

Belgian Case Series Identifies Non-Cow Mammalian Milk Allergy as a Rare, Severe, Selective, and Late-Onset Condition

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Design
- 13 patients with confirmed CMA, including two with concomitant goat’s milk allergy;
- 6 patients sensitized to cow’s milk but clinically tolerant;
- 3 patients with selective non-cow mammalian milk allergy.
2.2. Non-Cow Mammalian Milk Allergy Cases
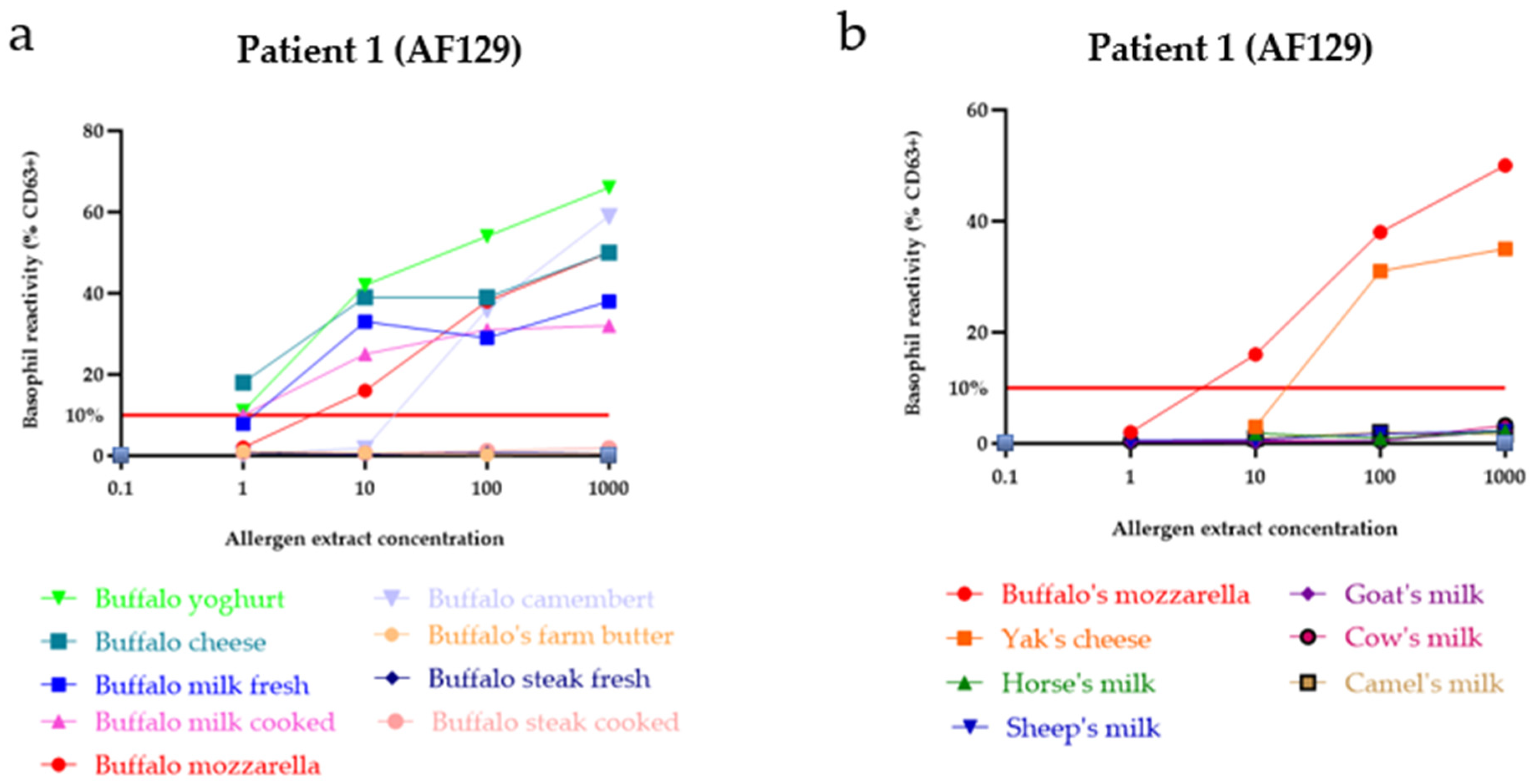
- Patient 1 (AF129), a 48-year-old female with buffalo milk allergy;
- Patient 2 (AF220), a 31-year-old female with mare milk allergy;
- Patient 3 (HV206), a 62-year-old female with mare milk allergy.
2.3. Skin Prick Test
2.4. Total and Specific IgE Determination
2.5. Preparation of Extracts
2.6. Sodium Dodecylsulfate-Polyacrylamide Gel Electrophoresis (SDS-PAGE)
2.7. Immunoblotting
2.8. Basophil Activation Test (BAT)
2.9. ImmunoCAP™ Assay with Biotinylated Buffalo’s Cheese Proteins
2.10. ImmunoCAP™ Inhibition-Assay
2.11. Comprehensive Overview of the Literature on Non-Cow Mammalian Milk Allergy
2.12. Statistical Analysis
3. Results
3.1. Patient Characteristics and Allergy Testing
3.1.1. Patient Characteristics
3.1.2. Allergy Testing: Skin Prick Test, Total and Specific IgE Determination
3.2. Allergen Identification in Non-Cow Mammalian Milk Allergy
3.3. Patient Reactivity
3.3.1. Immunoblotting
3.3.2. BAT Reflecting Outcomes of Oral Food Provocation
3.3.3. Quantification of sIgE to Buffalo’s Cheese Proteins
3.4. Potential Cross-Reactivity of Proteins
3.4.1. Cross-Reactivity Between Bovine Milk and Buffalo Cheese Proteins
3.4.2. Specific IgE Inhibition-Assay
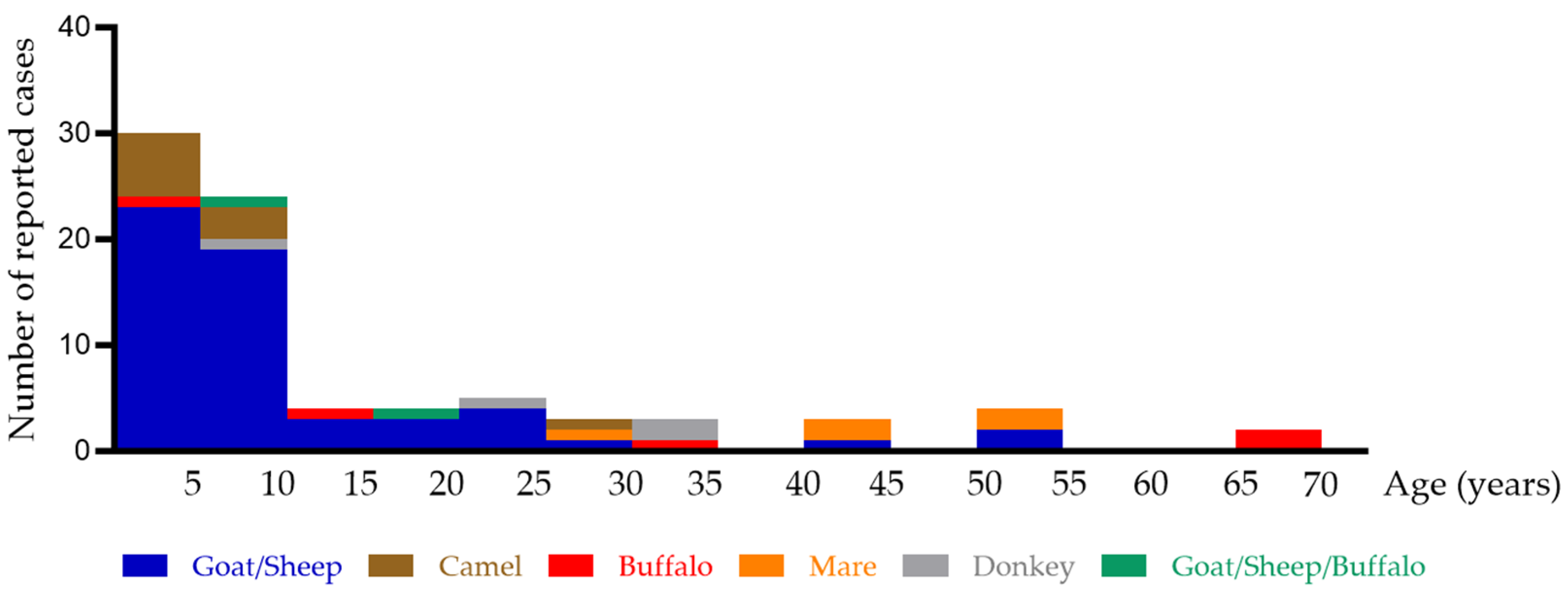
3.5. Comprehensive Overview of the Literature on Non-Cow Mammalian Milk Allergy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AA | allergic asthma |
| aIgE | anti-immunoglobuin E |
| AD | atopic dermatitis |
| ARC | allergic rhinoconjunctivitis |
| BAT | basophil activation test |
| BSB | basophil stimulation buffer |
| BM | buffalo milk |
| BC | buffalo cheese/buffalo camembert |
| BR | buffalo ricotta |
| Bmo | buffalo mozzarella |
| CaM | camel milk |
| CM | cow’s milk |
| CMA | cow’s milk allergy |
| CoFAR | Consortium for Food Allergy Research |
| DM | donkey milk |
| fMLP | n-formylmethione-leucyl-phenylalanine |
| GM | goat milk |
| IgE | immunoglobulin E |
| MM | mare milk |
| nbosd4 | α-lactalbumin |
| nbosd5 | β-lactoglobulin |
| nbosd6 | bovine serum albumin |
| nbosd8 | casein |
| OFC | oral food challenge |
| PBS | phosphate-buffered saline |
| kDa | kilodalton |
| rhIL-3 | recombinant human interleukin-3 |
| SDS-PAGE | sodium dodecylsulfate-polyacrylamide gel electrophoresis (SDS-PAGE) |
| SM | sheep milk |
| sIgE | specific immunoglobulin E |
| SPT | skin prick test |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient AF94 | Patient AF155 | Patient AF209 | |
|---|---|---|---|
| Concentration of CM in Serum | BM (kU/L) | BM (kU/L) | BM (kU/L) |
| PBS | 0.27 | 3.28 | 29.1 |
| 100 µg/mL | <0.10 | <0.10 | 2.22 |
| 10 µg/mL | <0.10 | 0.16 | 4.51 |
| 1 µg/mL | <0.10 | 1.19 | 10.1 |
| 0.1 µg/mL | 0.13 | 3.11 | 29.5 |
| 0.01 µg/mL | ND | 3.13 | 32.6 |
| Patient AF94 | Patient AF155 | Patient AF209 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Concentrations of BM in Serum | nBosd4 (kU/L) | nBosd5 (kU/L) | nBosd8 (kU/L) | nBosd4 (kU/L) | nBosd5 (kU/L) | nBosd8 (kU/L) | nBosd4 (kU/L) | nBosd5 (kU/L) | nBosd8 (kU/L) |
| PBS | 0.21 | <0.10 | 0.23 | <0.10 | 0.23 | 4.73 | 5.33 | 4.76 | 53.7 |
| 100 µg/mL | <0.10 | <0.10 | <0.10 | <0.10 | <0.10 | 0.7 | 1.62 | 0.89 | 9.01 |
| 10 µg/mL | <0.10 | <0.10 | <0.10 | <0.10 | <0.10 | 0.77 | 1.73 | 0.72 | 13 |
| 1 µg/mL | <0.10 | <0.10 | <0.10 | <0.10 | <0.10 | 1.62 | 1.88 | 1.6 | 21.8 |
| 0.1 µg/mL | <0.10 | <0.10 | <0.10 | <0.10 | 0.24 | 4.73 | 5.37 | 4.59 | 45.9 |
| 0.01 µg/mL | 0.18 | <0.10 | 0.18 | <0.10 | 0.22 | 4.95 | 5.32 | 4.64 | 55.7 |
References
- Sicherer, S.H.; Sampson, H.A. Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J. Allergy Clin. Immunol. 2018, 141, 41–58. [Google Scholar] [CrossRef] [PubMed]
- Flom, J.D.; Sicherer, S.H. Epidemiology of Cow’s Milk Allergy. Nutrients 2019, 11, 1051. [Google Scholar] [CrossRef] [PubMed]
- Luyt, D.; Ball, H.; Makwana, N.; Green, M.R.; Bravin, K.; Nasser, S.M.; Clark, A.T. BSACI guideline for the diagnosis and management of cow’s milk allergy. Clin. Exp. Allergy 2014, 44, 642–672. [Google Scholar] [CrossRef] [PubMed]
