
Effect of Almond Milk Versus Cow Milk on Postprandial Glycemia, Lipidemia, and Gastrointestinal Hormones in Patients with Overweight or Obesity and Type 2 Diabetes: A Randomized Controlled Clinical Trial

 , , ,
, , , Highlights
- This randomized, crossover trial provides novel insights into the acute metabolic effects of plant-based milk versus dairy milk on individuals with type 2 diabetes.
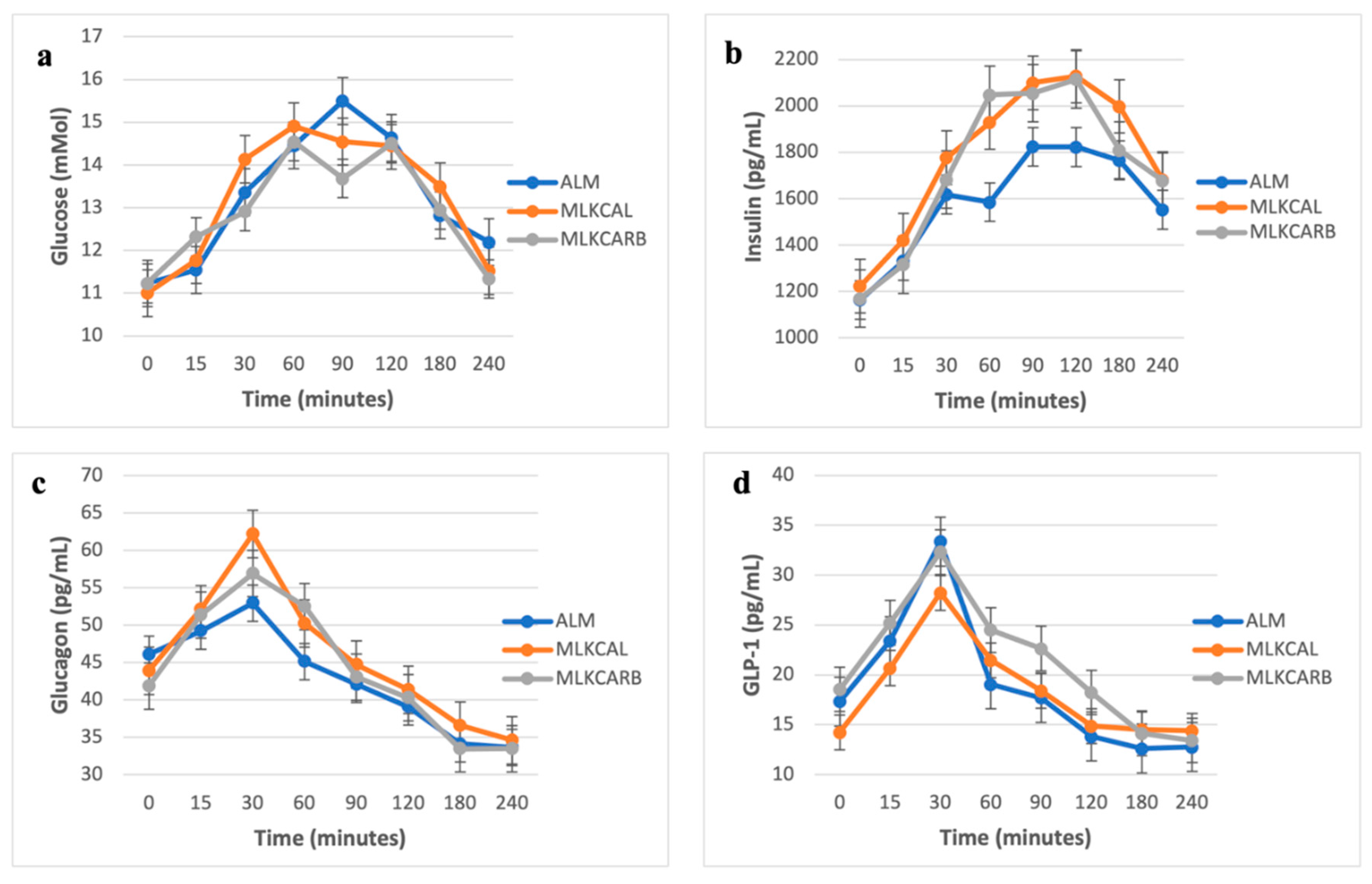
- Almond milk and 2% cow milk produced similar 4-hour postprandial glycemic responses in individuals with type 2 diabetes.
- No significant differences were observed in postprandial free fatty acids, triglycerides, leptins, or gastrointestinal hormones.
