
Vitamin Status and Risk of Age-Related Diseases Among Adult Residents of the Pearl River Delta Region

 ,
,
Abstract

1. Introduction
2. Materials
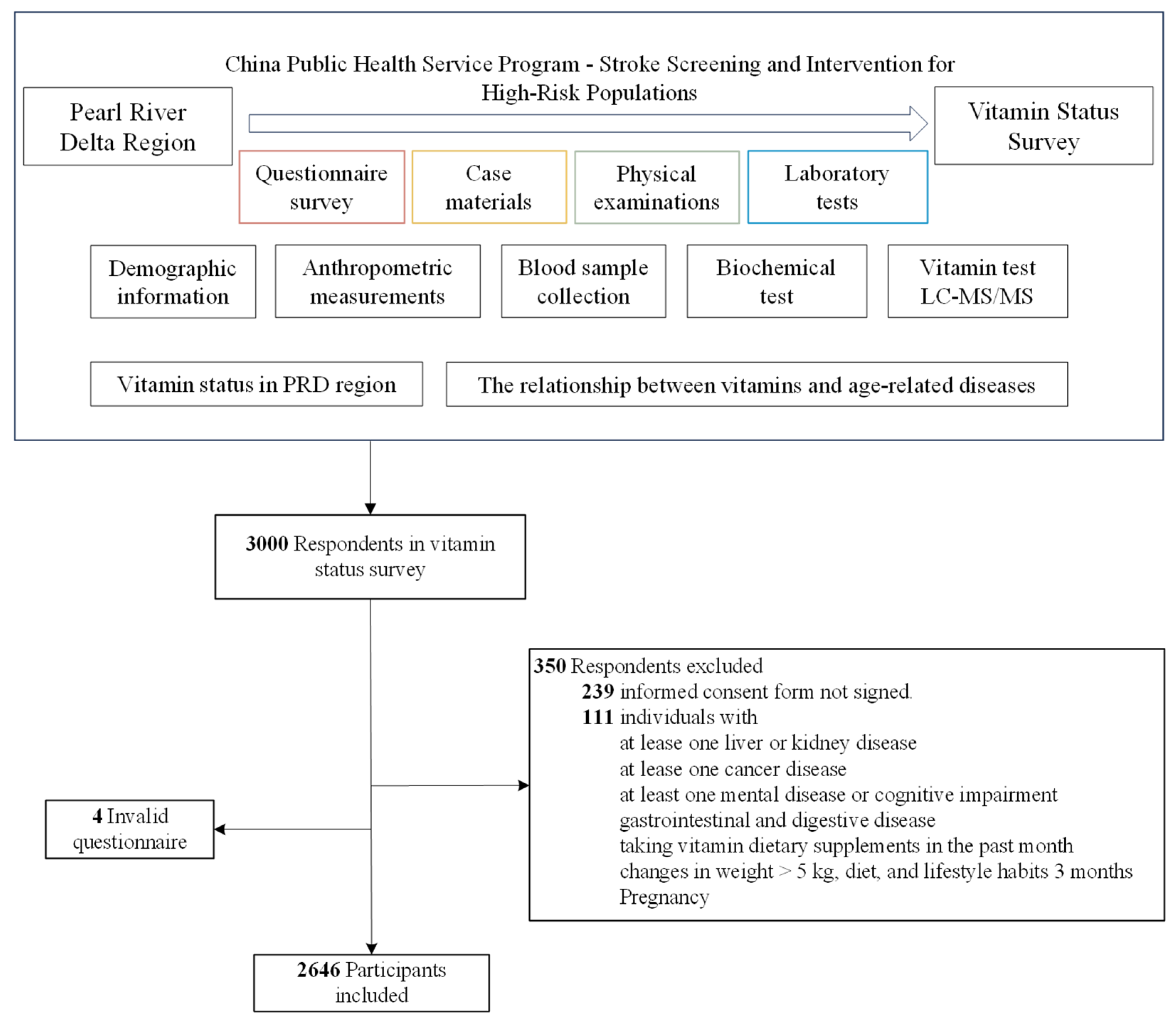
2.1. Study Design and Participants
2.2. Blood Biochemistry Test
2.3. Definition of Age-Related Diseases
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Main Findings
4.1.1. Blood Vitamin Status
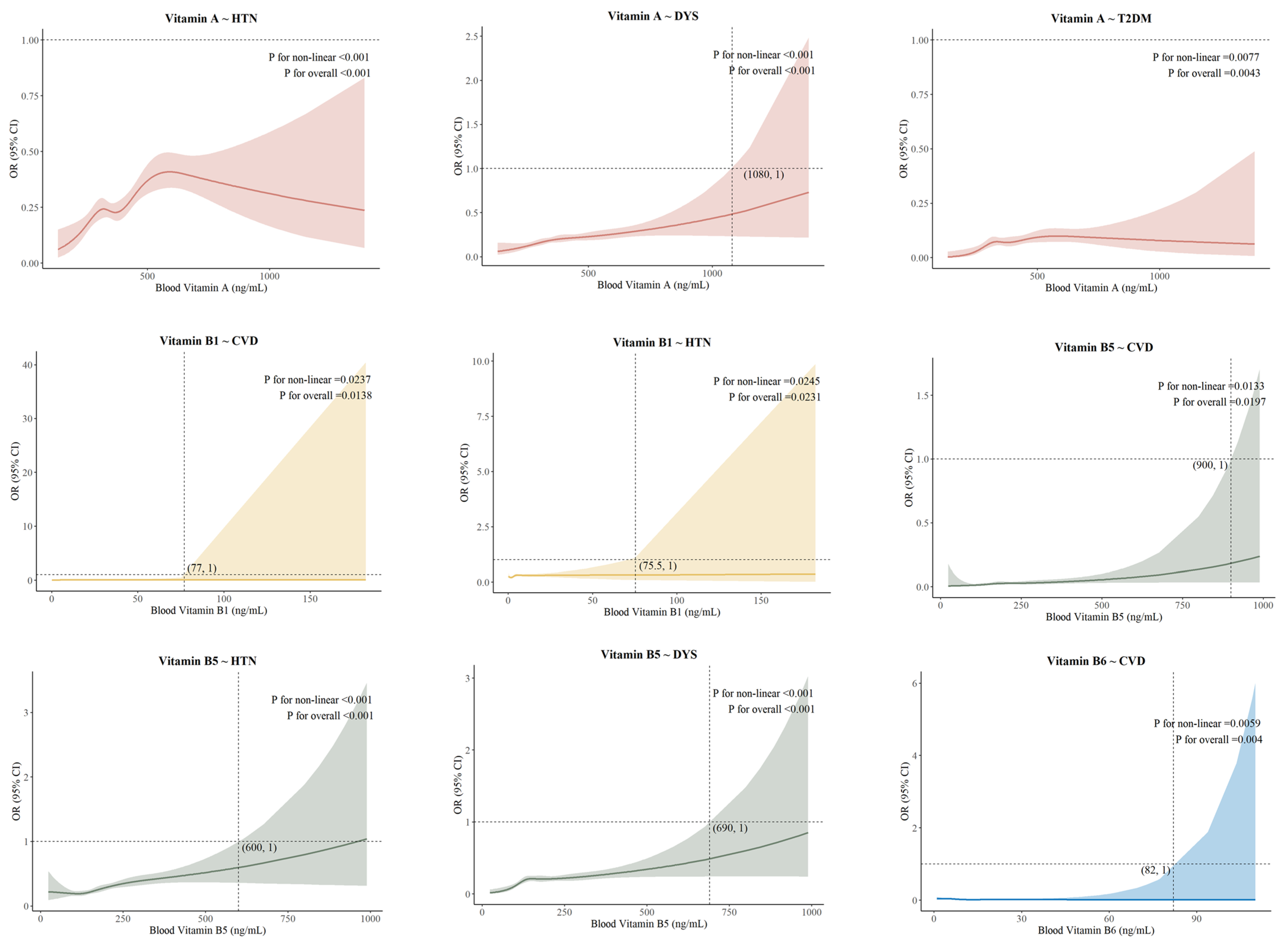
4.1.2. Dose–Response Associations
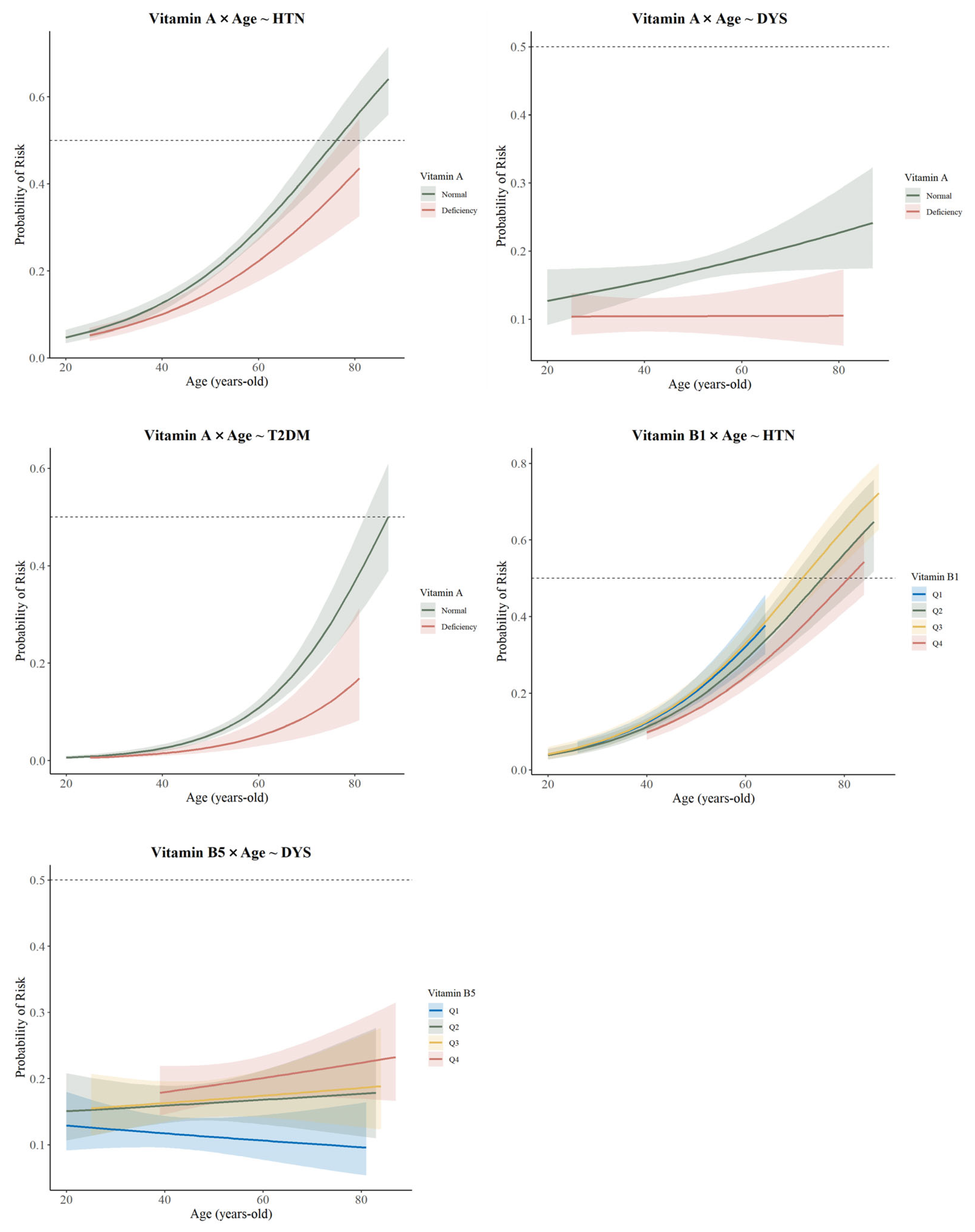
4.1.3. The Interaction Effect of Age
4.1.4. Mediating Effect of BRI and Physical Activity
4.2. Implication
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PRD | Pearl River Delta |
| HbA1c | Glycosylated hemoglobin |
| LDL-C | Low-Density Lipoprotein Cholesterol |
| HDL-C | High-Density Lipoprotein Cholesterol |
| Cys | Homocysteine |
| BRI | Body Roundness Index |
| SD | Standard deviation |
| CI | Confidence intervals |
| RCS | Restricted Cubic Spline |
| OR | Odds ratio |
| CVD | Cerebrovascular Disease |
| CHD | Coronary Heart Disease |
| HTN | Hypertension |
