

Curcumin Supplementation Improves Gastrointestinal Symptoms in Women with Severe Obesity: A Double-Blind, Randomized, Placebo-Controlled Trial—A Pilot Study
 , , , and
, , , and
Abstract

1. Introduction
2. Materials and Methods
2.1. Subjects
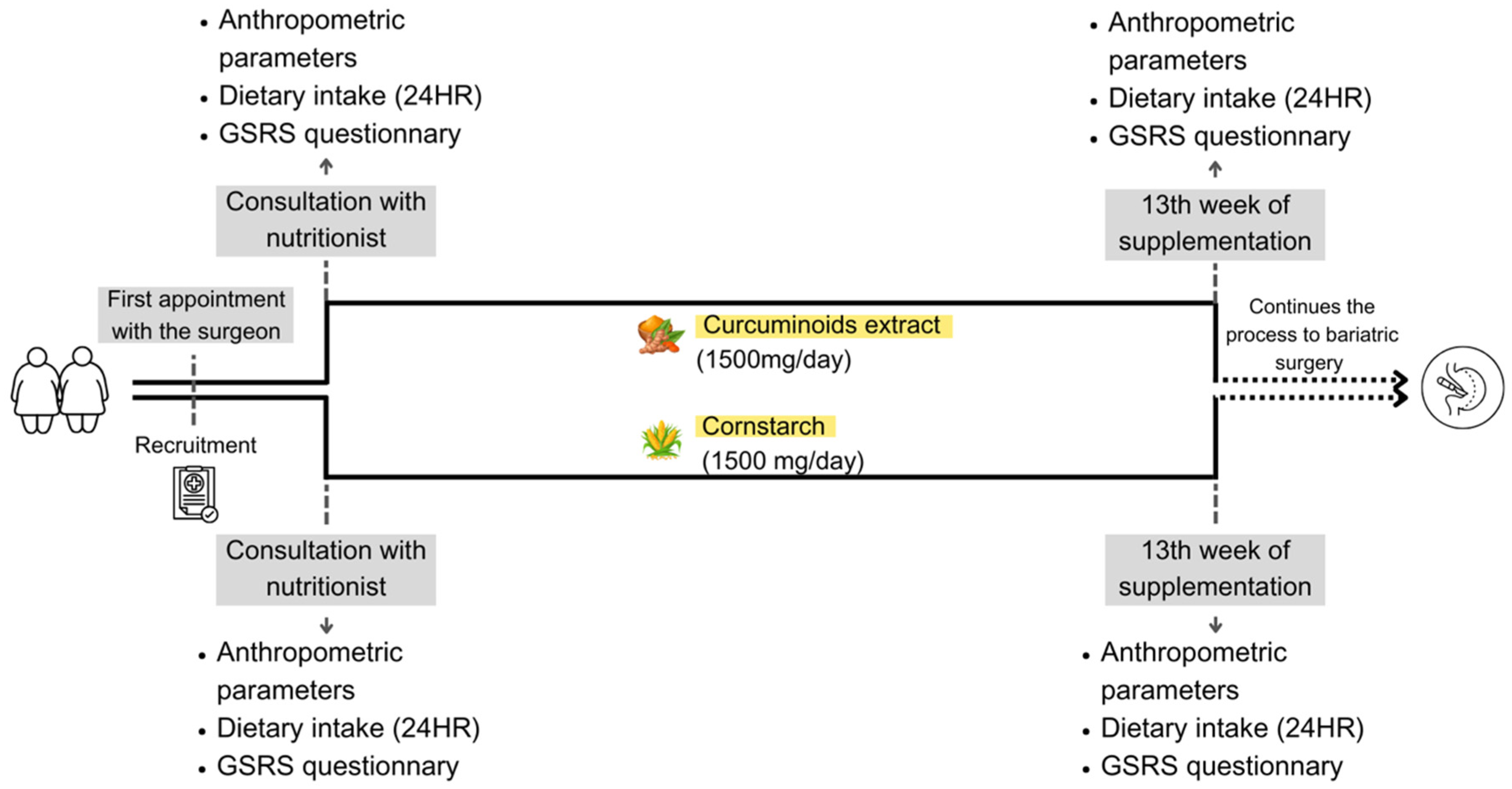
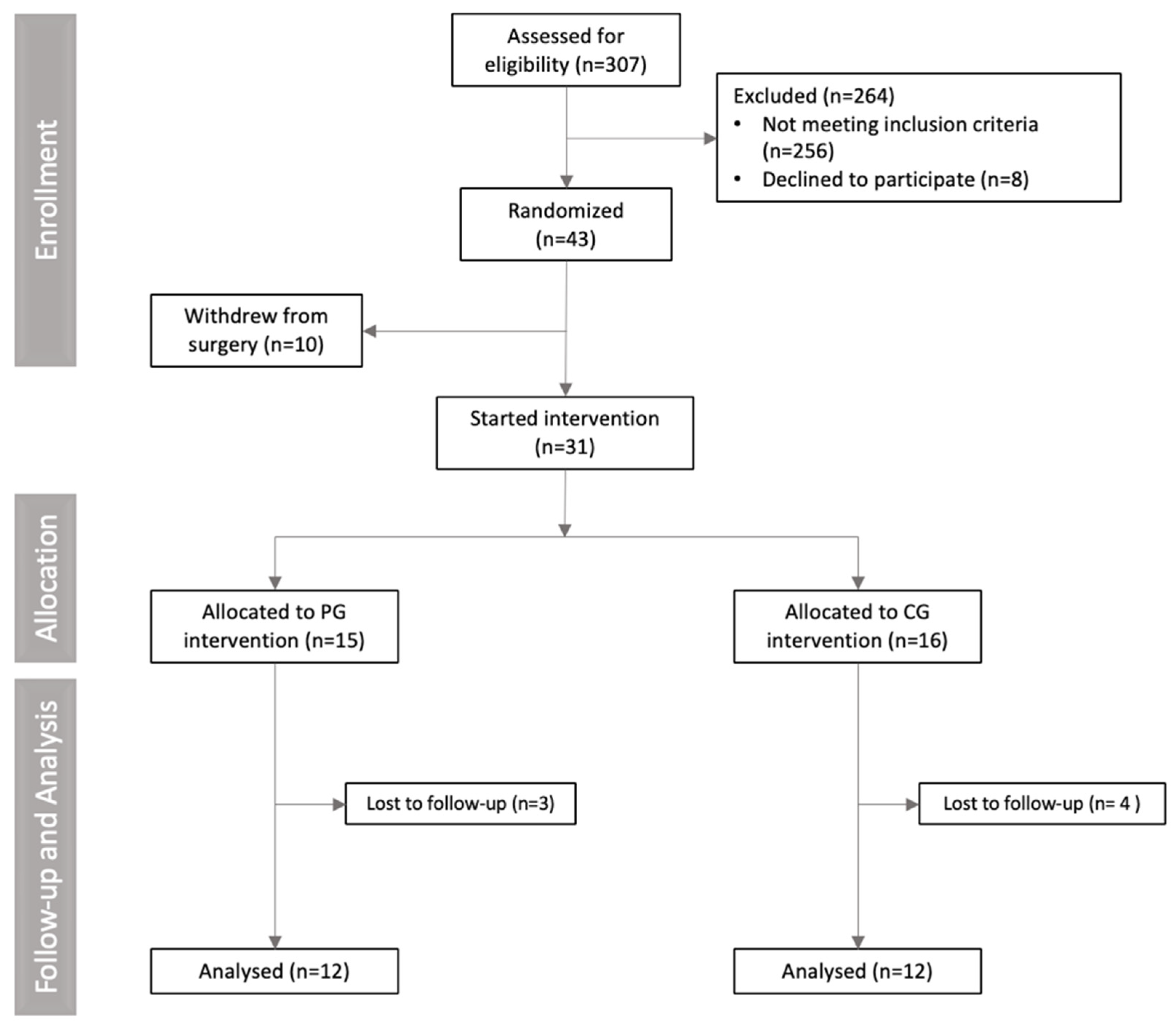
2.2. Experimental Design and Randomization
2.3. Total Score of Gastrointestinal Symptom Rating Scale (GSRS)
2.4. Anthropometric and Food Consumption Assessment
2.5. Statistical Analysis
3. Results
Sample Description
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| CG | Curcumin group |
| GSRS | Gastrointestinal Symptom Rating Scale |
| PG | Placebo group |
| WC | Waist circumference |
| HC | Hip circumference |
| NC | Neck circumference |
References
- Rubino, F.; Cummings, D.E.; Eckel, R.H.; Cohen, R.V.; Wilding, J.P.H.; Brown, W.A.; Stanford, F.C.; Batterham, R.L.; Farooqi, I.S.; Farpour-Lamb, N.J.; et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. 2025, 13, 221–262. [Google Scholar] [CrossRef] [PubMed]
- Steenackers, N.; Eksteen, G.; Wauters, L.; Augustijns, P.; Van der Schueren, B.; Vanuytsel, T.; Matthys, C. Understanding the gastrointestinal tract in obesity: From gut motility patterns to enzyme secretion. Neurogastroenterol. Motil. 2024, 36, e14758. [Google Scholar] [CrossRef] [PubMed]
- Poylin, V.; Serrot, F.J.; Madoff, R.D.; Ikramuddin, S.; Mellgren, A.; Lowry, A.C.; Melton, G.B. Obesity and bariatric surgery: A systematic review of associations with defecatory dysfunction. Color. Dis. 2011, 13, e92–e103. [Google Scholar] [CrossRef]
- Massier, L.; Chakaroun, R.; Tabei, S.; Crane, A.; Didt, K.D.; Fallmann, J.; von Bergen, M.; Haange, S.-B.; Heyne, H.; Stumvoll, M.; et al. Adipose tissue derived bacteria are associated with inflammation in obesity and type 2 diabetes. Gut 2020, 69, 1796–1806. [Google Scholar] [CrossRef]
- Hood, M.M.; Corsica, J.; Bradley, L.; Wilson, R.; Chirinos, D.A.; Vivo, A. Managing severe obesity: Understanding and improving treatment adherence in bariatric surgery. J. Behav. Med. 2016, 39, 1092–1103. [Google Scholar] [CrossRef] [PubMed]
- Abell, T.L.; Minocha, A. Gastrointestinal Complications of Bariatric Surgery: Diagnosis and Therapy. Am. J. Med. Sci. 2006, 331, 214–218. [Google Scholar] [CrossRef]
