

The Effectiveness of Time-Restricted Eating as an Intermittent Fasting Approach on Shift Workers’ Glucose Metabolism: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Screening and Eligibility
2.4. Data Extraction
2.5. Methodological Quality Appraisal
2.6. Overall Evidence Grading
2.7. Data Analysis
3. Results
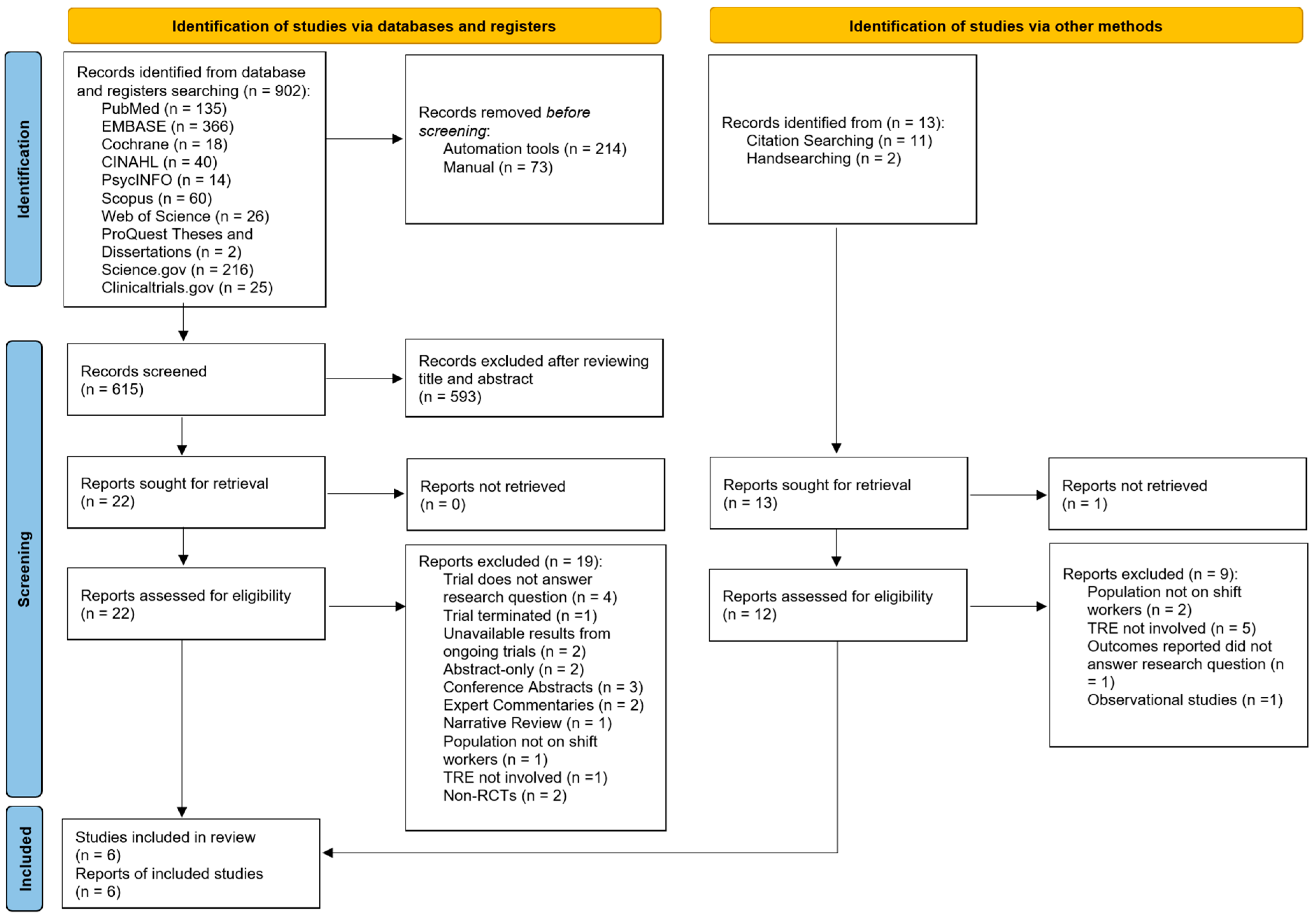
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Methodological Quality
3.4. Overall Certainty of Evidence
3.5. Outcomes
3.5.1. Fasting Blood Glucose
3.5.2. Fasting Blood Insulin
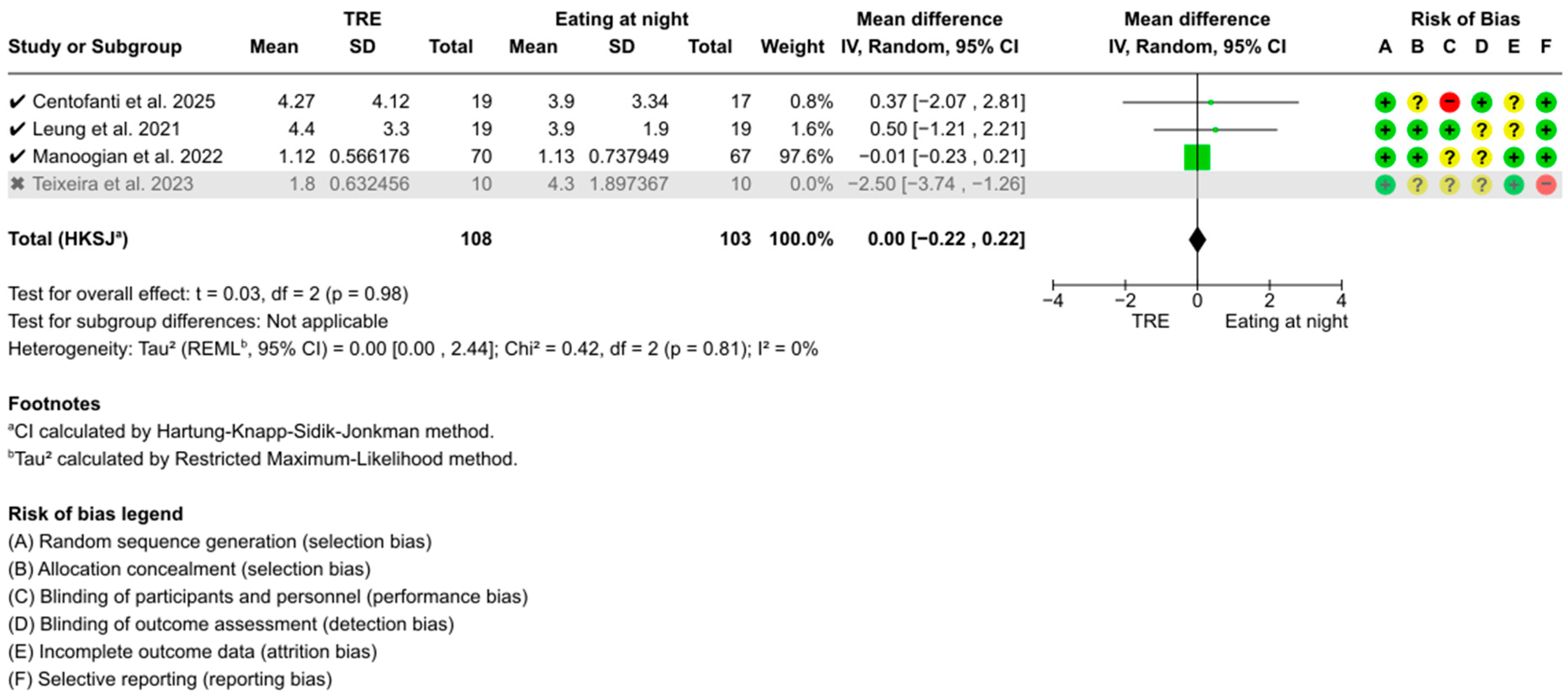
3.5.3. HOMA-IR
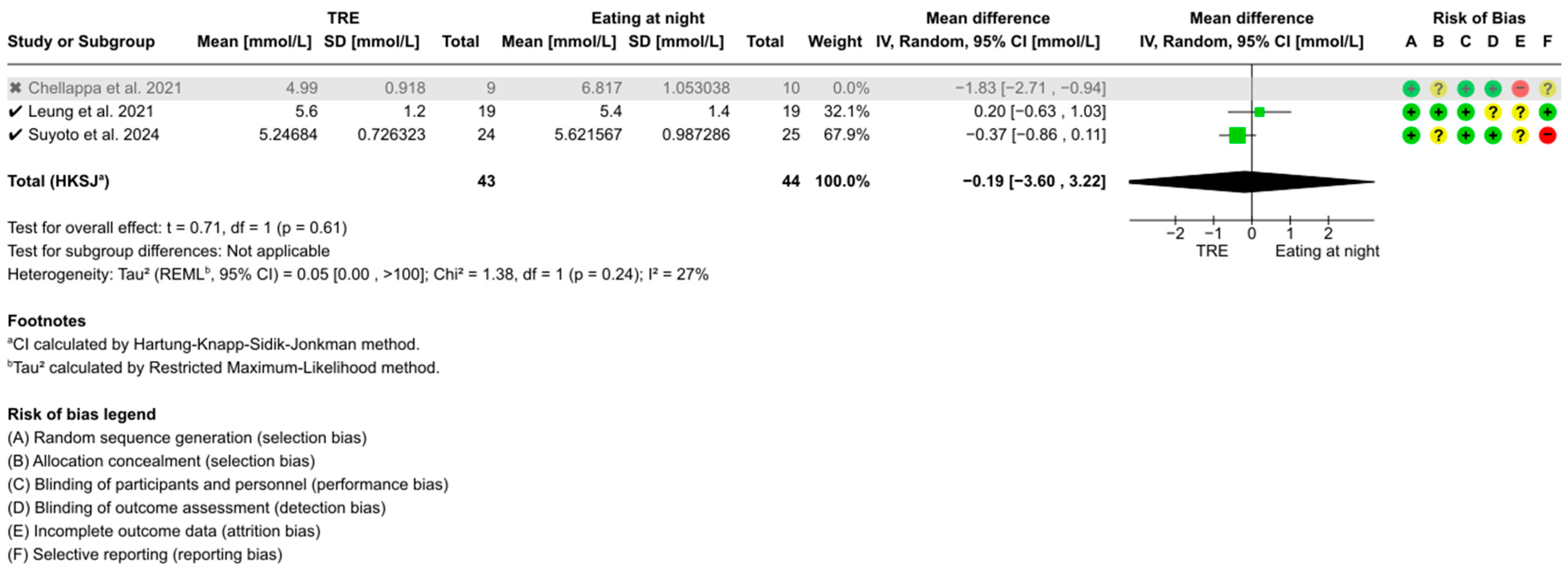
3.5.4. Two-Hour Postprandial Glucose
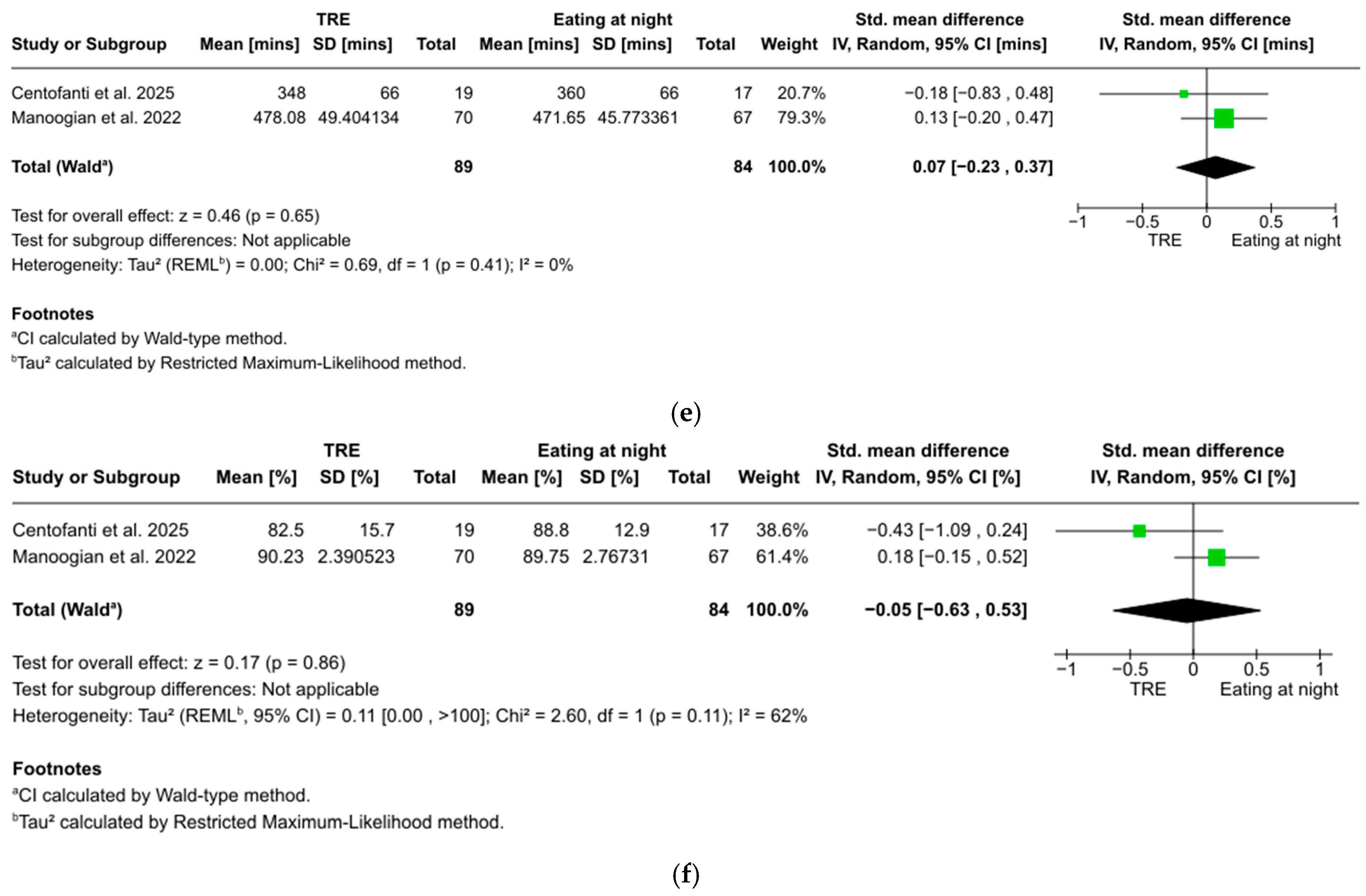
3.5.5. Total Sleep Time
3.5.6. Sleep Efficiency
3.5.7. Sensitivity Analyses
3.5.8. Narrative Summary
4. Discussion
4.1. Summary of Findings
4.2. Glucose Regulation (FBG, 2 Hour Postprandial Glucose, Fasting Blood Insulin, HOMA-IR)
4.3. Sleep (Total Sleep Time, Sleep Efficiency)
4.4. Implications for Future Research and Practice
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| FBG | Fasting blood glucose |
| CMD | Cardiometabolic disease |
| SCN | Suprachiasmatic nucleus |
| TRE | Time-restricted eating |
| HbA1c | Glycated hemoglobin |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PROSPERO | International Prospective Register of Systematic Reviews |
| PICO | Population, intervention, control, outcome |
| HOMA-IR | Homeostatic Model Assessment of Insulin Resistance |
| RCT | Randomized controlled trial |
| SD | Standard deviation |
| RoB-1 | Risk of bias-1 |
| GRADE | Grading of Recommendations, Assessment, Development, and Evaluation |
| CI | Confidence interval |
| SE | Standard error |
| WMD | Weighted mean difference |
| SMD | Standardized mean difference |
| CVD | Cardiovascular disease |
| ITT | Intention-to-treat |
Appendix A


References
- Reinganum, M.I.; Thomas, J. Shift Work Hazards. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Cao, Y.; Feng, Y.; Xia, N.; Zhang, J.-C. Evaluating the impact of shift work on the risk of cardiometabolic disease: A Mendelian randomization study. Nutr. Metab. Cardiovasc. Dis. 2024, 34, 2720–2728. [Google Scholar] [CrossRef] [PubMed]
