
High-Protein Dietary Interventions in Heart Failure: A Systematic Review of Clinical and Functional Outcomes
 , , ,
, , ,  and
and Highlights
- The systematic review showed that heart failure patients who followed high-protein diets experienced significant improvements in exercise ability, nutritional status, and body composition, as seen in controlled studies.
- Individuals on high-protein diets often reported gains in lean body mass and better quality of life. Additionally, some studies showed positive changes in lab results and physical performance.
- In randomized trials, providing protein-rich nutritional support to people with heart failure who are malnourished or at high risk was linked to fewer hospital readmissions and lower morbidity and mortality.
- The review suggests that high-protein nutrition could be a useful addition to standard heart failure care, which involves a range of treatments. However, the review also emphasizes the need for more research to identify optimal dosages, the best times to take them, and their long-term safety.
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Data Extraction
2.4. Data Synthesis and Heterogeneity
2.5. Risk of Bias Assessment Method
2.6. Synthesis
3. Results
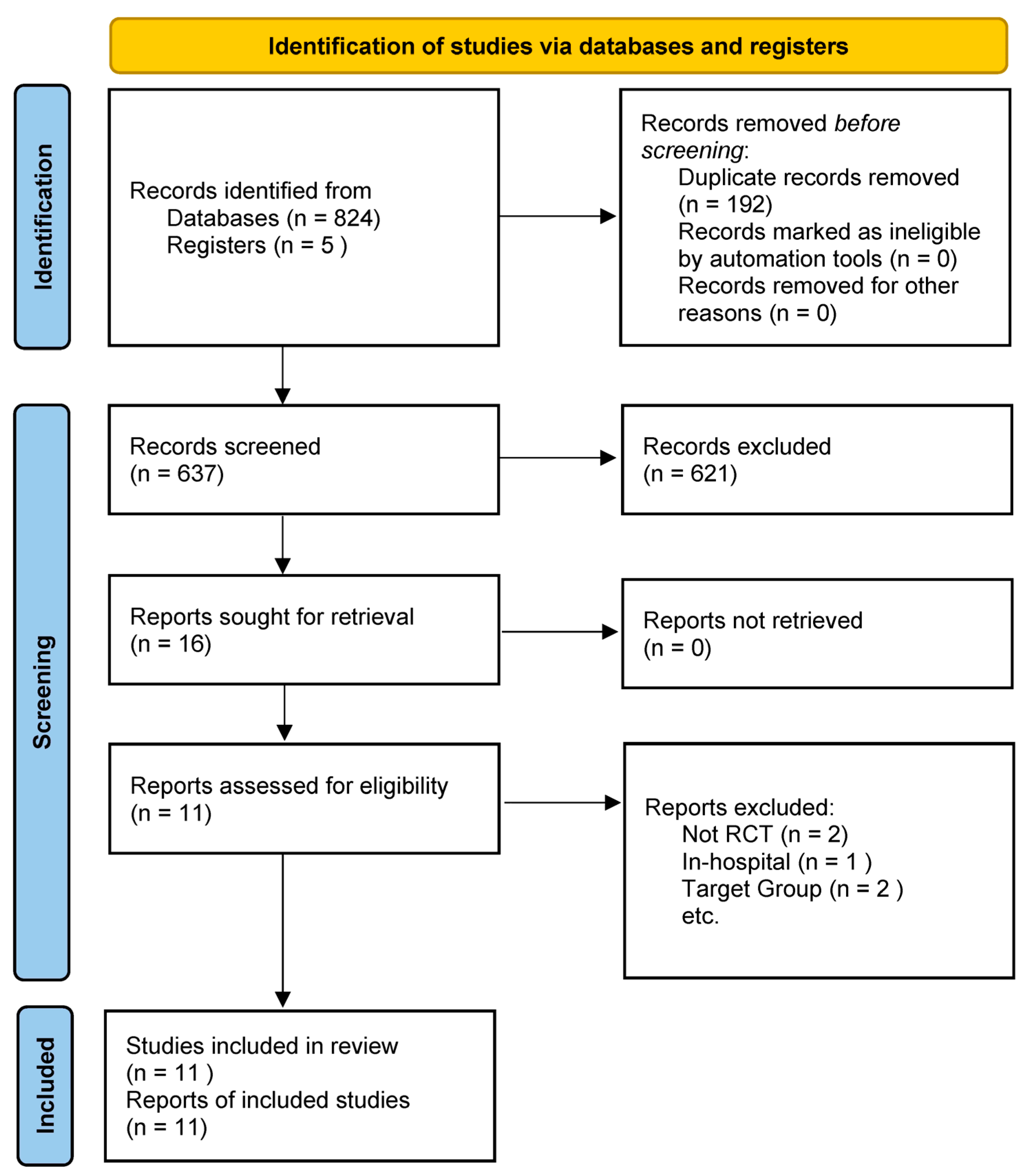
3.1. Study Selection and Characteristics
3.2. Interventions
3.3. Outcomes Measured
3.4. Summary of Quantitative Findings
3.5. Risk of Bias Assessment Results
3.6. Effects of High-Protein Interventions on Outcomes
3.6.1. Nutritional Status and Body Composition
3.6.2. Laboratory Nutritional Markers
3.6.3. Functional Capacity and Exercise Performance
3.6.4. Clinical Outcomes: Mortality and Hospitalizations
4. Discussion
4.1. Key Findings
4.2. Interpreting Functional Results
4.3. Interpreting Clinical Outcomes Results
4.4. Quality of Evidence
4.5. Comparison with Other Reviews
4.6. Clinical Implications
4.7. Future Guideline Development
4.8. Limitations and Research Needs
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HF | Heart failure |
References
- Lena, A.; Anker, M.S.; Springer, J. Muscle wasting and sarcopenia in heart failure-the current state of science. Int. J. Mol. Sci. 2020, 21, 6549. [Google Scholar] [CrossRef]
- Beltrami, M.; Fumagalli, C.; Milli, M. Frailty, sarcopenia and cachexia in heart failure patients: Different clinical entities of the same painting. World J. Cardiol. 2021, 13, 1–10. [Google Scholar] [CrossRef]
- Esteban-Fernández, A.; Villar-Taibo, R.; Alejo, M.; Arroyo, D.; Bonilla Palomas, J.L.; Cachero, M.; Joaquin, C.; Méndez Bailón, M.; Pérez-Rivera, J.; Romero-Vigara, J.C.; et al. Diagnosis and management of malnutrition in patients with heart failure. J. Clin. Med. 2023, 12, 3320. [Google Scholar] [CrossRef]
