
Validation of the Greek Cardiovascular Diet Questionnaire 2 (CDQ-2) and Single-Center Cross-Sectional Insights into the Dietary Habits of Cardiovascular Patients

 , , ,
, , ,  , ,
, , 
Abstract

1. Introduction
2. Materials and Methods
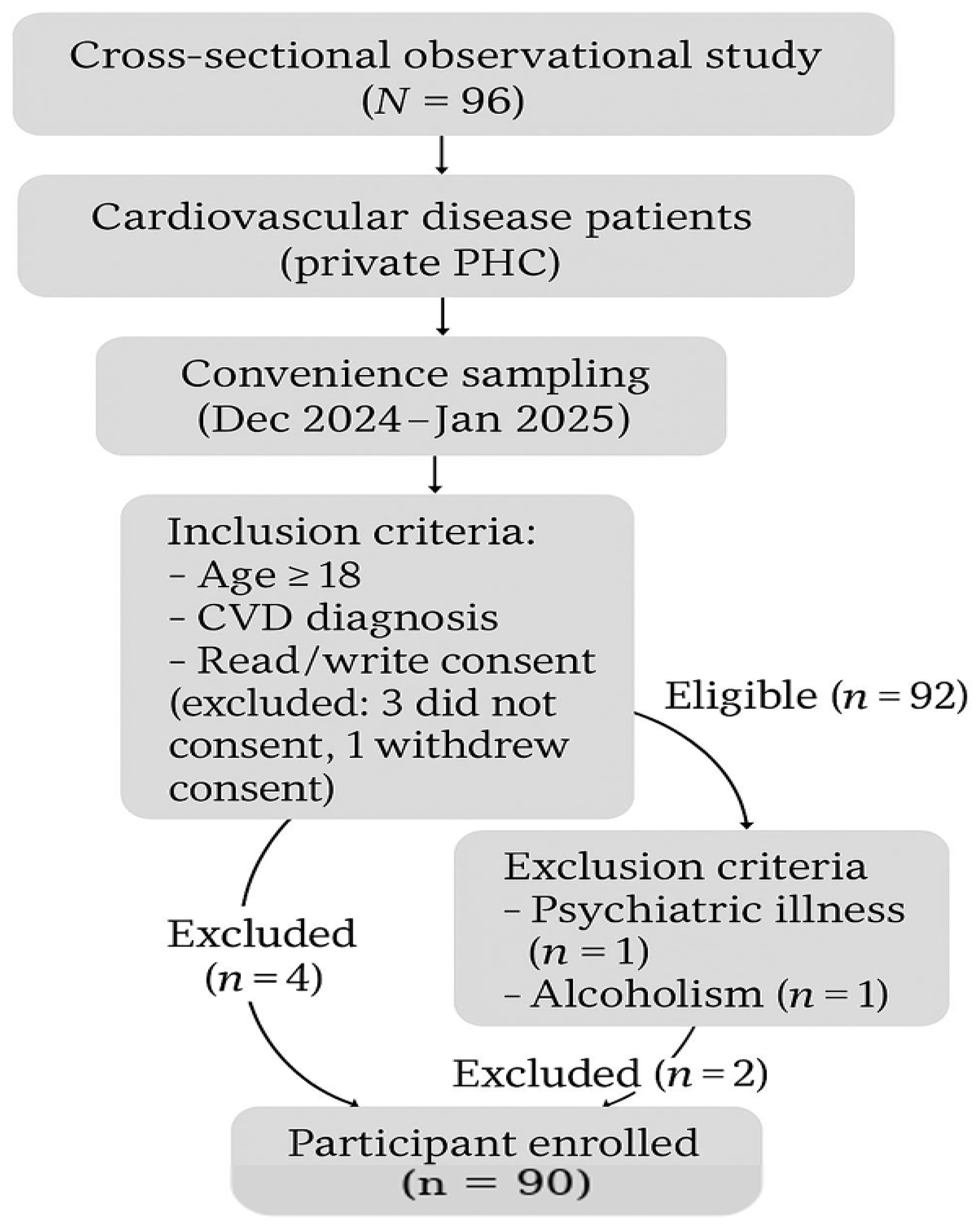
2.1. Study Design
2.2. Translation of CDQ-2