- Skripak, J.M.; Matsui, E.C.; Mudd, K.; Wood, R.A. The natural history of IgE-mediated cow’s milk allergy. J. Allergy Clin. Immunol. 2007, 120, 1172–1177. [Google Scholar] [CrossRef] [PubMed]
- Skripak, J.M.; Wood, R.A. Mammalian milk allergy: Avoidance strategies and oral desensitization. Curr. Opin. Allergy Clin. Immunol. 2009, 9, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Lajnaf, R.; Feki, S.; Ben Ameur, S.; Attia, H.; Kammoun, T.; Ayadi, M.A.; Masmoudi, H. Recent advances in selective allergies to mammalian milk proteins not associated with Cow’s Milk Proteins Allergy. Food Chem. Toxicol. 2023, 178, 113929. [Google Scholar] [CrossRef] [PubMed]
- Hinz, K.; O’Connor, P.M.; Huppertz, T.; Ross, R.P.; Kelly, A.L. Comparison of the principal proteins in bovine, caprine, buffalo, equine and camel milk. J. Dairy Res. 2012, 79, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Katz, Y.; Zadik-Mnuchin, G. Individuals with cow’s milk allergy are sensitized to milk from deer and ibex but not to milk from pork. Is there a “kosher” epitope? J. Allergy Clin. Immunol. 2004, 113, 156. [Google Scholar] [CrossRef]
- Sheehan, W.J.; Gardynski, A.; Phipatanakul, W. Skin Testing with Water Buffalo’s Milk in Children with Cow’s Milk Allergy. Pediatr. Asthma Allergy Immunol. 2009, 22, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, W.J.; Phipatanakul, W. Tolerance to water buffalo milk in a child with cow milk allergy. Ann. Allergy Asthma Immunol. 2009, 102, 349. [Google Scholar] [CrossRef] [PubMed]
- Garcia, B.E.; Lizaso, M.T. Cross-reactivity syndromes in food allergy. J. Investig. Allergol. Clin. Immunol. 2011, 21, 162–170. [Google Scholar] [PubMed]
- Bellioni-Businco, B.; Paganelli, R.; Lucenti, P.; Giampietro, P.G.; Perborn, H.; Businco, L. Allergenicity of goat’s milk in children with cow’s milk allergy. J. Allergy Clin. Immunol. 1999, 103, 1191–1194. [Google Scholar] [CrossRef] [PubMed]
- Businco, L.; Giampietro, P.G.; Lucenti, P.; Lucaroni, F.; Pini, C.; Di Felice, G.; Iacovacci, P.; Curadi, C.; Orlandi, M. Allergenicity of mare’s milk in children with cow’s milk allergy. J. Allergy Clin. Immunol. 2000, 105, 1031–1034. [Google Scholar] [CrossRef] [PubMed]
- Restani, P.; Gaiaschi, A.; Plebani, A.; Beretta, B.; Cavagni, G.; Fiocchi, A.; Poiesi, C.; Velonà, T.; Ugazio, A.G.; Galli, C.L. Cross-reactivity between milk proteins from different animal species. Clin. Exp. Allergy 1999, 29, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Iacono, G.; Carroccio, A.; Cavataio, F.; Montalto, G.; Soresi, M.; Balsamo, V. Use of Ass’ Milk in Multiple Food Allergy. J. Pediatr. Gastroenterol. Nutr. 1992, 14, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Lajnaf, R.; Feki, S.; Ameur, S.B.; Attia, H.; Kammoun, T.; Ayadi, M.A.; Masmoudi, H. Cow’s milk alternatives for children with cow’s milk protein allergy—Review of health benefits and risks of allergic reaction. Int. Dairy J. 2023, 141, 105624. [Google Scholar] [CrossRef]
- Uniacke-Lowe, T.; Huppertz, T.; Fox, P.F. Equine milk proteins: Chemistry, structure and nutritional significance. Int. Dairy J. 2010, 20, 609–629. [Google Scholar] [CrossRef]
- Pham, M.N.; Wang, J. Mammalian milk allergy: Case presentation and review of prevalence, diagnosis, and treatment. Ann. Allergy Asthma Immunol. 2017, 118, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Fanta, C.; Ebner, C. Allergy to mare’s milk. Allergy 1998, 53, 539–540. [Google Scholar] [CrossRef] [PubMed]
- Ieven, T.; Coorevits, L.; Vandebotermet, M.; Tuyls, S.; Vanneste, H.; Santy, L.; Wets, D.; Proost, P.; Frans, G.; Devolder, D.; et al. Endotyping of IgE-Mediated Polyethylene Glycol and/or Polysorbate 80 Allergy. J. Allergy Clin. Immunol. Pract. 2023, 11, 3146–3160. [Google Scholar] [CrossRef] [PubMed]
- Boumiza, R.; Debard, A.L.; Monneret, G. The basophil activation test by flow cytometry: Recent developments in clinical studies, standardization and emerging perspectives. Clin. Mol. Allergy 2005, 30, 9. [Google Scholar] [CrossRef] [PubMed]
- Sonder, S.U.; Plassmeyer, M.; Schroeder, N.; Peyton, S.; Paige, M.; Girgis, M.; Safi, H.; Alpan, O. Basophil activation test; User’s manual. J. Immunol. Methods 2025, 537, 113815. [Google Scholar] [CrossRef] [PubMed]