| DYS | Dyslipidemia |
| T2DM | Type-2 Diabetes Mellitus |
References
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.; Mahanani, W.R.; et al. The World Report on Ageing and Health: A Policy Framework for Healthy Ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Yin, P.; Qi, J.; Zhou, M. Burden of non-Communicable Diseases in China and Its Provinces, 1990–2021: Results from the Global Burden of Disease Study 2021. Chin. Med. J. 2024, 137, 2325–2333. [Google Scholar] [CrossRef] [PubMed]
- Hacker, K. The Burden of Chronic Disease. Mayo Clin. Proc. Innov. Qual. Outcomes 2024, 8, 112–119. [Google Scholar] [CrossRef]
- Jia, X.; Xu, L.; Zhang, Y.; Hu, H.; Wang, X.; Zhuo, L.; Chen, J. The Current Status of Common Chronic Diseases Among Chinese 15-Year-Olds and Their Impact on Quality of Life. China Public Health 2017, 33, 1567–1570. [Google Scholar] [CrossRef]
- Ma, X.; Guo, Y.; Li, P.; Xu, J.; Gao, Y.; Ren, X.; Van Halm-Lutterodt, N.; Yuan, L. Association Between ApoE Status, Circulating Vitamin A and Vitamin E Levels with Dyslipidemia in Aging Adults. Arch. Med. Res. 2021, 52, 703–712. [Google Scholar] [CrossRef]
