
The Association Between the American Heart Association Life’s Essential 8 and Metabolic Syndrome Among Postmenopausal Women: Findings from NHANES 2011–2020

 , , ,
, , ,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
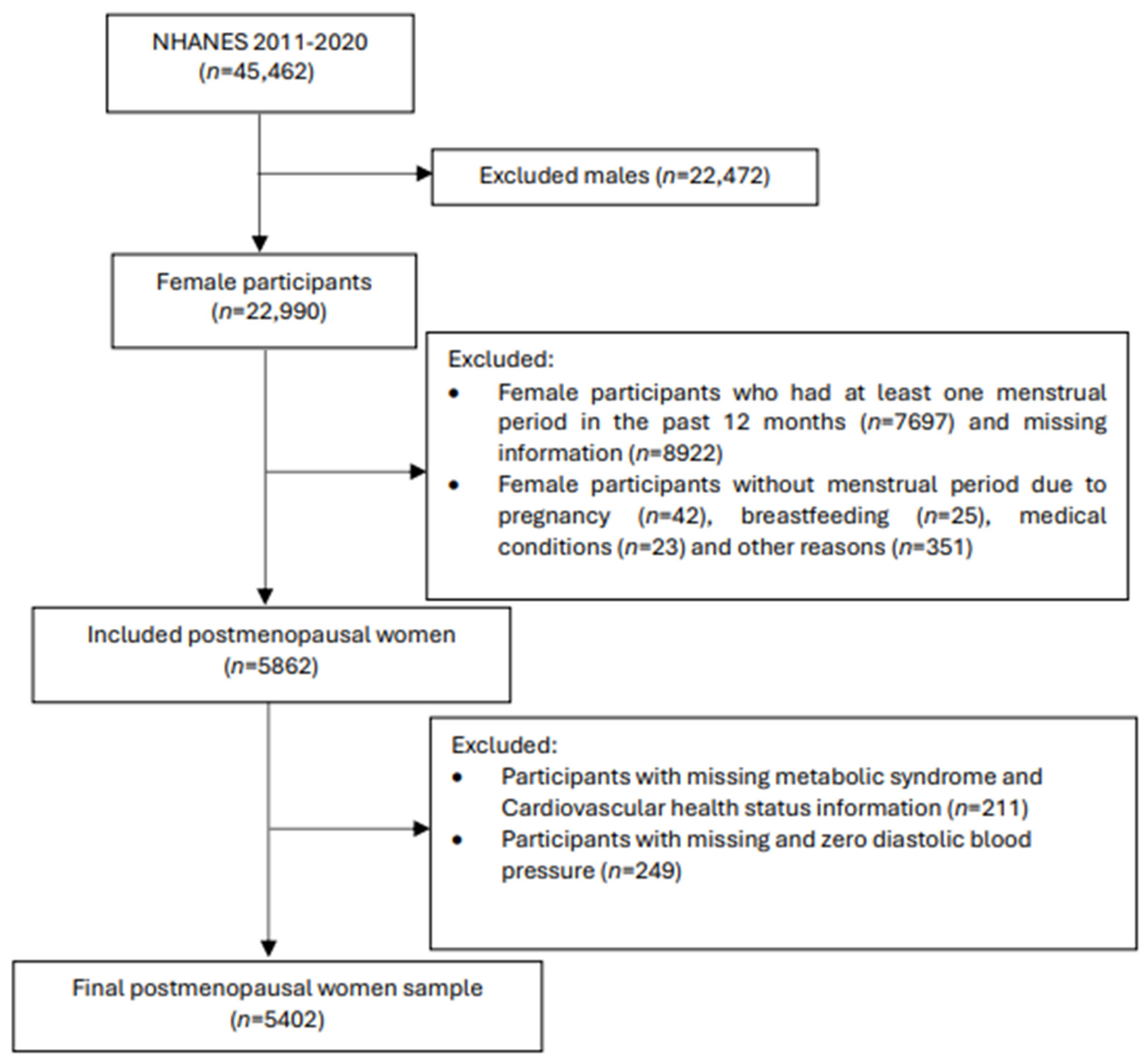
2.2. Study Design and Population
2.3. Measurement of Life’s Essential 8 Score
2.4. Measurements and Criteria of MetS
2.5. Other Measurements
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Relationships Between Life’s Essential 8 and Metabolic Syndrome in Postmenopausal Women
3.3. Decomposition of Life’s Essential 8 and Metabolic Syndrome in Postmenopausal Women
3.4. Effect Modification by Race and Female Hormone Usage
3.4.1. Effect Modification by Race
3.4.2. Effect Modification by Female Hormone Usage
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| CI | Confidence intervals |
| CVD | Cardiovascular disease |
| HbA1c | Haemoglobin A1c |
| HEI | Healthy Eating Index |
| LE8 | Life’s Essential 8 |
| MetS | Metabolic syndrome |
| non-HDL | Non-high-density lipoprotein cholesterol |
| OR | Odds ratio |
| SD | Standard deviation |
| NHANES | The National Health and Nutrition Examination Survey |
| T2DM | Type 2 diabetes mellitus |
References
- Grundy, S.M.; Brewer, H.B.; Cleeman, J.I.; Smith, S.C.; Lenfant, C. Definition of Metabolic Syndrome. Circulation 2004, 109, 433–438. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.S.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Barone Gibbs, B.; Beaton, A.Z.; Boehme, A.K.; et al. 2024 Heart Disease and Stroke Statistics: A Report of US and Global Data From the American Heart Association. Circulation 2024, 149, e347–e913. [Google Scholar] [CrossRef] [PubMed]
- El Khoudary, S.R.; Aggarwal, B.; Beckie, T.M.; Hodis, H.N.; Johnson, A.E.; Langer, R.D.; Limacher, M.C.; Manson, J.E.; Stefanick, M.L.; Allison, M.A.; et al. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement from the American Heart Association. Circulation 2020, 142, e506–e532. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Heart Disease Facts & Statistics. Available online: https://www.cdc.gov/heart-disease/data-research/facts-stats/index.html#cdcreference_1 (accessed on 8 January 2025).