- Soltanzadeh, A.; Eyvazlou, M.; Mohammad-ghasemi, M.; Sadeghi-Yarandi, M.; Rahimkhani, M.; Ghasemi, N.; Bonyadi, M.; Sadeghi-Yarandi, M. Investigating the relationship between shift work schedule and blood and metabolic parameters: A 10-years retrospective cohort study. Sci. Rep. 2024, 14, 17297. [Google Scholar] [CrossRef]
- Poggiogalle, E.; Jamshed, H.; Peterson, C.M. Circadian regulation of glucose, lipid, and energy metabolism in humans. Metabolism 2018, 84, 11–27. [Google Scholar] [CrossRef]
- Morris, C.J.; Yang, J.N.; Garcia, J.I.; Myers, S.; Bozzi, I.; Wang, W.; Buxton, O.M.; Shea, S.A.; Scheer, F.A.J.L. Endogenous circadian system and circadian misalignment impact glucose tolerance via separate mechanisms in humans. Proc. Natl. Acad. Sci. USA 2015, 112, E2225–E2234. [Google Scholar] [CrossRef]
- Lu, X.; Xie, Q.; Pan, X.; Zhang, R.; Zhang, X.; Peng, G.; Zhang, Y.; Shen, S.; Tong, N. Type 2 diabetes mellitus in adults: Pathogenesis, prevention and therapy. Signal Transduct. Target. Ther. 2024, 9, 262. [Google Scholar] [CrossRef] [PubMed]
- Giri, B.; Dey, S.; Das, T.; Sarkar, M.; Banerjee, J.; Dash, S.K. Chronic hyperglycemia mediated physiological alteration and metabolic distortion leads to organ dysfunction, infection, cancer progression and other pathophysiological consequences: An update on glucose toxicity. Biomed. Pharmacother. 2018, 107, 306–328. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Lee, J.-W.; Choi, W.S.; Myong, J.-P. Dose-Response Relationship between Night Work and the Prevalence of Impaired Fasting Glucose: The Korean Worker’s Special Health Examination for Night Workers Cohort. Int. J. Environ. Res. Public Health 2021, 18, 1854. [Google Scholar] [CrossRef]
- Gupta, C.C.; Vincent, G.E.; Coates, A.M.; Khalesi, S.; Irwin, C.; Dorrian, J.; Ferguson, S.A. A Time to Rest, a Time to Dine: Sleep, Time-Restricted Eating, and Cardiometabolic Health. Nutrients 2022, 14, 420. [Google Scholar] [CrossRef]
- Pickel, L.; Sung, H.-K. Feeding Rhythms and the Circadian Regulation of Metabolism. Front. Nutr. 2020, 7, 39. [Google Scholar] [CrossRef]