- Hong, Y.; Zhou, Z.; Zhang, N.; He, Q.; Guo, Z.; Liu, L.; Song, Y.; Chen, P.; Wei, Y.; Xu, Q.; et al. Association Between Plasma Vitamin B5 levels and All-Cause Mortality: A Nested Case-Control Study. J. Clin. Hypertens 2022, 24, 945–954. [Google Scholar] [CrossRef]
- Lips, P.; Eekhoff, M.; van Schoor, N.; Oosterwerff, M.; de Jongh, R.; Krul-Poel, Y.; Simsek, S. Vitamin D and Type 2 Diabetes. J. Steroid Biochem. Mol. Biol. 2017, 173, 280–285. [Google Scholar] [CrossRef]
- Saito, Y. Lipid Peroxidation Products as a Mediator of Toxicity and Adaptive Response—The Regulatory Role of Selenoprotein and Vitamin E. Arch. Biochem. Biophys. 2021, 703, 108840. [Google Scholar] [CrossRef]
- Guangdong Provincial Development and Reform Commission. Special Plan for the Pearl River Delta to Take the Lead in Basically Realizing Modernization—Special Plan for the Open Economic Intensive Area of the Pearl River Delta. Available online: https://drc.gd.gov.cn/fzgh5637/content/post_1056846.html (accessed on 1 January 2025).