- Roberts, H.; Hickey, M. Managing the menopause: An update. Maturitas 2016, 86, 53–58. [Google Scholar] [CrossRef]
- Lovejoy, J.C.; Champagne, C.M.; de Jonge, L.; Xie, H.; Smith, S.R. Increased visceral fat and decreased energy expenditure during the menopausal transition. Int. J. Obes. 2008, 32, 949–958. [Google Scholar] [CrossRef]
- Eslam, M.; Sanyal, A.J.; George, J.; International Consensus, P. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014.e1991. [Google Scholar] [CrossRef]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Meegaswatte, H.; Speer, K.; McKune, A.J.; Naumovski, N. Functional Foods and Nutraceuticals for the Management of Cardiovascular Disease Risk in Postmenopausal Women. Rev. Cardiovasc. Med. 2024, 25, 460. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Allen, N.B.; Anderson, C.A.M.; Black, T.; Brewer, L.C.; Foraker, R.E.; Grandner, M.A.; Lavretsky, H.; Perak, A.M.; Sharma, G.; et al. Life’s Essential 8: Updating and Enhancing the American Heart Association’s Construct of Cardiovascular Health: A Presidential Advisory From the American Heart Association. Circulation 2022, 146, e18–e43. [Google Scholar] [CrossRef]
- Liu, Y.; Tang, J.; Gao, S. The inverse relationship between Life’s Essential 8 and risk of metabolic syndrome: Evidence from NHANES 2005–2018. Front. Endocrinol. 2024, 15, 1449930. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Qiu, X.; He, C.; Deng, R.; Huo, C.; Fang, B. From Life’s Essential 8 to metabolic syndrome: Insights from NHANES database and network pharmacology analysis of quercetin. Front. Nutr. 2024, 11, 1452374. [Google Scholar] [CrossRef] [PubMed]