- Vest, A.R.; Chan, M.; Deswal, A.; Givertz, M.M.; Lekavich, C.; Lennie, T.; Litwin, S.E.; Parsly, L.; Rodgers, J.E.; Rich, M.W.; et al. Nutrition, obesity, and cachexia in patients with heart failure: A consensus statement from the Heart Failure Society of America Scientific Statements Committee. J. Card. Fail. 2019, 25, 380–400. [Google Scholar] [CrossRef] [PubMed]
- Hersberger, L.; Dietz, A.; Bürgler, H.; Bargetzi, A.; Bargetzi, L.; Kägi-Braun, N.; Tribolet, P.; Gomes, F.; Hoess, C.; Pavlicek, V.; et al. Individualized nutritional support for hospitalized patients with chronic heart failure. J. Am. Coll. Cardiol. 2021, 77, 2307–2319. [Google Scholar] [CrossRef] [PubMed]
- Katano, S.; Yano, T.; Yamano, K.; Numazawa, R.; Nagaoka, R.; Honma, S.; Fujisawa, Y.; Ohori, K.; Kouzu, H.; Kunihara, H.; et al. Associations between in-hospital daily protein intake and adverse clinical outcomes in older patients with heart failure. ESC Heart Fail. 2024, 11, 2591–2605. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Fung, T.T.; Hu, F.B.; Willett, W.C.; Longo, V.D.; Chan, A.T.; Giovannucci, E.L. Association of animal and plant protein intake with all-cause and cause-specific mortality. JAMA Intern. Med. 2016, 176, 1453–1463. [Google Scholar] [CrossRef]
- Saitoh, M.; Rodrigues Dos Santos, M.; von Haehling, S. Muscle wasting in heart failure: The role of nutrition. Wien. Klin. Wochenschr. 2016, 128 (Suppl. S7), 455–465. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane Database Syst. Rev. 2019, 10, Ed000142. [Google Scholar] [CrossRef]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef]
- Cumpston, M.S.; McKenzie, J.E.; Welch, V.A.; Brennan, S.E. Strengthening systematic reviews in public health: Guidance in the Cochrane Handbook for Systematic Reviews of Interventions. J. Public Health 2022, 44, e588–e592. [Google Scholar] [CrossRef]
- Pollock, D.; Peters, M.D.J.; Khalil, H.; McInerney, P.; Alexander, L.; Tricco, A.C.; Evans, C.; de Moraes, É.B.; Godfrey, C.M.; Pieper, D.; et al. Recommendations for the extraction, analysis, and presentation of results in scoping reviews. JBI Evid. Synth. 2023, 21, 520–532. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Broqvist, M.; Arnqvist, H.; Dahlström, U.; Larsson, J.; Nylander, E.; Permert, J. Nutritional assessment and muscle energy metabolism in severe chronic congestive heart failure—effects of long-term dietary supplementation. Eur. Heart J. 1994, 15, 1641–1650. [Google Scholar] [CrossRef] [PubMed]
- Aquilani, R.; Opasich, C.; Gualco, A.; Verri, M.; Testa, A.; Pasini, E.; Viglio, S.; Iadarola, P.; Pastoris, O.; Dossena, M.; et al. Adequate energy-protein intake is not enough to improve nutritional and metabolic status in muscle-depleted patients with chronic heart failure. Eur. J. Heart Fail. 2008, 10, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Rozentryt, P.; von Haehling, S.; Lainscak, M.; Nowak, J.U.; Kalantar-Zadeh, K.; Polonski, L.; Anker, S.D. The effects of a high-caloric protein-rich oral nutritional supplement in patients with chronic heart failure and cachexia on quality of life, body composition, and inflammation markers: A randomized, double-blind pilot study. J. Cachexia Sarcopenia Muscle 2010, 1, 35–42. [Google Scholar] [CrossRef]