- Carbohydrate-matched 2% milk induced significantly higher insulin and glucagon secretion compared to almond milk.
- This highlights the potential influence of milk composition on pancreatic hormone secretions.
Abstract
1. Introduction
2. Methods
2.1. Study Design and Subjects
2.2. Study Procedures
2.3. Sample Collection and Processing
2.4. Sample Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williams, R.; Karuranga, S.; Malanda, B.; Saeedi, P.; Basit, A.; Besançon, S.; Colagiuri, S. Global and regional estimates and projections of diabetes-related health expenditure: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2020, 162, 108072. [Google Scholar] [CrossRef]
- Zhang, K.; Dong, R.; Hu, X.; Ren, C.; Li, Y. Oat-Based Foods: Chemical Constituents, Glycemic Index, and the Effect of Processing. Foods 2021, 10, 1304. [Google Scholar] [CrossRef] [PubMed]
- Walsh, M.C.; Gunn, C. Non-dairy milk substitutes: Are they of adequate nutritional composition? In Milk and Dairy Foods; Elsevier: Amsterdam, The Netherlands, 2020; pp. 347–369. Available online: https://linkinghub.elsevier.com/retrieve/pii/B9780128156032000139 (accessed on 13 August 2024).
- Mitri, J.; Mohd Yusof, B.N.; Maryniuk, M.; Schrager, C.; Hamdy, O.; Salsberg, V. Dairy intake and type 2 diabetes risk factors: A narrative review. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2879–2887. [Google Scholar] [CrossRef] [PubMed]
- Imamura, F.; Micha, R.; Wu, J.H.Y.; De Oliveira Otto, M.C.; Otite, F.O.; Abioye, A.I.; Mozaffarian, D. Effects of Saturated Fat, Polyunsaturated Fat, Monounsaturated Fat, and Carbohydrate on Glucose-Insulin Homeostasis: A Systematic Review and Meta-analysis of Randomised Controlled Feeding Trials. PLOS Med. 2016, 13, e1002087. [Google Scholar] [CrossRef]
- Mann, J. Diet and risk of coronary heart disease and type 2 diabetes. Lancet 2002, 360, 783–789. [Google Scholar] [CrossRef]
- Tomah, S.; Eldib, A.H.; Tasabehji, M.W.; Mitri, J.; Salsberg, V.; Al-Badri, M.R.; Gardner, H.; Hamdy, O. Dairy Consumption and Cardiometabolic Risk Factors in Patients with Type 2 Diabetes and Overweight or Obesity during Intensive Multidisciplinary Weight Management: A Prospective Observational Study. Nutrients 2020, 12, 1643. [Google Scholar] [CrossRef] [PubMed]
- Baylin, A.; Kabagambe, E.K.; Siles, X.; Campos, H. Adipose tissue biomarkers of fatty acid intake. Am. J. Clin. Nutr. 2002, 76, 750–757. [Google Scholar] [CrossRef]
- Zock, P.L.; Mensink, R.P.; Harryvan, J.; de Vries, J.H.; Katan, M.B. Fatty acids in serum cholesteryl esters as quantitative biomarkers of dietary intake in humans. Am. J. Epidemiol. 1997, 145, 1114–1122. [Google Scholar] [CrossRef]
- Zock, P.L.; Mensink, R.P. Dietary trans-fatty acids and serum lipoproteins in humans. Curr. Opin. Lipidol. 1996, 7, 34. [Google Scholar] [CrossRef]
- Unger, R.H.; Cherrington, A.D. Glucagonocentric restructuring of diabetes: A pathophysiologic and therapeutic makeover. J. Clin. Investig. 2012, 122, 4–12. [Google Scholar] [CrossRef]
- van Loon, L.J.C. Leucine as a pharmaconutrient in health and disease. Curr. Opin. Clin. Nutr. Metab. Care. 2012, 15, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, M.; Stenberg, M.; Frid, A.H.; Holst, J.J.; Björck, I.M. Glycemia and insulinemia in healthy subjects after lactose-equivalent meals of milk and other food proteins: The role of plasma amino acids and incretins2. Am. J. Clin. Nutr. 2004, 80, 1246–1253. [Google Scholar] [CrossRef]