- Gou, R.; Xiong, S.; Liang, X.; Wu, H.; Qin, S.; Li, B.; Luo, C.; Chen, J. Relationship between Life’s Essential 8 and metabolic syndrome among older Americans (NHANES, 2007–2010): Navigating biological aging and inflammation. Front. Med. 2024, 11, 1380464. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.C.; Liang, J.L.; Hu, X.Y.; Fang, H.C.; Liu, D.L.; Zhao, H.X.; Li, H.L.; Xu, W.H. Adherence to higher Life’s Essential 8 scores is linearly associated with reduced all-cause and cardiovascular mortality among US adults with metabolic syndrome: Results from NHANES 2005–2018. PLoS ONE 2024, 19, e0314152. [Google Scholar] [CrossRef]
- Yang, T.; Yi, J.; Shao, M.; Linlin, Z.; Wang, J.; Huang, F.; Guo, F.; Qin, G.; Zhao, Y. Associations between life’s essential 8 and metabolic health among us adults: Insights of NHANES from 2005 to 2018. Acta Diabetol. 2024, 61, 963–974. [Google Scholar] [CrossRef]
- Vogel, B.; Acevedo, M.; Appelman, Y.; Bairey Merz, C.N.; Chieffo, A.; Figtree, G.A.; Guerrero, M.; Kunadian, V.; Lam, C.S.P.; Maas, A.; et al. The Lancet women and cardiovascular disease Commission: Reducing the global burden by 2030. Lancet 2021, 397, 2385–2438. [Google Scholar] [CrossRef]
- Akinbami, L.J.; Chen, T.-C.; Davy, O.; Ogden, C.L.; Fink, S.; Clark, J.; Riddles, M.K.; Mohadjer, L.K. National Health and Nutrition Examination Survey, 2017–March 2020 Prepandemic File: Sample Design, Estimation, and Analytic Guidelines. Vital. Health Stat. Ser. 2022, 2, 1–36. [Google Scholar]
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey (NHANES): Continuous NHANES. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/default.aspx (accessed on 8 January 2025).
- Lloyd-Jones, D.M.; Ning, H.; Labarthe, D.; Brewer, L.; Sharma, G.; Rosamond, W.; Foraker, R.E.; Black, T.; Grandner, M.A.; Allen, N.B.; et al. Status of Cardiovascular Health in US Adults and Children Using the American Heart Association’s New “Life’s Essential 8” Metrics: Prevalence Estimates From the National Health and Nutrition Examination Survey (NHANES), 2013 Through 2018. Circulation 2022, 146, 822–835. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef]
- National Cancer Institute. Healthy Eating Index SAS Code. Available online: https://epi.grants.cancer.gov/hei/sas-code.html (accessed on 20 January 2025).