- Bonilla-Palomas, J.L.; Gámez-López, A.L.; Castillo-Domínguez, J.C.; Moreno-Conde, M.; López Ibáñez, M.C.; Alhambra Expósito, R.; Ramiro Ortega, E.; Anguita-Sánchez, M.P.; Villar-Ráez, A. Nutritional intervention in malnourished hospitalized patients with heart failure. Arch. Med. Res. 2016, 47, 535–540. [Google Scholar] [CrossRef]
- Deutz, N.E.; Matheson, E.M.; Matarese, L.E.; Luo, M.; Baggs, G.E.; Nelson, J.L.; Hegazi, R.A.; Tappenden, K.A.; Ziegler, T.R. Readmission and mortality in malnourished, older, hospitalized adults treated with a specialized oral nutritional supplement: A randomized clinical trial. Clin. Nutr. 2016, 35, 18–26. [Google Scholar] [CrossRef]
- Pineda-Juárez, J.A.; Sánchez-Ortiz, N.A.; Castillo-Martínez, L.; Orea-Tejeda, A.; Cervantes-Gaytán, R.; Keirns-Davis, C.; Pérez-Ocampo, C.; Quiroz-Bautista, K.; Tenorio-Dupont, M.; Ronquillo-Martínez, A. Changes in body composition in heart failure patients after a resistance exercise program and branched chain amino acid supplementation. Clin. Nutr. 2016, 35, 41–47. [Google Scholar] [CrossRef]
- Evangelista, L.S.; Jose, M.M.; Sallam, H.; Serag, H.; Golovko, G.; Khanipov, K.; Hamilton, M.A.; Fonarow, G.C. High-protein vs. standard-protein diets in overweight and obese patients with heart failure and diabetes mellitus: Findings of the Pro-HEART trial. ESC Heart Fail. 2021, 8, 1342–1348. [Google Scholar] [CrossRef]
- Dos Santos, E.M.; Moreira, A.S.B.; Huguenin, G.V.B.; Tibiriça, E.; De Lorenzo, A. Effects of whey protein isolate on body composition, muscle mass, and strength of chronic heart failure patients: A randomized clinical trial. Nutrients 2023, 15, 2320. [Google Scholar] [CrossRef]
- Azhar, G.; Wei, J.Y.; Schutzler, S.E.; Coker, K.; Gibson, R.V.; Kirby, M.F.; Ferrando, A.A.; Wolfe, R.R. Daily consumption of a specially formulated essential amino acid-based dietary supplement improves physical performance in older adults with low physical functioning. J. Gerontol. A Biol. Sci. Med. Sci. 2021, 76, 1184–1191. [Google Scholar] [CrossRef]
- Herrera-Martínez, A.D.; Jiménez, C.M.; Romo, A.N.; Aguilera, J.L.; Crespin, M.C.; Baena, B.T.; Casado-Díaz, A.; Moreno, M.Á.G.; Puerta, M.J.M.; Roger, A.J. Nutritional support reduces circulating cytokines in patients with heart failure. Nutrients 2024, 16, 1637. [Google Scholar] [CrossRef]