2.3. Reliability
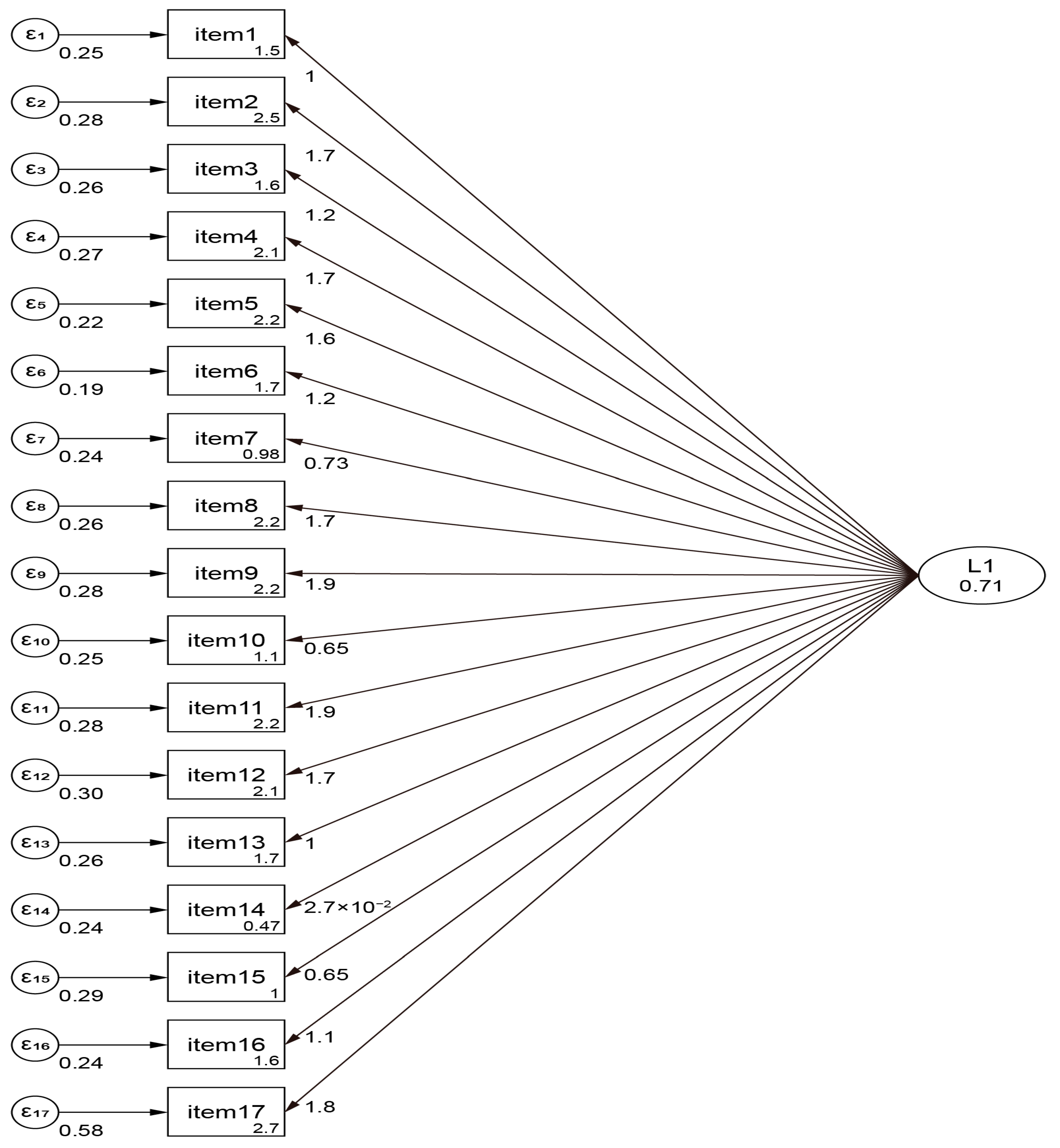
2.4. Validity
2.5. Translation and Weighting Questionnaire
- -
- The first concerned the following demographic characteristics: (a) age, (b) biological sex, (c) educational level, (d) subjective economic situation, and (e) family situation.