- Ahluwalia, M.K. Chrononutrition—When We Eat Is of the Essence in Tackling Obesity. Nutrients 2022, 14, 5080. [Google Scholar] [CrossRef]
- Lee, J.; Liu, R.; De Jesus, D.; Kim, B.S.; Ma, K.; Moulik, M.; Yechoor, V. Circadian control of β-cell function and stress responses. Diabetes Obes. Metab. 2015, 17, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Mason, I.C.; Qian, J.; Adler, G.K.; Scheer, F.A.J.L. Impact of circadian disruption on glucose metabolism: Implications for type 2 diabetes. Diabetologia 2020, 63, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Molzof, H.E.; Peterson, C.M.; Thomas, S.J.; Gloston, G.F.; Johnson, R.L.; Gamble, K.L. Nightshift Work and Nighttime Eating Are Associated with Higher Insulin and Leptin Levels in Hospital Nurses. Front. Endocrinol. 2022, 13, 876752. [Google Scholar] [CrossRef]
- Waldman, H.S.; Renteria, L.I.; McAllister, M.J. Time-restricted feeding for the prevention of cardiometabolic diseases in high-stress occupations: A mechanistic review. Nutr. Rev. 2020, 78, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Gallant, A.; Lundgren, J.; Drapeau, V. Nutritional Aspects of Late Eating and Night Eating. Curr. Obes. Rep. 2014, 3, 101–107. [Google Scholar] [CrossRef]
- Gu, C.; Brereton, N.; Schweitzer, A.; Cotter, M.; Duan, D.; Børsheim, E.; Wolfe, R.R.; Pham, L.V.; Polotsky, V.Y.; Jun, J.C. Metabolic Effects of Late Dinner in Healthy Volunteers—A Randomized Crossover Clinical Trial. J. Clin. Endocrinol. Metab. 2020, 105, 2789–2802. [Google Scholar] [CrossRef]
- Marot, L.P.; Lopes, T.D.V.C.; Balieiro, L.C.T.; Crispim, C.A.; Moreno, C.R.C. Impact of Nighttime Food Consumption and Feasibility of Fasting during Night Work: A Narrative Review. Nutrients 2023, 15, 2570. [Google Scholar] [CrossRef]
- Regmi, P.; Heilbronn, L.K. Time-Restricted Eating: Benefits, Mechanisms, and Challenges in Translation. iScience 2020, 23, 101161. [Google Scholar] [CrossRef]
- Che, T.; Yan, C.; Tian, D.; Zhang, X.; Liu, X.; Wu, Z. Time-restricted feeding improves blood glucose and insulin sensitivity in overweight patients with type 2 diabetes: A randomised controlled trial. Nutr. Metab. 2021, 18, 88. [Google Scholar] [CrossRef]