- Carnahan, R.M.; Brown, G.D. The power and pitfalls of underpowered studies. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2024, 44, 698–700. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Vargas, A.I.; Fuentes-Abolafio, I.J.; García-Conejo, C.; Díaz-Balboa, E.; Trinidad-Fernández, M.; Gutiérrez-Sánchez, D.; Escriche-Escuder, A.; Cobos-Palacios, L.; López-Sampalo, A.; Pérez-Ruíz, J.M.; et al. Effectiveness of a cardiac rehabilitation program on biomechanical, imaging, and physiological biomarkers in elderly patients with heart failure with preserved ejection fraction (HFpEF): FUNNEL + study protocol. BMC Cardiovasc. Disord. 2023, 23, 550. [Google Scholar] [CrossRef] [PubMed]
- Kitzman, D.W.; Brubaker, P.; Morgan, T.; Haykowsky, M.; Hundley, G.; Kraus, W.E.; Eggebeen, J.; Nicklas, B.J. Effect of caloric restriction or aerobic exercise training on peak oxygen consumption and quality of life in obese older patients with heart failure with preserved ejection fraction: A randomized clinical trial. JAMA 2016, 315, 36–46. [Google Scholar] [CrossRef]
- Alhebshi, A.; Alsharif, N.; Thorley, J.; James, L.J.; Clifford, T. The effects of dietary protein supplementation on exercise-induced inflammation and oxidative stress: A systematic review of human trials. Antioxidants 2021, 11, 13. [Google Scholar] [CrossRef]
- Ilha, J.; do Espírito-Santo, C.C.; de Freitas, G.R. mTOR signaling pathway and protein synthesis: From training to aging and muscle autophagy. Adv. Exp. Med. Biol. 2018, 1088, 139–151. [Google Scholar]
- Bolster, D.R.; Jefferson, L.S.; Kimball, S.R. Regulation of protein synthesis associated with skeletal muscle hypertrophy by insulin-, amino acid- and exercise-induced signalling. Proc. Nutr. Soc. 2004, 63, 351–356. [Google Scholar] [CrossRef]
- Yoshihisa, A.; Kanno, Y.; Watanabe, S.; Yokokawa, T.; Abe, S.; Miyata, M.; Sato, T.; Suzuki, S.; Oikawa, M.; Kobayashi, A.; et al. Impact of nutritional indices on mortality in patients with heart failure. Open Heart 2018, 5, e000730. [Google Scholar] [CrossRef]
- Lv, S.; Ru, S. The prevalence of malnutrition and its effects on the all-cause mortality among patients with heart failure: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0259300. [Google Scholar] [CrossRef]
- Phillips, S.M. A brief review of critical processes in exercise-induced muscular hypertrophy. Sports Med. 2014, 44 (Suppl. S1), S71–S77. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef] [PubMed]
- Kittleson Michelle, M.; Breathett, K.; Ziaeian, B.; Aguilar, D.; Blumer, V.; Bozkurt, B.; Diekemper Rebecca, L.; Dorsch Michael, P.; Heidenreich Paul, A.; Jurgens Corrine, Y.; et al. 2024 update to the 2020 ACC/AHA clinical performance and quality measures for adults with heart failure. JACC 2024, 84, 1123–1143. [Google Scholar] [CrossRef] [PubMed]
- Beghini, A.; Sammartino, A.M.; Papp, Z.; von Haehling, S.; Biegus, J.; Ponikowski, P.; Adamo, M.; Falco, L.; Lombardi, C.M.; Pagnesi, M.; et al. 2024 update in heart failure. ESC Heart Fail. 2025, 12, 8–42. [Google Scholar] [CrossRef] [PubMed]
- Dwan, K.; Gamble, C.; Williamson, P.R.; Kirkham, J.J. Systematic review of the empirical evidence of study publication bias and outcome reporting bias—An updated review. PloS ONE 2013, 8, e66844. [Google Scholar] [CrossRef]