- Stefanska, A.; Bergmann, K.; Sypniewska, G. Metabolic Syndrome and Menopause: Pathophysiology, Clinical and Diagnostic Significance. Adv. Clin. Chem. 2015, 72, 1–75. [Google Scholar] [CrossRef]
- Makarem, N.; St-Onge, M.P.; Liao, M.; Lloyd-Jones, D.M.; Aggarwal, B. Association of sleep characteristics with cardiovascular health among women and differences by race/ethnicity and menopausal status: Findings from the American Heart Association Go Red for Women Strategically Focused Research Network. Sleep Health 2019, 5, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Kline, C.E.; Hall, M.H.; Buysse, D.J.; Earnest, C.P.; Church, T.S. Poor Sleep Quality is Associated with Insulin Resistance in Postmenopausal Women With and Without Metabolic Syndrome. Metab. Syndr. Relat. Disord. 2018, 16, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Peila, R.; Xue, X.; Feliciano, E.M.C.; Allison, M.; Sturgeon, S.; Zaslavsky, O.; Stone, K.L.; Ochs-Balcom, H.M.; Mossavar-Rahmani, Y.; Crane, T.E.; et al. Association of sleep duration and insomnia with metabolic syndrome and its components in the Women’s Health Initiative. BMC Endocr. Disord. 2022, 22, 228. [Google Scholar] [CrossRef] [PubMed]
- Cengiz, H.; Kaya, C.; Suzen Caypinar, S.; Alay, I. The relationship between menopausal symptoms and metabolic syndrome in postmenopausal women. J. Obstet. Gynaecol. 2019, 39, 529–533. [Google Scholar] [CrossRef]
- Smiley, A.; King, D.; Bidulescu, A. The Association between Sleep Duration and Metabolic Syndrome: The NHANES 2013/2014. Nutrients 2019, 11, 2582. [Google Scholar] [CrossRef]
- Moradi, L.; Hashemi, S.J.; Zaman, F.; Alipour, M.; Farhangiyan, Z.; Sharifzadeh, M. Comparison of metabolic risk factors, lipid indices, healthy eating index, and physical activity among premenopausal, menopausal, and postmenopausal women. Rom. J. Intern. Med. 2024, 62, 260–271. [Google Scholar] [CrossRef]
- Kim, Y.J.; Hwang, J.-Y.; Kim, H.; Park, S.; Kwon, O. Diet quality, physical activity, and their association with metabolic syndrome in Korean adults. Nutrition 2019, 59, 138–144. [Google Scholar] [CrossRef]
- Jowshan, M.R.; Rafraf, M.; Hashemi, A.H.; Hajjarzadeh, S.; Asghari-Jafarabadi, M.; Asghari, S. Association between healthy eating index-2015 scores and metabolic syndrome among Iranian women: A cross-sectional study. BMC Womens Health 2024, 24, 30. [Google Scholar] [CrossRef]
- Lizcano, F.; Guzman, G. Estrogen Deficiency and the Origin of Obesity during Menopause. Biomed. Res. Int. 2014, 2014, 757461. [Google Scholar] [CrossRef]
- Harvey, A.; Montezano, A.C.; Touyz, R.M. Vascular biology of ageing-Implications in hypertension. J. Mol. Cell Cardiol. 2015, 83, 112–121. [Google Scholar] [CrossRef]
- Green, D.J.; Hopkins, N.D.; Jones, H.; Thijssen, D.H.; Eijsvogels, T.M.; Yeap, B.B. Sex differences in vascular endothelial function and health in humans: Impacts of exercise. Exp. Physiol. 2016, 101, 230–242. [Google Scholar] [CrossRef] [PubMed]