- Sander, I.; Kespohl, S.; Merget, R.; Goldscheid, N.; Degens, P.O.; Brüning, T.; Raulf-Heimsoth, M. A New Method to Bind Allergens for the Measurement of Specific IgE Antibodies. Int. Arch. Allergy Immunol. 2005, 136, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.J.; Ansotegui, I.J.; Campbell, D.E.; Cardona, V.; Carr, S.; Custovic, A.; Durham, S.; Ebisawa, M.; Geller, M.; Gonzalez-Estrada, A.; et al. Updated grading system for systemic allergic reactions: Joint Statement of the World Allergy Organization Anaphylaxis Committee and Allergen Immunotherapy Committee. World Allergy Organ. J. 2024, 17, 100876. [Google Scholar] [CrossRef] [PubMed]
- Wüthrich, B.; Johansson, S.G.O. Allergy to cheese produced from sheep’s and goat’s milk but not to cheese produced from cow’s milk. J. Allergy Clin. Immunol. 1995, 96, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Ehlayel, M.; Abdulbari, B. Camel’s milk allergy. Allergy Asthma Proc. 2018, 39, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Gall, H.; Kalveram, C.M.; Sick, H.; Sterry, W. Allergy to the heat-labile proteins α-lactalbumin and β-lactoglobulin in mare’s milk. J. Allergy Clin. Immunol. 1996, 97, 1304–1307. [Google Scholar] [CrossRef] [PubMed]
- Martín, T.M.; de la Hoz Caballer, B.; Lizana, F.M.; Mendiola, R.G.; Montaño, P.P.; Cano, M.S. Selective allergy to sheep’s and goat’s milk proteins. Allergol. Immunopathol. 2004, 32, 39–42. [Google Scholar]
- Umpiérrez, A.; Quirce, S.; Marañón, F.; Cuesta, J.; García-Villamuza, Y.; Lahoz, C.; Sastre, J. Sastre Allergy to goat and sheep cheese with good tolerance to cow cheese. Clin. Exp. Allergy 1999, 29, 1064–1068. [Google Scholar] [CrossRef] [PubMed]
- Ibañez, D.; Gonzalez, G.; Jimenez, G.; Escudero, C.; Laso, T.; Moneo, I. Allergy to sheep’s and goat’s milk cheese with good tolerance to cow’s milk. J. Allergy Clin. Immunol. 2006, 117, S46. [Google Scholar] [CrossRef]
- Khan, Z.; Carla, M.; Davis, M. Perinatal environmental influences on goat’s and sheep’s milk allergy without cow’s milk allergy. Ann. Allergy Asthma Immunol. 2013, 111, 574–575. [Google Scholar]
- de Boissieu, D.; Dupont, C. Allergie au lait de chèvre et de brebis sans allergie au lait de vache. Arch. Pédiatrie 2008, 15, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Mulé, P.; Gabrielli, S.; Upton, J.; Em, A.; Ben-Shoshan, M. Anaphylaxis to goat/sheep’s milk in a 4-year-old boy tolerant to cow’s milk. BMJ Case Rep. 2020, 13, e232844. [Google Scholar] [CrossRef] [PubMed]
- Piotin, A.; Hazebrouck, S.; Bernard, H.; de Blay, F.; Metz-Favre, C. Buffalo’s milk allergy: Role of sensitization to caprine β-casein. Pediatr. Allergy Immunol. 2023, 34, e13971. [Google Scholar] [CrossRef] [PubMed]
- Martins, P.; Borrego, L.M.; Pires, G.; Pinto, P.L.; Afonso, A.R.; Rosado-Pinto, J. Sheep and goat’s milk allergy—A case study. Allergy 2005, 60, 129–130. [Google Scholar] [CrossRef] [PubMed]
- Calvani, M., Jr.; Alessandri, C.; Calvani, M. Anaphylaxis to sheep’s milk cheese in a child unaffected by cow’s milk protein allergy. Eur. J. Pediatr. 1998, 157, 17–19. [Google Scholar] [CrossRef] [PubMed]
- Viñas, M.; Carnés, J.; López-Matas, M.A.; Hernández, N.; Castillo, M.J.; Ibero, M. Allergy to goat and sheep cheese with tolerance to cow’s milk and its derivatives. Allergol. Immunopathol. 2014, 42, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Mori, F.; Restani, P.; Pucci, N.; Ballabio, C.; Uberti, F.; Penas, E.; Novembre, E. Allergy to all mammalian Bovidae proteins but cow’s milk in a child. Allergol. Immunopathol. 2013, 41, 349–350. [Google Scholar] [CrossRef] [PubMed]
- Al-Hammadi, S.; El-Hassan, T.; Al-Reyami, L. Anaphylaxis to camel milk in an atopic child. Allergy 2010, 65, 1623–1625. [Google Scholar] [CrossRef] [PubMed]
- Vitte, J.; Bongrand, P. Anaphylaxie fatale au lait de brebis: Place de la biologie. Arch. Pédiatrie 2008, 15, 1300–1303. [Google Scholar] [CrossRef] [PubMed]
- Martini, M.; Swiontek, K.; Antonicelli, L.; Garritani, M.S.; Bilò, M.B.; Mistrello, G.; Amato, S.; Revets, D.; Ollert, M.; Morisset, M.; et al. Lysozyme, a new allergen in donkey’s milk. Clin. Exp. Allergy 2018, 48, 1521–1523. [Google Scholar] [CrossRef] [PubMed]
- Pazheri, D.F.; Melton, D.A.L., Jr.; Poptic, D.E.; Willard, D.B. Allergy to Sheep Milk with or Without Allergy to Cow Milk. J. Allergy Clin. Immunol. 2014, 133, AB199. [Google Scholar] [CrossRef]
- Lamblin, C.; Bourrier, T.; Orlando, J.P.; Sauvage, C.; Wallaert, B. Allergie aux laits de chèvre et de brebis sans allergie associée au lait de vache. Rev. Fr. Allergol. Immunol. Clin. 2001, 41, 165–168. [Google Scholar] [CrossRef]
- DAttou, A.; Caherec, S.; Bensakhria, P.; Dookna; Faverge, B. Allergy to goat and sheep milk without cow milk allergy: General revue and case report. Rev. Fr. Allergol. Immunol. Clin. 2005, 45, 601–607. [Google Scholar]
