [PubMed]
- Qiu, W.; Cai, A.; Li, L.; Feng, Y. Trend in Prevalence, Associated Risk Factors, and Longitudinal Outcomes of Sarcopenia in China: A National Cohort Study. J. Intern. Med. 2024, 296, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Heymsfield, S.B.; Wang, Z.M.; Ross, R. Skeletal Muscle Mass and Distribution in 468 Men and Women Aged 18–88 Yr. J. Appl. Physiol. (1985) 2000, 89, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Tankó, L.B.; Movsesyan, L.; Mouritzen, U.; Christiansen, C.; Svendsen, O.L. Appendicular Lean Tissue Mass and the Prevalence of Sarcopenia among Healthy Women. Metabolism 2002, 51, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Collins, B.C.; Laakkonen, E.K.; Lowe, D.A. Aging of the Musculoskeletal System: How the Loss of Estrogen Impacts Muscle Strength. Bone 2019, 123, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Juppi, H.-K.; Sipilä, S.; Cronin, N.J.; Karvinen, S.; Karppinen, J.E.; Tammelin, T.H.; Aukee, P.; Kovanen, V.; Kujala, U.M.; Laakkonen, E.K. Role of Menopausal Transition and Physical Activity in Loss of Lean and Muscle Mass: A Follow-Up Study in Middle-Aged Finnish Women. J. Clin. Med. 2020, 9, 1588. [Google Scholar] [CrossRef] [PubMed]
- Payette, H.; Roubenoff, R.; Jacques, P.F.; Dinarello, C.A.; Wilson, P.W.F.; Abad, L.W.; Harris, T. Insulin-like Growth Factor-1 and Interleukin 6 Predict Sarcopenia in Very Old Community-Living Men and Women: The Framingham Heart Study. J. Am. Geriatr. Soc. 2003, 51, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Cheng, R.; Maloney, A.; Moran, J.; Newman, T.H.; Gardner, E.C. Resistance Training as Treatment for Sarcopenia: Examining Sex-Related Differences in Physiology and Response. Clin. Ther. 2022, 44, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zou, L.; Chen, S.-T.; Bae, J.H.; Kim, D.Y.; Liu, X.; Song, W. Effects and Moderators of Exercise on Sarcopenic Components in Sarcopenic Elderly: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 649748. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.-W.; Tan, H.-L.; Hsu, M.-F.; Huang, H.-L.; Chung, Y.-C. Effect of Non-Pharmacological Interventions on the Prevention of Sarcopenia in Menopausal Women: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. BMC Womens Health 2023, 23, 606. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-M.; Kim, Y.-H.; Lee, S.-Y.; Kim, A.-J. Effect Size of Dietary Supplementation and Physical Exercise Interventions for Sarcopenia in Middle-Aged Women. Prev. Nutr. Food Sci. 2021, 26, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-Analyses of Health Care Interventions: Checklist and Explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2008; Available online: http://www.cochrane-handbook.org (accessed on 1 June 2025).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Nikolakopoulou, A.; Higgins, J.P.T.; Papakonstantinou, T.; Chaimani, A.; Del Giovane, C.; Egger, M.; Salanti, G. CINeMA: An Approach for Assessing Confidence in the Results of a Network Meta-Analysis. PLoS Med. 2020, 17, e1003082. [Google Scholar] [CrossRef] [PubMed]
- Papakonstantinou, T.; Nikolakopoulou, A.; Higgins, J.P.T.; Egger, M.; Salanti, G. CINeMA: Software for Semiautomated Assessment of the Confidence in the Results of Network Meta-Analysis. Campbell Syst. Rev. 2020, 16, e1080. [Google Scholar] [CrossRef] [PubMed]