- Habaybeh, D.; de Moraes, M.B.; Slee, A.; Avgerinou, C. Nutritional interventions for heart failure patients who are malnourished or at risk of malnutrition or cachexia: A systematic review and meta-analysis. Heart Fail. Rev. 2021, 26, 1103–1118. [Google Scholar] [CrossRef]
- Mantzouranis, E.; Kakargia, E.; Kakargias, F.; Lazaros, G.; Tsioufis, K. The impact of high protein diets on cardiovascular outcomes: A systematic review and meta-analysis of prospective cohort studies. Nutrients 2023, 15, 1372. [Google Scholar] [CrossRef]
- Luu, T.N.; Ha, T.P. Effectiveness of high-energy, high-protein nutritional supplementation on patients with chronic heart failure and malnutrition: A pilot open-label randomized trial. Medicine 2025, 104, e42941. [Google Scholar] [CrossRef]
- Tang, W.H.W.; Bakitas, M.A.; Cheng, X.S.; Fang, J.C.; Fedson, S.E.; Fiedler, A.G.; Martens, P.; McCallum, W.I.; Ogunniyi, M.O.; Rangaswami, J.; et al. Evaluation and management of kidney dysfunction in advanced heart failure: A scientific statement from the American Heart Association. Circulation 2024, 150, e280–e295. [Google Scholar] [CrossRef]
- Roehm, B.; McAdams, M.; Hedayati, S.S. Novel biomarkers of kidney disease in advanced heart failure: Beyond GFR and proteinuria. Curr. Heart Fail. Rep. 2022, 19, 223–235. [Google Scholar] [CrossRef]
- Kelly, J.T.; Law, L.; De Guzman, K.R.; Hickman, I.J.; Mayr, H.L.; Campbell, K.L.; Snoswell, C.L.; Erku, D. Cost-effectiveness of telehealth-delivered nutrition interventions: A systematic review of randomized controlled trials. Nutr. Rev. 2023, 81, 1599–1611. [Google Scholar] [CrossRef]

{kind=link}
| Study Author, Year | Population | Intervention (Protein Target) | Control | Duration | Clinical Outcomes | Surrogate Markers |
|---|---|---|---|---|---|---|
| Broqvist et al., 1994 [15] | 22 patients, NYHA III-IV | High-calorie, high-protein liquid supplement (30 g/day) | Isocaloric placebo (no protein) | ~3 months | No difference in survival; signs of clinical deterioration in the control group | No change in ATP or creatine; no improvement in function or nutritional status |
| Aquilani et al., 2008 [16] | 38 stable HF patients | 8 g/day essential amino acids | No supplement | 2 months | Not reported | ↑ Weight (in 80% of supplemented); ↓ lactate & pyruvate; ↑ peak VO2 and walking test |
| Rozentryt et al., 2010 [17] | 29 cachectic HF patients | ONS: +600 kcal/day, +20 g protein/day | Placebo (non-caloric) | 6 weeks + 18-week follow-up | Not reported | ↑ Weight (+2.3 kg), improved QoL, ↓ TNF-α (p < 0.05) |
| Bonilla-Palomas et al., 2016 (PICNIC) [18] | 120 hospitalized, malnourished HF patients | Individualized high-protein diet (~≥1.2 g/kg/day) + ONS + HF care | Usual HF care only | 12 months | ↓ Mortality (20.3% vs. 47.5%), ↓ HF readmissions (10.2% vs. 36.1%) | ↑ Albumin, hemoglobin; ↑ handgrip strength; improved QoL |
