
Artificial Intelligence-Assisted Muscular Ultrasonography for Assessing Inflammation and Muscle Mass in Patients at Risk of Malnutrition

 , , ,
, , ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Eligibility Criteria
2.2. Variables
2.2.1. Anthropometric Measures
2.2.2. Electrical Bioimpedanciometry (BIA)
2.2.3. AI-Based Muscular Ultrasonography
2.2.4. Functional Status
2.2.5. Nutritional Blood Biomarkers
2.2.6. Nutritional Diagnosis
- Malnutrition diagnosis: A malnutrition diagnosis was made through the Global Leadership Initiative on Malnutrition (GLIM) criteria. Patients must have one phenotypic criterion and one etiologic criterion [1].
- -
- Phenotypic criteria: BMI and percentage of weight loss was assessed by anthropometric measures. Loss of muscle mass was assessed by BIA-estimated ASMI with Sergi’s Formula (ASMI < 7 kg/m2 in men and ASMI < 5.5 kg/m2 in women).
- -
- Etiologic criteria: Reduced food intake was assessed by a semiquantitative method in patient’s anamnesis, and disease burden/inflammation was considered based on their C-reactive protein levels. Low food intake was considered as below 75% of usual intake, and inflammation was considered with a level of C-reactive protein over 3 mg/L.
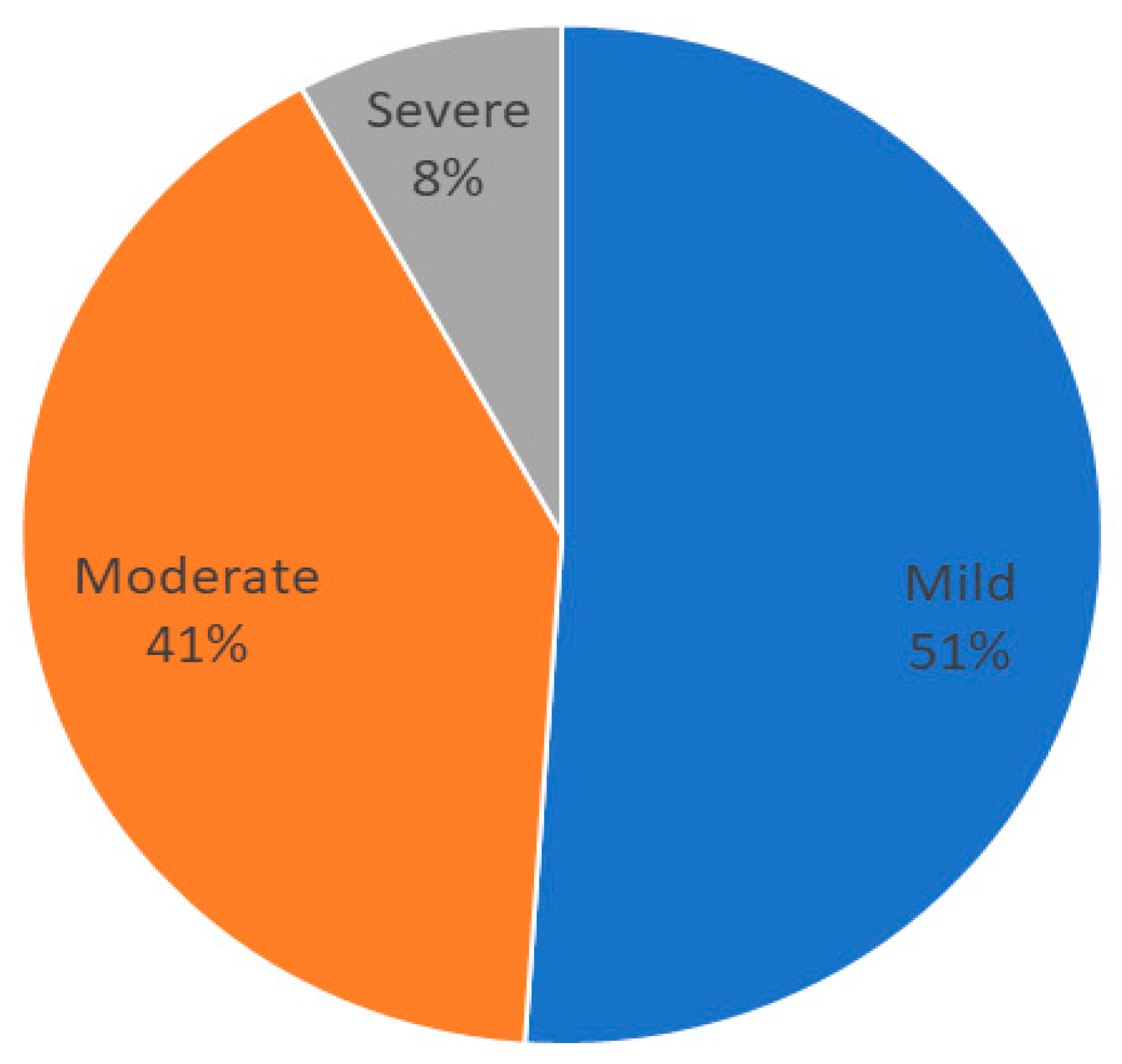
- Inflammation diagnosis: The degree of inflammation was assessed as the recommendation made in the Cederholm et al. Delphi study for guidance of etiologic criterion in GLIM [2]. We consider the following degrees of inflammation: no inflammation (CRP < 3 mg/L); mild inflammation (CRP = 3–9.9 mg/L); moderate inflammation (CRP = 10–49.9 mg/L); and severe inflammation (CRP > 50 mg/L).