- Thorsen, B.; Gjeilo, K.H.; Sandvik, J.; Follestad, T.; Græslie, H.; Nymo, S. Self-Reported Gastrointestinal Symptoms Two To Four Years After Bariatric Surgery. A Cross-Sectional Study Comparing Roux-en-Y Gastric Bypass and Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2021, 31, 4338–4346. [Google Scholar] [CrossRef]
- Boerlage, T.C.C.; Westerink, F.; van de Laar, A.W.J.M.; Hutten, B.A.; Brandjes, D.P.M.; Gerdes, V.E.A. Gastrointestinal symptoms before and after laparoscopic Roux-en-Y gastric bypass: A longitudinal assessment. Surg. Obes. Relat. Dis. 2019, 15, 871–877. [Google Scholar] [CrossRef]
- Patcharatrakul, T.; Gonlachanvit, S. Chili Peppers, Curcumins, and Prebiotics in Gastrointestinal Health and Disease. Curr. Gastroenterol. Rep. 2016, 18, 19. [Google Scholar] [CrossRef]
- Chiu, H.-F.; Venkatakrishnan, K.; Golovinskaia, O.; Wang, C.-K. Gastroprotective Effects of Polyphenols against Various Gastro-Intestinal Disorders: A Mini-Review with Special Focus on Clinical Evidence. Molecules 2021, 26, 2090. [Google Scholar] [CrossRef]
- Pan, Y.; Zhao, D.; Yu, N.; An, T.; Miao, J.; Mo, F.; Gu, Y.; Zhang, D.; Gao, S.; Jiang, G. Curcumin improves glycolipid metabolism through regulating peroxisome proliferator activated receptor γ signalling pathway in high-fat diet-induced obese mice and 3T3-L1 adipocytes. R. Soc. Open Sci. 2017, 4, 170917. [Google Scholar] [CrossRef] [PubMed]
- Ghiamati Yazdi, F.; Soleimanian-Zad, S.; van den Worm, E.; Folkerts, G. Turmeric Extract: Potential Use as a Prebiotic and Anti-Inflammatory Compound? Plant Foods Hum. Nutr. 2019, 74, 293–299. [Google Scholar] [CrossRef]
- Yang, C.; Du, Y.; Zhao, T.; Zhao, L.; Liu, L.; Liu, L.; Yang, X. Consumption of dietary turmeric promotes fat browning and thermogenesis in association with gut microbiota regulation in high-fat diet-fed mice. Food Funct. 2024, 15, 8153–8167. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Daza, M.C.; Pulido-Mateos, E.C.; Lupien-Meilleur, J.; Guyonnet, D.; Desjardins, Y.; Roy, D. Polyphenol-Mediated Gut Microbiota Modulation: Toward Prebiotics and Further. Front. Nutr. 2021, 8, 689456. [Google Scholar] [CrossRef] [PubMed]
- Islam, T.; Albracht-Schulte, K.; Ramalingam, L.; Schlabritz-Lutsevich, N.; Park, O.-H.; Zabet-Moghaddam, M.; Kalupahana, N.S.; Moustaid-Moussa, N. Anti-inflammatory mechanisms of polyphenols in adipose tissue: Role of gut microbiota, intestinal barrier integrity and zinc homeostasis. J. Nutr. Biochem. 2023, 115, 109242. [Google Scholar] [CrossRef]