- Bu, T.; Tang, D.; Liu, Y.; Chen, D. Trends in Dietary Patterns and Diet-Related Behaviors in China. Am. J. Health Behav. 2021, 45, 371–383. [Google Scholar] [CrossRef]
- Jia, X.; Su, C.; He, Y.; Du, W.; Zhang, J.; Huang, F.; Zhang, X.; Guan, F.; Bai, J.; Wei, Y.; et al. Current Status and Food Sources of Macronutrient Intake of Adult Residents in 10 Provinces (Autonomous Regions) of China from 2022 to 2023. J. Hyg. Res. 2024, 53, 862–869, 879. [Google Scholar] [CrossRef]
- Liu, W.; Hu, J.; Fang, Y.; Wang, P.; Lu, Y.; Shen, N. Vitamin D status in Mainland of China: A Systematic Review and Meta-Analysis. eClinicalMedicine 2021, 38, 101017. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zheng, C.; Tinker, L.F.; Neuhouser, M.L.; Prentice, R.L. Biomarker-Based Methods and Study Designs to Calibrate Dietary Intake for Assessing Diet–Disease Associations. J. Nutr. 2022, 152, 899–906. [Google Scholar] [CrossRef] [PubMed]
- ISO/IEC17025:2005-5-15; Accreditation Criteria for the Competence of Testing and Calibration Laboratories. Available online: https://www.zcmlab.com/uploads/soft/20201124/ISOIEC170252017.pdf (accessed on 8 May 2025).
- WS/T 553-2017; Method for Vitamin A Deficiency Screening. Available online: http://www.nhc.gov.cn/ewebeditor/uploadfile/2017/08/20170811093617394.pdf (accessed on 8 May 2025).
- WS/T 677-2020; Method for Vitamin D Deficiency Screening. Available online: https://std.samr.gov.cn/hb/search/stdHBDetailed?id=A701D7A974CFA3B7E05397BE0A0AEB89 (accessed on 8 May 2025).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2024; Available online: https://R-project.org/ (accessed on 8 May 2025).
- National Health Commission. Report on the Nutrition and Chronic Disease Status of Chinese Residents (2020). J. Nutr. 2020, 42, 521. [Google Scholar]
- Ji, S.; Zhou, Y.; Zhao, Q.; Chen, R.; Su, Z. Trends in Three Malnutrition Factors in the Global Burden of Disease: Iodine Deficiency, Vitamin A Deficiency, and Protein-Energy Malnutrition (1990–2019). Front. Nutr. 2024, 11, 1426790. [Google Scholar] [CrossRef]
- Ning, Z.; Song, S.; Miao, L.; Zhang, P.; Wang, X.; Liu, J.; Hu, Y.; Xu, Y.; Zhao, T.; Liang, Y.; et al. High Prevalence of Vitamin D Deficiency in Urban Health Checkup Population. Clin. Nutr. 2016, 35, 859–863. [Google Scholar] [CrossRef]
- Wierzbicka, A.; Oczkowicz, M. Sex Differences in Vitamin D Metabolism, Serum Levels and Action. Br. J. Nutr. 2022, 128, 2115–2130. [Google Scholar] [CrossRef]
- Miao, X.; Li, B.; Zhu, Z.; Yang, T. Sex Differences in the Association Between Composite Dietary Antioxidant Index and Hyperlipidemia: Insights from Nhanes. PLoS ONE 2025, 20, e0316130. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-H.; Liu, L.-K.; Chen, M.-J.; Lee, W.-J.; Lin, M.-H.; Peng, L.-N.; Chen, L.-K. Associations Between Vitamin D Deficiency, Musculoskeletal Health, and Cardiometabolic Risk Among Community-Living People in Taiwan: Age and Sex-Specific Relationship. Medicine 2018, 97, e13886. [Google Scholar] [CrossRef] [PubMed]
- Kestenbaum, B.; Katz, R.; de Boer, I.; Hoofnagle, A.; Sarnak, M.J.; Shlipak, M.G.; Jenny, N.S.; Siscovick, D.S. Vitamin D, Parathyroid Hormone, and Cardiovascular Events Among Older Adults. J. Am. Coll. Cardiol. 2011, 58, 1433–1441. [Google Scholar] [CrossRef]