| Deutz et al., 2016 [19] | 652 malnourished older adults (~51% HF) | ONS with protein (40 g/day), HMB, vitamins | Placebo ONS | 90 days post-discharge | 50% ↓ mortality in the intervention group | ↑ Weight and nutritional status; improved lab markers |
| Pineda-Juárez et al., 2016 [20] | 66 stable HF patients | BCAA supplement + resistance training | Resistance training only | 3 months | Not reported | ↑ VO2max and METs in both groups; no significant difference between arms |
| Evangelista et al., 2021 [21] | 67 obese HF + diabetes | High protein (~1.3 g/kg/day), low-calorie diet (30% protein) | Standard-protein diet (~0.8 g/kg/day) | 3 months | Not reported | ↓ HbA1c (–0.7% vs. –0.1%); ↓ TG, LDL, SBP |
| Dos Santos et al., 2023 [22] | 25 chronic HF (many sarcopenic) | Whey protein isolate (30 g/day) | Isocaloric non-protein powder | 12 weeks | Not reported | ↑ Skeletal muscle mass, ↓ fat mass, ↑ handgrip strength (NS); safe renal profile |
| Azhar et al., 2021 [23] | 23 elderly HFpEF patients | (1) Control, (2) whey protein supplement (3) EAA supplement | See arms | 12 weeks | Not reported | ↑ 6MWD, gait speed, quadriceps strength (only in protein + exercise group) |
| Herrera-Martínez et al., 2024 [24] | 38 chronic HF (66% sarcopenic) | Mediterranean diet + high-protein ONS + vitamin D | Mediterranean diet + vitamin D (no ONS) | 24 weeks | ↓ NT-proBNP, ↑ LVEF (34% to 45%) in intervention | ↑ Lean mass, ↓ fat gain, improved body composition, and QoL |
| Study Author, Year | Design (Sample, Duration) | Risk of Bias Rating * | Rationale |
|---|---|---|---|
| Broqvist et al., 1994 [15] | RCT (n = 21), 8 weeks; high-protein ONS vs. placebo ONS | Moderate | Although a placebo was used, the small sample size and limited detail on randomization and allocation concealment raise some concerns. |
| Aquilani et al., 2008 [16] | Controlled trial (n ≈ 30 †), 2 months; EAA supplement vs. no supplement | High Risk | The controlled trial compared essential amino acid supplementation with “no supplements” (i.e., a non-placebo control), making blinding and control for confounders problematic. |
| Rozentryt et al., 2010 [17] | RCT (double-blind, n = 29), 18 weeks; high-calorie/protein ONS vs. placebo | Low Risk | This study used a placebo-controlled design in a cachectic population with objective outcomes (weight changes, QoL, and inflammatory markers), supporting robust internal validity. |
| Bonilla-Palomas et al., 2016 [18] | RCT (n = 120), 6–12 months; personalized nutrition & ONS vs. standard care | Moderate | The individualized nutritional intervention versus standard care was performed open-label; although objective outcomes were assessed, the lack of blinding introduces some bias risk. |