- Brignardello-Petersen, R.; Izcovich, A.; Rochwerg, B.; Florez, I.D.; Hazlewood, G.; Alhazanni, W.; Yepes-Nuñez, J.; Santesso, N.; Guyatt, G.H.; Schünemann, H.J. GRADE Approach to Drawing Conclusions from a Network Meta-Analysis Using a Partially Contextualised Framework. BMJ 2020, 371, m3907. [Google Scholar] [CrossRef] [PubMed]
- The GRADE Working Group. Clarifies the Construct of Certainty of Evidence. J. Clin. Epidemiol. 2017, 87, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Zeng, L.; Brignardello-Petersen, R.; Hultcrantz, M.; Siemieniuk, R.A.; Santesso, N.; Traversy, G.; Izcovich, A.; Sadeghirad, B.; Alexander, P.E.; Devji, T.; et al. GRADE Guidelines 32: GRADE Offers Guidance on Choosing Targets of GRADE Certainty of Evidence Ratings. J. Clin. Epidemiol. 2021, 137, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Minimal Clinically Important Difference for Grip Strength: A Systematic Review. J. Phys. Ther. Sci. 2019, 31, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Bobos, P.; Nazari, G.; Lu, Z.; MacDermid, J.C. Measurement Properties of the Hand Grip Strength Assessment: A Systematic Review with Meta-Analysis. Arch. Phys. Med. Rehabil. 2020, 101, 553–565. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Glenney, S.S. Minimal Clinically Important Difference for Change in Comfortable Gait Speed of Adults with Pathology: A Systematic Review. J. Eval. Clin. Pract. 2014, 20, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Welton, N.J.; Sutton, A.J.; Cooper, N.; Abrams, K.R.; Ades, A.E. Evidence Synthesis for Decision Making in Healthcare; John Wiley & Sons: Hoboken, NJ, USA, 2012; Volume 132, ISBN 0-470-06109-X. [Google Scholar]
- Mavridis, D.; Salanti, G. A Practical Introduction to Multivariate Meta-Analysis. Stat. Methods Med. Res. 2013, 22, 133–158. [Google Scholar] [CrossRef] [PubMed]
- Dias, S.; Welton, N.J.; Sutton, A.J.; Caldwell, D.M.; Lu, G.; Ades, A.E. Evidence Synthesis for Decision Making 4: Inconsistency in Networks of Evidence Based on Randomized Controlled Trials. Med. Decis. Mak. Int. J. Soc. Med. Decis. Mak. 2013, 33, 641–656. [Google Scholar] [CrossRef] [PubMed]
- Mbuagbaw, L.; Rochwerg, B.; Jaeschke, R.; Heels-Andsell, D.; Alhazzani, W.; Thabane, L.; Guyatt, G.H. Approaches to Interpreting and Choosing the Best Treatments in Network Meta-Analyses. Syst. Rev. 2017, 6, 79. [Google Scholar] [CrossRef] [PubMed]
- Veroniki, A.A.; Straus, S.E.; Fyraridis, A.; Tricco, A.C. The Rank-Heat Plot Is a Novel Way to Present the Results from a Network Meta-Analysis Including Multiple Outcomes. J. Clin. Epidemiol. 2016, 76, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-T.; Wu, H.-J.; Chen, Y.-J.; Ho, S.-Y.; Chung, Y.-C. Effects of 8-Week Kettlebell Training on Body Composition, Muscle Strength, Pulmonary Function, and Chronic Low-Grade Inflammation in Elderly Women with Sarcopenia. Exp. Gerontol. 2018, 112, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Chen, Y.; Shin, S.; Jie, C.; Chang, Z.; Ding, H.; Yang, H. Effect of a Moderate-Intensity Comprehensive Exercise Program on Body Composition, Muscle Strength, and Physical Performance in Elderly Females with Sarcopenia. Heliyon 2023, 9, e18951. [Google Scholar] [CrossRef] [PubMed]