- Bundy, R.; Walker, A.F.; Middleton, R.W.; Booth, J. Turmeric Extract May Improve Irritable Bowel Syndrome Symptomology in Otherwise Healthy Adults: A Pilot Study. J. Altern. Complement. Med. 2004, 10, 1015–1018. [Google Scholar] [CrossRef]
- Cuomo, J.; Appendino, G.; Dern, A.S.; Schneider, E.; McKinnon, T.P.; Brown, M.J.; Togni, S.; Dixon, B.M. Comparative Absorption of a Standardized Curcuminoid Mixture and Its Lecithin Formulation. J. Nat. Prod. 2011, 74, 664–669. [Google Scholar] [CrossRef]
- Souza, G.S.; Sardá, F.A.H.; Giuntini, E.B.; Gumbrevicius, I.; Morais, M.B.; Menezes, E.W. Tradução e validação da versão brasileira do questionário Gastrointestinal Symptom Rating Scale (GSRS). Arq. Gastroenterol. 2016, 53, 146–151. [Google Scholar] [CrossRef]
- Gharagozlian, S.; Mala, T.; Brekke, H.K.; Kolbjørnsen, L.C.; Ullerud, Å.A.; Johnson, E. Nutritional status, sarcopenia, gastrointestinal symptoms and quality of life after gastrectomy for cancer—A cross-sectional pilot study. Clin. Nutr. ESPEN 2020, 37, 195–201. [Google Scholar] [CrossRef]
- Morvaridi, M.; Jafarirad, S.; Seyedian, S.S.; Alavinejad, P.; Cheraghian, B. The effects of extra virgin olive oil and canola oil on inflammatory markers and gastrointestinal symptoms in patients with ulcerative colitis. Eur. J. Clin. Nutr. 2020, 74, 891–899. [Google Scholar] [CrossRef]
- Pereira, S.E.; Rossoni, C.; Cambi, M.P.C.; Faria, S.L.; Mattos, F.C.C.; De Campos, T.B.F.; Petry, T.B.Z.; Silva, S.A.; Pereira, A.Z.; Umeda, L.M.; et al. Brazilian guide to nutrition in bariatric and metabolic surgery. Langenbecks Arch. Surg. 2023, 408, 143. [Google Scholar] [CrossRef] [PubMed]
- Assyov, Y.; Gateva, A.; Tsakova, A.; Kamenov, Z. A comparison of the clinical usefulness of neck circumference and waist circumference in individuals with severe obesity. Endocr. Res. 2017, 42, 6–14. [Google Scholar] [CrossRef]
- Kattah, F.M.; Oliveira, E.S.; Figueiredo, N.; Melo, C.C.; Benetti, B.B.d.C.; Lima, G.B.; Favoritto É, A.M.; Schincaglia, R.M.; Lima, G.C.; Corgosinho, F.C. Proposal for a new cut-off point for waist-to-hip ratio in women with severe obesity: A cross-sectional study. Clin. Nutr. ESPEN 2024, 62, 241–246. [Google Scholar] [CrossRef]