- AI-based muscle ultrasonography diagnosis: In order to analyze the effect of inflammation on muscle parameters, we considered a quantitative method to diagnose low muscle mass and low muscle quality with the median values of our sample:
- -
- Muscle mass: A diagnosis of low muscle mass by US ultrasonography was made based on RFMA and RFMT. Low muscle mass was considered positive by RFMA with a value lower than the median of the sample (3.5 cm2 in men and 2.7 cm2 in women). Low muscle mass was considered positive by RFMT with a value lower than the median of the sample (1.06 cm in male and 0.9 cm in women).
- -
- Muscle quality: A diagnosis of low muscle quality by US ultrasonography was made based on low MiT and high FATiT. Muscle quality was considered low by MiT with a value lower than the median of the sample (< 47% in men and <44% in women). Muscle quality was considered low by FATiT with a value higher than the median of the sample (>36% in men and women).
2.3. Data Analysis
3. Results
3.1. Sample Description
3.2. AI-Assisted Muscular Ultrasonography in Malnutrition and Inflammation
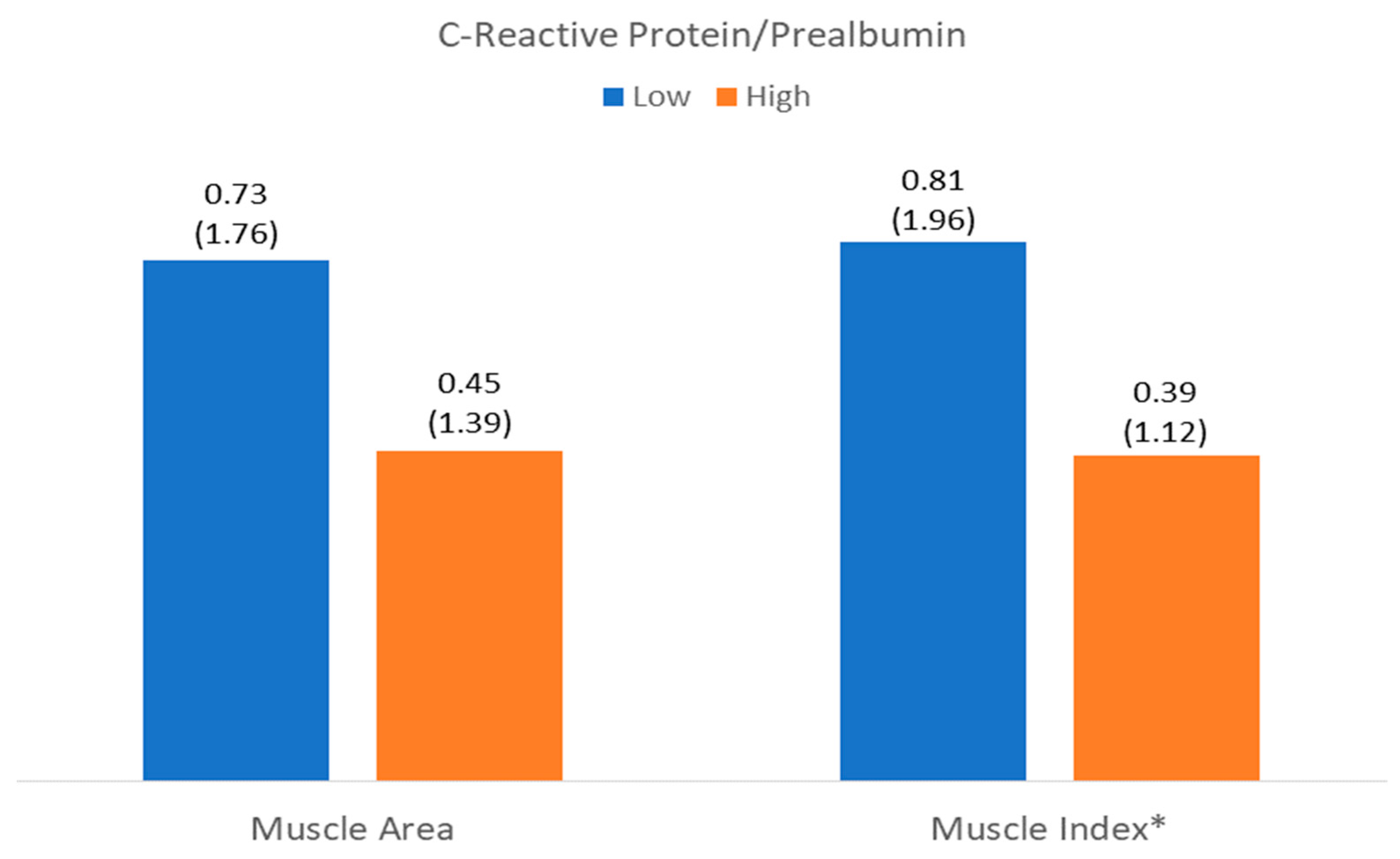
3.3. Relationship Between Muscle Mass and Quality with Inflammation
3.3.1. Muscle Mass
3.3.2. Muscle Quality
4. Discussion
4.1. Sample Characteristics
4.2. Muscle Mass and Quality and Inflammatory Status
4.3. Clinical Implications
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM Criteria for the Diagnosis of Malnutrition—A Consensus Report from the Global Clinical Nutrition Community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jensen, G.L.; Cederholm, T.; Ballesteros-Pomar, M.D.; Blaauw, R.; Correia, M.I.T.D.; Cuerda, C.; Evans, D.C.; Fukushima, R.; Gautier, J.B.O.; Gonzalez, M.C.; et al. Guidance for Assessment of the Inflammation Etiologic Criterion for the GLIM Diagnosis of Malnutrition: A Modified Delphi Approach. JPEN J. Parenter. Enteral Nutr. 2024, 48, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.; Yuan, K.; Ruan, G.; Wei, L.; Zhang, H.; Ge, Y.; Lin, S.; Song, M.; Wang, Z.; Liu, C.; et al. Improving the Assessment of Malnutrition in Cancer: Using Systemic Inflammation Markers as a Supplement to the Inflammation Items of the GLIM Criteria. Clin. Nutr. 2023, 42, 2036–2044. [Google Scholar] [CrossRef]
- Brown, D.; Loeliger, J.; Stewart, J.; Graham, K.L.; Goradia, S.; Gerges, C.; Lyons, S.; Connor, M.; Stewart, S.; Di Giovanni, A.; et al. Relationship between Global Leadership Initiative on Malnutrition (GLIM) Defined Malnutrition and Survival, Length of Stay and Post-Operative Complications in People with Cancer: A Systematic Review. Clin. Nutr. 2023, 42, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; Birdsell, L.; MacDonald, N.; Reiman, T.; Clandinin, M.T.; McCargar, L.J.; Murphy, R.; Ghosh, S.; Sawyer, M.B.; Baracos, V.E. Cancer Cachexia in the Age of Obesity: Skeletal Muscle Depletion Is a Powerful Prognostic Factor, Independent of Body Mass Index. J. Clin. Oncol. 2013, 31, 1539–1547. [Google Scholar] [CrossRef]