- Connelly, P.J.; Casey, H.; Montezano, A.C.; Touyz, R.M.; Delles, C. Sex steroids receptors, hypertension, and vascular ageing. J. Hum. Hypertens. 2022, 36, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Djibo, D.A.; Araneta, M.R.; Kritz-Silverstein, D.; Barrett-Connor, E.; Wooten, W. Body adiposity index as a risk factor for the metabolic syndrome in postmenopausal Caucasian, African American, and Filipina women. Diabetes Metab. Syndr. 2015, 9, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Gaston, S.A.; Park, Y.M.; McWhorter, K.L.; Sandler, D.P.; Jackson, C.L. Multiple poor sleep characteristics and metabolic abnormalities consistent with metabolic syndrome among white, black, and Hispanic/Latina women: Modification by menopausal status. Diabetol. Metab. Syndr. 2019, 11, 17. [Google Scholar] [CrossRef]
- Matthews, K.A.; Hall, M.H.; Lee, L.; Kravitz, H.M.; Chang, Y.; Appelhans, B.M.; Swanson, L.M.; Neal-Perry, G.S.; Joffe, H. Racial/ethnic disparities in women’s sleep duration, continuity, and quality, and their statistical mediators: Study of Women’s Health Across the Nation. Sleep 2019, 42, zsz042. [Google Scholar] [CrossRef]
- Jehan, S.; Masters-Isarilov, A.; Salifu, I.; Zizi, F.; Jean-Louis, G.; Pandi-Perumal, S.R.; Gupta, R.; Brzezinski, A.; McFarlane, S.I. Sleep Disorders in Postmenopausal Women. J. Sleep Disord. Ther. 2015, 4, 212. [Google Scholar]
- Koren, D.; Dumin, M.; Gozal, D. Role of sleep quality in the metabolic syndrome. Diabetes Metab. Syndr. Obes. 2016, 9, 281–310. [Google Scholar] [CrossRef]
- Lachat, C.; Hawwash, D.; Ocké, M.C.; Berg, C.; Forsum, E.; Hörnell, A.; Larsson, C.; Sonestedt, E.; Wirfält, E.; Åkesson, A.; et al. Strengthening the Reporting of Observational studies in Epidemiology—Nutritional Epidemiology (STROBE-nut): An extension of the STROBE statement. PLoS Med. 2016, 13, e1002036. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | Total (n = 5402) | Metabolic Syndrome (n = 3152) | No Metabolic Syndrome (n = 2250) | p Value |
|---|---|---|---|---|
| Age (year) | 63 ± 10 | 65 ± 10 | 61 ± 10 | <0.001 |
| Race/Hispanic origin, n (%) | ||||
| Mexican American | 574 (4.4) | 367 (5.0) | 207 (3.7) | 0.001 |
| Other Hispanic | 653 (5.2) | 398 (5.7) | 255 (4.7) | 0.033 |
| Non-Hispanic White | 2245 (73.5) | 1262 (71.1) | 983 (76.3) | <0.001 |
| Non-Hispanic Black | 1301 (10.2) | 796 (11.3) | 505 (8.9) | <0.001 |
| Other Race—Including Multi-Racial | 629 (6.7) | 329 (7.0) | 300 (6.3) | 0.414 |
| Marital status, n (%) | ||||
| Married/Living with Partner | 2653 (57.8) | 1481 (55.2) | 1172 (60.8) | 0.007 |
| Widowed/Divorced/Separated | 2297 (36.7) | 1417 (39.2) | 880 (33.7) | 0.004 |
| Never married | 446 (5.6) | 250 (5.6) | 196 (5.5) | 0.93 |