- Luttmann-Gibson, H.; Mora, S.; Camargo, C.A.; Cook, N.R.; Demler, O.V.; Ghoshal, A.; Wohlgemuth, J.; Kulkarni, K.; Larsen, J.; Prentice, J. Serum 25-Hydroxyvitamin D in the Vitamin D and Omega-3 Trial (Vital): Clinical and Demographic Characteristics Associated with Baseline and Change with Randomized Vitamin D Treatment. Contemp. Clin. Trials 2019, 87, 105854. [Google Scholar] [CrossRef]
- Sun, P.; Weng, H.; Fan, F.; Zhang, N.; Liu, Z.; Chen, P.; Jia, J.; Zheng, B.; Yi, T.; Li, Y.; et al. Association between Plasma Vitamin B5 and Coronary Heart Disease: Results from a Case-Control Study. Front. Cardiovasc. Med. 2022, 9, 906232. [Google Scholar] [CrossRef]
- Yu, L.; Wang, Y.; Yu, D.; Zhang, S.; Zheng, F.; Ding, N.; Zhu, L.; Zhu, Q.; Sun, W.; Li, S.; et al. Association Between Serum Vitamin A, Blood Lipid Level and Dyslipidemia among Chinese Children and Adolescents. Nutrients 2022, 14, 1444. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Mason, A.M.; Carter, P.; Burgess, S.; Larsson, S.C. Homocysteine, B Vitamins, and Cardiovascular Disease: A Mendelian Randomization Study. BMC Med. 2021, 19, 97. [Google Scholar] [CrossRef] [PubMed]
- Duester, G. Retinoic Acid Synthesis and Signaling During Early Organogenesis. Cell 2008, 134, 921–931. [Google Scholar] [CrossRef]
- Li, P.; Xu, J.; Guo, Y.; Ma, X.; Zhou, S.; Zhang, C.; Yu, H.; Wang, Y.; Wang, X.; Yuan, L. Association of Plasma Vitamin A Level with Type 2 Diabetes Mellitus: A Community Aging Population-Based Cross-Sectional Study. Food Sci. Hum. Wellness 2024, 13, 2079–2089. [Google Scholar] [CrossRef]
- Wang, L.; Li, X.; Montazeri, A.; MacFarlane, A.J.; Momoli, F.; Duthie, S.; Senekal, M.; Eguiagaray, I.M.; Munger, R.; Bennett, D.; et al. Phenome-Wide Association Study of Genetically Predicted B Vitamins and Homocysteine Biomarkers with Multiple Health and Disease Outcomes: Analysis of the UK Biobank. Am. J. Clin. Nutr. 2023, 117, 564–575. [Google Scholar] [CrossRef]
- Li, Y.M.; Xu, X.H.; Xu, X.F.; Yang, X.X.; Dai, Y.L.; Song, D.X.; Jin, C.Q.; Jia, Y.X. Association Between Vitamin B1 Intake and Hyperuricemia in Adults. Sci. Rep. 2024, 14, 16428. [Google Scholar] [CrossRef]
- Lonsdale, D. A Review of the Biochemistry, Metabolism and Clinical Benefits of Thiamin(E) and Its Derivatives. Evid. Based Complement. Altern. Med. 2006, 3, 49–59. [Google Scholar] [CrossRef]
- Lotto, V.; Choi, S.W.; Friso, S. Vitamin B6: A Challenging Link between Nutrition and Inflammation in Cvd. Br. J. Nutr. 2011, 106, 183–195. [Google Scholar] [CrossRef]
- Gholizadeh, M.; Basafa Roodi, P.; Abaj, F.; Shab-Bidar, S.; Saedisomeolia, A.; Asbaghi, O.; Lak, M. Influence of Vitamin a Supplementation on Inflammatory Biomarkers in Adults: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Sci. Rep. 2022, 12, 21384. [Google Scholar] [CrossRef]
- Li, H.; Ye, J.; Dong, Y.; Kong, W.; Qian, G.; Xie, Y. U-Shaped Association of Serum Vitamin a Concentrations with All-Cause Mortality in Patients with Nafld: Results from the Nhanes Database Prospective Cohort Study. Front. Nutr. 2024, 11, 1467659. [Google Scholar] [CrossRef]
- Wu, Z.; Yang, W.; Fang, H.; Chen, Y.; Wu, Y.; Gong, R. Exploring the Association between Dietary Vitamin a and Coronary Artery Disease Risk in Men and Women: Findings from a Us Population Study. Front. Nutr. 2024, 11, 1418159. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Xiao, Y.; Yang, F.; Gao, X.; Zhu, X.; Qiao, G. Association between Dietary Total Vitamin a, Β-Carotene, and Retinol Intake and Risk of Cardiometabolic Multimorbidity: Results from the China Health and Nutrition Survey, 1997–2015. Res. Sq. 2024. [Google Scholar] [CrossRef]