- Conway, J.M.; Ingwersen, L.A.; Vinyard, B.T.; Moshfegh, A.J. Effectiveness of the US Department of Agriculture 5-step multiple-pass method in assessing food intake in obese and nonobese women. Am. J. Clin. Nutr. 2003, 77, 1171–1178. [Google Scholar] [CrossRef]
- Di Mario, F.; Cavallaro, L.G.; Nouvenne, A.; Stefani, N.; Cavestro, G.M.; Iori, V.; Maino, M.; Comparato, G.; Fanigliulo, L.; Morana, E.; et al. A Curcumin-Based 1-Week Triple Therapy for Eradication of Helicobacter pylori Infection: Something to Learn From Failure? Helicobacter 2007, 12, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Boyanova, L.; Medeiros, J.; Yordanov, D.; Gergova, R.; Markovska, R. Turmeric and curcumin as adjuncts in controlling Helicobacter pylori-associated diseases: A narrative review. Lett. Appl. Microbiol. 2024, 77, ovae049. [Google Scholar] [CrossRef] [PubMed]
- Ried, K.; Travica, N.; Dorairaj, R.; Sali, A. Herbal formula improves upper and lower gastrointestinal symptoms and gut health in Australian adults with digestive disorders. Nutr. Res. 2020, 76, 37–51. [Google Scholar] [CrossRef]
- Yao, Y.; Luo, R.; Xiong, S.; Zhang, C.; Zhang, Y. Protective effects of curcumin against rat intestinal inflammation-related motility disorders. Mol. Med. Rep. 2021, 23, 391. [Google Scholar] [CrossRef]
- Dulbecco, P.; Savarino, V. Therapeutic potential of curcumin in digestive diseases. World J. Gastroenterol. 2013, 19, 9256–9270. [Google Scholar] [CrossRef]
- Yang, M.; Wang, J.; Yang, C.; Han, H.; Rong, W.; Zhang, G. Oral administration of curcumin attenuates visceral hyperalgesia through inhibiting phosphorylation of TRPV1 in rat model of ulcerative colitis. Mol. Pain 2017, 13, 1744806917726416. [Google Scholar] [CrossRef]
- Lin, Y.; Liu, H.; Bu, L.; Chen, C.; Ye, X. Review of the Effects and Mechanism of Curcumin in the Treatment of Inflammatory Bowel Disease. Front. Pharmacol. 2022, 13, 908077. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.; Docena, G.; MacDonald, T.T.; Sanderson, I.R. Curcumin suppresses p38 mitogen-activated protein kinase activation, reduces IL-1β and matrix metalloproteinase-3 and enhances IL-10 in the mucosa of children and adults with inflammatory bowel disease. Br. J. Nutr. 2010, 103, 824–832. [Google Scholar] [CrossRef]