- Dieli-Conwright, C.M.; Courneya, K.S.; Demark-Wahnefried, W.; Sami, N.; Lee, K.; Buchanan, T.A.; Spicer, D.V.; Tripathy, D.; Bernstein, L.; Mortimer, J.E. Effects of Aerobic and Resistance Exercise on Metabolic Syndrome, Sarcopenic Obesity, and Circulating Biomarkers in Overweight or Obese Survivors of Breast Cancer: A Randomized Controlled Trial. JCO 2018, 36, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Gad, M.G.E.-H.I.; El-Hak, S.E.-B.; El-SayedEl-Mekawy, H.; Moustafa, M.H. Efficacy of Aerobic and Core Exercise Training on Improving Muscle Mass and Physical Performance in Postmenopausal Women with Sarcopenic Obesity. J. Cardiovasc. Dis. Res. 2021, 12, 802–813. [Google Scholar]
- Huang, S.-W.; Ku, J.-W.; Lin, L.-F.; Liao, C.-D.; Chou, L.-C.; Liou, T.-H. Body Composition Influenced by Progressive Elastic Band Resistance Exercise of Sarcopenic Obesity Elderly Women: A Pilot Randomized Controlled Trial. Eur. J. Phys. Rehabil. Med. 2017, 53, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.-S.; Ahn, H.; Kim, S.-W.; Park, H.-Y. Effects of 12-Week Circuit Exercise Intervention on Blood Pressure, Vascular Function, and Inflammatory Cytokines in Obese Older Women with Sarcopenia. Rev. Cardiovasc. Med. 2024, 25, 185. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.K.; Suzuki, T.; Saito, K.; Yoshida, H.; Kobayashi, H.; Kato, H.; Katayama, M. Effects of Exercise and Amino Acid Supplementation on Body Composition and Physical Function in Community-dwelling Elderly Japanese Sarcopenic Women: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2012, 60, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Suzuki, T.; Saito, K.; Yoshida, H.; Kojima, N.; Kim, M.; Sudo, M.; Yamashiro, Y.; Tokimitsu, I. Effects of Exercise and Tea Catechins on Muscle Mass, Strength and Walking Ability in Community-dwelling Elderly Japanese Sarcopenic Women: A Randomized Controlled Trial. Geriatr. Gerontol. Int. 2013, 13, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, M.; Kojima, N.; Fujino, K.; Hosoi, E.; Kobayashi, H.; Somekawa, S.; Niki, Y.; Yamashiro, Y.; Yoshida, H. Exercise and Nutritional Supplementation on Community-Dwelling Elderly Japanese Women with Sarcopenic Obesity: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2016, 17, 1011–1019. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-H.; Lee, P.-H.; Lin, L.-F.; Liao, C.-D.; Liou, T.-H.; Huang, S.-W. Effects of Progressive Elastic Band Resistance Exercise for Aged Osteosarcopenic Adiposity Women. Exp. Gerontol. 2021, 147, 111272. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.-D.; Tsauo, J.-Y.; Lin, L.-F.; Huang, S.-W.; Ku, J.-W.; Chou, L.-C.; Liou, T.-H. Effects of Elastic Resistance Exercise on Body Composition and Physical Capacity in Older Women with Sarcopenic Obesity: A CONSORT-Compliant Prospective Randomized Controlled Trial. Medicine 2017, 96, e7115. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.-D.; Tsauo, J.-Y.; Huang, S.-W.; Ku, J.-W.; Hsiao, D.-J.; Liou, T.-H. Effects of Elastic Band Exercise on Lean Mass and Physical Capacity in Older Women with Sarcopenic Obesity: A Randomized Controlled Trial. Sci. Rep. 2018, 8, 2317. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.-D.; Liao, Y.-H.; Liou, T.-H.; Hsieh, C.-Y.; Kuo, Y.-C.; Chen, H.-C. Effects of Protein-Rich Nutritional Composition Supplementation on Sarcopenia Indices and Physical Activity during Resistance Exercise Training in Older Women with Knee Osteoarthritis. Nutrients 2021, 13, 2487. [Google Scholar] [CrossRef] [PubMed]