- -
- CDQ-2 includes 17 closed-ended questions designed to identify major sources of nutrients. For each of the 9 questions related to the saturated fatty acid (SFA) intake, the total score ranges from 0 to 27. The monounsaturated fatty acid (MUFA) intake is investigated with one question (total score range 0–6). Omega-3 fatty acid (ω3FA) intake is investigated with 3 questions (total score range 0–10). Finally, there are 4 questions on fruit and vegetable (FV) consumption (range 0–14). The total nutritional score is calculated as [(FV + MUFA + ω3FA) − SFA], fluctuating from −27 to +30. Higher scores indicate better nutrition, whereas the existing literature does not provide universal cut-off points.
2.6. Statistical Methodology
3. Results
4. Discussion
Study’s Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vanzella, L.M.; Rouse, V.; Ajwani, F.; Deilami, N.; Pokosh, M.; Oh, P.; Ghisi, G.L.M. Barriers and facilitators to participant adherence of dietary recommendations within comprehensive cardiac rehabilitation programmes: A systematic review. Public Health Nutr. 2021, 24, 4823–4839. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.; Sigala, E.G.; Damigou, E.; Loukina, A.; Dalmyras, D.; Mentzantonakis, G.; Barkas, F.; Adamidis, P.S.; Kravvariti, E.; Liberopoulos, E. The burden of cardiovascular disease and related risk factors in Greece: The ATTICA epidemiological study (2002–2022). Hellenic J. Cardiol. 2024. [CrossRef] [PubMed]
- Vervoort, D.; Tchienga, D.; Ouzounian, M.; Mvondo, C.M. Thoracic aortic surgery in low- and middle-income countries: Time to bridge the gap? JTCVS Open 2024, 19, 210–214. [Google Scholar] [CrossRef]
- Yang, G.-J.; Ouyang, H.-Q.; Zhao, Z.-Y.; Li, W.-H.; Fall, I.S.; Djirmay, A.G.; Zhou, X.-N. Discrepancies in neglected tropical diseases burden estimates in China: Comparative study of real-world data and Global Burden of Disease 2021 data (2004-–2020). BMJ 2025, 388, e080969. [Google Scholar] [CrossRef]
- Coyan, G.N.; Reeder, K.M.; Vacek, J.L. Diet and exercise interventions following coronary artery bypass graft surgery: A review and call to action. Phys. Sportsmed. 2014, 42, 119–129. [Google Scholar] [CrossRef]
- Casquel De Tomasi, L.; Salomé Campos, D.H.; Grippa Sant’Ana, P.; Okoshi, K.; Padovani, C.R.; Masahiro Murata, G.; Nguyen, S.; Kolwicz, S.C., Jr.; Cicogna, A.C. Pathological hypertrophy and cardiac dysfunction are linked to aberrant endogenous unsaturated fatty acid metabolism. PLoS ONE 2018, 13, e0193553. [Google Scholar] [CrossRef]
- Engelman, D.T.; Ben Ali, W.; Williams, J.B.; Perrault, L.P.; Reddy, V.S.; Arora, R.C.; Roselli, E.E.; Khoynezhad, A.; Gerdisch, M.; Levy, J.H.; et al. Guidelines for Perioperative Care in Cardiac Surgery: Enhanced Recovery After Surgery Society Recommendations. JAMA Surg. 2019, 154, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2019, 3, Cd009825. [Google Scholar] [CrossRef]
- Sansone, R.A.; Dittoe, N.; Hahn, H.S.; Wiederman, M.W. The prevalence of borderline personality disorder in a consecutive sample of cardiac stress test patients. Prim. Care Companion CNS Disord. 2011, 13, 27129. [Google Scholar] [CrossRef]