| Ratio of family income to poverty | 3.08 ± 1.61 | 2.85 ± 1.59 | 3.35 ± 1.60 | <0.001 |
| Education levels, n (%) | ||||
| Less than 9th grade | 574 (5.0) | 409 (6.5) | 165 (3.2) | <0.001 |
| 9–11th grade | 661 (8.6) | 433 (10.2) | 228 (6.6) | <0.001 |
| High school graduate | 1319 (25.9) | 807 (29.1) | 512 (22.3) | <0.001 |
| Some college | 1728 (33.7) | 989 (33.9) | 739 (33.4) | 0.789 |
| College graduate or above | 1117 (26.8) | 512 (20.3) | 605 (34.4) | <0.001 |
| Body mass index (Kgm−2) | 29.79 ± 7.17 | 31.77 ± 7.19 | 27.50 ± 6.42 | <0.001 |
| Waist circumference (cm) | 100.27 ± 15.49 | 105.42 ± 14.70 | 94.47 ± 14.25 | <0.001 |
| Average alcohol consumed (drinks per day) | 0.258 ± 0.63 | 0.179 ± 0.48 | 0.350 ± 0.76 | <0.001 |
| Life’s Essential 8 score b | 63.74 ± 15.19 | 58.08 ± 13.76 | 70.34 ± 14.07 | <0.001 |
| Health behaviour score b | 67.95 ± 21.13 | 65.02 ± 21.48 | 71.37 ± 20.18 | <0.001 |
| Healthy Eating Index-2015 diet score | 49.30 ± 31.21 | 47.41 ± 30.92 | 51.48 ± 31.39 | 0.002 |
| Physical activity score | 62.63 ± 45.19 | 56.30 ± 46.71 | 70.01 ± 42.19 | <0.001 |
| Nicotine exposure score | 78.60 ± 39.23 | 77.51 ± 40.01 | 79.83 ± 38.31 | 0.184 |
| Sleep health score | 83.58 ± 24.60 | 82.13 ± 25.44 | 85.26 ± 23.47 | 0.004 |
| Health factor score b | 59.70 ± 18.81 | 51.38 ± 16.10 | 69.38 ± 17.03 | <0.001 |
| Body mass index score | 56.49 ± 34.42 | 46.65 ± 32.92 | 67.87 ± 32.55 | <0.001 |
| Blood lipids score | 58.83 ± 29.36 | 55.97 ± 29.16 | 62.22 ± 29.24 | <0.001 |
| Blood glucose score | 70.01 ± 26.69 | 58.65 ± 25.29 | 83.38 ± 21.62 | <0.001 |
| Blood pressure score | 54.19 ± 34.52 | 45.03 ± 31.91 | 64.88 ± 34.39 | <0.001 |
| Cardiovascular Health, n (%) c | ||||
| Low | 836 (17.9) | 674 (26.0) | 162 (8.5) | <0.001 |
| Moderate | 3780 (65.7) | 2313 (68.4) | 1467 (62.5) | 0.007 |
| High | 786 (16.4) | 165 (5.6) | 621 (29.0) | <0.001 |
| Crude Model a | Full Model b | |||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | |
| Life’s Essential 8 score (per 10 units) | 0.53 (0.50–0.57) | <0.001 | 0.53 (0.48–0.57) | <0.001 |
| Cardiovascular health status | <0.001 | |||
| Low (0–49) | 1 (Reference) | 1 (Reference) | ||
| Moderate (50–79) | 0.36 (0.28–0.45) | <0.001 | 0.37 (0.28–0.50) | <0.001 |
| High (80–100) | 0.06 (0.05–0.08) | <0.001 | 0.07 (0.05–0.10) | <0.001 |
| Health behaviour score (per 10 units) | 0.86 (0.83–0.90) | <0.001 | 0.87 (0.84–0.92) | <0.001 |
| Health behaviour status | <0.001 | |||
| Low (0–49) | 1 (Reference) | 1 (Reference) | ||
| Moderate (50–79) | 0.66 (0.54–0.81) | <0.001 | 0.66 (0.51–0.85) | <0.001 |
| High (80–100) | 0.46 (0.37–0.57) | <0.001 | 0.50 (0.38–0.67) | <0.001 |
| Health factor score (per 10 units) | 0.52 (0.50–0.55) | <0.001 | 0.54 (0.51–0.60) | <0.001 |
| Health factor status | <0.001 | |||
| Low (0–49) | 1 (Reference) | 1 (Reference) | ||