- Nabuco, H.C.G.; Tomeleri, C.M.; Fernandes, R.R.; Sugihara Junior, P.; Cavalcante, E.F.; Cunha, P.M.; Antunes, M.; Nunes, J.P.; Venturini, D.; Barbosa, D.S.; et al. Effect of Whey Protein Supplementation Combined with Resistance Training on Body Composition, Muscular Strength, Functional Capacity, and Plasma-Metabolism Biomarkers in Older Women with Sarcopenic Obesity: A Randomized, Double-Blind, Placebo-Controlled Trial. Clin. Nutr. ESPEN 2019, 32, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Osuka, Y.; Kojima, N.; Sasai, H.; Wakaba, K.; Miyauchi, D.; Tanaka, K.; Kim, H. Effects of Exercise and/or β-Hydroxy-β-Methylbutyrate Supplementation on Muscle Mass, Muscle Strength, and Physical Performance in Older Women with Low Muscle Mass: A Randomized, Double-Blind, Placebo-Controlled Trial. Am. J. Clin. Nutr. 2021, 114, 1371–1385. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kwon, Y.; Park, H. Effects of 24-Week Aerobic and Resistance Training on Carotid Artery Intima-Media Thickness and Flow Velocity in Elderly Women with Sarcopenic Obesity. J. Atheroscler. Thromb. 2017, 24, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Flor-Rufino, C.; Barrachina-Igual, J.; Pérez-Ros, P.; Pablos-Monzó, A.; Sanz-Requena, R.; Martínez-Arnau, F.M. Fat Infiltration and Muscle Hydration Improve after High-Intensity Resistance Training in Women with Sarcopenia. A Randomized Clinical Trial. Maturitas 2023, 168, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Sammarco, R.; Marra, M.; Di Guglielmo, M.L.; Naccarato, M.; Contaldo, F.; Poggiogalle, E.; Donini, L.M.; Pasanisi, F. Evaluation of Hypocaloric Diet with Protein Supplementation in Middle-Aged Sarcopenic Obese Women: A Pilot Study. Obes. Facts 2017, 10, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Seo, M.-W.; Jung, S.-W.; Kim, S.-W.; Lee, J.-M.; Jung, H.C.; Song, J.-K. Effects of 16 Weeks of Resistance Training on Muscle Quality and Muscle Growth Factors in Older Adult Women with Sarcopenia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 6762. [Google Scholar] [CrossRef] [PubMed]
- Valdés-Badilla, P.; Guzmán-Muñoz, E.; Hernandez-Martinez, J.; Núñez-Espinosa, C.; Delgado-Floody, P.; Herrera-Valenzuela, T.; Branco, B.H.M.; Zapata-Bastias, J.; Nobari, H. Effectiveness of Elastic Band Training and Group-Based Dance on Physical-Functional Performance in Older Women with Sarcopenia: A Pilot Study. BMC Public Health 2023, 23, 2113. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, K.S.S.; Dias, J.M.D.; Araújo, M.C.; Pinheiro, A.C.; Moreira, B.S.; Dias, R.C. Effects of a Progressive Resistance Exercise Program with High-Speed Component on the Physical Function of Older Women with Sarcopenic Obesity: A Randomized Controlled Trial. Braz. J. Phys. Ther. 2016, 20, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Huang, W.Y.; Zhao, Y. Efficacy of Exercise on Muscle Function and Physical Performance in Older Adults with Sarcopenia: An Updated Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 8212. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.-Y.; Huang, K.-S.; Chen, K.-M.; Chou, C.-P.; Tu, Y.-K. Exercise, Nutrition, and Combined Exercise and Nutrition in Older Adults with Sarcopenia: A Systematic Review and Network Meta-Analysis. Maturitas 2021, 145, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.-D.; Chen, H.-C.; Huang, S.-W.; Liou, T.-H. The Role of Muscle Mass Gain Following Protein Supplementation plus Exercise Therapy in Older Adults with Sarcopenia and Frailty Risks: A Systematic Review and Meta-Regression Analysis of Randomized Trials. Nutrients 2019, 11, 1713. [Google Scholar] [CrossRef] [PubMed]