- Elgazzar, E.; Ahmed, E.; Ahmed, S.A.; Karousa, M.M. Effects of betaine as feed additive on behavioral patterns and growth performance of Japanese quail. Benha Vet. Med. J. 2022, 42, 214–218. [Google Scholar] [CrossRef]
- Saczynski, J.S.; Marcantonio, E.R.; Quach, L.; Fong, T.G.; Gross, A.; Inouye, S.K.; Jones, R.N. Cognitive trajectories after postoperative delirium. N. Engl. J. Med. 2012, 367, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Beirão, S.; Costa, J.G.; Ferreira-Pêgo, C. Assessing knowledge and awareness of Food and Drug Interactions among nutrition sciences students: Implications for education and clinical practice. Nutr. Health 2024. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J. Am. Coll. Cardiol. 2017, 70, 776–803. [Google Scholar] [PubMed]
- Paillard, F.; Flageul, O.; Mahé, G.; Laviolle, B.; Dourmap, C.; Auffret, V. Validation and reproducibility of a short food frequency questionnaire for cardiovascular prevention. Arch. Cardiovasc. Dis. 2021, 114, 570–576. [Google Scholar] [CrossRef]
- Gregório, M.J.; Rodrigues, A.M.; Salvador, C.; Dias, S.S.; de Sousa, R.D.; Mendes, J.M.; Coelho, P.S.; Branco, J.C.; Lopes, C.; Martínez-González, M.A. Validation of the telephone-administered version of the mediterranean diet adherence screener (Medas) questionnaire. Nutrients 2020, 12, 1511. [Google Scholar] [CrossRef]
- Michalis, A.; Costarelli, V. The Greek version of the Mediterranean diet adherence screener: Development and validation. Nutr. Food Sci. 2021, 52, 129–139. [Google Scholar] [CrossRef]
- Vieira, L.M.; Gottschall, C.B.A.; Vinholes, D.B.; Martinez-Gonzalez, M.A.; Marcadenti, A. Translation and cross-cultural adaptation of 14-item Mediterranean Diet Adherence Screener and low-fat diet adherence questionnaire. Clin. Nutr. ESPEN 2020, 39, 180–189. [Google Scholar] [CrossRef]
- Cangemi, R.; Miglionico, M.; D’Amico, T.; Fasano, S.; Proietti, M.; Romiti, G.F.; Corica, B.; Stefanini, L.; Tanzilli, G.; Basili, S.; et al. Adherence to the Mediterranean Diet in Preventing Major Cardiovascular Events in Patients with Ischemic Heart Disease: The EVA Study. Nutrients 2023, 15, 3150. [Google Scholar] [CrossRef]
- Mertens, E.; Markey, O.; Geleijnse, J.M.; Lovegrove, J.A.; Givens, D.I. Adherence to a healthy diet in relation to cardiovascular incidence and risk markers: Evidence from the Caerphilly Prospective Study. Eur. J. Nutr. 2018, 57, 1245–1258. [Google Scholar] [CrossRef]
- Furbatto, M.; Lelli, D.; Antonelli Incalzi, R.; Pedone, C. Mediterranean Diet in Older Adults: Cardiovascular Outcomes and Mortality from Observational and Interventional Studies—A Systematic Review and Meta-Analysis. Nutrients 2024, 16, 3947. [Google Scholar] [CrossRef] [PubMed]
- Pant, A.; Chew, D.P.; Mamas, M.A.; Zaman, S. Cardiovascular Disease and the Mediterranean Diet: Insights into Sex-Specific Responses. Nutrients 2024, 16, 570. [Google Scholar] [CrossRef] [PubMed]
- Martimianaki, G.; Peppa, E.; Valanou, E.; Papatesta, E.M.; Klinaki, E.; Trichopoulou, A. Today’s Mediterranean Diet in Greece: Findings from the National Health and Nutrition Survey—HYDRIA (2013–2014). Nutrients 2022, 14, 1193. [Google Scholar] [CrossRef]