| Moderate (50–79) | 0.23 (0.19–0.27) | <0.001 | 0.24 (0.19–0.29) | <0.001 |
| High (80–100) | 0.04 (0.03–0.06) | <0.001 | 0.05 (0.03–0.07) | <0.001 |
| Model 1 | Model 2 | |||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Health behaviour scores: | ||||
| Healthy eating index-2015 diet score (percentile) | 0.076 | 0.852 | ||
| 0 (1st–24th) | 1 (Reference) | 1 (Reference) | ||
| 25 (25th–49th) | 0.97 (0.73–1.29) | 0.89 (0.59–1.36) | ||
| 50 (50th–74th) | 0.86 (0.69–1.07) | 0.83 (0.55–1.24) | ||
| 80 (75th–94th) | 0.84 (0.65–1.08) | 0.98 (0.63–1.51) | ||
| 100 (≥95th) | 0.61 (0.42–0.86) | 0.85 (0.49–1.48) | ||
| Physical activity score (min of moderate-to-vigorous physical activity per week) | <0.001 | 0.096 | ||
| 0 (0 min) | 1 (Reference) | 0 (Reference) | ||
| 20 (1–29 min) | 0.58 (0.30–1.12) | 0.44 (0.10–1.86) | ||
| 40 (30–59 min) | 0.66 (0.38–1.15) | 0.83 (0.29–2.32) | ||
| 60 (60–89 min) | 0.54 (0.35–0.81) | 0.44 (0.23–0.87) | ||
| 80 (90–119 min) | 1.19 (0.64–2.21) | 1.53 (0.58–4.04) | ||
| 90 (120–149 min) | 0.58 (0.37–0.89) | 1.07 (0.57–2.01) | ||
| 100 (≥150 min) | 0.65 (0.52–0.80) | 1.12 (0.77–1.63) | ||
| Nicotine exposure score | 0.071 | 0.022 | ||
| 0 (Current smoker) | 1 (Reference) | 1 (Reference) | ||
| 25 (quit < 1 yr) | 0.66 (0.18–2.42) | 0.69 (0.10–4.69) | ||
| 50 (quit 1–<5 yrs) | 0.45 (0.16–1.23) | 0.22 (0.03–1.53) | ||
| 75 (quit ≥5 yrs) | 0.76 (0.45–1.29) | 0.59 (0.31–1.11) | ||
| 100 (Never Smoker) | 0.65 (0.48–0.87) | 0.52 (0.34–0.80) | ||
| Sleep health score | 0.009 | 0.34 | ||
| 0 (<4 h) | 1 (Reference) | 1 (Reference) | ||
| 20 (4–<5 h) | 0.96 (0.39–2.38) | 1.08 (0.32–3.60) | ||
| 40 (5–<6 or ≥10 h) | 1.31 (0.58–2.98) | 0.89 (0.27–2.99) | ||
| 70 (6–<7 h) | 0.75 (0.33–1.73) | 0.60 (0.17–2.18) | ||
| 90 (9–<10 h) | 0.95 (0.41–2.24) | 0.58 (0.17–1.95) | ||
| 100 (7–<9 h) | 0.78 (0.36–1.66) | 0.78 (0.22–2.77) | ||
| Health factor scores: | ||||
| Body mass index score (kg/m2) | <0.001 | <0.001 | ||
| 0 (>40) | 1 (Reference) | 1 (Reference) | ||
| 15 (35.0–39.9) | 0.76 (0.52–1.11) | 1.09 (0.60–1.97) | ||
| 30 (30.0–34.9) | 0.57 (0.39–0.81) | 0.89 (0.49–1.61) | ||
| 70 (25.0–29.9) | 0.33 (0.23–0.46) | 0.71 (0.42–1.19) | ||
| 100 (<25) | 0.13 (0.09–0.18) | 0.19 (0.11–0.31) | ||
| Blood lipids score (non–HDL cholesterol level) | <0.001 | <0.001 | ||
| 0 (>220 or 190–219 mg/dL and using medication) | 1 (Reference) | 1 (Reference) | ||
| 20 (190–219 or 160–189 mg/dL and using medication) | 0.57 (0.36–0.91) | 0.30 (0.16–0.56) | ||
| 40 (160–189 or 130–159 mg/dL and using medication) | 0.43 (0.30–0.62) | 0.35 (0.19–0.62) | ||
| 60 (130–159 mg/dL) | 0.16 (0.11–0.24) | 0.10 (0.05–0.19) | ||
| 80 (<130 mg/dL and using medication) | 8.08 (4.36–14.98) | 12.65 (5.15–31.12) | ||
| 100 (<130 mg/dL) | 0.13 (0.09–0.21) | 0.08 (0.05–0.14) | ||
| Blood glucose score | <0.001 | <0.001 | ||