- Holst, J.J.; Gromada, J. Role of incretin hormones in the regulation of insulin secretion in diabetic and nondiabetic humans. Am. J. Physiol.-Endocrinol. Metab. 2004, 287, E199–E206. [Google Scholar] [CrossRef]
- McGregor, R.A.; Poppitt, S.D. Milk protein for improved metabolic health: A review of the evidence. Nutr. Metab. 2013, 10, 46. [Google Scholar] [CrossRef]
- Vanga, S.K.; Raghavan, V. How well do plant based alternatives fare nutritionally compared to cow’s milk? J. Food Sci. Technol. 2018, 55, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.O.; Holbrook, M.; Duess, M.A.; Dohadwala, M.M.; Hamburg, N.M.; Asztalos, B.F.; Milbury, P.E.; Blumberg, J.B.; Vita, J.A. Effect of almond consumption on vascular function in patients with coronary artery disease: A randomized, controlled, cross-over trial. Nutr. J. 2015, 14, 61. [Google Scholar] [CrossRef] [PubMed]
- Shkembi, B.; Huppertz, T. Glycemic Responses of Milk and Plant-Based Drinks: Food Matrix Effects. Foods 2023, 12, 453. [Google Scholar] [CrossRef]
- Dos Santos, K.C.; Olofsson, C.; Cunha, J.P.M.C.M.; Roberts, F.; Catrina, S.; Fex, M.; Ekberg, N.R.; Spégel, P. The impact of macronutrient composition on metabolic regulation: An Islet-Centric view. Acta Physiol. 2022, 236, e13884. [Google Scholar] [CrossRef]
- Gadgil, M.D.; Appel, L.J.; Yeung, E.; Anderson, C.A.M.; Sacks, F.M.; Miller, E.R. The Effects of Carbohydrate, Unsaturated Fat, and Protein Intake on Measures of Insulin Sensitivity. Diabetes Care 2013, 36, 1132–1137. [Google Scholar] [CrossRef]
- Dreher, M.L. A Comprehensive Review of Almond Clinical Trials on Weight Measures, Metabolic Health Biomarkers and Outcomes, and the Gut Microbiota. Nutrients 2021, 13, 1968. [Google Scholar] [CrossRef]
- Craig, W.J.; Messina, V.; Rowland, I.; Frankowska, A.; Bradbury, J.; Smetana, S.; Medici, E. Plant-Based Dairy Alternatives Contribute to a Healthy and Sustainable Diet. Nutrients 2023, 15, 3393. [Google Scholar] [CrossRef] [PubMed]
- Walther, B.; Guggisberg, D.; Badertscher, R.; Egger, L.; Portmann, R.; Dubois, S.; Haldimann, M.; Kopf-Bolanz, K.; Rhyn, P.; Zoller, O.; et al. Comparison of nutritional composition between plant-based drinks and cow’s milk. Front. Nutr. 2022, 9, 988707. [Google Scholar] [CrossRef] [PubMed]
- Wien, M.; Bleich, D.; Raghuwanshi, M.; Gould-Forgerite, S.; Gomes, J.; Monahan-Couch, L.; Oda, K. Almond Consumption and Cardiovascular Risk Factors in Adults with Prediabetes. J. Am. Coll. Nutr. 2010, 29, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Gulati, S.; Misra, A.; Pandey, R.M. Effect of Almond Supplementation on Glycemia and Cardiovascular Risk Factors in Asian Indians in North India with Type 2 Diabetes Mellitus: A 24–Week Study. Metab. Syndr. Relat. Disord. 2017, 15, 98–105. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ALM: Oatmeal + Almond Milk (1.5 Cups) * | |
| Carbohydrates | 27.3 g + 12 g = 39.3 g |
| Protein | 5.0 g + 1.5 g = 6.5 g |
| Fat | 3.0 g + 3.8 g = 6.8 g |
| Calories | 150 kcal + 90 kcal = 240 kcal |
| MLKCRB: Oatmeal + Carbohydrate-matched 2% Milk (1 cup) | |
| Carbohydrates | 27.3 g + 12 g = 39.3 g |
| Protein | 5.0 g + 8.1 g = 13.1 g |
| Fat | 3.0 g + 4.8 g = 7.8 g |
| Calories | 150 kcal + 122 kcal = 272 kcal |
| MLKCAL: Oatmeal + Calorie-matched 2% Milk (0.74 cups) | |
| Carbohydrates | 27.3 g + 8.88 g = 36.2 g |