- Mousavi, S.M.; Milajerdi, A.; Kord Varkaneh, H.; Gorjipour, M.M.; Esmaillzadeh, A. The effects of curcumin supplementation on body weight, body mass index and waist circumference: A systematic review and dose-response meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2020, 60, 171–180. [Google Scholar] [CrossRef]
- Unhapipatpong, C.; Polruang, N.; Chattranukulchai Shantavasinkul, P.; Julanon, N.; Numthavaj, P.; Thakkinstian, A. The effect of curcumin supplementation on weight loss and anthropometric indices: An umbrella review and updated meta-analyses of randomized controlled trials. Am. J. Clin. Nutr. 2023, 117, 1005–1016. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.S.; Ouyang, A.; Charnigo, R.J.; Westgate, P.M.; Fleenor, B.S. Influence of enhanced bioavailable curcumin on obesity-associated cardiovascular disease risk factors and arterial function: A double-blinded, randomized, controlled trial. Nutrition 2019, 62, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, A.; Sahebkar, A.; Iranshahi, M.; Amini, M.; Khojasteh, R.; Ghayour-Mobarhan, M.; Ferns, G.A. Effects of supplementation with curcuminoids on dyslipidemia in obese patients: A randomized crossover trial. Phytother. Res. 2013, 27, 374–379. [Google Scholar] [CrossRef]
- Esmaily, H.; Sahebkar, A.; Iranshahi, M.; Ganjali, S.; Mohammadi, A.; Ferns, G.; Ghayour-Mobarhan, M. An investigation of the effects of curcumin on anxiety and depression in obese individuals: A randomized controlled trial. Chin. J. Integr. Med. 2015, 21, 332–338. [Google Scholar] [CrossRef]
- Mohajer, A.; Ghayour-Mobarhan, M.; Parizadeh, S.M.R.; Tavallaie, S. Effects of supplementation with curcuminoids on serum copper and zinc concentrations and superoxide dismutase enzyme activity in obese subjects. Trace Elem. Electrolytes 2014, 32, 16–21. [Google Scholar] [CrossRef]
- Jazayeri-Tehrani, S.A.; Rezayat, S.M.; Mansouri, S.; Qorbani, M.; Alavian, S.M.; Daneshi-Maskooni, M.; Hosseinzadeh-Attar, M.-J. Nano-curcumin improves glucose indices, lipids, inflammation, and Nesfatin in overweight and obese patients with non-alcoholic fatty liver disease (NAFLD): A double-blind randomized placebo-controlled clinical trial. Nutr. Metab. 2019, 16, 8. [Google Scholar] [CrossRef]