- Tu, H.; Li, Y.L. Inflammation Balance in Skeletal Muscle Damage and Repair. Front. Immunol. 2023, 14, 1133355. [Google Scholar] [CrossRef]
- Ji, Y.; Li, M.; Chang, M.; Liu, R.; Qiu, J.; Wang, K.; Deng, C.; Shen, Y.; Zhu, J.; Wang, W.; et al. Inflammation: Roles in Skeletal Muscle Atrophy. Antioxidants 2022, 11, 1686. [Google Scholar] [CrossRef]
- Shokri-Mashhadi, N.; Moradi, S.; Heidari, Z.; Saadat, S. Association of Circulating C-Reactive Protein and High-Sensitivity C-Reactive Protein with Components of Sarcopenia: A Systematic Review and Meta-Analysis of Observational Studies. Exp. Gerontol. 2021, 150, 111330. [Google Scholar] [CrossRef]
- Kim, B.J.; Lee, S.H.; Kwak, M.K.; Isales, C.M.; Koh, J.M.; Hamrick, M.W. Inverse Relationship between Serum hsCRP Concentration and Hand Grip Strength in Older Adults: A Nationwide Population-Based Study. Aging 2018, 10, 2051–2061. [Google Scholar] [CrossRef]
- Vieira, F.T.; Cai, Y.; Gonzalez, M.C.; Goodpaster, B.H.; Prado, C.M.; Haqq, A.M. Poor Muscle Quality: A Hidden and Detrimental Health Condition in Obesity. Rev. Endocr. Metab. Disord. 2025, 1–22, Online ahead of print. [Google Scholar] [CrossRef]
- Tuñón-Suárez, M.; Reyes-Ponce, A.; Godoy-Órdenes, R.; Quezada, N.; Flores-Opazo, M. Exercise Training to Decrease Ectopic Intermuscular Adipose Tissue in Individuals with Chronic Diseases: A Systematic Review and Meta-Analysis. Phys. Ther. 2021, 101, pzab162. [Google Scholar] [CrossRef]
- Bellido, D.; García-García, C.; Talluri, A.; Lukaski, H.C.; García-Almeida, J.M. Future Lines of Research on Phase Angle: Strengths and Limitations. Rev. Endocr. Metab. Disord. 2023, 24, 563–583. [Google Scholar] [CrossRef]
- de Luis Roman, D.; López Gómez, J.J.; Muñoz, M.; Primo, D.; Izaola, O.; Sánchez, I. Evaluation of Muscle Mass and Malnutrition in Patients with Colorectal Cancer Using the Global Leadership Initiative on Malnutrition Criteria and Comparing Bioelectrical Impedance Analysis and Computed Tomography Measurements. Nutrients 2024, 16, 3035. [Google Scholar] [CrossRef] [PubMed]
- García-Almeida, J.M.; García-García, C.; Ballesteros-Pomar, M.D.; Olveira, G.; Lopez-Gomez, J.J.; Bellido, V.; Bretón Lesmes, I.; Burgos, R.; Sanz-Paris, A.; Matia-Martin, P.; et al. Expert Consensus on Morphofunctional Assessment in Disease-Related Malnutrition: Grade Review and Delphi Study. Nutrients 2023, 15, 612. [Google Scholar] [CrossRef]
- López-Gómez, J.J.; García-Beneitez, D.; Jiménez-Sahagún, R.; Izaola-Jauregui, O.; Primo-Martín, D.; Ramos-Bachiller, B.; Gómez-Hoyos, E.; Delgado-García, E.; Pérez-López, P.; De Luis-Román, D.A. Nutritional Ultrasonography, a Method to Evaluate Muscle Mass and Quality in Morphofunctional Assessment of Disease-Related Malnutrition. Nutrients 2023, 15, 3923. [Google Scholar] [CrossRef] [PubMed]