- Luo, D.; Lin, Z.; Li, S.; Liu, S.-J. Effect of Nutritional Supplement Combined with Exercise Intervention on Sarcopenia in the Elderly: A Meta-Analysis. Int. J. Nurs. Sci. 2017, 4, 389–401. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.-D.; Tsauo, J.-Y.; Wu, Y.-T.; Cheng, C.-P.; Chen, H.-C.; Huang, Y.-C.; Chen, H.-C.; Liou, T.-H. Effects of Protein Supplementation Combined with Resistance Exercise on Body Composition and Physical Function in Older Adults: A Systematic Review and Meta-Analysis. Am. J. Clin. Nutr. 2017, 106, 1078–1091. [Google Scholar] [CrossRef] [PubMed]
- Cuyul-Vásquez, I.; Pezo-Navarrete, J.; Vargas-Arriagada, C.; Ortega-Díaz, C.; Sepúlveda-Loyola, W.; Hirabara, S.M.; Marzuca-Nassr, G.N. Effectiveness of Whey Protein Supplementation during Resistance Exercise Training on Skeletal Muscle Mass and Strength in Older People with Sarcopenia: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 3424. [Google Scholar] [CrossRef] [PubMed]
- Nasimi, N.; Sohrabi, Z.; Nunes, E.A.; Sadeghi, E.; Jamshidi, S.; Gholami, Z.; Akbarzadeh, M.; Faghih, S.; Akhlaghi, M.; Phillips, S.M. Whey Protein Supplementation with or without Vitamin D on Sarcopenia-Related Measures: A Systematic Review and Meta-Analysis. Adv. Nutr. 2023, 14, 762–773. [Google Scholar] [CrossRef] [PubMed]
- Li, M.-L.; Zhang, F.; Luo, H.-Y.; Quan, Z.-W.; Wang, Y.-F.; Huang, L.-T.; Wang, J.-H. Improving Sarcopenia in Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials of Whey Protein Supplementation with or without Resistance Training. J. Nutr. Health Aging 2024, 28, 100184. [Google Scholar] [CrossRef] [PubMed]
- Kamińska, M.S.; Rachubińska, K.; Grochans, S.; Skonieczna-Żydecka, K.; Cybulska, A.M.; Grochans, E.; Karakiewicz, B. The Impact of Whey Protein Supplementation on Sarcopenia Progression among the Elderly: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 2039. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, Y.; Matsumoto, A.; Inoue, T.; Okamura, M.; Kuzuya, M. Protein Supplementation Alone or Combined with Exercise for Sarcopenia and Physical Frailty: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Arch. Gerontol. Geriatr. 2025, 131, 105783. [Google Scholar] [CrossRef] [PubMed]
- Negm, A.M.; Lee, J.; Hamidian, R.; Jones, C.A.; Khadaroo, R.G. Management of Sarcopenia: A Network Meta-Analysis of Randomized Controlled Trials. J. Am. Med. Dir. Assoc. 2022, 23, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Markofski, M.; Volpi, E. Protein Metabolism in Women and Men: Similarities and Disparities. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Berner, L.; Becker, G.; Wise, M.; Doi, J. Characterization of Dietary Protein among Older Adults in the United States: Amount, Animal Sources, and Meal Patterns. J. Acad. Nutr. Diet. 2013, 113, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Gui, Q.; Chen, L.; Xu, K.; Xu, Z. Associations between Dietary Protein and Vitamin Intake and the Physical Functioning of Older Adults with Sarcopenia. Eur. Geriatr. Med. 2018, 9, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.-Y.; Chang, H.; Huang, Y.-C.; Liu, C.-W. Effect of Whey Protein Supplementation in Postmenopausal Women: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 4210. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Intervention | Age (Mean ± SD) | Sample Size | Duration (Weeks) | Detailed Intervention Description | Diagnostic Criteria | Country | Setting |