| Protein | 5.0 g + 6.0 g = 11.0 g |
| Fat | 3.0 g + 3.6 g = 6.6 g |
| Calories | 150 kcal + 90 kcal = 240 kcal |
| Gender | |
|---|---|
| Male | 14 (64%) |
| Female | 8 (36%) |
| Age (years) | 66 ± 7.4 |
| BMI (kg/m2) | 30 ± 3.4 |
| Diabetes duration (years) | 11 ± 4.9 |
| Participants using diabetes medications (n) | 22 |
| Participants using lipid-lowering medications (n) | 15 |
| Almond Milk (ALM) | Calorie-Matched 2% Milk (MLKCAL) | Carbohydrate-Matched 2% Milk (MLKCARB) | |
|---|---|---|---|
| Glucose (mM) | 550.23 ± 518.52 | 617.73 ± 424.53 | 474.40 ± 555.05 |
| Insulin (pg/mL) | 119,921.59 ± 166142.80 | 160,748.50 ± 214,665.20 | 160,581.57 ± 177,361.60 * |
| Glucagon (pg/mL) | −1418.86 ± 2151.29 | −162.61 ± 3142.83 | −37.99 ± 1849.96 * |
| Triglycerides (mM) | −21.14 ± 67.07 | 37.50 ± 82.45 * | −16.80 ± 56.04 |
| Active Ghrelin (pg/mL) | −4180.98 ± 9148.15 | −2124.87 ± 7268.45 | 1186.76 ± 5237.95 |
| Total peptide YY (pg/mL) | 779.24 ± 3887.09 | 2273.74 ± 3595.94 | 2823.81 ± 5459.89 |
| Active GLP1 (pg/mL) | −117.61 ± 2968.72 | 760.23 ± 1524.81 | 415.62 ± 3810.31 |
| Active Amylin (pg/mL) | 892.24 ± 1910.84 | 1150.12 ± 1805.47 | 1054.52 ± 1493.46 |
| Leptin (pg/mL) | −348,345.68 ± 435,386.80 | −288,347.73 ± 343,471.50 | −245,751.77 ± 419,293.50 |
| GIP (pg/mL) | 13,890.34 ± 13,590.38 | 15,117.61 ± 7477.78 | 16,124.42 ± 9831.71 |
| Cholecystokinin (pg/mL) | −2896.70 ± 10,809.27 | −2070.00 ± 16,739.91 | −1286.06 ± 13,608.64 |
| Palmitic Acid | 37.50 ± 222.63 | −67.16 ± 250.05 | 58.44 ± 281.24 |
| Stearic Acid | −49.09 ± 122.16 | −6.48 ± 110.69 | 11.79 ± 114.64 |
| Oleic Acid | 18.07 ± 182.15 | −78.75 ± 234.49 | −84.30 ± 154.23 |
| Linoleic Acid | 35.80 ± 150.84 | 14.32 ± 132.45 | −28.78 ± 115.74 |
| Arachidonic Acid | 22.84 ± 138.19 | 29.66 ± 157.69 | 15.10 ± 92.94 |
| Adrenic Acid | −14.32 ± 75.81 | −2.39 ± 66.29 | 12.95 ± 72.35 |
| DHA | 11.59 ± 63.5 | 19.09 ± 93.64 | 26.59 ± 82.18 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dhaver, S.; Al-Badri, M.; Mitri, J.; Barbar Askar, A.A.; Mottalib, A.; Hamdy, O. Effect of Almond Milk Versus Cow Milk on Postprandial Glycemia, Lipidemia, and Gastrointestinal Hormones in Patients with Overweight or Obesity and Type 2 Diabetes: A Randomized Controlled Clinical Trial. Nutrients 2025, 17, 2092. https://doi.org/10.3390/nu17132092
Dhaver S, Al-Badri M, Mitri J, Barbar Askar AA, Mottalib A, Hamdy O. Effect of Almond Milk Versus Cow Milk on Postprandial Glycemia, Lipidemia, and Gastrointestinal Hormones in Patients with Overweight or Obesity and Type 2 Diabetes: A Randomized Controlled Clinical Trial. Nutrients. 2025; 17(13):2092. https://doi.org/10.3390/nu17132092
Chicago/Turabian StyleDhaver, Shilton, Marwa Al-Badri, Joanna Mitri, Abd Almasih Barbar Askar, Adham Mottalib, and Osama Hamdy. 2025. "Effect of Almond Milk Versus Cow Milk on Postprandial Glycemia, Lipidemia, and Gastrointestinal Hormones in Patients with Overweight or Obesity and Type 2 Diabetes: A Randomized Controlled Clinical Trial" Nutrients 17, no. 13: 2092. https://doi.org/10.3390/nu17132092
APA StyleDhaver, S., Al-Badri, M., Mitri, J., Barbar Askar, A. A., Mottalib, A., & Hamdy, O. (2025). Effect of Almond Milk Versus Cow Milk on Postprandial Glycemia, Lipidemia, and Gastrointestinal Hormones in Patients with Overweight or Obesity and Type 2 Diabetes: A Randomized Controlled Clinical Trial. Nutrients, 17(13), 2092. https://doi.org/10.3390/nu17132092