- De Luis Roman, D.; García Almeida, J.M.; Bellido Guerrero, D.; Guzmán Rolo, G.; Martín, A.; Primo Martín, D.; García-Delgado, Y.; Guirado-Peláez, P.; Palmas, F.; Tejera Pérez, C.; et al. Ultrasound Cut-Off Values for Rectus Femoris for Detecting Sarcopenia in Patients with Nutritional Risk. Nutrients 2024, 16, 1552. [Google Scholar] [CrossRef]
- Di Ludovico, A.; La Bella, S.; Ciarelli, F.; Chiarelli, F.; Breda, L.; Mohn, A. Skeletal Muscle as a Pro- and Anti-Inflammatory Tissue: Insights from Children to Adults and Ultrasound Findings. J. Ultrasound 2024, 27, 769–779. [Google Scholar] [CrossRef] [PubMed]
- Attanasio, S.; Forte, S.M.; Restante, G.; Gabelloni, M.; Guglielmi, G.; Neri, E. Artificial Intelligence, Radiomics and Other Horizons in Body Composition Assessment. Quant. Imaging Med. Surg. 2020, 10, 1650–1660. [Google Scholar] [CrossRef]
- García-Herreros, S.; López Gómez, J.J.; Cebria, A.; Izaola, O.; Salvador Coloma, P.; Nozal, S.; Cano, J.; Primo, D.; Godoy, E.J.; de Luis, D. Validation of an Artificial Intelligence-Based Ultrasound Imaging System for Quantifying Muscle Architecture Parameters of the Rectus Femoris in Disease-Related Malnutrition (DRM). Nutrients 2024, 16, 1806. [Google Scholar] [CrossRef]
- López-Gómez, J.J.; Primo-Martín, D.; Cebria, A.; Izaola-Jauregui, O.; Godoy-Órdenes, R.; Pérez-López, P.; Jiménez Sahagún, R.; Jiménez Sahagún, R.; Ramos Bachiller, B.; González Gutiérrez, J.; et al. Effectiveness of High-Protein Energy-Dense Oral Supplements on Patients with Malnutrition Using Morphofunctional Assessment with AI-Assisted Muscle Ultrasonography: A Real-World One-Arm Study. Nutrients 2024, 16, 3136. [Google Scholar] [CrossRef]
- Campa, F.; Coratella, G.; Cerullo, G.; Noriega, Z.; Francisco, R.; Charrier, D.; Irurtia, A.; Lukaski, H.; Silva, A.M.; Paoli, A. High-Standard Predictive Equations for Estimating Body Composition Using Bioelectrical Impedance Analysis: A Systematic Review. J. Transl. Med. 2024, 22, 224. [Google Scholar] [CrossRef]
- García-Almeida, J.M.; García-García, C.; Vegas-Aguilar, I.M.; Ballesteros Pomar, M.D.; Cornejo-Pareja, I.M.; Fernández Medina, B.; de Luis Román, D.A.; Bellido Guerrero, D.; Bretón Lesmes, I.; Tinahones Madueño, F.J. Nutritional Ultrasound®: Conceptualisation, Technical Considerations and Standardisation. Endocrinol. Diabetes Nutr. 2023, 70, 74–84. [Google Scholar] [CrossRef]
- Rockenfeller, R.; Günther, M.; Clemente, C.J.; Dick, T.J.M. Rethinking the Physiological Cross-Sectional Area of Skeletal Muscle Reveals the Mechanical Advantage of Pennation. R. Soc. Open Sci. 2024, 11, 240037. [Google Scholar] [CrossRef]