- Rastogi, S.; Verma, N.; Raghuwanshi, G.S.; Atam, V.; Kumar Verma, D. The Impact of Time-Restricted Meal Intake on Glycemic Control and Weight Management in Type 2 Diabetes Mellitus Patients: An 18-Month Longitudinal Study. Cureus 2024, 16, e53680. [Google Scholar] [CrossRef]
- Rothschild, J.; Hoddy, K.K.; Jambazian, P.; Varady, K.A. Time-restricted feeding and risk of metabolic disease: A review of human and animal studies. Nutr. Rev. 2014, 72, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Paschos, G.K. Diurnal rhythms and obesity. Curr. Opin. Clin. Nutr. Metab. Care 2021, 24, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarek, J.L.; Thompson, S.V.; Holscher, H.D. Complex interactions of circadian rhythms, eating behaviors, and the gastrointestinal microbiota and their potential impact on health. Nutr. Rev. 2017, 75, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Goens, D.; Virzi, N.E.; Jung, S.E.; Rutledge, T.R.; Zarrinpar, A. Obesity, Chronic Stress, and Stress Reduction. Gastroenterol. Clin. N. Am. 2023, 52, 347–362. [Google Scholar] [CrossRef]
- Marhefkova, N.; Sládek, M.; Sumová, A.; Dubsky, M. Circadian dysfunction and cardio-metabolic disorders in humans. Front. Endocrinol. 2024, 15, 1328139. [Google Scholar] [CrossRef]
- Ribas-Latre, A.; Fernández-Veledo, S.; Vendrell, J. Time-restricted eating, the clock ticking behind the scenes. Front. Pharmacol. 2024, 15, 1428601. [Google Scholar] [CrossRef]
- Takahashi, M.; Tahara, Y. Timing of Food/Nutrient Intake and Its Health Benefits: Chrono-Nutrition (SY(T1)4). J. Nutr. Sci. Vitaminol. 2022, 68, S2–S4. [Google Scholar] [CrossRef]
- Engin, A. Misalignment of Circadian Rhythms in Diet-Induced Obesity. In Obesity and Lipotoxicity; Engin, A.B., Engin, A., Eds.; Springer International Publishing: Cham, Switzerland, 2024; Volume 1460, pp. 27–71. Available online: https://link.springer.com/10.1007/978-3-031-63657-8_2 (accessed on 22 November 2024).
- Sebti, Y.; Hebras, A.; Pourcet, B.; Staels, B.; Duez, H. The Circadian Clock and Obesity. In From Obesity to Diabetes; Eckel, J., Clément, K., Eds.; Springer International Publishing: Cham, Switzerland, 2022; Volume 274, pp. 29–56. Available online: https://link.springer.com/10.1007/164_2021_579 (accessed on 22 November 2024).