- Franco-Robles, E.; Campos-Cervantes, A.; Murillo-Ortiz, B.O.; Segovia, J.; López-Briones, S.; Vergara, P.; Pérez-Vázquez, V.; Solís-Ortiz, M.S.; Ramírez-Emiliano, J. Effects of curcumin on brain-derived neurotrophic factor levels and oxidative damage in obesity and diabetes. Appl. Physiol. Nutr. Metab. 2013, 39, 211–218. [Google Scholar] [CrossRef]
- Ataie-Jafari, A.; Namazi, N.; Djalalinia, S.; Chaghamirzayi, P.; Esmaeili Abdar, M.; Sarrafi Zadehe, S.; Asayesh, H.; Zarei, M.; Mahdavi Gorabi, A.; Mansourian, M.; et al. Neck circumference and its association with cardiometabolic risk factors: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2018, 10, 72. [Google Scholar] [CrossRef] [PubMed]
- Stephen, A.M.; Champ, M.-J.; Cloran, S.J.; Fleith, M.; van Lieshout, L.; Mejborn, H.; Burley, V.J. Dietary fibre in Europe: Current state of knowledge on definitions, sources, recommendations, intakes and relationships to health. Nutr. Res. Rev. 2017, 30, 149–190. [Google Scholar] [CrossRef] [PubMed]
- Igudesman, D.; Crandell, J.L.; Corbin, K.D.; Hooper, J.; Thomas, J.M.; Bulik, C.M.; Pence, B.W.; Pratley, R.E.; Kosorok, M.R.; Maahs, D.M.; et al. Associations of Dietary Intake with the Intestinal Microbiota and Short-Chain Fatty Acids Among Young Adults with Type 1 Diabetes and Overweight or Obesity. J. Nutr. 2023, 153, 1178–1188. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Placebo Group | Curcumin Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline (n = 12) | Follow-Up (n = 12) | Delta | p Value † | Baseline (n = 12) | Follow-Up (n = 12) | Delta | p Value † | p Follow-Up § | p Value Delta § | Cohen’s d /Biennial ‡ | |
| Age | 36.09 ± 8.38 | 36.09 ± 8.38 | - | 1.000 | 31.5± 6.38 | 31.5± 6.38 | - | 1.000 | 0.205 | - | - |
| BMI (kg/m2) | 45.03 (41.6–50.9) | 45.29 (40.72–50.9) | 0.268 | 0.832 | 48.35 (42.3–52.9) | 44.1 (41.6–50.3) | −1.67 | 0.273 | 0.895 | 0.019 | 0.017 |
| Weight (kg) | 117.4 (103–127) | 115 (105.6–124 | −12.45 | 0.660 | 119.9 (90.3–143) | 116.7 ± 91.7–144.1 | −3.83 | 0.645 | 0.608 | 0.207 | 0.236 |
| Height (m) | 1.59 (1.52–1.65) | 1.59 (1.52–1.65) | - | 1.000 | 1.61 ± (1.47–1.74) | 1.61 ± (1.47–1.74) | - | 1.000 | - | 0.205 | - |
| WC (cm) | 123.6 ± 10.7 | 122.3 ± 11.02 | −12.72 | 0.787 | 129.6 ± 8.57 | 126.04 ± 10.52 | −3.58 | 0.371 | 0.422 | 0.322 | −0.228 |
| NC (cm) | 37 (34.7–48) | 39 (36–45.5) | 13.86 | 0.147 | 39.8 (36–46.8) | 40.2 (33–45.5) | −0.06 | 0.954 | 0.307 | 0.042 | 0.440 |