- Herz, A.; Kopp, M.V. Anaphylactic reaction at a pizzeria in a 13-year-old female patient. Allergo J. Int. 2020, 29, 165–167. [Google Scholar] [CrossRef]
- Pétrus, M.; Rayssac, M.; Cossarizza, G.; Lasserre, J.; Dutau, G. Allergie à la mozzarella au lait de bufflonne. À propos d’une observation chez un adolescent de 16 ans. Rev. Fr. Allergol. 2011, 51, 553–555. [Google Scholar] [CrossRef]
- Beaumesnil, M.; Denery-Papini, S.; Drouet, M.; Gaudin, J.-C. Allergy to Goat/Sheep’s Milk with Good Tolerance to Cow’s Milk but Not to Cow’s Milk Cheese: Identification of 1-105 Peptide from κ-Casein as the Molecular Basis of Reactivity toward Cow’s Milk Cheese for Two Patients. Res. Immunol. Int. J. 2013, 2013, 168397. [Google Scholar] [CrossRef]
- Peeters, C.; Herman, A.; Baeck, M. Donkey’s milk allergy. Br. J. Dermatol. 2017, 177, 1760–1761. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Futamura, K.; Hasegawa, E.; Aoki, Y.; Nakamura, M.; Matsunaga, K.; Yagami, A. Adult-Onset Sheep’s Milk Allergy in a Patient Without Cow’s Milk Allergy. J. Investig. Allergol. Clin. Immunol. 2021, 31, 273–274. [Google Scholar] [CrossRef] [PubMed]
- Tavares, B.; Pereira, C.; Rodrigues, F.; Loureiro, G.; Chieira, C. Goat’s milk allergy. Allergol. Immunopathol. 2007, 35, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Bahal, S. Second Reported Case of Buffalo Milk Protein Allergy without Cross Reactivity to Cow’s Milk. J. Allergy Immunol. 2017, 1, 5. [Google Scholar]
- Giorgis, V.; Rolla, G.; Raie, A.; Geuna, M.; Boita, M.; Lamberti, C.; Nebbia, S.; Giribaldi, M.; Giuffrida, M.G.; Brussino, L.; et al. A Case of Work-Related Donkey Milk Allergy. J. Investig. Allergol. Clin. Immunol. 2018, 28, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, M.J.; Lombardero, M. IgE-mediated anaphylaxis to sheep’s and goat’s milk. Allergy 2002, 57, 1091–1092. [Google Scholar] [CrossRef] [PubMed]
- Doyen, V.; Leduc, V.; Corazza, F.; Mairesse, M.; Ledent, C.; Michel, O. Protein contact dermatitis and food allergy to mare milk. Ann. Allergy Asthma Immunol. 2013, 110, 390–391. [Google Scholar] [CrossRef] [PubMed]
- Verhulst, L.; Kerre, S.; Goossens, A. The unsuspected power of mare’s milk. Contact Dermat. 2016, 74, 376–377. [Google Scholar] [CrossRef] [PubMed]
- Robles, S.; Torres, M.J.; Mayorga, C.; Rodríguez-bada, J.L.; Fernández, T.D.; Blanca, M.; Bartolomé, B. Anaphylaxis to mare’s milk. Ann. Allergy Asthma Immunol. 2007, 98, 600–602. [Google Scholar] [CrossRef] [PubMed]
- Ruiz del Barrio, L.; Martinez, M.J.; Pineda, F.; Dominguez Romero, I.; Menéndez-Rivero, E.; Prados-Castano, M. The threat of pizza: A rare case report of buffalo mozzarella allergy. In Proceedings of the EAACI Congress 2024, Valencia, Spain, 31 May–3 June 2024. [Google Scholar]
- Broekaert, S.M.C.; Darsow, U.; Ring, J.; Krause, I.; Schulmeister, U.; Spitzauer, S.; Valenta, R. Anaphylactic shock caused by buffalo’s mozzarella cheese. Ann. Allergy Asthma Immunol. 2008, 101, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Ah-Leung, S.; Bernard, H.; Bidat, E.; Paty, E.; Rancé, F.; Scheinmann, P.; Wal, J.M. Allergy to goat and sheep milk without allergy to cow’s milk. Allergy 2006, 61, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Trifonova, D.; Tulaeva, I.; Riabova, K.; Karsonova, A.; Kozlov, E.; Elisyutina, O.; Khaitov, M.; Focke-Tejkl, M.; Chen, T.-H.; et al. Albumins represent highly cross-reactive animal allergens. Front. Immunol. 2023, 14, 1241518. [Google Scholar] [CrossRef] [PubMed]


| Patient Characteristics | SPT | sIgE (kU/L) | Total IgE (kU/L) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Subject | Sex (M/F) | Age (Years) | Age at Onset (Years) | Clinical Presentation | Buffalo Milk | Cow`s Milk | Mare Milk | Goat Milk | Buffalo Cheese * | Cow`s Milk | n Bos d4 | n Bos d5 | n Bos d8 | Mare Milk | Goat Milk | |
| AF209 | M | 22 | 0 | Grade 3 | NP | NP | NP | NP | 43.2 | 64.2 | 5.63 | 4.85 | 74.2 | NP | 34 | 154 |
| AF264 | M | 25 | 0 | Grade 1 | NP | 2+ | NP | NP | <0.10 | 0.99 | 0.29 | <0.10 | 0.14 | NP | NP | 199 |
| AF278 | F | 24 | 0 | Grade 3 | NP | 4+ | NP | NP | >100 | >100 | 14.9 | 5.14 | >100 | NP | >100 | 663 |
| AF094 | F | 25 | 1 | Grade 1 | NP | 4+ | NP | NP | 0.49 | 0.51 | 0.25 | 0.11 | 0.41 | NP | NP | 1270 |
| AF192 | M | 25 | < 2 | Grade 3 | NP | 2+ | NP | NP | <0.10 | 0.19 | <0.10 | <0.10 | 0.12 | NP | NP | 35 |