- Mi, W.; Zhang, H.; Zhang, L.; Li, X.; Wang, Z.; Sun, Y.; Shen, T.; Fan, K.; Liu, C.; Xu, S. Age but Not Vitamin D Is Related to Sarcopenia in Vitamin D Sufficient Male Elderly in Rural China. Sci. Rep. 2025, 15, 765. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Peng, R.; Cao, J.; Kang, Y.; Qu, P.; Liu, Y.; Xiao, X.; Li, T. Serum Vitamin a Status Is Associated with Obesity and the Metabolic Syndrome among School-Age Children in Chongqing, China. Asia Pac. J. Clin. Nutr. 2016, 25, 563–570. [Google Scholar] [CrossRef]
- Lee, C.Y. Effects of Dietary Vitamins on Obesity-Related Metabolic Parameters. J. Nutr. Sci. 2023, 12, e47. [Google Scholar] [CrossRef]
- Brancaccio, M.; Mennitti, C.; Cesaro, A.; Fimiani, F.; Vano, M.; Gargiulo, B.; Caiazza, M.; Amodio, F.; Coto, I.; D’Alicandro, G.; et al. he Biological Role of Vitamins in Athletes’ Muscle, Heart and Microbiota. Int. J. Environ. Res. Public Health 2022, 19, 1249. [Google Scholar] [CrossRef]
- Chen, M.; Cheng, L.; Yang, S.; Zhang, Y. Physical Activity, Vitamin D, and All-Cause/Cardiovascular Mortality: A Prospective Study in Older Chinese Adults. BMC Geriatr. 2025, 25, 38. [Google Scholar] [CrossRef]
- Guo, J.; Huang, X.; Dou, L.; Yan, M.; Shen, T.; Tang, W.; Li, J. Aging and Aging-Related Diseases: From Molecular Mechanisms to Interventions and Treatments. Signal Transduct. Target. Ther. 2022, 7, 391. [Google Scholar] [CrossRef]
- Wang, Y.; Shi, H.; Zhang, Y.; Li, X.; Zhao, M.; Sun, B. Assessing the Foodshed and Food Self-Sufficiency of the Pearl River Delta Megacity Region in China. Foods 2023, 12, 4210. [Google Scholar] [CrossRef]
- Abad-Segura, E.; González-Zamar, M.D.; Gómez-Galán, J.; Bernal-Bravo, C. Management Accounting for Healthy Nutrition Education: Meta-Analysis. Nutrients 2020, 12, 3715. [Google Scholar] [CrossRef] [PubMed]
- Kaźmierczak-Barańska, J.; Karwowski, B.T. The Protective Role of Vitamin K in Aging and Age-Related Diseases. Nutrients 2024, 16, 4341. [Google Scholar] [CrossRef] [PubMed]
- Seib, C.; Moriarty, S.; McDonald, N.; Anderson, D.; Parkinson, J. Changes in Health Behaviours in Adults at-Risk of Chronic Disease: Primary Outcomes from the My Health for Life Program. BMC Public Health 2022, 22, 1648. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.L.; Grandpre, J.; Katz, D.L.; Shenson, D. The Impact of Key Modifiable Risk Factors on Leading Chronic Conditions. Prev. Med. 2019, 120, 113–118. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | CVD | p-Value | CHD | p-Value | HTN | p-Value | DYS | p-Value | T2DM | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (mean ± SD, years) | 50.92 ± 9.30 | 61.66 ± 10.76 | <0.001 | 65.48 ± 12.70 | <0.001 | 54.87 ± 10.62 | <0.001 | 53.72 ± 9.12 | <0.001 | 58.94 ± 10.40 | <0.001 |
| Sex (n, %) | |||||||||||
| Female | 951 (35.94) | 36 (2.13) | 0.966 | 22 (1.30) | 0.229 | 368 (21.71) | 0.026 | 286 (16.87) | 0.036 | 103 (6.08) | 0.330 |
| Male | 1695 (64.06) | 20 (2.15) | 18 (2.00) | 172 (18.09) | 131 (13.78) | 67 (7.05) | |||||
| Education (n, %) | |||||||||||
| Primary School and Below | 307 (11.60) | 16 (5.25) | <0.001 | 10 (3.26) | 0.048 | 91 (29.64) | <0.001 | 37 (12.05) | <0.001 | 44 (14.33) | <0.001 |
| Middle School | 885 (33.45) | 20 (2.27) | 8 (0.90) | 156 (17.63) | 75 (8.48) | 45 (5.09) | |||||
| High School | 990 (37.41) | 8 (0.81) | 16 (1.62) | 200 (20.20) | 168 (16.98) | 58 (5.86) | |||||
| Undergraduate | 434 (16.40) | 12 (2.77) | 5 (1.15) | 88 (20.28) | 125 (28.80) | 22 (5.07) | |||||