- Lao, P.-S.; Chen, T.-S.; Chung, P.-C. A Fast Algorithm for Multilevel Thresholding. J. Inf. Sci. Eng. 2001, 17, 713–727. [Google Scholar]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Aihie Sayer, A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Pub. Med. 2019, 48, 16–31. [Google Scholar] [CrossRef]
- McGovern, J.; Skipworth, R.J.E.; Laird, B.J.A.; McMillan, D.C. Global Leadership Initiative on Malnutrition Cachexia: An Inflammation-First Approach for the Diagnosis of Disease-Related Malnutrition. Curr. Opin. Clin. Nutr. Metab. Care 2024, 27, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Jensen, G.L.; Ballesteros-Pomar, M.D.; Blaauw, R.; Correia, M.I.T.D.; Cuerda, C.; Evans, D.C.; Fukushima, R.; Ochoa Gautier, J.B.; Gonzalez, M.C.; et al. Guidance for Assessment of the Inflammation Etiologic Criterion for the GLIM Diagnosis of Malnutrition: A Modified Delphi Approach. Clin. Nutr. 2024, 43, 1025–1032. [Google Scholar] [CrossRef]
- Barazzoni, R.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Higashiguchi, T.; Shi, H.P.; Bischoff, S.C.; Heymsfield, S.; Mourtzakis, M.; Muscaritoli, M.; et al. Guidance for Assessment of the Muscle Mass Phenotypic Criterion for the Global Leadership Initiative on Malnutrition (GLIM) Diagnosis of Malnutrition. Clin. Nutr. 2022, 41, 1425–1433. [Google Scholar] [CrossRef]
- Dalle, S.; Rossmeislova, L.; Koppo, K. The Role of Inflammation in Age-Related Sarcopenia. Front. Physiol. 2017, 8, 1045. [Google Scholar] [CrossRef]
- Antuña, E.; Cachán-Vega, C.; Bermejo-Millo, J.C.; Potes, Y.; Caballero, B.; Vega-Naredo, I.; Coto-Montes, A.; Garcia-Gonzalez, C. Inflammaging: Implications in Sarcopenia. Int. J. Mol. Sci. 2022, 23, 15039. [Google Scholar] [CrossRef]
- Karanth, S.D.; Washington, C.; Cheng, T.Y.D.; Zhou, D.; Leeuwenburgh, C.; Braithwaite, D.; Zhang, D. Inflammation in Relation to Sarcopenia and Sarcopenic Obesity among Older Adults Living with Chronic Comorbidities: Results from the National Health and Nutrition Examination Survey 1999–2006. Nutrients 2021, 13, 3957. [Google Scholar] [CrossRef]
- Battaglia, Y.; Ullo, I.; Massarenti, S.; Esposito, P.; Prencipe, M.; Ciancio, G.; Fiorini, F.; Andreucci, M.; Storari, A.; Sabatino, A.; et al. Ultrasonography of Quadriceps Femoris Muscle and Subcutaneous Fat Tissue and Body Composition by BIVA in Chronic Dialysis Patients. Nutrients 2020, 12, 1388. [Google Scholar] [CrossRef] [PubMed]
- Palakshappa, J.A.; Reilly, J.P.; Schweickert, W.D.; Anderson, B.J.; Khoury, V.; Shashaty, M.G.; Forker, C.; Butler, K.; Ittner, C.A.; Feng, R.; et al. Quantitative Peripheral Muscle Ultrasound in Sepsis: Muscle Area Superior to Thickness. J. Crit. Care 2018, 47, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Stanley, B.; Greig, C.; Jackson, T.; Lewis, D.; Moorey, H.; Majid, Z.; Pinkney, T.; Welch, C. Investigating the Impact of Fluid Status on the Ultrasound Assessment of Muscle Quantity and Quality in the Diagnosis of Sarcopenia—A Multidimensional Cross-Sectional Study. BMC Geriatr. 2023, 23, 493. [Google Scholar] [CrossRef] [PubMed]