| 0 (Diabetes with HbA1C ≥10.0) | 1 (Reference) | 1 (Reference) | ||
| 10 (Diabetes with HbA1C 9.0–9.9) | 0.78 (0.16–3.88) | 0.43 (0.05–4.06) | ||
| 20 (Diabetes with HbA1C 8.0–8.9) | 1.21 (0.33–4.45) | 1.22 (0.17–8.66) | ||
| 30 (Diabetes with HbA1C 7.0–7.9) | 0.38 (0.12–1.18) | 0.34 (0.06–1.96) | ||
| 40 (Diabetes with HbA1C <7.0) | 0.31 (0.12–0.80) | 0.23 (0.05–1.17) | ||
| 60 (No diabetes with HbA1C 5.7–7.0) | 0.07 (0.03–0.18) | 0.10 (0.02–0.47) | ||
| 100 (No diabetes with HbA1C <5.7) | 0.02 (0.01–0.05) | 0.02 (0.00–0.10) | ||
| Blood pressure score | <0.001 | <0.001 | ||
| 0 (≥160 or ≥100 mmHg) | 1 (Reference) | 1 (Reference) | ||
| 5 (140–150 or 90–99 mmHg and using medication) | 1.86 (1.26–2.75) | 2.08 (1.13–3.82) | ||
| 25 (140–150 or 90–99 mmHg) | 1.00 (0.59–1.69) | 1.62 (0.76–3.46) | ||
| 30 (130–139 or 80–89 mmHg and using medication) | 1.61 (1.06–2.45) | 1.49 (0.81–2.76) | ||
| 50 (130–139 or 80–89 mmHg) | 0.54 (0.38–0.77) | 0.63 (0.36–1.11) | ||
| 55 (120–129/<90 mmHg and using medication) | 2.83 (1.70–4.73) | 2.09 (0.90–4.87) | ||
| 75 (120–129/<90 mmHg) | 0.32 (0.20–0.51) | 0.27 (0.14–0.54) | ||
| 80 (<120/<80 mmHg and using medication) | 2.81 (1.79–4.40) | 2.81 (1.52–5.21) | ||
| 100 (<120/<80 mmHg) | 0.20 (0.14–0.29) | 0.17 (0.09–0.32) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meegaswatte, H.; McKune, A.J.; Panagiotakos, D.B.; Osiriphun, S.; Leksawasdi, N.; Rachtanapun, P.; Veysey, M.; Naumovski, N.; Taesuwan, S. The Association Between the American Heart Association Life’s Essential 8 and Metabolic Syndrome Among Postmenopausal Women: Findings from NHANES 2011–2020. Nutrients 2025, 17, 1688. https://doi.org/10.3390/nu17101688
Meegaswatte H, McKune AJ, Panagiotakos DB, Osiriphun S, Leksawasdi N, Rachtanapun P, Veysey M, Naumovski N, Taesuwan S. The Association Between the American Heart Association Life’s Essential 8 and Metabolic Syndrome Among Postmenopausal Women: Findings from NHANES 2011–2020. Nutrients. 2025; 17(10):1688. https://doi.org/10.3390/nu17101688
Chicago/Turabian StyleMeegaswatte, Harshini, Andrew J. McKune, Demosthenes B. Panagiotakos, Sukhuntha Osiriphun, Noppol Leksawasdi, Pornchai Rachtanapun, Martin Veysey, Nenad Naumovski, and Siraphat Taesuwan. 2025. "The Association Between the American Heart Association Life’s Essential 8 and Metabolic Syndrome Among Postmenopausal Women: Findings from NHANES 2011–2020" Nutrients 17, no. 10: 1688. https://doi.org/10.3390/nu17101688
APA StyleMeegaswatte, H., McKune, A. J., Panagiotakos, D. B., Osiriphun, S., Leksawasdi, N., Rachtanapun, P., Veysey, M., Naumovski, N., & Taesuwan, S. (2025). The Association Between the American Heart Association Life’s Essential 8 and Metabolic Syndrome Among Postmenopausal Women: Findings from NHANES 2011–2020. Nutrients, 17(10), 1688. https://doi.org/10.3390/nu17101688