| AF168 | F | 27 | 2 | Grade 1 | NP | 3+ | NP | NP | 0.11 | 1.01 | 0.47 | 0.14 | <0.10 | 1.41 | 2.01 | 279 |
| AF005 | F | 52 | Child | Grade 1 + 3 | NP | NP | NP | NP | 0.27 | 3.3 | 0.31 | 0.59 | 3.34 | NP | 5.1 | 2565 |
| AF220 | F | 31 | Child | Grade 3 | NP | 4+ | NP | NP | 11.1 | 0.96 | NP | NP | NP | 8.97 | NP | 3536 |
| AF155 | M | 26 | 8 | Grade 1 + 3 | NP | 3+ | NP | NP | 4.92 | 30 | <0.10 | 0.28 | 5.47 | NP | NP | 1388 |
| AF259 | M | 33 | 9 | Grade 1 | NP | 2+ | NP | NP | 2.31 | 2.38 | 0.53 | 0.11 | 3.35 | NP | NP | 1719 |
| AF164 | M | 26 | 20 | Grade 1 | NP | 3+ | NP | NP | 1.94 | 2.36 | <0.10 | 1.49 | 1.26 | NP | NP | 748 |
| AF268 | F | 51 | 36 | Grade 3 | NP | 4+ | NP | NP | >100 | >100 | 0.21 | 6.51 | >100 | NP | NP | 1196 |
| AF129 | F | 48 | 48 | Grade 3 | 3+ | - | - | - | 1 | <0.10 | <0.10 | <0.10 | <0.10 | NP | <0.10 | 614 |
| HV206 | F | 62 | 62 | Grade 3 | NP | - | 3+ | NP | <0.10 | 0.2 | <0.10 | 0.29 | <0.10 | 49.1 | NP | 330 |
| AF092 | M | 60 | NR | NR | NP | 2+ | NP | NP | <0.10 | 0.36 | <0.10 | <0.10 | <0.10 | NP | NP | 141 |
| AF097 | F | 22 | NR | NR | NP | − | NP | NP | 0.24 | NP | NP | NP | NP | <0.10 | 0.52 | >5000 |
| AF100 | F | 31 | NR | NR | NP | 2+ | NP | NP | <0.10 | 0.74 | 0.21 | 0.42 | 0.15 | NP | NP | 990 |
| AF101 | F | 46 | NR | NR | NP | 2+ | NP | NP | <0.10 | 0.82 | <0.10 | <0.10 | <0.10 | NP | NP | 1393 |
| AF112 | M | 51 | NR | Grade 1 | NP | 2+ | NP | NP | <0.10 | 7.81 | 1.09 | 0.87 | 0.47 | NP | NP | >5000 |
| AF182 | F | 21 | NR | NR | NP | − | NP | NP | <0.10 | 0.42 | NP | <0.10 | 0.34 | NP | NP | 853 |
| AF210 | F | 66 | NR | Grade 2 | NP | 1+ | NP | NP | 0.12 | 3.83 | 0.17 | 6.42 | 0.27 | NP | NP | 3490 |
| AF249 | M | 26 | NR | NR | NP | NP | NP | NP | 0.29 | 2 | <0.10 | <0.10 | 2.75 | NP | NP | 0 |
| Patient | Patient Characteristics | CMA | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | Age | Atopy | Presenting Symptoms | Culprit Food | |||||||||||
| AD | AA | ARC | FA | U | AE | GI | Resp | CVS | CNS | CoFar | |||||
| 1 (AF129) | F | 48 y | − | − | − | − | + | + | + | + | − | + | 3 | Buffalo ricotta | No |
| 2 (AF220) | F | 31 y | + | − | + | + | − | + | − | + | − | + | 3 | Mare milk | No |
| 3 (HV206) | F | 62 y | − | − | + | − | − | + | − | + | − | − | 3 | Mare milk/meat | No |
| Reference | Patient Characteristics | Mammalian Milk Allergy | Diagnostic Test Non-Cow’s Milk | Diagnostic Test Cow’s Milk | CMA | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | Age | Atopy | Type of MM | Presenting Symptoms | Culprit Food | SPT + | sIgE + | Immunoblot + | SPT + | sIgE + | Immunoblot + | ||||||||||||||||
| AD | AA | ARC | FA | F | U | AE | GI | Resp | CVS | CNS | CoFar | Age | CM | CM f2 | nBosd4 | nBosd5 | nBosd8 | ||||||||||
| Ehlayel et al. (2018) [26] | F | 1 y | − | − | − | − | CaM | − | + | + | − | − | − | − | Grade 1 | 1 y | CaM | CaM | NP | NP | NP | NP | NP | NP | NP | NP | No |
| Ah-Leung et al. (2006) [59] | M | 1.25 y | − | + | − | + | GM | − | − | − | − | + | − | − | Grade 3 | 1.25 y | GMC | GM/SM | GM/SM | NP | − | NP | NP | − | + | NP | No |
| Ehlayel et al. (2018) [26] | M | 1.5 y | + | − | − | + | CaM | − | + | + | + | − | − | Grade 2 | 1.5 y | CaM | CaM | NP | NP | NP | NP | NP | NP | NP | NP | No | |
| Ah-Leung et al. (2006) [59] | M | 2 y | − | + | + | − | GM | − | + | − | − | + | − | − | Grade 3 | 2 y | GMC | GM/SM | GM/SM | NP | − | NP | NP | − | + | NP | No |
| Ah-Leung et al. (2006) [59] | F | 2 y | + | + | − | + | GM | − | + | + | + | − | − | − | Grade 2 | 2 y | GMC | GM/SM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Martín et al. (2004) [28] | M | 2 y | NM | NM | NM | NM | SM | − | + | + | − | − | − | − | Grade 1 | 2 y | SC | GM/SM | GM/SM | GM/SM | − | − | − | − | − | − | No |
| Umpiérrez et al. (1999) [29] | F | 2 y | NM | NM | NM | + | GM/SM | − | − | + | − | + | − | − | Grade 3 | 2 y | GMC | GM/SM | GM/SM | GM/SM | − | − | − | − | − | + | No |
| Ibanez et al. (2006) [30] | F | 2 y | NM | NM | NM | NM | GM/SM | NM | NM | NM | NM | NM | NM | NM | Anaph | 2 y | SC | GM/SM | GM/SM | GM/SM | − | + | − | − | + | − | No |
| Khan et al. (2013) [31] | F | 3 y | NM | NM | NM | NM | GM/SM | + | + | + | + | − | − | − | Grade 2 | 3 y | GMC | GM/SM | GM/SM | NP | − | − | NP | NP | NP | NP | No |
| Ehlayel et al. (2018) [26] | M | 3 y | + | − | − | − | CaM | − | + | + | − | − | − | − | Grade 1 | 3 y | CaM | CaM | NP | NP | NP | NP | NP | NP | NP | NP | No |