|---|---|---|---|---|---|---|---|---|
| Chen et al., 2018 [46] | Exercise | 66.7 ± 5.3 | 17 | 8 | Twice-weekly kettlebell training | AWGS | China | Community |
| CG | 68.3 ± 2.8 | 16 | 8 | Maintained daily routine activities without structured intervention | AWGS | China | Community | |
| Chen et al., 2023 [47] | Exercise | 65.68 ± 2.5 | 25 | 8 | Combined Tai Chi and resistance band training, performed three times per week | AWGS | China | Community |
| CG | 65.21 ± 2.6 | 24 | 8 | Received health education only | AWGS | China | Community | |
| Dieli-Conwright et al., 2018 [48] | Exercise | 52.8 ± 10.6 | 50 | 16 | Supervised combined aerobic and resistance exercise program, performed three times per week | AWGS | USA | Institution |
| CG | 53.6 ± 10.1 | 50 | 16 | Maintained habitual lifestyle without additional intervention | AWGS | USA | Institution | |
| El-Hak et al., 2021 [49] | Exercise | 58.15 ± 3.06 | 20 | 12 | Walking exercise performed three times per week | EWGSOP | Egypt | Institution |
| Exercise | 58.30 ± 2.81 | 20 | 12 | Core muscle training and walking exercise, both performed three times per week | EWGSOP | Egypt | Institution | |
| Huang et al., 2017 [50] | Exercise | 68.89 ± 4.91 | 18 | 12 | Progressive resistance training program using elastic bands | Study-defined criteria | China | Community |
| CG | 68.89 ± 4.91 | 17 | 12 | Received health education only | Study-defined criteria | China | Community | |
| Jung et al., 2024 [51] | Exercise | 78.14 ± 3.72 | 14 | 12 | Circuit training performed three times per week | AWGS | Korea | Community |
| CG | 78.21 ± 3.72 | 14 | 12 | Maintained regular daily activities | AWGS | Korea | Community | |
| Kim et al., 2012 [52] | Exercise + Nutrition | 79.5 ± 2.9 | 38 | 12 | Resistance plus balance training (twice weekly) combined with twice-daily supplementation of 3 g leucine-rich essential amino acids (6 g/day total) | Study-defined criteria | Japan | Community |
| Nutrition | 79.2 ± 2.8 | 39 | 12 | Supplementation with 3 g leucine-rich essential amino acids, twice daily (6 g/day total) | Study-defined criteria | Japan | Community | |
| Exercise | 79.0 ± 2.9 | 39 | 12 | Resistance plus balance training performed twice weekly | Study-defined criteria | Japan | Community | |
| CG | 78.7 ± 2.8 | 39 | 12 | Received health education only | Study-defined criteria | Japan | Community | |
| Kim et al., 2013 [53] | Exercise | 79.6 ± 4.2 | 32 | 12 | Same as above (resistance + balance training) | Study-defined criteria | Japan | Community |
| CG | 80.2 ± 5.6 | 32 | 12 | Received health education only | Study-defined criteria | Japan | Community | |
| Kim et al., 2016 [54] | Exercise + Nutrition | 80.9 ± 4.2 | 36 | 12 | Resistance and aerobic training (twice weekly) combined with essential amino acid supplementation (3 g/dose, twice daily, 6 g/day total) | Study-defined criteria | Japan | Community |
| Exercise | 81.4 ± 4.3 | 35 | 12 | Resistance and aerobic training performed twice weekly | Study-defined criteria | Japan | Community | |
| Nutrition | 81.2 ± 4.9 | 34 | 12 | Supplementation with essential amino acids (3 g/dose, twice daily, 6 g/day total) | Study-defined criteria | Japan | Community | |