| Postgraduate and Above | 30 (1.13) | 0 (0.00) | 1 (3.33) | 5 (16.67) | 12 (40.00) | 1 (3.33) | |||||
| BRI a (n, %) | |||||||||||
| <3.41 (Very thin) | 2590 (97.88) | 55 (2.13) | 0.990 | 38 (1.47) | 0.552 | 521 (2.01) | 0.016 | 405 (15.64) | 0.621 | 1665.41) | 0.916 |
| 3.41–4.44 (Thin) | 51 (1.93) | 1 (1.96) | 2 (3.92) | 19 (37.26) | 11 (21.57) | 4 (7.84) | |||||
| 4.45–5.45 (Normal) | 4 (0.15) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 1 (25.00) | 0 (0.00) | |||||
| >5.46 (Mellow) | 1 (0.04) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |||||
| Smoking (n, %) | 642 (24.26) | 14 (2.19) | 0.892 | 7 (1.09) | 0.315 | 116 (18.07) | 0.091 | 91 (14.17) | 0.205 | 32 (4.98) | 0.087 |
| Alcohol Consumption (n, %) | 1026 (38.78) | 10 (0.98) | 0.003 | 8 (0.78) | 0.031 | 188 (18.32) | <0.001 | 164 (15.99) | 0.033 | 52 (5.07) | 0.018 |
| Physical inactivity (n, %) | 1075 (40.63) | 20 (1.86) | 0.444 | 14 (1.30) | 0.465 | 237 (22.05) | 0.084 | 187 (17.40) | 0.056 | 64 (5.95) | 0.413 |
| Family history of disease (n, %) | - | 14 (5.28) | <0.001 | 8 (4.37) | 0.001 | 277 (34.62) | <0.001 | 60 (14.42) | 0.004 | 51 (30.18) | <0.001 |
| Fasting blood glucose (mmol/L) | 4.87 ± 1.55 | 5.52 ± 2.31 | 0.217 | 5.46 ± 1.40 | 0.108 | 5.14 ± 1.80 | 0.804 | 4.99 ± 1.41 | 0.980 | 6.74 ± 2.56 | <0.001 |
| Glycosylated hemoglobin (%) | 5.25 ± 0.81 | 5.52 ± 0.87 | 0.298 | 5.43 ± 0.74 | 0.583 | 5.33 ± 0.90 | 0.702 | 5.33 ± 0.76 | 0.714 | 6.21 ± 1.45 | <0.001 |
| Triglyceride (mmol/L) | 1.49 ± 0.84 | 1.50 ± 0.70 | 0.803 | 1.48 ± 0.80 | 0.917 | 1.64 ± 0.88 | 0.264 | 1.84 ± 0.96 | <0.001 | 1.58 ± 0.82 | 0.429 |
| Total cholesterol (mmol/L) | 4.55 ± 0.93 | 4.30 ± 1.04 | 0.312 | 4.41 ± 0.93 | 0.687 | 4.58 ± 0.98 | 0.109 | 4.80 ± 0.99 | <0.001 | 4.51 ± 1.03 | 0.201 |
| LDL-C (mmol/L) | 2.44 ± 1.04 | 2.42 ± 0.95 | 0.517 | 2.52 ± 0.91 | 0.323 | 2.60 ± 0.81 | 0.103 | 2.78 ± 0.95 | <0.001 | 2.59 ± 0.85 | 0.900 |
| HDL-C (mmol/L) | 1.25 ± 0.32 | 1.24 ± 0.43 | 0.826 | 1.20 ± 0.25 | 0.472 | 1.19 ± 0.26 | 0.269 | 1.18 ± 0.29 | 0.106 | 1.20 ± 0.26 | 0.399 |
| Homocysteine (mol/L) | 13.58 ± 6.91 | 13.83 ± 5.69 | <0.001 | 14.22 ± 8.54 | <0.001 | 14.14 ± 6.68 | <0.001 | 13.65 ± 6.93 | 0.067 | 14.48 ± 8.64 | <0.001 |
| Total Effect (95%CI) | Direct Effect (95% CI) | Indirect Effect (95% CI) | pMe (%) a | |
|---|---|---|---|---|
| Vitamin A—HTN | ||||
| BRI | 0.200 (0.106, 0.294) *** | 0.161 (0.065, 0.255) *** | 0.039 (0.022, 0.056) *** | 19.73 |
| Smoking | 0.191 (0.099, 0.287) *** | 0.193 (0.099, 0.287) *** | −0.002 (−0.008, 0.003) | - |
| Alcohol | 0.190 (0.097, 0.283) *** | 0.193 (0.100, 0.287) *** | −0.003 (−0.013, 0.006) | - |
| Physical Activity | 0.186 (0.092, 0.280) *** | 0.190 (0.096, 0.284) *** | −0.003 (−0.010, 0.004) | - |
| Vitamin A—DYS | ||||
| BRI | 0.234 (0.132, 0.335) *** | 0.205 (0.103, 0.307) *** | 0.029 (0.013, 0.044) *** | 12.35 |
| Smoking | 0.231 (0.130, 0.332) *** | 0.233 (0.132, 0.334) *** | −0.002 (−0.006, 0.003) | - |
| Alcohol | 0.230 (0.128, 0.330) *** | 0.230 (0.129, 0.331) *** | −0.008 (−0.011, 0.010) | - |
| Physical Activity | 0.228 (0.126, 0.330) *** | 0.231 (0.129, 0.332) *** | −0.002 (−0.008, 0.003) | - |
| Vitamin A—T2DM | ||||
| BRI | 0.144 (−0.007, 0.296) | 0.129 (−0.023, 0.282) | 0.015 (−0.004, 0.034) | - |
| Smoking | 0.140 (−0.011, 0.292) | 0.143 (−0.008, 0.295) | −0.003 (−0.010, 0.004) | - |
| Alcohol | 0.140 (−0.011, 0.291) | 0.141 (−0.011, 0.292) | −0.001 (−0.017, 0.015) | - |