| Ah-Leung et al. (2006) [59] | M | 3 y | + | − | − | + | GM | − | + | + | − | + | − | − | Grade 3 | 3 y | GMC | GM | GM/SM | NP | − | NP | NP | − | + | NP | No |
| Ah-Leung et al. (2006) [59] | M | 3 y | − | + | − | − | SM | − | − | − | − | + | − | − | Grade 3 | 3 y | SC | GM/SM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Ah-Leung et al. (2006) [59] | M | 3 y | + | − | − | + | GM | − | − | + | − | + | − | − | Grade 3 | 3 y | GMC | GM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Ah-Leung et al. (2006) [59] | M | 3 y | − | + | + | − | GM | − | − | + | − | + | − | − | Grade 3 | 3 y | GMC | GM/SM | GM/SM | NP | − | NP | NP | − | + | NP | No |
| Ah-Leung et al. (2006) [59] | M | 4 y | + | + | − | + | SM | − | + | + | + | − | − | − | Grade 2 | 4 y | SC | GM/SM | NP | − | NP | NP | − | + | NP | No | |
| Ah-Leung et al. (2006) [59] | M | 4 y | − | + | + | + | SM | − | − | + | + | + | − | − | Grade 3 | 4 y | SC | GM/SM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Ah-Leung et al. (2006) [59] | M | 4 y | + | + | + | − | SM | − | − | + | − | + | − | − | Grade 3 | 4 y | SMyoghurt/moussaka | GM/SM | GM/SM | NP | − | NP | NP | − | + | NP | No |
| De Boissieu et al. (2008) [32] | M | 4 y | − | + | − | − | GM/SM | − | + | − | − | + | − | − | Grade 3 | 4 y | Feta | GM/SM | GM/SM | NP | − | NP | NP | NP | NP | NP | No |
| Mulé et al. (2020) [33] | M | 4 y | + | + | NM | NM | GM/SM | + | + | − | + | + | − | + | Grade 3 | 4 y | Feta | GM/SM | NP | NP | − | NP | NP | NP | NP | NP | No |
| Piotin et al. (2023) [34] | F | 4 y | + | + | + | + | BM | − | − | − | + | − | + | − | Grade 3 | 4 y | BMo | GM/SM/BM | GM/SM | NP | − | NP | − | + | + | NP | No |
| Martins et al. (2005) [35] | M | 4 y | NM | NM | NM | + | GM/SM | − | + | + | − | − | − | − | Grade 1 | 2 y | GMC/SC | GM/SM | NP | GM | + | + | − | − | + | + | No |
| Ehlayel et al. (2018) [26] | F | 4.5 y | − | − | − | − | CaM | NM | NM | NM | NM | NM | NM | NM | Grade 3 | 4.5 y | CaM | CaM | NP | NP | NP | NP | NP | NP | NP | NP | No |
| Calvani et al. (1998) [36] | M | 5 y | + | + | + | + | SM | − | + | − | − | + | − | − | Grade 3 | 5 y | SC | GM/SM | NP | NP | − | − | NP | − | − | NP | No |
| Ehlayel et al. (2018) [26] | F | 5 y | + | − | − | + | CaM | − | + | + | − | − | − | − | Grade 1 | 5 y | CaM | CaM | NP | NP | NP | NP | NP | NP | NP | NP | Yes |
| Ehlayel et al. (2018) [26] | M | 5 y | + | − | − | − | CaM | NM | NM | NM | NM | NM | NM | NM | Grade 3 | 5 y | CaM | CaM | NP | NP | NP | NP | NP | NP | NP | NP | No |
| Pham et al. (2017) [18] | M | 5 y | − | + | + | − | GM/SM | − | + | − | + | + | NM | NM | Grade 4 | NM | GMC/SC | GM/SM | GM/SM | NP | + | + | NP | NP | NP | NP | No |
| Ah-Leung et al. (2006) [59] | M | 5 y | + | + | − | − | SM | − | − | + | − | + | − | − | Grade 3 | 5 y | SC | GM/SM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Ah-Leung et al. (2006) [59] | F | 5 y | − | + | − | − | GM/SM | − | + | − | − | + | − | − | Grade 3 | 5 y | SC/GM candy | GM/SM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Ah-Leung et al. (2006) [59] | F | 5 y | − | + | − | + | GM | − | − | − | − | + | − | − | Grade 3 | 5 y | GMC | GM/SM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Ah-Leung et al. (2006) [59] | F | 5 y | + | − | − | + | GM | − | + | + | − | − | − | − | Grade 2 | 5 y | GMC | GM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Ah-Leung et al. (2006) [59] | M | 6 y | + | − | − | + | GM | − | − | − | + | − | − | − | Grade 1 | 6 y | GMC | GM/SM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Ah-Leung et al. (2006) [59] | M | 6 y | + | + | + | + | GM | − | − | − | − | + | − | − | Grade 3 | 6 y | GMC/GM | GM/SM | GM/SM | NP | − | NP | NP | − | + | NP | No |
| Ah-Leung et al. (2006) [59] | M | 6 y | + | + | − | + | GM | − | + | + | + | + | − | − | Grade 3 | 6 y | GMC | GM/SM | GM/SM | NP | − | NP | NP | − | + | NP | No |
| Ah-Leung et al. (2006) [59] | F | 6 y | − | + | + | − | SM | − | + | − | + | + | − | − | Grade 3 | 6 y | SC | GM/SM | GM/SM | NP | − | NP | NP | − | + | NP | No |
| Vinas et al. (2014) [37] | M | 6 y | − | − | − | + | GM/SM | NM | NM | NM | NM | NM | NM | NM | Grade 3 | 6 y | Roquefort | GM/SM | GM/SM | GM/SM | + | − | − | − | + | + | No |
| Mori et al. (2012) [38] | M | 6 y | + | + | NM | − | GM/SM/BM | − | + | − | + | + | − | − | Grade 1–3 | 3/4/5y | Ewe/GMC/BC | GM/SM/BM | GM/SM | GM/SM | − | − | − | − | − | − | No |
| Al-Hammadi et (2010) [39] | B | 6 y | + | + | NM | + | CaM | − | − | + | − | + | + | + | Grade 4 | 6 y | CaM | CaM | NP | NP | − | − | NP | NP | NP | NP | No |