| Deutz et al., 2016 [19] | RCT (placebo-controlled, double-blind, n = 652), 90 days, specialized ONS vs. placebo | Low Risk | With a large sample size, a double-blind, placebo-controlled design, and objective endpoints, this trial minimizes potential biases. |
| Pineda-Juárez et al., 2016 [20] | RCT (n = 28), 12 weeks; exercise + BCAA supplementation vs. exercise alone | Moderate | The trial combined exercise with BCAA supplementation versus exercise alone in an unblinded design. Although randomization may have been used, the absence of participant and assessor blinding may impact outcomes. |
| Evangelista et al., 2021 [21] | RCT (n = 67), 3 months; high protein diet vs. standard protein diet. | Moderate | Dietary intervention trials typically face challenges in blinding. This study’s design (high-protein versus standard-protein diets) carries a risk of performance bias even though objective endpoints were measured. |
| Dos Santos et al., 2023 [22] | RCT (n = 25), 12 weeks, whey protein isolate vs. placebo powder | Moderate | Despite using a placebo powder, the small study size and potential for subtle unblinding or expectation bias (given the nature of nutritional supplementation interventions) warrant a moderate rating. |
| Azhar et al., 2021 [23] | RCT (n = 23), 12 weeks, EAA supplement vs. whey protein vs. control (no supplement) | Moderate | The pilot study with multiple arms (control, protein only, and protein plus exercise) was not blinded, and the small sample increased susceptibility to confounding factors. |
| Herrera-Martinez et al., 2024 [24] | RCT (n = 38), 24 weeks, Mediterranean diet alone vs. Mediterranean + ONS+ omega-3 | Moderate | The intervention combined Mediterranean diet advice with high-protein supplements in an open-label setting. The lack of blinding and small sample size contribute to a moderate risk of bias. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evangelista, L.S.; Meraz, R.; Wierenga, K.L.; Nguyen, A.P.; Angosta, A.D.; Kawi, J. High-Protein Dietary Interventions in Heart Failure: A Systematic Review of Clinical and Functional Outcomes. Nutrients 2025, 17, 2361. https://doi.org/10.3390/nu17142361
Evangelista LS, Meraz R, Wierenga KL, Nguyen AP, Angosta AD, Kawi J. High-Protein Dietary Interventions in Heart Failure: A Systematic Review of Clinical and Functional Outcomes. Nutrients. 2025; 17(14):2361. https://doi.org/10.3390/nu17142361
Chicago/Turabian StyleEvangelista, Lorraine S., Rebecca Meraz, Kelly L. Wierenga, Angelina P. Nguyen, Alona D. Angosta, and Jennifer Kawi. 2025. "High-Protein Dietary Interventions in Heart Failure: A Systematic Review of Clinical and Functional Outcomes" Nutrients 17, no. 14: 2361. https://doi.org/10.3390/nu17142361
APA StyleEvangelista, L. S., Meraz, R., Wierenga, K. L., Nguyen, A. P., Angosta, A. D., & Kawi, J. (2025). High-Protein Dietary Interventions in Heart Failure: A Systematic Review of Clinical and Functional Outcomes. Nutrients, 17(14), 2361. https://doi.org/10.3390/nu17142361