| Physical Activity | 0.130 (−0.023, 0.284) | 0.132 (−0.022, 0.285) | −0.001 (−0.006, 0.003) | - |
| Vitamin B1—CVD | ||||
| BRI | 0.045 (−0.131, 0.221) | 0.042 (−0.134, 0.219) | 0.002 (−0.005, 0.010) | - |
| Smoking | 0.004 (−0.130, 0.216) | 0.046 (−0.127, 0.219) | −0.003 (−0.012, 0.006) | - |
| Alcohol | 0.045 (−0.133, 0.224) | 0.041 (−0.138, 0.219) | 0.005 (−0.008, 0.017) | - |
| Physical Activity | 0.140 (−0.111, 0.391) | 0.157 (−0.094, 0.408) | −0.017 (−0.046, 0.012) | - |
| Vitamin B1—HTN | ||||
| BRI | 0.023 (−0.073, 0.120) | 0.015 (−0.082, 0.111) | 0.008 (−0.007, 0.024) | - |
| Smoking | 0.021 (−0.075, 0.118) | 0.018 (−0.078, 0.115) | 0.003 (−0.002, 0.008) | - |
| Alcohol | 0.022 (−0.074, 0.118) | 0.022 (−0.074, 0.118) | 0.0002 (−0.002, 0.002) | - |
| Physical Activity | 0.070 (−0.051, 0.191) | 0.086 (−0.035, 0.208) | −0.016 (−0.030,−0.003) | - |
| Vitamin B5—CVD | ||||
| BRI | 0.110 (−0.123, 0.343) | 0.096 (−0.141, 0.333) | 0.014 (−0.030, 0.058) | - |
| Smoking | 0.110 (−0.124, 0.344) | 0.116 (−0.120, 0.351) | −0.004 (−0.020, 0.008) | - |
| Alcohol | 0.107 (−0.127, 0.340) | 0.105 (−0.129, 0.338) | 0.002 (−0.009, 0.013) | - |
| Physical Activity | 0.087 (−0.151, 0.326) | 0.101 (−0.137, 0.339) | −0.014 (−0.038, 0.010) | - |
| Vitamin B5—HTN | ||||
| BRI | 0.178 (0.078, 0.279) *** | 0.123 (0.022, 0.225) * | 0.055 (0.034, 0.076) *** | 30.81 |
| Smoking | 0.172 (0.079, 0.271) *** | 0.167 (0.068, 0.265) *** | 0.005 (−0.0009, 0.012) | - |
| Alcohol | 0.172 (0.073, 0.270) *** | 0.172 (0.074, 0.270) *** | 0.0008 (−0.0007, 0.0009) | |
| Physical Activity | 0.177 (0.077, 0.276) *** | 0.191 (0.090, 0.291) *** | −0.014 (−0.025, 0.003) * | −8.10 |
| Vitamin B5—DYS | ||||
| BRI | 0.233 (0.127, 0.340) *** | 0.194 (0.087, 0.301) *** | 0.039 (0.019, 0.059) *** | 16.80 |
| Smoking | 0.229 (0.123, 0.334) *** | 0.225 (0.119, 0.330) *** | 0.004 (−0.002, 0.010) | - |
| Alcohol | 0.228 (0.123, 0.334) *** | 0.229 (0.123, 0.334) *** | −0.0008 (−0.0009, 0.0007) | - |
| Physical Activity | 0.242 (0.136, 0.348) *** | 0.254 (0.148, 0.361) *** | −0.012 (−0.023,−0.001) * | −5.07 |
| Vitamin B6—CVD | ||||
| BRI | −0.117 (−0.470, 0.236) | −0.116 (−0.469, 0.237) | −0.001 (−0.006, 0.004) | - |
| Smoking | −0.120 (−0.474, 0.234) | −0.131 (−0.487, 0.225) | 0.011 (−0.015, 0.037) | - |
| Alcohol | −0.125 (−0.477, 0.228) | −0.118 (−0.471, 0.234) | −0.006 (−0.020, 0.007) | - |
| Physical Activity | −0.130 (−0.495, 0.236) | −0.146 (−0.512, 0.220) | 0.016 (−0.012, 0.044) | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Y.; Zheng, S.; Wang, B.; Xiao, W.; He, P.; Bian, Y. Vitamin Status and Risk of Age-Related Diseases Among Adult Residents of the Pearl River Delta Region. Nutrients 2025, 17, 1637. https://doi.org/10.3390/nu17101637
Zhao Y, Zheng S, Wang B, Xiao W, He P, Bian Y. Vitamin Status and Risk of Age-Related Diseases Among Adult Residents of the Pearl River Delta Region. Nutrients. 2025; 17(10):1637. https://doi.org/10.3390/nu17101637
Chicago/Turabian StyleZhao, Yongze, Siqian Zheng, Bohan Wang, Wenhui Xiao, Ping He, and Ying Bian. 2025. "Vitamin Status and Risk of Age-Related Diseases Among Adult Residents of the Pearl River Delta Region" Nutrients 17, no. 10: 1637. https://doi.org/10.3390/nu17101637
APA StyleZhao, Y., Zheng, S., Wang, B., Xiao, W., He, P., & Bian, Y. (2025). Vitamin Status and Risk of Age-Related Diseases Among Adult Residents of the Pearl River Delta Region. Nutrients, 17(10), 1637. https://doi.org/10.3390/nu17101637