| CG | 81.1 ± 5.1 | 34 | 12 | Received health education only | Study-defined criteria | Japan | Community | |
| Lee et al., 2021 [55] | Exercise | 70.13 ± 4.51 | 15 | 12 | Progressive elastic resistance band training performed three times per week | EWGSOP | China | Community |
| CG | 71.82 ± 5.33 | 12 | 12 | Maintained usual daily activities | EWGSOP | China | Community | |
| Liao et al., 2017 [56] | Exercise | 68.42 ± 5.86 | 25 | 12 | Elastic resistance band training | EWGSOP | China | Institution |
| CG | 66.39 ± 4.49 | 21 | 12 | Maintained daily activity | EWGSOP | China | Institution | |
| Liao et al., 2018 [57] | Exercise | 66.67 ± 4.54 | 33 | 12 | Elastic resistance band training | Study-defined criteria | China | Institution |
| CG | 68.32 ± 6.05 | 23 | 12 | Maintained daily activity | Study-defined criteria | China | Institution | |
| Liao et al., 2021 [58] | Exercise | 69.81 ± 7.24 | 36 | 12 | Elastic resistance band training twice weekly | AWGS | China | Institution |
| Exercise + Nutrition | 68.64 ± 7.42 | 36 | 12 | Elastic resistance band training twice weekly combined with daily protein supplement (24.2 g/day: 11 g plant oligopeptides, 4 g casein peptides, 5 g BCAA), taken in two divided doses | AWGS | China | Institution | |
| Nabuco et al., 2019 [59] | Exercise + Nutrition | 68.0 ± 4.2 | 13 | 12 | Daily supplementation with 35 g whey protein combined with resistance training three times per week | FNIH | Brazil | Community |
| Exercise | 70.1 ± 3.9 | 13 | 12 | Daily placebo supplementation combined with the same resistance training protocol | FNIH | Brazil | Community | |
| Osuka et al., 2021 [60] | Exercise + Nutrition | 73.5 ± 4.2 | 36 | 12 | Resistance training performed twice weekly combined with daily 1500 mg Ca-HMB supplementation | AWGS | Japan | Institution |
| Exercise | 71.8 ± 4.1 | 38 | 12 | Resistance training performed twice per week | AWGS | Japan | Institution | |
| Nutrition | 71.5 ± 4.5 | 37 | 12 | Daily supplementation with 1500 mg Ca-HMB | AWGS | Japan | Institution | |
| CG | 71.6 ± 4.2 | 38 | 12 | Health education plus placebo supplementation | AWGS | Japan | Institution | |
| Park et al., 2017 [61] | CG | 74.7 ± 5.1 | 25 | 26 | Health education only | Study-defined criteria | Korea | Community |
| Exercise | 73.5 ± 7.1 | 25 | 26 | Combined aerobic and resistance training conducted five times per week | Study-defined criteria | Korea | Community | |
| Rufino et al., 2023 [62] | Exercise | 79.9 ± 7.2 | 20 | 26 | High-intensity resistance training | EWGSOP | Spain | Community |
| CG | 79.6 ± 7.7 | 18 | 26 | Maintained usual activity | EWGSOP | Spain | Community | |
| Sammarco et al., 2017 [63] | CG | 58 ± 10 | 9 | 16 | Low-calorie placebo supplement | Study-defined criteria | Italy | Institution |
| Nutrition | 53 ± 8.9 | 9 | 16 | Low-calorie, high-protein diet providing 1.2–1.4 g/kg/day of protein | Study-defined criteria | Italy | Institution | |
| Seo et al., 2021 [64] | Exercise | 70.3 ± 5.38 | 12 | 16 | Bodyweight and resistance band exercises, three times per week | EWGSOP | Korea | Institution |
| CG | 72.9 ± 4.75 | 10 | 16 | Maintained usual activity | EWGSOP | Korea | Institution | |
| Valdés-Badilla et al., 2023 [65] | Exercise | 73.91 ± 8.27 | 21 | 12 | Progressive resistance band training, three times per week | EWGSOP | Chile | Community |
| Exercise | 72.85 ± 8.67 | 19 | 12 | Structured group dance program, three times per week | EWGSOP | Chile | Community | |