| HC (cm) | 135.9 ± 10.5 | 138 ± 9.3 | 29.09 | 0.639 | 138.7 ± 7.43 | 137.7 ± 8.12 | −0.11 | 0.665 | 0.769 | 0.498 | 0.194 |
| GSRS | 28.3 ± 6.40 | 30.25 ± 8.09 | 1.917 | 0.323 | 33.82 ± 9.90 | 30.25 ± 8.09 | −7.36 | 0.004 | 0.253 | 0.003 | −1.17 |
| Bristol Stool Chart | 4 (2–7) | 5 (3–7) | 0.1 | 0.881 | 4 (2–7) | 4 (3–6) | −0.1 | 0.866 | 0.324 | 0.842 | 0.010 |
| Placebo | Curcumin | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline (n = 12) | Follow-Up (n = 12) | Delta | Baseline (n = 12) | Follow-Up (n = 12) | Delta | p Value Follow-Up § | p Value Delta § | Cohen’s d/ Biennial ‡ | |
| Abdominal pain | 1 (1–6) | 1 (1–4) | 0.45 | 1 (1–7) | 1 (1–6) | −0.91 | 0.888 | 0.126 | 0.284 |
| Heartburn | 1 (1–3) | 1 (1–5) | 0.00 | 2 (1–7) | 1 (1–7) | −10.0 | 0.701 | 0.358 | 0.104 |
| Acid regurgitation | 1 (1–2) | 1 (1–7) | 0.36 | 1 (1–7) | 1 (1–7) | −0.66 | 0.402 | 0.240 | 0.250 |
| Hunger pains | 1 (1–4) | 1 (1–5) | 0.00 | 1 (1–5) | 1 (1–4) | −0.08 | 0.716 | 0.848 | 0.000 |
| Nausea/vomiting | 1 (1–3) | 1 (1–7) | 0.36 | 1 (1–6) | 1 (1–7) | −10.00 | 0.674 | 0.365 | 0.194 |
| Borborygmus | 2 (1–7) | 1 (1–5) | −0.54 | 3 (1–7) | 1 (1–3) | −18.33 | 0.325 | 0.320 | −0.434 |
| Bloating | 1 (1–4) | 1 (1–4) | −0.27 | 1 (1–1) | 1 (1–4) | 0.66 | 0.375 | 0.102 | 0.828 |
| Eructation | 3 (1–7) | 4 (1–7) | 0.90 | 3 (1–6) | 2 (1–4) | −10.00 | 0.016 | 0.011 | −0.858 |
| Flatulence | 4 (1–7) | 4 (1–7) | 0.09 | 4.5(1–7) | 2.5 (1–7) | −14.16 | 0.330 | 0.162 | −0.436 |
| Hard stools | 1 (1–2) | 1 (1–1) | −0.09 | 1 (1–7) | 1 (1–4) | −0.75 | 0.186 | 0.284 | 0.187 |
| Constipation | 1 (1–5) | 1 (1–7) | 10.91 | 1 (1–7) | 1 (1–1) | −12.50 | 0.066 | 0.007 | 0.562 |
| Loose stools | 1 (1–7) | 1 (1–7) | 0.72 | 1 (1–7) | 1 (1–4) | −0.66 | 0.082 | 0.278 | 0.291 |
| Diarrhea | 1 (1–5) | 1 (1–2) | −0.36 | 1 (1–4) | 1 (1–4) | −0.16 | 0.045 | 0.968 | −0.006 |
| Urgent need to defecate | 1 (1–4) | 1 (1–2) | −0.63 | 1 (1–6) | 1 (1–4) | −0.41 | 0.608 | 0.765 | −0.062 |
| Incomplete evacuations | 1 (1–6) | 1 (1–6) | 0.81 | 1 (1–5) | 1 (1–5) | −0.50 | 0.162 | 0.107 | 0.333 |
| Placebo | Curcumin | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline (n = 12) | Follow-Up (n = 12) | Delta | p Value † | Baseline (n = 12) | Follow-Up (n = 12) | Delta | p Value † | p Value Follow-up § | p Delta § | Cohen’s d/Biennial ‡ | |