- Tsitsou, S.; Zacharodimos, N.; Poulia, K.-A.; Karatzi, K.; Dimitriadis, G.; Papakonstantinou, E. Effects of Time-Restricted Feeding and Ramadan Fasting on Body Weight, Body Composition, Glucose Responses, and Insulin Resistance: A Systematic Review of Randomized Controlled Trials. Nutrients 2022, 14, 4778. [Google Scholar] [CrossRef]
- Adafer, R.; Messaadi, W.; Meddahi, M.; Patey, A.; Haderbache, A.; Bayen, S.; Messaadi, N. Food Timing, Circadian Rhythm and Chrononutrition: A Systematic Review of Time-Restricted Eating’s Effects on Human Health. Nutrients 2020, 12, 3770. [Google Scholar] [CrossRef]
- Sepúlveda, B.; Marín, A.; Burrows, R.; Sepúlveda, A.; Chamorro, R. It’s About Timing: Contrasting the Metabolic Effects of Early vs. Late Time-Restricted Eating in Humans. Curr. Nutr. Rep. 2024, 13, 214–239. [Google Scholar] [CrossRef]
- Pellegrini, M.; Cioffi, I.; Evangelista, A.; Ponzo, V.; Goitre, I.; Ciccone, G.; Ghigo, E.; Bo, S. Effects of time-restricted feeding on body weight and metabolism. A systematic review and meta-analysis. Rev. Endocr. Metab. Disord. 2020, 21, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Rovira-Llopis, S.; Luna-Marco, C.; Perea-Galera, L.; Bañuls, C.; Morillas, C.; Victor, V.M. Circadian alignment of food intake and glycaemic control by time-restricted eating: A systematic review and meta-analysis. Rev. Endocr. Metab. Disord. 2024, 25, 325–337. [Google Scholar] [CrossRef]
- Qi, D.; Nie, X.; Zhang, J. A Systematic Review and Meta-Analysis of the Impacts of Time-Restricted Eating on Metabolic Homeostasis. Angiology 2024, 00033197241228046. [Google Scholar] [CrossRef]
- Vekic, J.; Silva-Nunes, J.; Rizzo, M. Glucose Metabolism Disorders: Challenges and Opportunities for Diagnosis and Treatment. Metabolites 2022, 12, 712. [Google Scholar] [CrossRef]
- Speksnijder, E.M.; Bisschop, P.H.; Siegelaar, S.E.; Stenvers, D.J.; Kalsbeek, A. Circadian desynchrony and glucose metabolism. J. Pineal Res. 2024, 76, e12956. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Ross-White, A.; Lieggi, M.; Palacio, F.G.L.; Solomons, T.; Swab, M.; Rothfus, M.; Takahashi, J.; Cardoso, D. Section 2.4: Search Methodology for JBI Evidence Syntheses. In JBI Manual for Evidence Synthesis, 2024 ed.; Aromataris, E., Lockwood, C., Porritt, K., Pilla, B., Jordan, Z., Eds.; JBI: Adelaide, Australia, 2024; Available online: https://jbi-global-wiki.refined.site/space/MANUAL/355827873/2.4+Search+Methodology+for+JBI+Evidence+Syntheses (accessed on 22 November 2024).
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; Version 6.5; Cochrane: London, UK, 2024; Available online: https://training.cochrane.org/handbook (accessed on 22 November 2024).
- Rohatgi, A. WebPlotDigitizer. Version 5.2. Available online: https://automeris.io/ (accessed on 22 November 2024).
- Higgins, J.P.T.; Altman, D.G.; Sterne, J.A.C. Chapter 8: Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0; Higgins, J.P.T., Green, S., Eds.; Cochrane: London, UK, 2011; Available online: https://handbook-5-1.cochrane.org/chapter_8/8_assessing_risk_of_bias_in_included_studies.htm (accessed on 22 November 2024).
- GRADEpro GDT. GRADEpro Guideline Development Tool; McMaster University and Evidence Prime: Hamilton, ON, Canada, 2024; Available online: https://www.gradepro.org (accessed on 22 November 2024).
- Schünemann, H.; Brożek, J.; Guyatt, G.; Oxman, A. GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations, 2013 ed.; The GRADE Working Group: Hamilton, ON, Canada, 2013; Available online: https://gdt.gradepro.org/app/handbook/handbook.html (accessed on 22 November 2024).
- Hedges, L.V.; Olkin, I. Statistical Methods for Meta-Analysis; Academic Press: Orlando, FL, USA, 1985. [Google Scholar]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Chapter 10: Analysing Data and Undertaking Meta-Analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Version 6.5; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2024; Available online: https://training.cochrane.org/handbook/current/chapter-10 (accessed on 22 November 2024).
- Veroniki, A.; McKenzie, J. Introduction to New Random-Effects Methods in RevMan. Cochrane Methods. 2024. Available online: https://training.cochrane.org/sites/training.cochrane.org/files/public/uploads/Introduction%20to%20new%20random-effects%20methods%20in%20RevMan.pdf (accessed on 22 November 2024).
- Page, M.J.; Higgins, J.P.T.; Sterne, J.A.C. Chapter 13: Assessing Risk of Bias Due to Missing Evidence in a Meta-Analysis. In Cochrane Handbook for Systematic Reviews of Interventions; Version 6.5; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2024; Available online: https://training.cochrane.org/handbook/current/chapter-13 (accessed on 22 November 2024).