- Lei, L.; He, L.; Zou, T.; Qiu, J.; Li, Y.; Zhou, R.; Qin, Y.; Yin, W. Predicting Early Diagnosis of Intensive Care Unit-Acquired Weakness in Septic Patients Using Critical Ultrasound and Biological Markers. BMC Anesthesiol. 2025, 25, 39. [Google Scholar] [CrossRef]
- Yoshida, T.; Yamazaki, H.; Nishimori, Y.; Takamatsu, N.; Fukushima, K.; Osaki, Y.; Taniguchi, Y.; Nozaki, T.; Kumon, Y.; Albayda, J.; et al. Correlation of Muscle Ultrasound with Clinical and Pathological Findings in Idiopathic Inflammatory Myopathies. Muscle Nerve 2023, 68, 39–47. [Google Scholar] [CrossRef]
- Puthucheary, Z.A.; Phadke, R.; Rawal, J.; McPhail, M.J.W.; Sidhu, P.S.; Rowlerson, A.; Moxham, J.; Harridge, S.; Hart, N.; Montgomery, H.E. Qualitative Ultrasound in Acute Critical Illness Muscle Wasting. Crit. Care Med. 2015, 43, 1603–1611. [Google Scholar] [CrossRef]
- Grimm, A.; Teschner, U.; Porzelius, C.; Ludewig, K.; Zielske, J.; Witte, O.W.; Brunkhorst, F.M.; Axer, H. Muscle Ultrasound for Early Assessment of Critical Illness Neuromyopathy in Severe Sepsis. Crit. Care 2013, 17, R227. [Google Scholar] [CrossRef]
- De Luis, D.; Cebria, A.; Primo, D.; Izaola, O.; Godoy, E.J.; Lopez Gomez, J.J. Association between Muscle Mass Assessed by an Artificial Intelligence-Based Ultrasound Imaging System and Quality of Life in Patients with Cancer-Related Malnutrition. Nutrition 2025, 135, 112763. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TOTAL (n = 502) | MEN (n = 213) | WOMEN (n = 289) | p-Value | |
|---|---|---|---|---|
| ANTHROPOMETRY | ||||
| BMI (kg/m2) | 22.26 (4.84) | 23.29 (4.51) | 21.49 (4.94) | <0.01 |
| Arm circumference (cm) | 24.39 (3.72) | 25.40 (3.19) | 23.59 (3.92) | <0.01 |
| Calf circumference (cm) | 31.62 (4.10) | 32.26 (4.25) | 31.14 (3.93) | <0.01 |
| BIOIMPEDANCIOMETRY | ||||
| Resistance (ohm) | 597.97 (111.08) | 549.04 (94.91) | 634.08 (108.42) | <0.01 |
| Reactance (ohm) | 51.57 (12.21) | 49.72 (11.39) | 52.93 (12.62) | <0.01 |
| Phase Angle (°) | 4.97 (0.98) | 5.21 (0.99) | 4.79 (0.94) | <0.01 |
| TBW (l) | 9.12 (3.05) | 11.67 (2.39) | 7.24 (1.92) | <0.01 |
| ASMI (kg/m2) | 5.99 (1.06)) | 6.68 (0.93) | 5.49 (0.84) | <0.01 |
| RECTUS FEMORIS MUSCULAR ULTRASONOGRAPHY | ||||
| SFT (cm) | 0.78 (0.46) | 0.54 (0.28) | 0.97 (0.48) | <0.01 |
| RFMT (cm) | 0.98 (0.29) | 1.06 (0.32) | 0.91 (0.26) | <0.01 |
| RFMA (cm2) | 3.07 (1.16) | 3.51 (1.25) | 2.75 (0.96) | <0.01 |
| MiT (%) | 47.40 (11.39) | 49.40 (12.57) | 45.92 (10.22) | <0.01 |
| FATiT (%) | 38.68 (7.49) | 37.78 (8.34) | 39.34 (6.75) | 0.02 |
| NMNFiT (%) | 13.92 (5.48) | 12.82 (5.63) | 14.74 (5.23) | <0.01 |
| Pennation Angle (°) | 5.19 (2.89) | 5.61 (3.03) | 4.85 (2.75) | <0.01 |
| FUNCTIONAL MARKERS | ||||
| Handgrip Strength (kg) | 21.49 (9.31) | 26.44 (9.23) | 17.86 (7.53) | <0.01 |