| Ehlayel et al. (2018) [26] | F | 6.5 y | + | − | − | + | CaM | NM | NM | NM | NM | NM | NM | NM | Grade 3 | 6.5 y | CaM | CaM | NP | NP | + | NP | NP | NP | NP | NP | Yes |
| Ah-Leung et al. (2006) [59] | M | 7 y | − | + | + | + | GM | − | − | + | − | − | − | − | Grade 1 | 7 y | GMC | GM/SM | GM/SM | NP | − | NP | NP | − | + | NP | No |
| Ah-Leung et al. (2006) [59] | M | 7 y | − | + | + | − | SM | − | − | − | + | − | − | − | Grade 1 | 7 y | SC | GM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Ah-Leung et al. (2006) [59] | M | 7 y | + | + | − | − | SM | − | + | − | + | + | − | − | Grade 3 | 7 y | SM pasta | GM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Ah-Leung et al. (2006) [59] | M | 7 y | − | + | − | − | GM | − | + | − | − | + | − | − | Grade 3 | 7 y | GM | GM | GM/SM | NP | − | NP | NP | − | + | NP | Yes |
| Ah-Leung et al. (2006) [59] | F | 7 y | + | − | − | + | GM | − | − | + | − | − | − | − | Grade 1 | 7 y | GMC | GM | GM/SM | NP | − | NP | NP | + | − | NP | No |
| Vitte et al. (2008) [40] | M | 8 y | + | NM | NM | NM | SM | NM | NM | NM | NM | + | + | + | Grade 4 | 8 y | CMC/SC | NP | GM/SM | NP | NP | + | NP | NP | NP | NP | No |
| Ehlayel et al. (2018) [26] | M | 8 y | + | − | − | − | CaM | − | + | − | − | − | − | − | Grade 1 | 8 y | CaM | CaM | NP | NP | + | + | NP | NP | NP | NP | No |
| Vinas et al. (2014) [37] | M | 9 y | − | − | − | + | GM/SM | NM | NM | NM | NM | NM | NM | NM | Grade 3 | 9 y | Cheese | GM/SM | GM/SM | GM/SM | − | + | − | − | − | + | No |
| Vinas et al. (2014) [37] | M | 9 y | − | − | − | + | GM/SM | NM | NM | NM | NM | NM | NM | NM | Grade 4 | 9 y | CMC/GMC/SC | SM | GM/SM | SM | − | + | + | − | + | + | No |
| Martini et al. (2018) [41] | F | 9 y | NM | NM | NM | + | DM | − | + | − | − | − | − | − | Grade 1 | 9 y | DMcream | DM | NP | DM/MM | − | NP | NP | NP | NP | − | No |
| Martins et al. (2005) [35] | M | 9 y | NM | NM | NM | NM | GM/SM | − | − | + | − | + | − | − | Grade 3 | 6/7 y | Pizza cheese | GM/SM | NP | GM | − | − | NP | NP | NP | NP | No |
| Ah-Leung et al. (2006) [59] | F | 9 y | + | − | − | − | GM | − | + | + | − | − | − | − | Grade 1 | 9 y | GMC | GM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Ah-Leung et al. (2006) [59] | M | 10 y | + | − | + | + | GM/SM | − | + | − | − | − | − | − | Grade 1 | 10 y | Sandwich | GM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Ibanez et al. (2006) [30] | M | 10 y | NM | NM | NM | NM | GM/SM | NM | NM | NM | NM | NM | NM | NM | Anaph | 10 y | Cheese | GM/SM | GM/SM | GM/SM | − | + | − | − | + | + | No |
| Pazheri et al. (2014) [42] | M | 10 y | NM | NM | NM | NM | SM | NM | NM | NM | NM | NM | NM | NM | Anaph | 10 y | Romano/ricotta | NP | SM | NP | NP | − | NP | NP | NP | NP | No |
| Lamblin et al. (2001) [43] | M | 10 y | + | − | − | − | GM/SM | − | + | + | − | + | − | − | Grade 3 | 10 y | SC | GM/SM | GM/SM | NP | + | + | NP | NP | + | NP | No |
| Dattou et al. (2005) [44] | F | 11 y | + | + | NM | − | GM/SM/CM | + | + | + | − | + | − | − | Grade 1/3 | 11 y | CMC/GMC/SC | GM/SM | GM/SM | NP | + | + | NP | NP | NP | NP | Yes |
| Ah-Leung et al. (2006) [59] | M | 12 y | − | − | − | − | GM | − | + | − | − | − | − | − | Grade 1 | 12 y | GMC | GM | − | NP | − | NP | NP | − | − | NP | No |
| Her et al. (2020) [45] | F | 13 y | − | − | − | − | BM | − | − | + | + | + | − | + | Grade 3 | 13 y | BMo | BM | NP | NP | − | − | − | − | − | NP | No |
| Wüthrich et al. (1995) [25] | M | 15 y | + | − | + | − | GM/SM | + | − | + | − | − | − | − | Grade 1 | 15 y | Feta | GM | GM/SM | NP | − | − | − | − | − | NP | No |
| Pétrus et al. (2011) [46] | M | 16 y | NM | + | + | + | GM/SM/BM | − | + | + | − | + | − | − | Grade 3 | 11/16 y | CMC/GMC/SC | GM/SM/BM | GM/SM | NP | − | + | − | − | + | NP | No |
| Ah-Leung et al. (2006) [59] | F | 16 y | − | − | + | − | SM | − | − | − | − | + | − | − | Grade 3 | 16 y | SC/SM yoghurt | GM/SM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Ah-Leung et al. (2006) [59] | M | 16 y | − | − | + | − | GM | NM | NM | NM | NM | NM | NM | NM | Grade 3 | 16 y | GMC | GM/SM | GM/SM | NP | − | NP | NP | − | − | NP | No |
| Beaumesnil et al. (2013) [47] | M | 20 y | + | NM | NM | − | GM | − | + | + | − | + | − | − | Grade 3 | 4/7 y | GMC | GM | GM | GM | + | + | + | + | + | + | Yes |
| Beaumesnil et al. (2013) [47] | M | 22y | NM | NM | NM | − | GM/CM | NM | NM | NM | NM | NM | NM | NM | Grade 4 | 17 y | GMC/CMC | GM/SM | GM | GM | + | + | + | − | + | − | Yes |