- Centofanti, S.; Heilbronn, L.K.; Wittert, G.; Dorrian, J.; Coates, A.M.; Kennaway, D.; Gupta, C.; Stepien, J.M.; Catcheside, P.; Yates, C.; et al. Fasting as an intervention to alter the impact of simulated night-shift work on glucose metabolism in healthy adults: A cluster randomised controlled trial. Diabetologia 2025, 68, 203–216. [Google Scholar] [CrossRef]
- Chellappa, S.L.; Qian, J.; Vujovic, N.; Morris, C.J.; Nedeltcheva, A.; Nguyen, H.; Rahman, N.; Heng, S.W.; Kelly, L.; Kerlin-Monteiro, K.; et al. Daytime eating prevents internal circadian misalignment and glucose intolerance in night work. Sci. Adv. 2021, 7, eabg9910. [Google Scholar] [CrossRef]
- Leung, G.K.W.; Davis, R.; Huggins, C.E.; Ware, R.S.; Bonham, M.P. Does rearranging meal times at night improve cardiovascular risk factors? An Australian pilot randomised trial in night shift workers. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1890–1902. [Google Scholar] [CrossRef]
- Manoogian, E.N.C.; Zadourian, A.; Lo, H.C.; Gutierrez, N.R.; Shoghi, A.; Rosander, A.; Pazargadi, A.; Ormiston, C.K.; Wang, X.; Sui, J.; et al. Feasibility of time-restricted eating and impacts on cardiometabolic health in 24-h shift workers: The Healthy Heroes randomized control trial. Cell Metab. 2022, 34, 1442–1456.e7. [Google Scholar] [CrossRef]
- Suyoto, P.S.; De Rijk, M.G.; De Vries, J.H.; Feskens, E.J. The Effect of Meal Glycemic Index and Meal Frequency on Glycemic Control and Variability in Female Nurses Working Night Shifts: A Two-Arm Randomized Cross-Over Trial. J. Nutr. 2024, 154, 69–78. [Google Scholar] [CrossRef]
- Teixeira, B.S.; Silva, C.M.; Silva, A.T.F.; Santos, L.L.D.; De Paiva Maia, Y.C.; Pedrazzoli, M.; Wright, K.P.; Crispim, C.A. Influence of fasting during the night shift on next day eating behavior, hunger, and glucose and insulin levels: A randomized, three-condition, crossover trial. Eur. J. Nutr. 2023, 62, 1281–1293. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef] [PubMed]
- Columb, M.; Atkinson, M. Statistical analysis: Sample size and power estimations. BJA Educ. 2016, 16, 159–161. [Google Scholar] [CrossRef]
- Guolo, A.; Varin, C. Random-effects meta-analysis: The number of studies matters. Stat. Methods Med. Res. 2017, 26, 1500–1518. [Google Scholar] [CrossRef]
- Vasim, I.; Majeed, C.N.; DeBoer, M.D. Intermittent Fasting and Metabolic Health. Nutrients 2022, 14, 631. [Google Scholar] [CrossRef]
- Anton, S.D.; Moehl, K.; Donahoo, W.T.; Marosi, K.; Lee, S.A.; Mainous, A.G.; Leeuwenburgh, C.; Mattson, M.P. Flipping the Metabolic Switch: Understanding and Applying the Health Benefits of Fasting. Obesity 2018, 26, 254–268. [Google Scholar] [CrossRef]
- Jackson, D. The power of the standard test for the presence of heterogeneity in meta-analysis. Stat. Med. 2006, 25, 2688–2699. [Google Scholar] [CrossRef]
- Sun, M.-L.; Yao, W.; Wang, X.-Y.; Gao, S.; Varady, K.A.; Forslund, S.K.; Zhang, M.; Shi, Z.-Y.; Cao, F.; Zou, B.-J.; et al. Intermittent fasting and health outcomes: An umbrella review of systematic reviews and meta-analyses of randomised controlled trials. eClinicalMedicine 2024, 70, 102519. [Google Scholar] [CrossRef]
- Parr, E.B.; Devlin, B.L.; Radford, B.E.; Hawley, J.A. A Delayed Morning and Earlier Evening Time-Restricted Feeding Protocol for Improving Glycemic Control and Dietary Adherence in Men with Overweight/Obesity: A Randomized Controlled Trial. Nutrients 2020, 12, 505. [Google Scholar] [CrossRef]
- Martens, C.R.; Rossman, M.J.; Mazzo, M.R.; Jankowski, L.R.; Nagy, E.E.; Denman, B.A.; Richey, J.J.; Johnson, S.A.; Ziemba, B.P.; Wang, Y.; et al. Short-term time-restricted feeding is safe and feasible in non-obese healthy midlife and older adults. GeroScience 2020, 42, 667–686. [Google Scholar] [CrossRef] [PubMed]
- Bao, R.; Sun, Y.; Jiang, Y.; Ye, L.; Hong, J.; Wang, W. Effects of Time-Restricted Feeding on Energy Balance: A Cross-Over Trial in Healthy Subjects. Front. Endocrinol. 2022, 13, 870054. [Google Scholar] [CrossRef]
- Liang, X.; Chen, J.; An, X.; Ren, Y.; Liu, Q.; Huang, L.; Zhang, P.; Qu, P.; Li, J. The optimal time restricted eating interventions for blood pressure, weight, fat mass, glucose, and lipids: A meta-analysis and systematic review. Trends Cardiovasc. Med. 2024, 34, 389–401. [Google Scholar] [CrossRef] [PubMed]
- Akasheh, R.T.; Ankireddy, A.; Gabel, K.; Ezpeleta, M.; Lin, S.; Tamatam, C.M.; Reddy, S.P.; Spring, B.; Cheng, T.-Y.D.; Fontana, L.; et al. Effect of Time-Restricted Eating on Circulating Levels of IGF1 and Its Binding Proteins in Obesity: An Exploratory Analysis of a Randomized Controlled Trial. Nutrients 2024, 16, 3476. [Google Scholar] [CrossRef]
- Chang, Y.; Du, T.; Zhuang, X.; Ma, G. Time-restricted eating improves health because of energy deficit and circadian rhythm: A systematic review and meta-analysis. iScience 2024, 27, 109000. [Google Scholar] [CrossRef] [PubMed]