| Vasconcelos et al., 2016 [66] | Exercise | 72 ± 4.6 | 14 | 10 | Lower limb progressive resistance training, 2–3 times/week | Study-defined criteria | Brazil | Community |
| CG | 72 ± 3.6 | 14 | 10 | Maintained daily activities | Study-defined criteria | Brazil | Community |
| Outcome | Certainty of Evidence | Group | Intervention | Intervention vs. Control | SUCRA |
|---|---|---|---|---|---|
| Handgrip strength | Low certainty (low to very low certainty evidence) | Category 2: among the most effective | Exercise + Nutrition | 1.95 (0.10; 3.81) | 74 |
| Exercise | 1.85 (0.86; 2.85) | 71.8 | |||
| Category 0: among the least effective | Nutrition | 1.42 (−0.22; 3.05) | 52.05 | ||
| Knee extension strength | Low certainty (low to very low certainty evidence) | Category 2: among the most effective | Exercise | 0.75 (0.41; 1.08) | 84.58 |
| Exercise + Nutrition | 0.71 (0.28; 1.14) | 78.81 | |||
| Category 0: among the least effective | Nutrition | 0.34 (−0.11; 0.79) | 34.3 | ||
| Usual gait speed | Low certainty (low to very low certainty evidence) | Category 2: among the most effective | Exercise + Nutrition | 0.11 (0.04; 0.17) | 94.49 |
| Exercise | 0.08 (0.03; 0.12) | 72.12 | |||
| Category 0: among the least effective | Nutrition | −0.04 (−0.11; 0.03) | 5.11 | ||
| Maximal gait speed | Low certainty (low to very low certainty evidence) | Category 2: among the most effective | Exercise + Nutrition | 0.22 (0.06; 0.38) | 82.17 |
| Exercise | 0.21 (0.09; 0.33) | 79.37 | |||
| Category 0: among the least effective | Nutrition | 0.09 (−0.06; 0.25) | 34.12 | ||
| Appendicular skeletal muscle mass | High certainty (moderate to high certainty evidence) | Category 2: among the most effective | Exercise + Nutrition | 0.21 (0.05; 0.38) | 92.83 |
| Low certainty (low to very low certainty evidence) | Category 1: intermediately effective | Exercise | 0.11 (−0.02; 0.23) | 54.04 | |
| Category 0: among the least effective | Nutrition | 0.09 (−0.07; 0.26) | 47.14 | ||
| Skeletal muscle mass index | Low certainty (low to very low certainty evidence) | Category 0: among the least effective | Exercise + Nutrition | 0.32 (−0.21; 0.85) | 69.75 |
| Nutrition | 0.29 (−0.35; 0.92) | 61.71 | |||
| Exercise | 0.22 (−0.11; 0.55) | 55.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yan, R.; Huang, W.; Zhong, Y.; Du, X. Comparative Effectiveness of Exercise, Protein Supplementation, and Combined Interventions for Sarcopenia Management in Women: A Network Meta-Analysis. Nutrients 2025, 17, 2392. https://doi.org/10.3390/nu17152392
Yan R, Huang W, Zhong Y, Du X. Comparative Effectiveness of Exercise, Protein Supplementation, and Combined Interventions for Sarcopenia Management in Women: A Network Meta-Analysis. Nutrients. 2025; 17(15):2392. https://doi.org/10.3390/nu17152392
Chicago/Turabian StyleYan, Ruixiang, Wenrui Huang, Yuanhao Zhong, and Xuelian Du. 2025. "Comparative Effectiveness of Exercise, Protein Supplementation, and Combined Interventions for Sarcopenia Management in Women: A Network Meta-Analysis" Nutrients 17, no. 15: 2392. https://doi.org/10.3390/nu17152392
APA StyleYan, R., Huang, W., Zhong, Y., & Du, X. (2025). Comparative Effectiveness of Exercise, Protein Supplementation, and Combined Interventions for Sarcopenia Management in Women: A Network Meta-Analysis. Nutrients, 17(15), 2392. https://doi.org/10.3390/nu17152392