- Obeid, C.A.; Gubbels, J.S.; Jaalouk, D.; Kremers, S.P.J.; Oenema, A. Adherence to the Mediterranean diet among adults in Mediterranean countries: A systematic literature review. Eur. J. Nutr. 2022, 61, 3327–3344. [Google Scholar] [CrossRef]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisle, F. Gender differences in food choice: The contribution of health beliefs and dieting. Ann. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.H.; Wardle, J. Sex differences in health behaviours in young adults. Psychol. Health 2003, 18, 651–668. [Google Scholar]
- Courtenay, W.H. Constructions of masculinity and their influence on men’s well-being: A theory of gender and health. Soc. Sci. Med. 2000, 50, 1385–1401. [Google Scholar] [CrossRef]
- Lee, H.J.; Ryu, H.; Kang, H.S. The effects of marital status on health behaviors in middle-aged and elderly Koreans. Int. J. Environ. Res. Public Health 2020, 17, 628. [Google Scholar]
- Umberson, D. Gender, marital status and the social control of health behavior. Soc. Sci. Med. 1992, 34, 907–917. [Google Scholar] [CrossRef]
- Hanna, K.L.; Collins, P.F. Relationship between living alone and food and nutrient intake. Nutr. Rev. 2015, 73, 594–611. [Google Scholar] [CrossRef]
- Lenz, M.; Richter, T.; Mühlhauser, I. The morbidity and mortality associated with overweight and obesity in adulthood: A systematic review. Dtsch. Arztebl. Int. 2009, 106, 641–648. [Google Scholar] [PubMed]
- Plotnikoff, R.C.; Costigan, S.A.; Karunamuni, N.; Lubans, D.R. Social cognitive theories used to explain physical activity behavior in adolescents: A systematic review and meta-analysis. Prev. Med. 2013, 56, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Spring, B.; Moller, A.C.; Coons, M.J. Multiple health behaviours: Overview and implications. J. Public Health 2012, 34 (Suppl. S1), i3–i10. [Google Scholar] [CrossRef] [PubMed]
- Poortinga, W. The prevalence and clustering of four major lifestyle risk factors in an English adult population. Prev. Med. 2007, 44, 124–128. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| N | N % | ||
|---|---|---|---|
| Age (years) | 63.8 ± 9.6 * | ||
| Biological sex | Female | 13 | 14.4% |
| Male | 77 | 85.6% | |
| Higher level of education | Up to secondary education | 21 | 23.3% |
| Post-secondary non-tertiary education | 41 | 45.6% | |
| Tertiary education | 21 | 23.3% | |
| MSc/PhD | 7 | 7.8% | |
| Economic level | Low | 24 | 26.7% |
| Middle | 48 | 53.3% | |
| High | 18 | 20.0% | |
| Marital status | Single, divorced, or widowed | 30 | 33.3% |
| Married or cohabiting | 60 | 66.7% | |
| Physical activity | Low | 32 | 35.6% |
| Middle | 43 | 47.8% | |
| High | 15 | 16.7% | |
| Smoking | Smoker | 17 | 18.9% |
| Ex-smoker | 54 | 60.0% | |
| Non-smoker | 19 | 21.1% | |
| Alcohol consumption | Medium consumption | 19 | 21.1% |
| Social consumption | 55 | 61.1% | |
| No consumption | 16 | 17.8% | |
| Unstandardized Coefficients | Standardized Coefficients | t | Sig. | 95.0% Confidence Interval for B | |||
|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | Lower Bound | Upper Bound | |||