- Molcan, L.; Babarikova, K.; Cvikova, D.; Kincelova, N.; Kubincova, L.; Mauer Sutovska, H. Artificial light at night suppresses the day-night cardiovascular variability: Evidence from humans and rats. Pflügers Arch.-Eur. J. Physiol. 2024, 476, 295–306. [Google Scholar] [CrossRef]
- Niijima, A.; Nagai, K.; Nagai, N.; Nakagawa, H. Light enhances sympathetic and suppresses vagal outflows and lesions including the suprachiasmatic nucleus eliminate these changes in rats. J. Auton. Nerv. Syst. 1992, 40, 155–160. [Google Scholar] [CrossRef]
- Masís-Vargas, A.; Hicks, D.; Kalsbeek, A.; Mendoza, J. Blue light at night acutely impairs glucose tolerance and increases sugar intake in the diurnal rodent Arvicanthis ansorgei in a sex-dependent manner. Physiol. Rep. 2019, 7, e14257. [Google Scholar] [CrossRef]
- Mason, I.C.; Grimaldi, D.; Reid, K.J.; Warlick, C.D.; Malkani, R.G.; Abbott, S.M.; Zee, P.C. Light exposure during sleep impairs cardiometabolic function. Proc. Natl. Acad. Sci. USA 2022, 119, e2113290119. [Google Scholar] [CrossRef]
- Broussard, J.L.; Knud-Hansen, B.C.; Grady, S.; Knauer, O.A.; Ronda, J.M.; Aeschbach, D.; Czeisler, C.A.; Wright, K.P. Influence of circadian phase and extended wakefulness on glucose levels during forced desynchrony. Sleep Health 2024, 10, S96–S102. [Google Scholar] [CrossRef] [PubMed]
- La Fleur, S.E.; Kalsbeek, A.; Wortel, J.; Fekkes, M.L.; Buijs, R.M. A Daily Rhythm in Glucose Tolerance. Diabetes 2001, 50, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Rudic, R.D.; McNamara, P.; Curtis, A.-M.; Boston, R.C.; Panda, S.; Hogenesch, J.B.; FitzGerald, G.A. BMAL1 and CLOCK, Two Essential Components of the Circadian Clock, Are Involved in Glucose Homeostasis. PLoS Biol. 2004, 2, e377. [Google Scholar] [CrossRef] [PubMed]
- Opperhuizen, A.L.; Wang, D.; Foppen, E.; Jansen, R.; Boudzovitch-Surovtseva, O.; De Vries, J.; Fliers, E.; Kalsbeek, A. Feeding during the resting phase causes profound changes in physiology and desynchronization between liver and muscle rhythms of rats. Eur. J. Neurosci. 2016, 44, 2795–2806. [Google Scholar] [CrossRef]
- Smith, J.G.; Koronowski, K.B.; Mortimer, T.; Sato, T.; Greco, C.M.; Petrus, P.; Verlande, A.; Chen, S.; Samad, M.; Deyneka, E.; et al. Liver and muscle circadian clocks cooperate to support glucose tolerance in mice. Cell Rep. 2023, 42, 112588. [Google Scholar] [CrossRef]
- He, M.; Li, B.; Li, M.; Gao, S. Does early time-restricted eating reduce body weight and preserve fat-free mass in adults? A systematic review and meta-analysis of randomized controlled trials. Diabetes Metab. Syndr. Clin. Res. Rev. 2024, 18, 102952. [Google Scholar] [CrossRef]
- Jones, R.; Pabla, P.; Mallinson, J.; Nixon, A.; Taylor, T.; Bennett, A.; Tsintzas, K. Two weeks of early time-restricted feeding (eTRF) improves skeletal muscle insulin and anabolic sensitivity in healthy men. Am. J. Clin. Nutr. 2020, 112, 1015–1028. [Google Scholar] [CrossRef]
- Jamshed, H.; Beyl, R.; Della Manna, D.; Yang, E.; Ravussin, E.; Peterson, C. Early Time-Restricted Feeding Improves 24-Hour Glucose Levels and Affects Markers of the Circadian Clock, Aging, and Autophagy in Humans. Nutrients 2019, 11, 1234. [Google Scholar] [CrossRef]
- Hutchison, A.T.; Regmi, P.; Manoogian, E.N.C.; Fleischer, J.G.; Wittert, G.A.; Panda, S.; Heilbronn, L.K. Time-Restricted Feeding Improves Glucose Tolerance in Men at Risk for Type 2 Diabetes: A Randomized Crossover Trial. Obesity 2019, 27, 724–732. [Google Scholar] [CrossRef]
- Kesztyüs, D.; Fuchs, M.; Cermak, P.; Kesztyüs, T. Associations of time-restricted eating with health-related quality of life and sleep in adults: A secondary analysis of two pre-post pilot studies. BMC Nutr. 2020, 6, 76. [Google Scholar] [CrossRef]
- Wilkinson, M.J.; Manoogian, E.N.C.; Zadourian, A.; Lo, H.; Fakhouri, S.; Shoghi, A.; Wang, X.; Fleischer, J.G.; Navlakha, S.; Panda, S.; et al. Ten-Hour Time-Restricted Eating Reduces Weight, Blood Pressure, and Atherogenic Lipids in Patients with Metabolic Syndrome. Cell Metab. 2020, 31, 92–104.e5. [Google Scholar] [CrossRef] [PubMed]
- Lowe, D.A.; Wu, N.; Rohdin-Bibby, L.; Moore, A.H.; Kelly, N.; Liu, Y.E.; Philip, E.; Vittinghoff, E.; Heymsfield, S.B.; Olgin, J.E.; et al. Effects of Time-Restricted Eating on Weight Loss and Other Metabolic Parameters in Women and Men with Overweight and Obesity: The TREAT Randomized Clinical Trial. JAMA Intern. Med. 2020, 180, 1491. [Google Scholar] [CrossRef]
- Bohlman, C.; McLaren, C.; Ezzati, A.; Vial, P.; Ibrahim, D.; Anton, S.D. The effects of time-restricted eating on sleep in adults: A systematic review of randomized controlled trials. Front. Nutr. 2024, 11, 1419811. [Google Scholar] [CrossRef] [PubMed]
- Knutson, K.L. Sleep duration and cardiometabolic risk: A review of the epidemiologic evidence. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Yan, P.; Wu, X.; Zhang, W.; Cui, H.; Zhang, L.; Xu, Z.; Peng, S.; Tang, M.; Wang, Y.; et al. Associations of sleep with cardiometabolic risk factors and cardiovascular diseases: An umbrella review of observational and mendelian randomization studies. Sleep Med. Rev. 2024, 77, 101965. [Google Scholar] [CrossRef]