| Lamblin et al. (2001) [43] | M | 22 y | + | + | NM | NM | GM/SM | − | + | + | − | + | + | − | Grade 3 | 22 y | GMC | NP | GM/SM | NP | NP | − | − | − | NP | NP | No |
| Wüthrich et al. (1995) [25] | M | 25 y | − | − | − | − | GM/SM | − | + | + | − | + | − | − | Grade 3 | 25 y | GMC/SC | GM | GM/SM | NP | − | − | − | − | − | NP | No |
| Peeters et al. (2017) [48] | F | 25 y | + | + | + | − | DM | + | − | + | − | + | + | + | Grade 3 | 25 y | DM | DM | NP | NP | − | − | − | − | − | NP | No |
| Suzuki et al. (2021) [49] | F | 25 y | + | + | NM | − | SM | − | − | + | + | + | − | − | Grade 3 | 21/22/23 y | Picorino | GM/SM | SM | SM | − | − | − | − | − | − | No |
| Tavares et al. (2007) [50] | F | 27 y | NM | + | + | NM | GM | − | + | − | − | − | − | − | Grade 1 | 24 y | Caprine | GM | − | GM | − | − | − | − | − | − | No |
| Ehlayel et al. (2018) [26] | F | 30 y | − | − | + | − | CaM | NM | NM | NM | NM | NM | NM | NM | Grade 3 | 30 y | CaM | CaM | NP | NP | NP | NP | NP | NP | NP | NP | No |
| Fanta et al. (1998) [19] | F | 30 y | NM | + | NM | NM | MM | − | + | + | − | + | − | − | Grade 3 | 30 y | MM | MM | MM | MM | NP | − | NP | NP | NP | NP | No |
| Martini et al. (2018) [41] | F | 33 y | + | − | + | − | DM | + | − | + | − | − | − | − | Grade 1 | 33 y | DM | DM | NP | DM/MM | − | NP | NP | NP | NP | − | No |
| Bahal et al. (2017) [51] | F | 34 y | NM | NM | NM | NM | BM | − | − | + | − | − | − | − | Grade 1 | NM | BMO | BM | − | NM | NM | − | NM | NM | NM | NM | No |
| Giorgis et (2018) [52] | F | 35 y | NM | + | + | − | DM | − | − | − | − | + | − | − | Grade 3 | 35 y | DM | DM | − | DM | − | − | − | − | − | NP | No |
| Alvarez et al. (2002) [53] | M | 43 y | − | − | − | − | SM | − | − | − | + | + | + | − | Grade 3 | 43 y | SM-curd | GM/SM | GM/SM | GM/SM | NP | − | − | − | − | − | No |
| Doyen et al. (2013) [54] | F | 44 y | NM | NM | + | NM | MM | + | − | − | + | − | − | − | Grade 1 | 44 y | MM cosmetics/pills | GM/SM/MM | GM/SM/MM | MM | − | + | + | + | + | NP | No |
| Verhulst et al. (2016) [55] | F | 45 y | NM | NM | NM | NM | MM | − | + | + | − | − | − | − | Grade 1 | 45 y | MM/CM cream | MM | MM | NP | − | + | + | − | − | NP | No |
| Gall et al. (1996) [27] | F | 51 y | NM | NM | NM | NM | MM | − | − | + | − | + | + | − | Grade 3 | 51 y | MM granulate | MM | MM | MM | − | NP | − | − | − | NP | No |
| Lamblin et al. (2001) [43] | F | 52 y | − | − | − | − | GM/SM | − | + | − | − | + | − | + | Grade 3 | 52 y | GMC/SC | GM/SM | GM/SM | NP | − | − | − | − | NP | NP | No |
| Robles et al. (2007) [56] | F | 53 y | NM | + | + | NM | MM | + | − | − | − | + | − | − | Grade 3 | 53 y | MM | MM | MM | NP | NP | NP | NP | NP | NP | + | No |
| Vinas et al. (2014) [37] | M | 54 y | − | − | − | − | GM/SM | NM | NM | NM | NM | NM | NM | NM | Grade 3 | 54 y | CMC/GMC/SC | GM/SM | SM | SM | + | − | − | − | − | + | No |
| Ruiz Del Barrio et al. (2024) [57] | M | 67 y | NM | NM | + | NM | BM | − | − | + | − | + | − | + | Grade 3 | 67 y | BMo | BM | NP | BM | − | NP | − | − | − | NP | No |
| Broekaert et al. (2008) [58] | M | 70 y | NM | NM | NM | − | BM | − | + | + | − | + | − | + | Grade 3 | 70 y | BMo | BM | NP | BM | − | − | − | − | − | − | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verelst, S.; Sinnesael, R.; Taïbi, F.; Tuyls, S.; Coorevits, L.; Breynaert, C.; Bullens, D.; Schrijvers, R. Belgian Case Series Identifies Non-Cow Mammalian Milk Allergy as a Rare, Severe, Selective, and Late-Onset Condition. Nutrients 2025, 17, 2393. https://doi.org/10.3390/nu17152393
Verelst S, Sinnesael R, Taïbi F, Tuyls S, Coorevits L, Breynaert C, Bullens D, Schrijvers R. Belgian Case Series Identifies Non-Cow Mammalian Milk Allergy as a Rare, Severe, Selective, and Late-Onset Condition. Nutrients. 2025; 17(15):2393. https://doi.org/10.3390/nu17152393
Chicago/Turabian StyleVerelst, Sophie, Robbe Sinnesael, Firoz Taïbi, Sebastian Tuyls, Lieve Coorevits, Christine Breynaert, Dominique Bullens, and Rik Schrijvers. 2025. "Belgian Case Series Identifies Non-Cow Mammalian Milk Allergy as a Rare, Severe, Selective, and Late-Onset Condition" Nutrients 17, no. 15: 2393. https://doi.org/10.3390/nu17152393
APA StyleVerelst, S., Sinnesael, R., Taïbi, F., Tuyls, S., Coorevits, L., Breynaert, C., Bullens, D., & Schrijvers, R. (2025). Belgian Case Series Identifies Non-Cow Mammalian Milk Allergy as a Rare, Severe, Selective, and Late-Onset Condition. Nutrients, 17(15), 2393. https://doi.org/10.3390/nu17152393