| BIOCHEMICAL BIOMARKERS | ||||
| CRP (mg/L) | 2.19 (1–7.8) | 2.6 (1.10–7.14) | 1.9 (1–7.93) | 0.51 |
| Albumin (g/dL | 4.36 (2.37) | 4.41 (2.44) | 4.32 (2.31) | 0.66 |
| Prealbumin (g/dL) | 22.43 (8.47) | 22.78 (7.24) | 22.17 (9.28) | 0.47 |
| CRP/prealbumin | 0.09 (0.05–0.38) | 0.11 (0.05–0.39) | 0.08 (0.05–0.38) | 0.24 |
| CRP/albumin | 0.51 (0.24–1.95) | 0.6 (0.26–1.77) | 0.42 (0.23–2.15) | 0.21 |
| No Inflammation (n = 277) | Mild Inflammation (n = 115) | Moderate Inflammation (n = 92) | Severe Inflammation (n = 18) | p-Value | |
|---|---|---|---|---|---|
| Sex (M/F) (%) | 40.4/59.6 | 47.8/52.2 | 43.5/56.5 | 33.3/66.7 | 0.48 |
| Age (years) | 61.27 (16.89) | 65.55 (13.27) | 66.61 (15.69) | 75 (7.81) | <0.01 |
| ANTHROPOMETRY | |||||
| BMI (kg/m2) | 21.73 (4.80) | 23.31 (4.14) | 22.28 (5.62) | 23.68 (4.16) | 0.02 |
| Arm circumference (cm) | 24.1 (3.61) | 25.67 (3.95) | 23.75 (3.67) | 23.48 (2.24) | <0.01 |
| Calf circumference (cm) | 31.59 (4.19) | 32.14 (3.95) | 31.05 (3.89) | 31.53 (4.59) | 0.30 |
| BIOIMPEDANCIOMETRY | |||||
| Resistance (ohm) | 607.85 (115.34) | 593.34 (103.84) | 580.81 (106.82) | 560.71 (96.61) | 0.09 |
| Reactance (ohm) | 53.05 (11.79) | 52.11 (12.32) | 47.65 (12.29) | 44.77 (11.73) | <0.01 |
| Phase Angle (°) | 5.04 (0.98) | 5.07 (0.97) | 4.71 (0.95) | 4.56 (0.85) | <0.01 |
| TBW (l) | 9.04 (2.72) | 9.42 (2.72) | 9.18 (3.46) | 8.19 (2.09) | 0.39 |
| ASMI (kg/m2) | 5.91 (1.08) | 6.15 (0.95) | 6.03 (5.82) | 6.14 (0.85) | 0.21 |
| RECTUS FEMORIS MUSCULAR ULTRASONOGRAPHY | |||||
| SFT (cm) | 0.78 (0.44) | 0.82 (0.52) | 0.69 (0.38) | 0.89 (0.57) | 0.19 |
| RFMT (cm) | 1.01 (0.30) | 0.96 (0.27) | 0.91 (0.29) | 0.89 (0.29) | 0.02 |
| RFMA (cm2) | 3.19 (1.19) | 3.01 (1.07) | 2.85 (1.14) | 2.68 (1.11) | 0.03 |
| MiT (%) | 49.10 (12.19) | 45.79 (9.94) | 45.67 (9.55) | 40.48 (11.57) | <0.01 |
| FATiT (%) | 37.58 (7.91) | 39.77 (6.41) | 39.76 (6.30) | 40.47 (11.58) | <0.01 |
| NMNFiT (%) | 13.33 (5.63) | 14.44 (5.32) | 14.57 (4.97) | 16.42 (5.74) | 0.03 |
| Pennation Angle (°) | 5.17 (2.72) | 5.09 (3.35) | 4.68 (2.95) | 6.38 (2.39) | 0.51 |
| FUNCTIONAL MARKERS | |||||
| Handgrip Strength (kg) | 20.75 (9.54) | 22.94 (9.21) | 21.69 (8.54) | 22.44 (9.49) | 0.20 |
| SFT (cm) | RFMA (cm2) | RFMT (cm) | Pennation Angle (°) | MiT (%) | FATiT (%) | NMNFiT (%) | |
|---|---|---|---|---|---|---|---|
| CRP (mg/L) | r = 0.02; p = 0.68 | r = −0.09; p = 0.04 | r = −0.09; p = 0.05 | r = 0.06; p = 0.19 | r = −0.16; p < 0.01 | r = 0.16; p < 0.01 | r = 0.12; p < 0.01 |
| CRP/prealbumin | r = 0.03; p = 0.58 | r = −0.64; p = 0.16 | r = −0.06; p = 0.18 | r = 0.05; p = 323 | r = −0.18; p < 0.01 | r = 0.19; p < 0.01 | r = 0.12; p < 0.01 |
| CRP/albumin | r = 0.02; p = 0.75 | r = −0.08; p = 0.09 | r = −0.07; p = 0.09 | r = 0.05; p = 0.29 | r = −0.18; p < 0.01 | r = 0.18; p < 0.01 | r = 0.12; p < 0.01 |