- Xu, Y.-X.; Zhang, J.-H.; Ding, W.-Q. Association of light at night with cardiometabolic disease: A systematic review and meta-analysis. Environ. Pollut. 2024, 342, 123130. [Google Scholar] [CrossRef]
- Chellappa, S.L.; Gao, L.; Qian, J.; Vujovic, N.; Li, P.; Hu, K.; Scheer, F.A.J.L. Daytime eating during simulated night work mitigates changes in cardiovascular risk factors: Secondary analyses of a randomized controlled trial. Nat. Commun. 2025, 16, 3186. [Google Scholar] [CrossRef]
- Manoogian, E.N.C.; Laferrère, B. Time-restricted eating: What we know and where the field is going. Obesity 2023, 31 (Suppl. S1), 7–8. [Google Scholar] [CrossRef]
- Knopp, J.L.; Holder-Pearson, L.; Chase, J.G. Insulin Units and Conversion Factors: A Story of Truth, Boots, and Faster Half-Truths. J. Diabetes Sci. Technol. 2019, 13, 597–600. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | Design | Study Duration | ITT/Per Protocol Analysis | Population Description | Shift Work Setting | n | Age (Mean ± SD) | BMI (Mean ± SD) | Sex (Male: Female) | Fasting: Feeding Hours | Fasting Blood Glucose (mmol/L, Mean ± SD) | Fasting Blood Insulin (pmol/L, Mean ± SD) | HOMA-IR (Mean ± SD) | 2 h Postprandial Glucose (mmol/L, Mean ± SD) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Centofanti et al., 2025 [51] | New Zealand | Parallel-group RCT 3-arm | 6 days | Not stated | Healthy non-shift working adults | Simulated | 55 | 24.5 ± 4.9 2 | 24.0 ± 2.5 2 | 32:23 | 11.5:12.5 6 | Fasting at night: 5.04 ± 1.098 | Fasting at night: 172.2 ± 118 | Fasting at night: 4.27 ± 4.12 | UN |
| Eating at night: 5.34 ± 1.083 | Eating at night: 113.1 ± 104.4 | Eating at night: 3.9 ± 3.34 | |||||||||||||
| Chellappa et al., 2021 [52] | USA | Parallel-group RCT 2-arm | 14 days | Per Protocol | Healthy young adults | Simulated | 20 | 26.5 ± 4.1 | 22.7 ± 2.1 | 13:7 | 9.4:14.6 4,6 | UN | UN | UN | Fasting at night: 4.99 ± 0.918 5 |
| Eating at night: 6.817 ± 1.053038 5 | |||||||||||||||
| Leung et al., 2021 [53] | Australia | Crossover pilot RCT 2-arm | 11 weeks | Per Protocol | Shift workers with abdominal obesity | Free living | 28 | 41 ± 10 | 30.7 ± 5.7 | 6:13 3 | 5:19 6 | Fasting at night: 5.8 ± 0.6 | Fasting at night: 99.6 ± 58.8 5 | Fasting at night: 4.4 ± 3.3 | Fasting at night: 5.6 ± 1.2 |
| Eating at night: 5.8 + 0.5 | Eating at night: 90 ± 43.2 5 | Eating at night: 3.9 ± 1.9 | Eating at night: 5.4 ± 1.4 | ||||||||||||
| Manoogian et al., 2022 [54] | USA | Parallel-group RCT 2-arm | 14 weeks | ITT | Firefighters with and without CVD risk factors | Free living | 150 | 40.36 ± 9.0 | Not stated | 125:25 | 14:10 | Fasting at night: 5.14 ± 0.377451 5 | Fasting at night: 29.04 ± 14.343136 5 | Fasting at night: 1.12 ± 0.566176 5 | UN |
| Eating at night: 5.15 ± 0.389473 5 | Eating at night: 29.1 ± 17.956769 5 | Eating at night: 1.13 ± 0.737949 5 | |||||||||||||
| Suyoto et al., 2024 [55] | The Netherlands | Crossover RCT 2-arm | 23 days | Per Protocol | Healthy nurses | Free living | 53 | 32.5 1,2 | 25.5 1,2 | 0:53 | 10:14 6 | UN | UN | UN | Fasting at night: 5.24684 ± 0.726323 5 |
| Eating at night: 5.621567 ± 0.987286 5 | |||||||||||||||
| Teixeira et al., 2023 [56] | Brazil | Crossover RCT 3-arm | 28 days | Not stated | Healthy police officers | Free living | 10 | 38.8 ± 4.0 | 25.9 ± 1.9 | 10:0 | 7.5:16.5 6 | Fasting at night: 4.84 ± 0.420583 5 | Fasting at night: 50.4 ± 15.811388 5 | Fasting at night: 1.8 ± 0.632456 5 | UN |
| Eating at night: 4.86 ± 0.404772 5 | Eating at night: 119.4 ± 41.10961 5 | Eating at night: 4.3 ± 1.897367 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koh, J.Y.J.; Tan, C.Y.H.; Li, M.; Liu, M.H.; Chew, H.S.J. The Effectiveness of Time-Restricted Eating as an Intermittent Fasting Approach on Shift Workers’ Glucose Metabolism: A Systematic Review and Meta-Analysis. Nutrients 2025, 17, 1689. https://doi.org/10.3390/nu17101689
Koh JYJ, Tan CYH, Li M, Liu MH, Chew HSJ. The Effectiveness of Time-Restricted Eating as an Intermittent Fasting Approach on Shift Workers’ Glucose Metabolism: A Systematic Review and Meta-Analysis. Nutrients. 2025; 17(10):1689. https://doi.org/10.3390/nu17101689
Chicago/Turabian StyleKoh, Jia Ying Jennell, Celine Yu Han Tan, Meng Li, Mei Hui Liu, and Han Shi Jocelyn Chew. 2025. "The Effectiveness of Time-Restricted Eating as an Intermittent Fasting Approach on Shift Workers’ Glucose Metabolism: A Systematic Review and Meta-Analysis" Nutrients 17, no. 10: 1689. https://doi.org/10.3390/nu17101689
APA StyleKoh, J. Y. J., Tan, C. Y. H., Li, M., Liu, M. H., & Chew, H. S. J. (2025). The Effectiveness of Time-Restricted Eating as an Intermittent Fasting Approach on Shift Workers’ Glucose Metabolism: A Systematic Review and Meta-Analysis. Nutrients, 17(10), 1689. https://doi.org/10.3390/nu17101689