| Energy (kcal) | 1345 ± 744 | 1175 ± 406 | −170.2 | 0.516 | 1655 ± 1310 | 1130 ± 360 | −234.8 | 0.190 | 0.672 | 0.837 | −0.077 |
| Carbohydrate (%) | 52.9 ± 9.77 | 39.67 ± 8.07 | −13.2 | 0.002 | 48.1 ± 10.1 | 47.4 ± 10.6 | 0.91 | 0.873 | 0.131 | 0.008 | 1.130 |
| Protein (%) | 15.58 ± 11.1 | 25.1 ± 10.3 | 9.25 | 0.002 | 21.1 ± 11.1 | 22.2 ± 6.83 | −0.41 | 0.701 | 0.482 | 0.001 | −1.163 |
| Lipid (%) | 31.5 ± 8.47 | 33.2 ± 9.25 | 1.69 | 0.666 | 30.8 ± 8.66 | 30.6 ± 6.57 | −0.24 | 0.953 | 0.538 | 0.708 | 0.003 |
| Total fiber | 8.72 (3.0–30.9) | 9.20 (3.4–13.3) | −1.69 | 0.847 | 10.6 (3.8–34.1) | 8.64 (3.9–12.9) | −1.62 | 0.364 | 0.952 | 0.903 | −0.060 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kattah, F.M.; Figueiredo, N.; Bezerra, K.K.; Oliveira, E.S.; Melo, C.C.d.; Lima, G.B.; Cavalcante, J.P.R.; Benetti, B.B.d.C.; Lima, G.C.; Mota, J.F.; et al. Curcumin Supplementation Improves Gastrointestinal Symptoms in Women with Severe Obesity: A Double-Blind, Randomized, Placebo-Controlled Trial—A Pilot Study. Nutrients 2025, 17, 2064. https://doi.org/10.3390/nu17132064
Kattah FM, Figueiredo N, Bezerra KK, Oliveira ES, Melo CCd, Lima GB, Cavalcante JPR, Benetti BBdC, Lima GC, Mota JF, et al. Curcumin Supplementation Improves Gastrointestinal Symptoms in Women with Severe Obesity: A Double-Blind, Randomized, Placebo-Controlled Trial—A Pilot Study. Nutrients. 2025; 17(13):2064. https://doi.org/10.3390/nu17132064
Chicago/Turabian StyleKattah, Fabiana Martins, Nayra Figueiredo, Kamilla Kenned Bezerra, Emilly Santos Oliveira, Cinara Costa de Melo, Gislene Batista Lima, Jocélia Paula Rocha Cavalcante, Beatriz Bacheschi do Carmo Benetti, Glaucia Carielo Lima, João Felipe Mota, and et al. 2025. "Curcumin Supplementation Improves Gastrointestinal Symptoms in Women with Severe Obesity: A Double-Blind, Randomized, Placebo-Controlled Trial—A Pilot Study" Nutrients 17, no. 13: 2064. https://doi.org/10.3390/nu17132064
APA StyleKattah, F. M., Figueiredo, N., Bezerra, K. K., Oliveira, E. S., Melo, C. C. d., Lima, G. B., Cavalcante, J. P. R., Benetti, B. B. d. C., Lima, G. C., Mota, J. F., & Corgosinho, F. C. (2025). Curcumin Supplementation Improves Gastrointestinal Symptoms in Women with Severe Obesity: A Double-Blind, Randomized, Placebo-Controlled Trial—A Pilot Study. Nutrients, 17(13), 2064. https://doi.org/10.3390/nu17132064