| Phase angle (°) | r = −0.05; p = 0.29 | r = 0.46; p < 0.01 | r = 0.44; p < 0.01 | r = 0.19; p < 0.01 | r = 0.29; p < 0.01 | r = −0.22; p < 0.01 | r = −0.31; p < 0.01 |
| TBW (l) | r = −1.59; p < 0.01 | r = 0.45; p < 0.01 | r = 0.45; p < 0.01 | r = 0.18; p < 0.01 | r = 0.14; p < 0.01 | r = −0.08; p = 0.08 | r = −0.19; p < 0.01 |
| OR | IC 95% | p-Value | |
|---|---|---|---|
| LowMMUSArea (Male < 3.5 cm2; Female < 2.7 cm2) | |||
| Sex | 0.91 | 0.62–1.32 | 0.61 |
| Age > 65 years | 3.04 | 2.09–4.41 | <0.01 |
| CRP > 3 | 1.59 | 1.10–2.31 | 0.01 |
| LowMMUSthickness (Male < 1.06 cm; Female < 0.9 cm) | |||
| Sex | 0.93 | 0.64–1.35 | 0.69 |
| Age > 65 years | 3.34 | 2.37–4.99 | <0.01 |
| CRP > 3 | 1.23 | 0.85–1.78 | 0.28 |
| OR | IC 95% | p-Value | |
|---|---|---|---|
| LowMiT (Male < 47%; Female < 44%) | |||
| Sex | 0.89 | 0.62–1.31 | 0.57 |
| Age > 65 years | 2.18 | 1.49–3.18 | <0.01 |
| CRP > 3 | 1.25 | 1.01–1.54 | 0.04 |
| Sarcopenia | 1.72 | 1.13–2.62 | 0.01 |
| HighFATiT (Male > 36%; Female > 36%) | |||
| Sex | 0.73 | 0.51–1.06 | 0.09 |
| Age > 65 years | 1.54 | 1.06–2.24 | 0.02 |
| CRP > 3 | 1.19 | 0.97–1.46 | 0.09 |
| Sarcopenia | 1.26 | 0.83–1.89 | 0.28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Gómez, J.J.; Estévez-Asensio, L.; Cebriá, Á.; Izaola-Jauregui, O.; Pérez López, P.; González-Gutiérrez, J.; Primo-Martín, D.; Jiménez-Sahagún, R.; Gómez-Hoyos, E.; Rico-Bargues, D.; et al. Artificial Intelligence-Assisted Muscular Ultrasonography for Assessing Inflammation and Muscle Mass in Patients at Risk of Malnutrition. Nutrients 2025, 17, 1620. https://doi.org/10.3390/nu17101620
López-Gómez JJ, Estévez-Asensio L, Cebriá Á, Izaola-Jauregui O, Pérez López P, González-Gutiérrez J, Primo-Martín D, Jiménez-Sahagún R, Gómez-Hoyos E, Rico-Bargues D, et al. Artificial Intelligence-Assisted Muscular Ultrasonography for Assessing Inflammation and Muscle Mass in Patients at Risk of Malnutrition. Nutrients. 2025; 17(10):1620. https://doi.org/10.3390/nu17101620
Chicago/Turabian StyleLópez-Gómez, Juan José, Lucía Estévez-Asensio, Ángela Cebriá, Olatz Izaola-Jauregui, Paloma Pérez López, Jaime González-Gutiérrez, David Primo-Martín, Rebeca Jiménez-Sahagún, Emilia Gómez-Hoyos, Daniel Rico-Bargues, and et al. 2025. "Artificial Intelligence-Assisted Muscular Ultrasonography for Assessing Inflammation and Muscle Mass in Patients at Risk of Malnutrition" Nutrients 17, no. 10: 1620. https://doi.org/10.3390/nu17101620
APA StyleLópez-Gómez, J. J., Estévez-Asensio, L., Cebriá, Á., Izaola-Jauregui, O., Pérez López, P., González-Gutiérrez, J., Primo-Martín, D., Jiménez-Sahagún, R., Gómez-Hoyos, E., Rico-Bargues, D., Godoy, E. J., & De Luis-Román, D. A. (2025). Artificial Intelligence-Assisted Muscular Ultrasonography for Assessing Inflammation and Muscle Mass in Patients at Risk of Malnutrition. Nutrients, 17(10), 1620. https://doi.org/10.3390/nu17101620