| (Constant) | 63.665 | 20.479 | 3.109 | 0.003 | 22.918 | 104.412 | |
| Age | −1.181 | 0.234 | −0.660 | −5.052 | 0.000 | −1.647 | −0.716 |
| Biological sex | 5.041 | 2.438 | 0.104 | 2.068 | 0.042 | 0.191 | 9.891 |
| Higher level of education | −0.564 | 1.647 | −0.029 | −0.342 | 0.733 | −3.842 | 2.714 |
| Economic level | 1.161 | 2.202 | 0.046 | 0.527 | 0.600 | −3.221 | 5.543 |
| Marital status | 10.905 | 2.118 | 0.301 | 5.149 | 0.000 | 6.691 | 15.120 |
| Physical activity | 4.500 | 1.355 | 0.184 | 3.321 | 0.001 | 1.804 | 7.196 |
| Smoking | −6.399 | 2.733 | −0.237 | −2.341 | 0.022 | −11.837 | −0.960 |
| Alcohol | 3.473 | 2.496 | 0.127 | 1.391 | 0.168 | −1.493 | 8.439 |
| CDQ-2 | |||
|---|---|---|---|
| Mean | Standard Deviation | ||
| Biological sex | Female | 19.3 | 5.4 |
| Male | 0.1 | 16.9 | |
| Higher level of education | Up to secondary education | −19.1 | 1.8 |
| Post-secondary non-tertiary education | 2.5 | 13.9 | |
| Tertiary education | 19.6 | 1.2 | |
| MSc/PhD | 21.1 | 1.7 | |
| Economic level | Low | −15.6 | 10.3 |
| Middle | 6.9 | 13.6 | |
| High | 16.8 | 12.5 | |
| Marital status | Single, divorced, or widowed | −16.7 | 4.8 |
| Married or cohabiting | 12.7 | 11.8 | |
| Physical activity | Low | −14.2 | 7.3 |
| Middle | 9.7 | 14.5 | |
| High | 19.9 | 1.4 | |
| Smoking | Smoker | −14.0 | 12.5 |
| Ex-smoker | 3.9 | 15.2 | |
| Non-smoker | 15.1 | 14.3 | |
| Alcohol consumption | Medium consumption | −13.6 | 11.8 |
| Social consumption | 3.3 | 15.7 | |
| No consumption | 21.1 | 0.9 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giakoumidakis, K.; Patelarou, E.; Chatziefstratiou, A.A.; Aloizou, D.; Vaitsis, N.; Brokalaki, H.; Fotos, N.V.; Geniataki, E.; Patelarou, A.E. Validation of the Greek Cardiovascular Diet Questionnaire 2 (CDQ-2) and Single-Center Cross-Sectional Insights into the Dietary Habits of Cardiovascular Patients. Nutrients 2025, 17, 1649. https://doi.org/10.3390/nu17101649
Giakoumidakis K, Patelarou E, Chatziefstratiou AA, Aloizou D, Vaitsis N, Brokalaki H, Fotos NV, Geniataki E, Patelarou AE. Validation of the Greek Cardiovascular Diet Questionnaire 2 (CDQ-2) and Single-Center Cross-Sectional Insights into the Dietary Habits of Cardiovascular Patients. Nutrients. 2025; 17(10):1649. https://doi.org/10.3390/nu17101649
Chicago/Turabian StyleGiakoumidakis, Konstantinos, Evridiki Patelarou, Anastasia A. Chatziefstratiou, Dimitra Aloizou, Nikolaos Vaitsis, Hero Brokalaki, Nikolaos V. Fotos, Elisabeth Geniataki, and Athina E. Patelarou. 2025. "Validation of the Greek Cardiovascular Diet Questionnaire 2 (CDQ-2) and Single-Center Cross-Sectional Insights into the Dietary Habits of Cardiovascular Patients" Nutrients 17, no. 10: 1649. https://doi.org/10.3390/nu17101649
APA StyleGiakoumidakis, K., Patelarou, E., Chatziefstratiou, A. A., Aloizou, D., Vaitsis, N., Brokalaki, H., Fotos, N. V., Geniataki, E., & Patelarou, A. E. (2025). Validation of the Greek Cardiovascular Diet Questionnaire 2 (CDQ-2) and Single-Center Cross-Sectional Insights into the Dietary Habits of Cardiovascular Patients. Nutrients, 17(10), 1649. https://doi.org/10.3390/nu17101649